
Metabolic Profile of Whole Unstimulated Saliva in Patients with Sjögren’s Syndrome
 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population selection
2.2. Saliva Collection
2.3. Sample Preparation
2.4. NMR Data Collection and Analysis
2.5. Statistical Analysis
3. Results
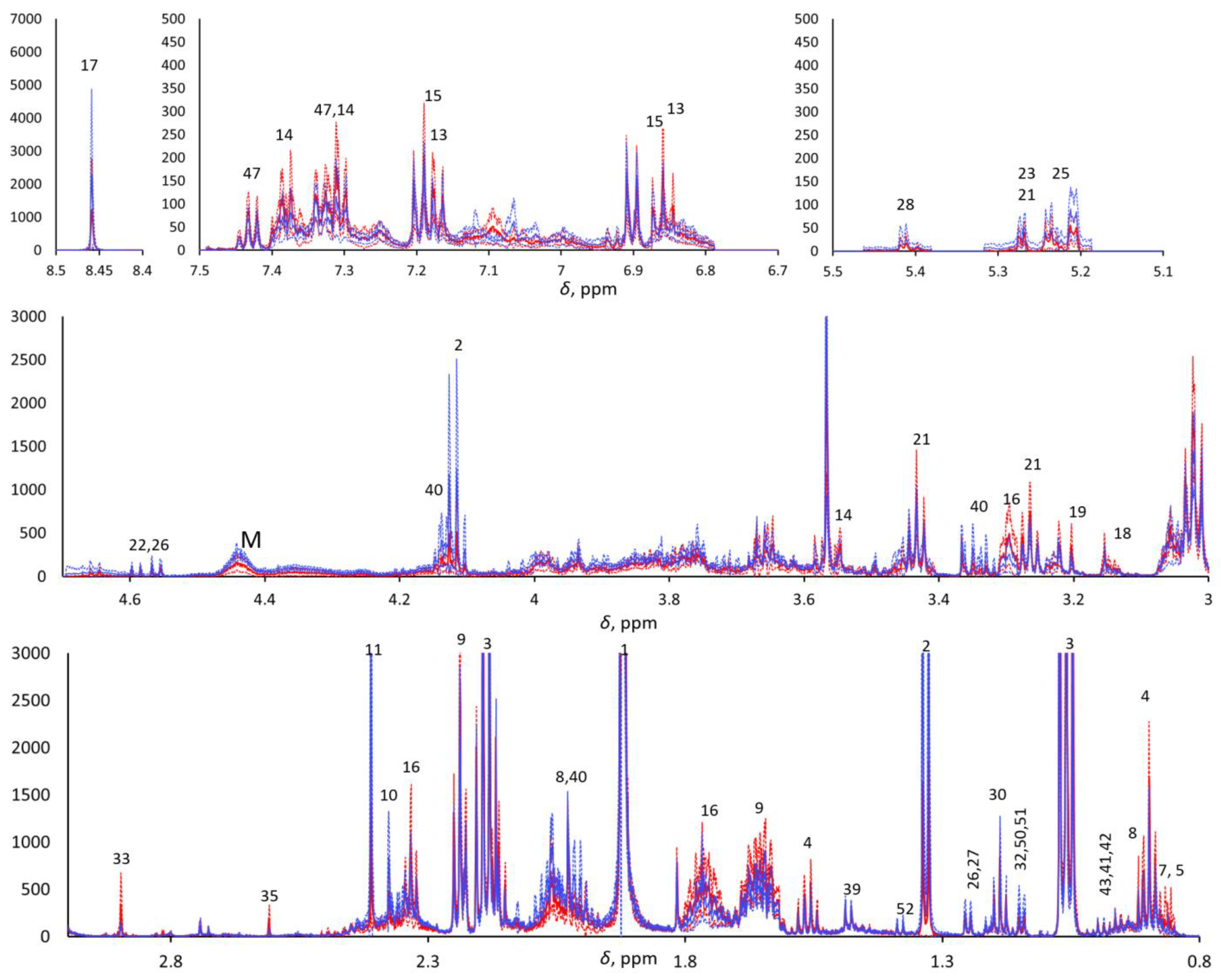
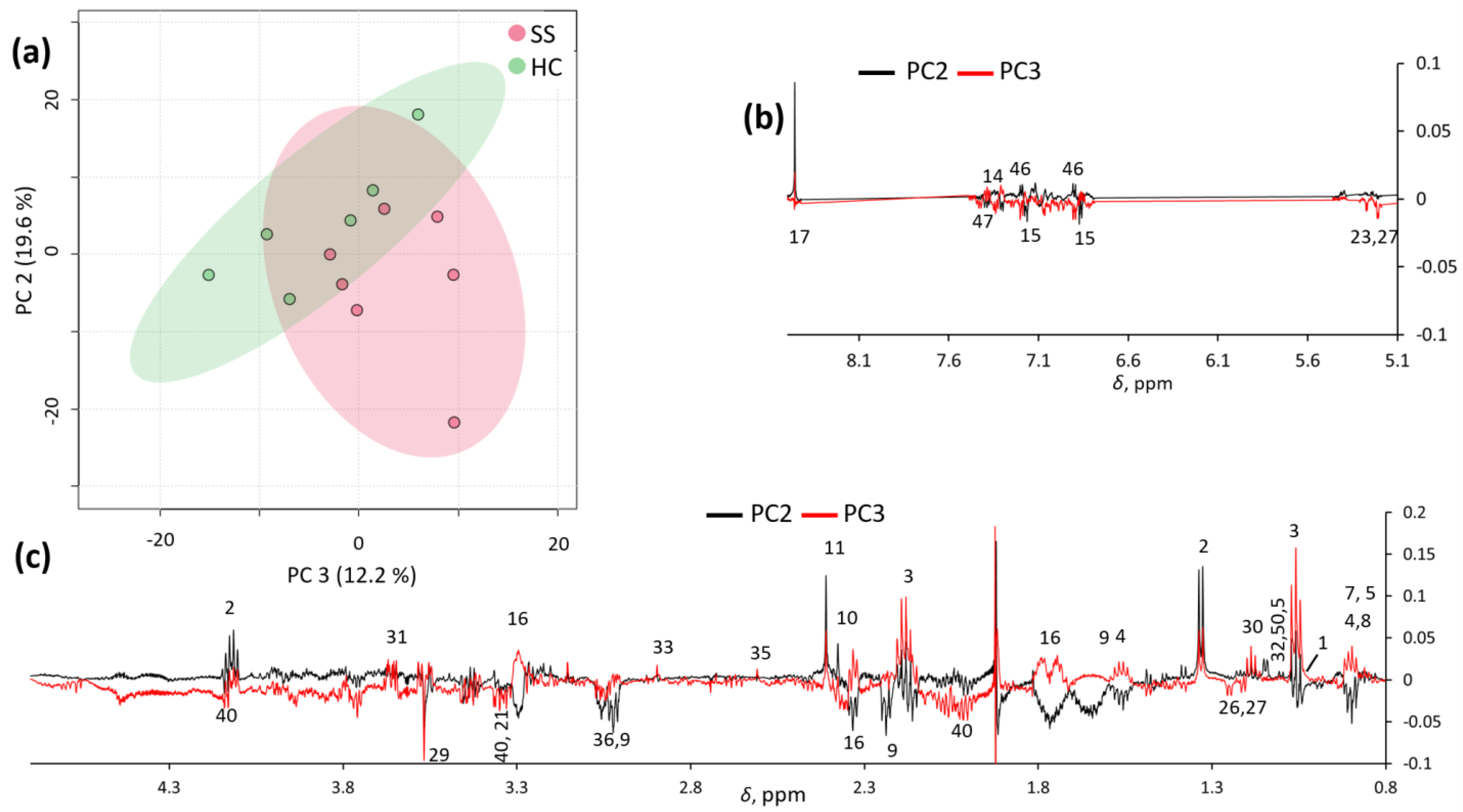
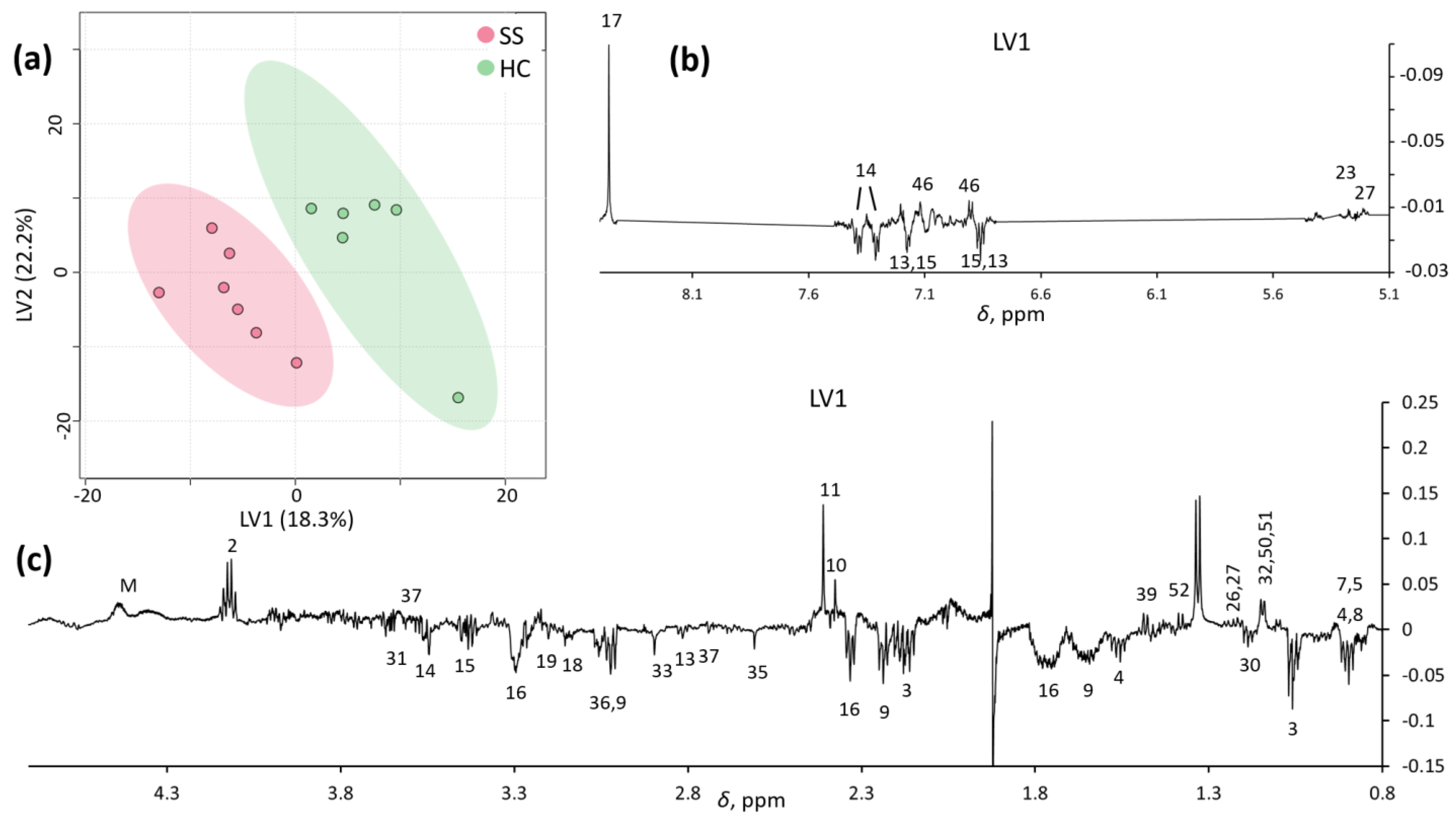
Metabolomic and Statistical Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chevet, B.; Chiche, L.Y.; Devauchelle-Pensec, V.; Cornec, D.Y.K. How rare is primary Sjogren’s syndrome? Jt. Bone Spine 2023, 90, 105480. [Google Scholar] [CrossRef]
- Ebert, E.C. Gastrointestinal and hepatic manifestations of Sjogren syndrome. J. Clin. Gastroenterol. 2012, 46, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Konttinen, Y.T.; Kasna-Ronkainen, L. Sjögren’s syndrome: Viewpoint on pathogenesis. Scand. J. Rheumatol. 2002, 31, 15–27. [Google Scholar] [CrossRef]
- Parisis, D.; Chivasso, C.; Perret, J.; Soyfoo, M.S.; Delporte, C. Current State of Knowledge on Primary Sjogren’s Syndrome, an Autoimmune Exocrinopathy. J. Clin. Med. 2020, 9, 2299. [Google Scholar] [CrossRef] [PubMed]
- Haldorsen, K.; Moen, K.; Jacobsen, H.; Jonsson, R.; Brun, J.G. Exocrine function in primary Sjogren syndrome: Natural course and prognostic factors. Ann. Rheum. Dis. 2008, 67, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.G.; Singh, S.; Matteson, E.L. Rate, risk factors and causes of mortality in patients with Sjogren’s syndrome: A systematic review and meta-analysis of cohort studies. Rheumatology 2016, 55, 450–460. [Google Scholar] [CrossRef]
- Ramirez Sepulveda, J.I.; Kvarnstrom, M.; Eriksson, P.; Mandl, T.; Norheim, K.B.; Johnsen, S.J.; Hammenfors, D.; Jonsson, M.V.; Skarstein, K.; Brun, J.G.; et al. Long-term follow-up in primary Sjogren’s syndrome reveals differences in clinical presentation between female and male patients. Biol. Sex Differ. 2017, 8, 25. [Google Scholar] [CrossRef]
- Jonsson, R.; Brokstad, K.A.; Jonsson, M.V.; Delaleu, N.; Skarstein, K. Current concepts on Sjogren’s syndrome—Classification criteria and biomarkers. Eur. J. Oral Sci. 2018, 126 (Suppl. 1), 37–48. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjogren’s syndrome: A consensus and data-driven methodology involving three international patient cohorts. Ann. Rheum. Dis. 2017, 76, 9–16. [Google Scholar] [CrossRef]
- de Almeida Pdel, V.; Gregio, A.M.; Machado, M.A.; de Lima, A.A.; Azevedo, L.R. Saliva composition and functions: A comprehensive review. J. Contemp. Dent. Pract. 2008, 9, 72–80. [Google Scholar] [PubMed]
- Meleti, M.; Quartieri, E.; Antonelli, R.; Pezzi, M.E.; Ghezzi, B.; Viani, M.V.; Setti, G.; Casali, E.; Ferrari, E.; Ciociola, T.; et al. Metabolic Profiles of Whole, Parotid and Submandibular/Sublingual Saliva. Metabolites 2020, 10, 318. [Google Scholar] [CrossRef]
- Setti, G.; Pezzi, M.E.; Viani, M.V.; Pertinhez, T.A.; Cassi, D.; Magnoni, C.; Bellini, P.; Musolino, A.; Vescovi, P.; Meleti, M. Salivary MicroRNA for Diagnosis of Cancer and Systemic Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 907. [Google Scholar] [CrossRef]
- Meleti, M.; Cassi, D.; Vescovi, P.; Setti, G.; Pertinhez, T.A.; Pezzi, M.E. Salivary biomarkers for diagnosis of systemic diseases and malignant tumors. A systematic review. Med. Oral Patol. Oral Cir. Bucal 2020, 25, e299–e310. [Google Scholar] [CrossRef] [PubMed]
- Baldini, C.; Giusti, L.; Ciregia, F.; Da Valle, Y.; Giacomelli, C.; Donadio, E.; Sernissi, F.; Bazzichi, L.; Giannaccini, G.; Bombardieri, S.; et al. Proteomic analysis of saliva: A unique tool to distinguish primary Sjogren’s syndrome from secondary Sjogren’s syndrome and other sicca syndromes. Arthritis Res. Ther. 2011, 13, R194. [Google Scholar] [CrossRef]
- Hu, S.; Wang, J.; Meijer, J.; Ieong, S.; Xie, Y.; Yu, T.; Zhou, H.; Henry, S.; Vissink, A.; Pijpe, J.; et al. Salivary proteomic and genomic biomarkers for primary Sjogren’s syndrome. Arthritis Rheum. 2007, 56, 3588–3600. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, G.; Saegusa, J.; Irino, Y.; Tanaka, S.; Tsuda, K.; Takahashi, S.; Sendo, S.; Morinobu, A. Metabolomics analysis of saliva from patients with primary Sjogren’s syndrome. Clin. Exp. Immunol. 2015, 182, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Mu, Y.; Guo, C.; You, X.; Liu, X.; Li, Q.; Sun, W. Analysis of the saliva metabolic signature in patients with primary Sjogren’s syndrome. PLoS ONE 2022, 17, e0269275. [Google Scholar] [CrossRef] [PubMed]
- Herrala, M.; Mikkonen, J.J.W.; Pesonen, P.; Lappalainen, R.; Tjaderhane, L.; Niemela, R.K.; Seitsalo, H.; Salo, T.; Myllymaa, S.; Kullaa, A.M. Variability of salivary metabolite levels in patients with Sjogren’s syndrome. J. Oral Sci. 2020, 63, 22–26. [Google Scholar] [CrossRef]
- Mikkonen, J.J.W. Metabolic Profiling of Saliva in Patients with Primary Sjögren’s syndrome. Metabolomics 2012, 3, 128. [Google Scholar] [CrossRef]
- Dame, Z.T.; Aziat, F.; Mandal, R.; Krishnamurthy, R.; Bouatra, S.; Borzouie, S.; Guo, A.C.; Sajed, T.; Deng, L.; Lin, H.; et al. The human saliva metabolome. Metabolomics 2015, 11, 1864–1883. [Google Scholar] [CrossRef]
- Emwas, A.H.; Roy, R.; McKay, R.T.; Tenori, L.; Saccenti, E.; Gowda, G.A.N.; Raftery, D.; Alahmari, F.; Jaremko, L.; Jaremko, M.; et al. NMR Spectroscopy for Metabolomics Research. Metabolites 2019, 9, 123. [Google Scholar] [CrossRef]
- Schenetti, L.; Mucci, A.; Parenti, F.; Cagnoli, R.; Righi, V.; Tosi, M.R.; Tugnoli, V. HR-MAS NMR spectroscopy in the characterization of human tissues: Application to healthy gastric mucosa. Concepts Magn. Reson. Part A 2006, 28A, 430–443. [Google Scholar] [CrossRef]
- Daniels, T.E.; Cox, D.; Shiboski, C.H.; Schiodt, M.; Wu, A.; Lanfranchi, H.; Umehara, H.; Zhao, Y.; Challacombe, S.; Lam, M.Y.; et al. Associations between salivary gland histopathologic diagnoses and phenotypic features of Sjogren’s syndrome among 1726 registry participants. Arthritis Rheum. 2011, 63, 2021–2030. [Google Scholar] [CrossRef] [PubMed]
- Scully, C. Chapter 8—Dry mouth (xerostomia and hyposalivation). In Oral and Maxillofacial Medicine, 3rd ed.; Scully, C., Ed.; Churchill Livingstone: London, UK, 2013; pp. 91–97. [Google Scholar]
- Navazesh, M. Methods for collecting saliva. Ann. N. Y. Acad. Sci. 1993, 694, 72–77. [Google Scholar] [CrossRef]
- Gardner, A.; Parkes, H.G.; Carpenter, G.H.; So, P.W. Developing and Standardizing a Protocol for Quantitative Proton Nuclear Magnetic Resonance ((1)H NMR) Spectroscopy of Saliva. J. Proteome Res. 2018, 17, 1521–1531. [Google Scholar] [CrossRef] [PubMed]
- Righi, V.; Reggiani, C.; Tarentini, E.; Mucci, A.; Paganelli, A.; Cesinaro, A.M.; Mataca, E.; Kaleci, S.; Ferrari, B.; Meleti, M.; et al. Metabolomic Analysis of Actinic Keratosis and SCC Suggests a Grade-Independent Model of Squamous Cancerization. Cancers 2021, 13, 5560. [Google Scholar] [CrossRef]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids. Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Russell, M.W. Chapter 15—Innate Humoral Defense Factors. In Mucosal Immunology, 4th ed.; Mestecky, J., Strober, W., Russell, M.W., Kelsall, B.L., Cheroutre, H., Lambrecht, B.N., Eds.; Academic Press: Boston, FL, USA, 2015; pp. 251–270. [Google Scholar]
- Bennick, A. Salivary proline-rich proteins. Mol. Cell. Biochem. 1982, 45, 83–99. [Google Scholar] [CrossRef]
- Azen, E.A.; Maeda, N. Molecular genetics of human salivary proteins and their polymorphisms. Adv. Hum. Genet. 1988, 17, 141–199. [Google Scholar] [CrossRef]
- Marchesi, J.R.; Holmes, E.; Khan, F.; Kochhar, S.; Scanlan, P.; Shanahan, F.; Wilson, I.D.; Wang, Y. Rapid and noninvasive metabonomic characterization of inflammatory bowel disease. J. Proteome Res. 2007, 6, 546–551. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Brito-Zeron, P.; Bombardieri, S.; Bootsma, H.; De Vita, S.; Dorner, T.; Fisher, B.A.; Gottenberg, J.E.; Hernandez-Molina, G.; Kocher, A.; et al. EULAR recommendations for the management of Sjogren’s syndrome with topical and systemic therapies. Ann. Rheum. Dis. 2020, 79, 3–18. [Google Scholar] [CrossRef]
- Lacombe, V.; Lacout, C.; Lozac’h, P.; Ghali, A.; Gury, A.; Lavigne, C.; Urbanski, G. Unstimulated whole saliva flow for diagnosis of primary Sjogren’s syndrome: Time to revisit the threshold? Arthritis Res. Ther. 2020, 22, 38. [Google Scholar] [CrossRef]
- Martinez-Ceballos, M.A.; Aguilera, N.; Garzon-Gonzalez, K.C.; Cajamarca-Baron, J.; Alzate-Granados, J.P.; Rojas-Villarraga, A. Unstimulated whole salivary flow in Sjogren’s Syndrome: Systematic literature review and meta-analysis. Adv. Rheumatol. 2021, 61, 8. [Google Scholar] [CrossRef] [PubMed]
- Lindon, J.C.; Nicholson, J.K.; Holmes, E.; Everett, J.R. Metabonomics: Metabolic processes studied by NMR spectroscopy of biofluids. Concepts Magn. Reson. 2000, 12, 289–320. [Google Scholar] [CrossRef]
- Aimetti, M.; Cacciatore, S.; Graziano, A.; Tenori, L. Metabonomic analysis of saliva reveals generalized chronic periodontitis signature. Metabolomics 2011, 8, 465–474. [Google Scholar] [CrossRef]
- Citterio, F.; Romano, F.; Meoni, G.; Iaderosa, G.; Grossi, S.; Sobrero, A.; Dego, F.; Corana, M.; Berta, G.N.; Tenori, L.; et al. Changes in the Salivary Metabolic Profile of Generalized Periodontitis Patients after Non-surgical Periodontal Therapy: A Metabolomic Analysis Using Nuclear Magnetic Resonance Spectroscopy. J. Clin. Med. 2020, 9, 3977. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Feng, S.; Pow, E.H.; Lam, O.L.; Mai, S.; Wang, H. Organic anion composition of human whole saliva as determined by ion chromatography. Clin. Chim. Acta. 2015, 438, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Klukowska, M.; Goyal, C.R.; Khambe, D.; Cannon, M.; Miner, M.; Gurich, N.; Circello, B.; Huggins, T.; Barker, M.L.; Furnish, C.; et al. Response of chronic gingivitis to hygiene therapy and experimental gingivitis. Clinical, microbiological and metabonomic changes. Am. J. Dent. 2015, 28, 273–284. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Patient | Histological Assessment before Standardization | Focus Score Following Slides Review [23] | Antibodies | Unstimulated SFR Test for Hyposalivation | Schirmer Test | Reported Symptoms |
|---|---|---|---|---|---|---|
| SJ01 | 1 focus | 1, severe | anti-SSA− anti-SSB− ANA− RF+ | negative | negative | xerophthalmia, xerostomia |
| SJ02 | grade 1 | 3, severe | anti-SSA+ anti-SSB− ANA− RF− | negative | negative | xerophthalmia, xerostomia |
| SJ03 | focus score 1+ | 5, severe | anti-SSA+ anti-SSB− ANA− RF− | positive | positive | xerophthalmia, xerostomia |
| SJ04 | 7 clusters, grade 2+ | 5, severe | anti-SSA− anti-SSB− ANA+ RF− | negative | negative | xerophthalmia, xerostomia |
| SJ05 | focus score > 1, grade 4 | 5, severe | anti-SSA+ anti-SSB− ANA− RF− | negative | negative | xerophthalmia, xerostomia |
| SJ06 | grade 1 | 1, severe | anti-SSA+ anti-SSB− ANA+ RF− | negative | negative | xerophthalmia, xerostomia |
| SJ07 | 1 focus | 1, severe | anti-SSA+ anti-SSB+ ANA− RF− | positive | positive | NR |
| PCA | PLS-DA | ||
|---|---|---|---|
| Sjögren’s Syndrome | Healthy Controls | Sjögren’s Syndrome | Healthy Controls |
| 2-methylbutanoic acid | lactic acid | 2-methylbutanoic acid | lactic acid |
| 4-methylpentanoic acid | succinic acid | 4-methylpentanoic acid | succinic acid |
| 3-methylbutanoic acid | pyruvic acid | 3-methylbutanoic acid | pyruvic acid |
| 2-methylpropionicacid | formic acid | 2-methylpropionicacid | formic acid |
| butanoic acid | propylene glycol or unknown 50/51 | butanoic acid | propylene glycol or unknown 50/51 |
| propanoic acid | fucose | propanoic acid | fucose |
| ethanol | galactose | ethanol | galactose |
| glycerol | proline | glycerol | tyrosine |
| 5-aminopentanoic c | glycine | 5-aminopentanoic c | alanine |
| δ-valerolactam | taurine | δ-valerolactam | unknown 52 |
| ethanolamine | phenylalanine | choline | |
| methylamines | ethanolamine | ||
| putrescine | methylamines | ||
| phenylacetic acid | putrescine | ||
| 4-hydroxyphenylacetic acid | sarcosine | ||
| phenylacetic acid | |||
| 4-hydroxyphenylacetic acid | |||
| phloretic acid | |||
| Metabolite | Deconvoluted Signal (ppm) | p-Value * | FC * | p-Value $ | FC $ |
|---|---|---|---|---|---|
| 2-methylbutanoic acid | 0.86 | 0.12 | 2.9 | 0.07 | 2.3 |
| 4-methylpentanoic acid | 0.88 | 0.23 | 2.0 | 0.31 | 2.0 |
| butanoic acid | 0.90 | 0.29 | 2.2 | 0.10 | 1.5 |
| 3-methylbutanoic acid | 0.91 | 0.21 | 2.5 | 0.09 | 2.0 |
| 1.15 ppm | 1.15 | 0.24 | 0.5 | 0.05 | 0.5 |
| ethanol | 1.19 | 0.14 | 1.5 | 0.43 | 1.3 |
| fucose | 1.25 | 0.59 | 0.9 | 0.26 | 0.7 |
| lactic acid | 1.33 | 0.42 | 0.4 | 0.39 | 0.5 |
| alanine | 1.48 | 0.71 | 0.9 | 0.28 | 0.8 |
| acetic acid | 1.92 | 0.66 | 1.2 | 0.26 | 1.1 |
| propanoic acid | 2.19 | 0.88 | 1.1 | 0.56 | 1.1 |
| 5-aminopentanoic acid | 2.24 | 0.37 | 1.9 | 0.23 | 1.3 |
| δ-valerolactam | 2.33 | 0.38 | 3.2 | 0.24 | 1.8 |
| pyruvic acid | 2.38 | 0.34 | 0.5 | 0.33 | 0.7 |
| succinic acid | 2.41 | 0.38 | 0.3 | 0.35 | 0.5 |
| methylamine | 2.61 | 0.01 | 2.3 | 0.05 | 2.3 |
| dimethylamine | 2.73 | 0.90 | 1.0 | 1.00 | 1.0 |
| sarcosine | 2.74 | 0.96 | 1.0 | 0.98 | 1.0 |
| trimethylamine | 2.90 | 0.08 | 3.0 | 0.13 | 2.7 |
| ethanolamine | 3.15 | 0.73 | 0.9 | 0.58 | 1.2 |
| unknown 53 | 3.16 | 0.35 | 2.0 | 0.41 | 1.4 |
| taurine | 3.26 | 0.35 | 1.4 | 0.15 | 1.3 |
| proline | 3.34 | 0.56 | 0.7 | 0.07 | 0.5 |
| phenylacetic acid | 3.54 | 0.42 | 2.4 | 0.35 | 1.6 |
| glycine | 3.56 | 0.72 | 1.3 | 0.67 | 0.8 |
| phloretic acid | 6.85 | 0.14 | 4.0 | 0.07 | 3.1 |
| 4-hydroxyphenylacetic acid | 6.87 | 0.65 | 1.4 | 0.85 | 1.1 |
| tyrosine | 6.90 | 0.67 | 0.8 | 0.64 | 0.9 |
| phenylalanine | 7.42 | 0.64 | 1.2 | 0.38 | 1.3 |
| formate | 8.46 | 0.57 | 0.6 | 0.47 | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Setti, G.; Righi, V.; Mucci, A.; Panari, L.; Bernardelli, G.; Tarentini, E.; Gambini, A.; Consolo, U.; Generali, L.; Magnoni, C.; et al. Metabolic Profile of Whole Unstimulated Saliva in Patients with Sjögren’s Syndrome. Metabolites 2023, 13, 348. https://doi.org/10.3390/metabo13030348
Setti G, Righi V, Mucci A, Panari L, Bernardelli G, Tarentini E, Gambini A, Consolo U, Generali L, Magnoni C, et al. Metabolic Profile of Whole Unstimulated Saliva in Patients with Sjögren’s Syndrome. Metabolites. 2023; 13(3):348. https://doi.org/10.3390/metabo13030348
Chicago/Turabian StyleSetti, Giacomo, Valeria Righi, Adele Mucci, Lucia Panari, Giuditta Bernardelli, Elisabetta Tarentini, Anna Gambini, Ugo Consolo, Luigi Generali, Cristina Magnoni, and et al. 2023. "Metabolic Profile of Whole Unstimulated Saliva in Patients with Sjögren’s Syndrome" Metabolites 13, no. 3: 348. https://doi.org/10.3390/metabo13030348