
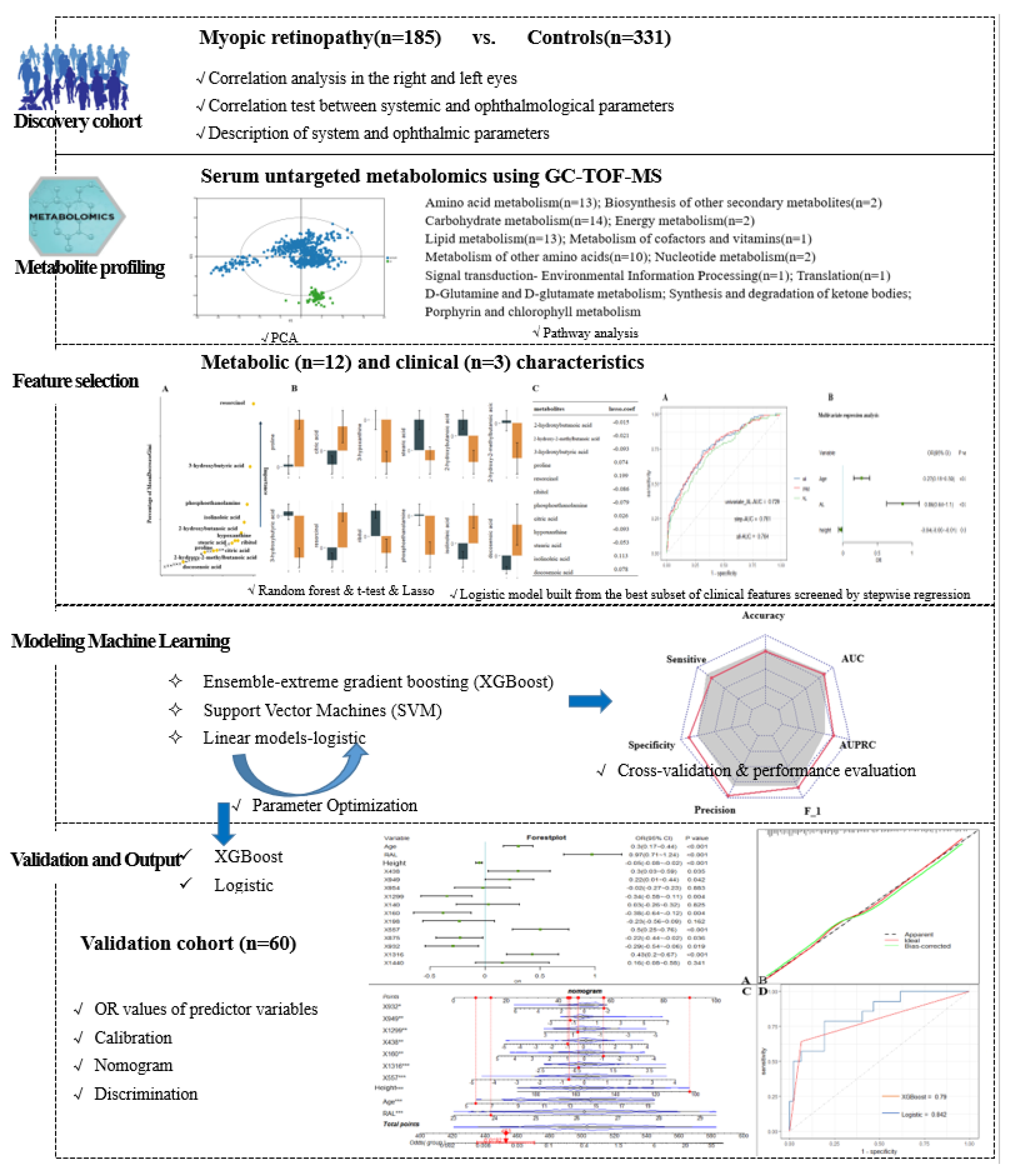
Machine Learning-Based Integration of Metabolomics Characterisation Predicts Progression of Myopic Retinopathy in Children and Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Protocol
2.3. Metabolite Analysis
2.4. Statistical and Data Analyses
3. Results
3.1. Systemic and Ophthalmological Characteristics
3.2. Systemic and Ophthalmological Parameters for Classifying Retinopathy in Training Cohort
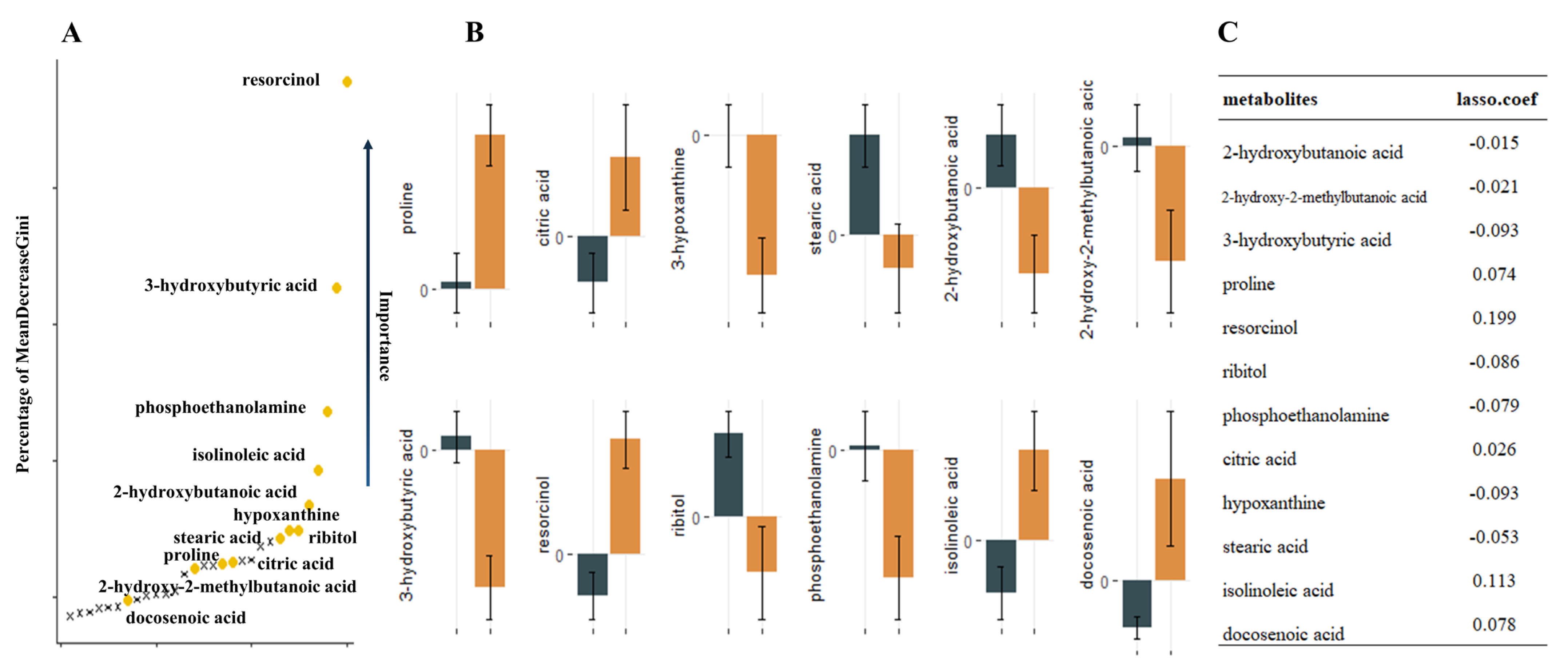
3.3. Identification of Serum Nontargeted Metabolic Profiles and Metabolic Signatures in Myopic Retinopathy
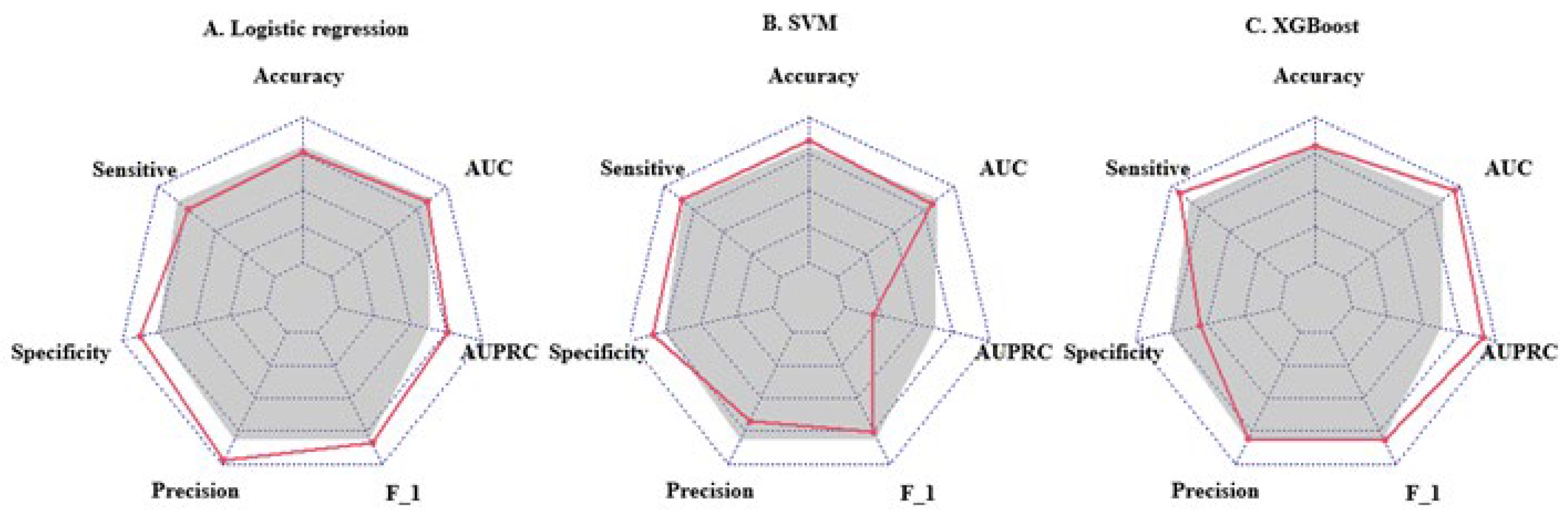
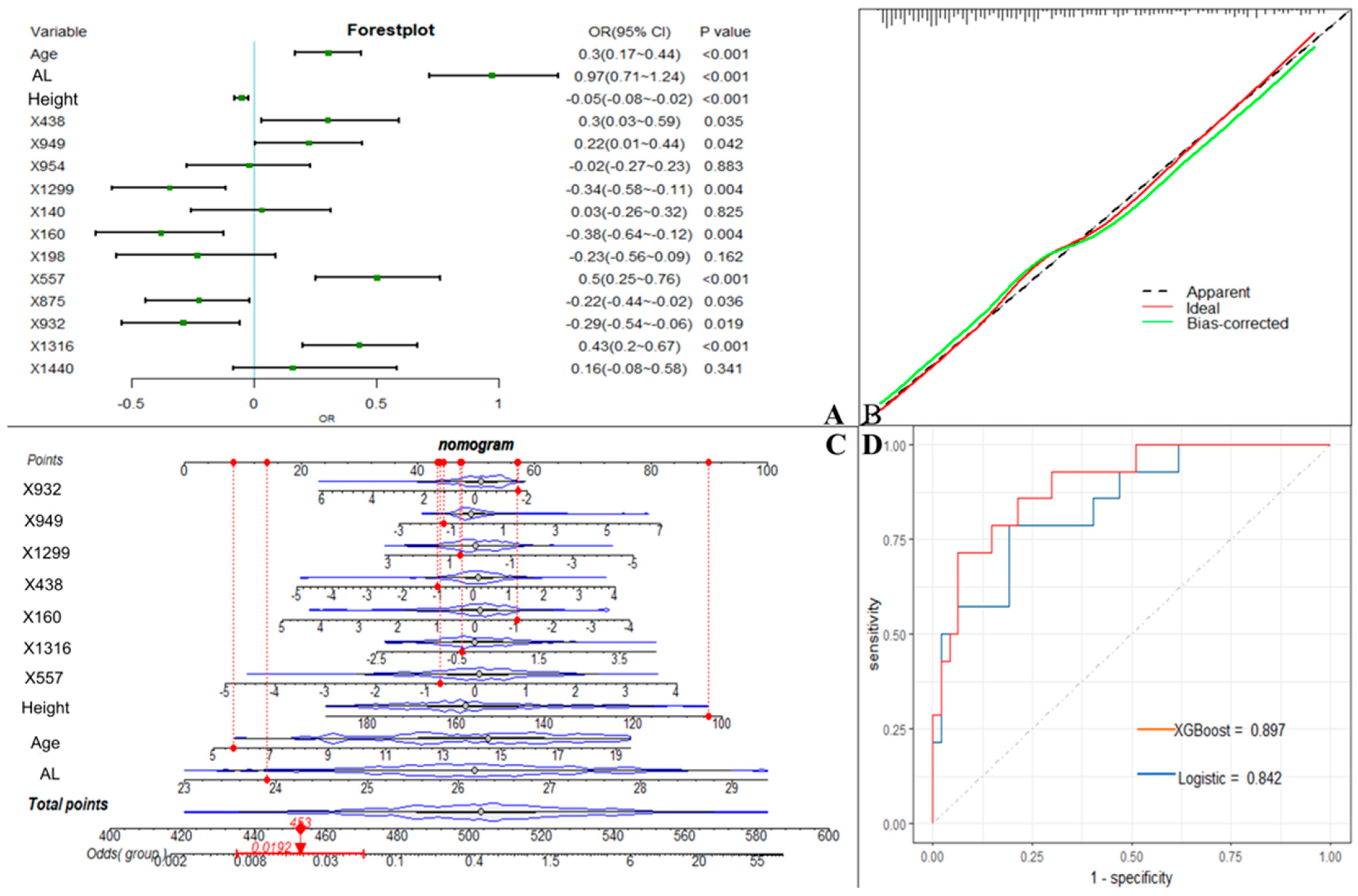
3.4. Machine Learning Disease Prediction Model Based on Metabolic Features and Clinical Data
3.5. Comparison of the Focused Metabolic Profiles with Those of the Myopic Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, L.L.; Shih, Y.F.; Hsiao, C.K.; Chen, C.J. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Ann. Acad. Med. Singap. 2004, 33, 27–33. [Google Scholar] [PubMed]
- Tang, T.; Yu, Z.; Xu, Q.; Peng, Z.; Fan, Y.; Wang, K.; Ren, Q.; Qu, J.; Zhao, M. A machine learning-based algorithm used to estimate the physiological elongation of ocular axial length in myopic children. Eye Vis. (Lond. Engl.) 2020, 7, 50. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.F.; Bi, H.S.; Wang, S.M.; Hu, Y.Y.; Wu, H.; Sun, W.; Lu, T.L.; Wang, X.R.; Jonas, J.B. Refractive error, visual acuity and causes of vision loss in children in Shandong, China. The Shandong Children Eye Study. PLoS ONE 2013, 8, e82763. [Google Scholar] [CrossRef]
- Foo, L.L.; Xu, L.; Sabanayagam, C.; Htoon, H.M.; Ang, M.; Zhang, J.; Ohno-Matsui, K.; Cheng, C.Y.; Hoang, Q.V.; Tan, C.S.; et al. Predictors of myopic macular degeneration in a 12-year longitudinal study of Singapore adults with myopia. Br. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Hayashi, K.; Ohno-Matsui, K.; Shimada, N.; Moriyama, M.; Kojima, A.; Hayashi, W.; Yasuzumi, K.; Nagaoka, N.; Saka, N.; Yoshida, T.; et al. Long-term pattern of progression of myopic maculopathy: A natural history study. Ophthalmology 2010, 117, 1595–1611, 1611.e1–4. [Google Scholar] [CrossRef]
- Ohno-Matsui, K.; Kawasaki, R.; Jonas, J.B.; Cheung, C.M.; Saw, S.M.; Verhoeven, V.J.; Klaver, C.C.; Moriyama, M.; Shinohara, K.; Kawasaki, Y.; et al. International photographic classification and grading system for myopic maculopathy. Am. J. Ophthalmol. 2015, 159, 877–883.e877. [Google Scholar] [CrossRef]
- Dirani, M.; Tong, L.; Gazzard, G.; Zhang, X.; Chia, A.; Young, T.L.; Rose, K.A.; Mitchell, P.; Saw, S.M. Outdoor activity and myopia in Singapore teenage children. Br. J. Ophthalmol. 2009, 93, 997–1000. [Google Scholar] [CrossRef]
- McKnight, C.M.; Sherwin, J.C.; Yazar, S.; Forward, H.; Tan, A.X.; Hewitt, A.W.; Pennell, C.E.; McAllister, I.L.; Young, T.L.; Coroneo, M.T.; et al. Myopia in young adults is inversely related to an objective marker of ocular sun exposure: The Western Australian Raine cohort study. Am. J. Ophthalmol. 2014, 158, 1079–1085. [Google Scholar] [CrossRef] [Green Version]
- Tideman, J.W.; Polling, J.R.; Voortman, T.; Jaddoe, V.W.; Uitterlinden, A.G.; Hofman, A.; Vingerling, J.R.; Franco, O.H.; Klaver, C.C. Low serum vitamin D is associated with axial length and risk of myopia in young children. Eur. J. Epidemiol. 2016, 31, 491–499. [Google Scholar] [CrossRef] [Green Version]
- Williams, K.M.; Bentham, G.C.; Young, I.S.; McGinty, A.; McKay, G.J.; Hogg, R.; Hammond, C.J.; Chakravarthy, U.; Rahu, M.; Seland, J.; et al. Association Between Myopia, Ultraviolet B Radiation Exposure, Serum Vitamin D Concentrations, and Genetic Polymorphisms in Vitamin D Metabolic Pathways in a Multicountry European Study. JAMA Ophthalmol. 2017, 135, 47–53. [Google Scholar] [CrossRef] [Green Version]
- Hou, X.W.; Wang, Y.; Ke, C.F.; Li, M.Y.; Pan, C.W. Metabolomics and Biomarkers in Retinal and Choroidal Vascular Diseases. Metabolites 2022, 12, 814. [Google Scholar] [CrossRef]
- Hou, X.W.; Wang, Y.; Pan, C.W. Metabolomics in Age-Related Macular Degeneration: A Systematic Review. Investig. Ophthalmol. Vis. Sci. 2020, 61, 13. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.W.; Wang, Y.; Pan, C.W. Metabolomics in Diabetic Retinopathy: A Systematic Review. Investig. Ophthalmol. Vis. Sci. 2021, 62, 4. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.W.; Wang, Y.; Ke, C.; Pan, C.W. Metabolomics facilitates the discovery of metabolic profiles and pathways for myopia: A systematic review. Eye (Lond. Engl.) 2022. [Google Scholar] [CrossRef] [PubMed]
- Bogunovic, H.; Montuoro, A.; Baratsits, M.; Karantonis, M.G.; Waldstein, S.M.; Schlanitz, F.; Schmidt-Erfurth, U. Machine Learning of the Progression of Intermediate Age-Related Macular Degeneration Based on OCT Imaging. Investig. Ophthalmol. Vis. Sci. 2017, 58, Bio141–Bio150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hood, D.C.; De Moraes, C.G. Efficacy of a Deep Learning System for Detecting Glaucomatous Optic Neuropathy Based on Color Fundus Photographs. Ophthalmology 2018, 125, 1207–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.S.; Baughman, D.M.; Lee, A.Y. Deep learning is effective for the classification of OCT images of normal versus Age-related Macular Degeneration. Ophthalmol. Retin. 2017, 1, 322–327. [Google Scholar] [CrossRef]
- Lin, H.; Long, E.; Ding, X.; Diao, H.; Chen, Z.; Liu, R.; Huang, J.; Cai, J.; Xu, S.; Zhang, X.; et al. Prediction of myopia development among Chinese school-aged children using refraction data from electronic medical records: A retrospective, multicentre machine learning study. PLoS Med. 2018, 15, e1002674. [Google Scholar] [CrossRef] [Green Version]
- Mao, J.; Luo, Y.; Liu, L.; Lao, J.; Shao, Y.; Zhang, M.; Zhang, C.; Sun, M.; Shen, L. Automated diagnosis and quantitative analysis of plus disease in retinopathy of prematurity based on deep convolutional neural networks. Acta Ophthalmol. 2020, 98, e339–e345. [Google Scholar] [CrossRef]
- Peng, Y.; Dharssi, S.; Chen, Q.; Keenan, T.D.; Agrón, E.; Wong, W.T.; Chew, E.Y.; Lu, Z. DeepSeeNet: A Deep Learning Model for Automated Classification of Patient-based Age-related Macular Degeneration Severity from Color Fundus Photographs. Ophthalmology 2019, 126, 565–575. [Google Scholar] [CrossRef]
- He, X.; Zhao, R.; Sankaridurg, P.; Zhu, J.; Naduvilath, T.; Ma, Y.; Lu, L.; Lv, M.; Smith, E.L., 3rd; Resnikoff, S.; et al. Design and methodology of the Shanghai child and adolescent large-scale eye study (SCALE). Clin. Exp. Ophthalmol. 2018, 46, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Tokoro, T. On the definition of pathologic myopia in group studies. Acta Ophthalmol. Suppl. 1988, 185, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Kind, T.; Wohlgemuth, G.; Lee, D.Y.; Lu, Y.; Palazoglu, M.; Shahbaz, S.; Fiehn, O. FiehnLib: Mass spectral and retention index libraries for metabolomics based on quadrupole and time-of-flight gas chromatography/mass spectrometry. Anal. Chem. 2009, 81, 10038–10048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, W.B.; Broadhurst, D.; Begley, P.; Zelena, E.; Francis-McIntyre, S.; Anderson, N.; Brown, M.; Knowles, J.D.; Halsall, A.; Haselden, J.N.; et al. Procedures for large-scale metabolic profiling of serum and plasma using gas chromatography and liquid chromatography coupled to mass spectrometry. Nat. Protoc. 2011, 6, 1060–1083. [Google Scholar] [CrossRef]
- Jiang, Y.; Wang, Y.; Zhang, J.; Xie, B.; Liao, J.; Liao, W. Outlier detection and robust variable selection via the penalized weighted LAD-LASSO method. J. Appl. Stat. 2021, 48, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Mantero, A.; Ishwaran, H. Unsupervised random forests. Stat. Anal. Data Min. 2021, 14, 144–167. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Usui, Y.; Wakita, R.; Aita, Y.; Tomita, A.; Tsubota, K.; Asakage, M.; Nezu, N.; Komatsu, H.; Umazume, K.; et al. Differential Tissue Metabolic Signatures in IgG4-Related Ophthalmic Disease and Orbital Mucosa-Associated Lymphoid Tissue Lymphoma. Investig. Ophthalmol. Vis. Sci. 2021, 62, 15. [Google Scholar] [CrossRef]
- Subudhi, S.; Verma, A.; Patel, A.B.; Hardin, C.C.; Khandekar, M.J.; Lee, H.; McEvoy, D.; Stylianopoulos, T.; Munn, L.L.; Dutta, S.; et al. Comparing machine learning algorithms for predicting ICU admission and mortality in COVID-19. NPJ Digit. Med. 2021, 4, 87. [Google Scholar] [CrossRef] [PubMed]
- Lei, Z.; Li, J.; Wu, D.; Xia, Y.; Wang, Q.; Si, A.; Wang, K.; Wan, X.; Lau, W.Y.; Wu, M.; et al. Nomogram for Preoperative Estimation of Microvascular Invasion Risk in Hepatitis B Virus-Related Hepatocellular Carcinoma Within the Milan Criteria. JAMA Surg. 2016, 151, 356–363. [Google Scholar] [CrossRef] [Green Version]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Sun, X.; Zhou, X.; Weng, C. Causes and 3-year-incidence of blindness in Jing-An District, Shanghai, China 2001–2009. BMC Ophthalmol. 2011, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, K.; Ohno-Matsui, K.; Kojima, A.; Shimada, N.; Yasuzumi, K.; Yoshida, T.; Futagami, S.; Tokoro, T.; Mochizuki, M. Fundus characteristics of high myopia in children. Jpn. J. Ophthalmol. 2005, 49, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Saw, S.M.; Chua, W.H.; Luu, C.; Cheng, B.; Yeo, I.; Wong, E.; Tan, D.; Koh, A. Optic disk and retinal characteristics in myopic children. Am. J. Ophthalmol. 2004, 138, 160–162. [Google Scholar] [CrossRef] [PubMed]
- Samarawickrama, C.; Mitchell, P.; Tong, L.; Gazzard, G.; Lim, L.; Wong, T.Y.; Saw, S.M. Myopia-related optic disc and retinal changes in adolescent children from singapore. Ophthalmology 2011, 118, 2050–2057. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Cheng, T.; Wang, J.; Zhang, B.; Chen, J.; Zhu, J.; Zou, H.; Liu, K.; He, X.; Xu, X. Role of corneal radius of curvature in early identification of fundus tessellation in children with low myopia. Br. J. Ophthalmol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Xiao, O.; Guo, X.; Wang, D.; Jong, M.; Lee, P.Y.; Chen, L.; Morgan, I.G.; Sankaridurg, P.; He, M. Distribution and Severity of Myopic Maculopathy Among Highly Myopic Eyes. Investig. Ophthalmol. Vis. Sci. 2018, 59, 4880–4885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, T.; Deng, J.; Xu, X.; Zhang, B.; Wang, J.; Xiong, S.; Du, Y.; Yu, S.; Gong, W.; Zhao, H.; et al. Prevalence of fundus tessellation and its associated factors in Chinese children and adolescents with high myopia. Acta Ophthalmol. 2021, 99, e1524–e1533. [Google Scholar] [CrossRef]
- Wong, Y.L.; Ding, Y.; Sabanayagam, C.; Wong, C.W.; Verkicharla, P.; Ohno-Matsui, K.; Tan, D.; Yeo, A.C.; Hoang, Q.V.; Lamoureux, E.; et al. Longitudinal Changes in Disc and Retinal Lesions Among Highly Myopic Adolescents in Singapore Over a 10-Year Period. Eye Contact Lens 2018, 44, 286–291. [Google Scholar] [CrossRef]
- Yan, Y.N.; Wang, Y.X.; Xu, L.; Xu, J.; Wei, W.B.; Jonas, J.B. Fundus Tessellation: Prevalence and Associated Factors: The Beijing Eye Study 2011. Ophthalmology 2015, 122, 1873–1880. [Google Scholar] [CrossRef]
- Yan, Y.N.; Wang, Y.X.; Yang, Y.; Xu, L.; Xu, J.; Wang, Q.; Yang, X.; Yang, J.Y.; Zhou, W.J.; Wei, W.B.; et al. Long-term Progression and Risk Factors of Fundus Tessellation in the Beijing Eye Study. Sci. Rep. 2018, 8, 10625. [Google Scholar] [CrossRef] [Green Version]
- Yokoi, T.; Jonas, J.B.; Shimada, N.; Nagaoka, N.; Moriyama, M.; Yoshida, T.; Ohno-Matsui, K. Peripapillary Diffuse Chorioretinal Atrophy in Children as a Sign of Eventual Pathologic Myopia in Adults. Ophthalmology 2016, 123, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.N.; Wang, Y.X.; Yang, Y.; Xu, L.; Xu, J.; Wang, Q.; Yang, J.Y.; Yang, X.; Zhou, W.J.; Ohno-Matsui, K.; et al. Ten-Year Progression of Myopic Maculopathy: The Beijing Eye Study 2001–2011. Ophthalmology 2018, 125, 1253–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Chen, Q.; Fan, Y.; Zhu, J.; He, J.; Zou, H.; Sun, D.; Xin, B.; Feng, D.; Fulham, M.; et al. Automatic identification of myopic maculopathy related imaging features in optic disc region via machine learning methods. J. Transl. Med. 2021, 19, 167. [Google Scholar] [CrossRef] [PubMed]
- Haarman, A.E.G.; Tedja, M.S.; Brussee, C.; Enthoven, C.A.; van Rijn, G.A.; Vingerling, J.R.; Keunen, J.E.E.; Boon, C.J.F.; Geerards, A.J.M.; Luyten, G.P.M.; et al. Prevalence of Myopic Macular Features in Dutch Individuals of European Ancestry With High Myopia. JAMA Ophthalmol. 2022, 140, 115–123. [Google Scholar] [CrossRef]
- Hopf, S.; Korb, C.; Nickels, S.; Schulz, A.; Münzel, T.; Wild, P.S.; Michal, M.; Schmidtmann, I.; Lackner, K.J.; Pfeiffer, N.; et al. Prevalence of myopic maculopathy in the German population: Results from the Gutenberg health study. Br. J. Ophthalmol. 2020, 104, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Liu, L.; Zheng, D.; Duan, J.; Wang, Y.; Jonas, J.B.; Tian, F.; Wang, S.; Sang, Y.; Zhang, X.; et al. Prevalence and Associations of Fundus Tessellation Among Junior Students From Greater Beijing. Investig. Ophthalmol. Vis. Sci. 2019, 60, 4033–4040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klau, S.; Jurinovic, V.; Hornung, R.; Herold, T.; Boulesteix, A.L. Priority-Lasso: A simple hierarchical approach to the prediction of clinical outcome using multi-omics data. BMC Bioinform. 2018, 19, 322. [Google Scholar] [CrossRef]
- Najjar, R.P.; Chao De La Barca, J.M.; Barathi, V.A.; Ho, C.E.H.; Lock, J.Z.; Muralidharan, A.R.; Tan, R.K.Y.; Dhand, C.; Lakshminarayanan, R.; Reynier, P.; et al. Ocular growth and metabolomics are dependent upon the spectral content of ambient white light. Sci. Rep. 2021, 11, 7586. [Google Scholar] [CrossRef]
- Datta, S.; Cano, M.; Ebrahimi, K.; Wang, L.; Handa, J.T. The impact of oxidative stress and inflammation on RPE degeneration in non-neovascular AMD. Prog. Retin. Eye Res. 2017, 60, 201–218. [Google Scholar] [CrossRef] [PubMed]
- Szabados, L.; Savouré, A. Proline: A multifunctional amino acid. Trends Plant Sci. 2010, 15, 89–97. [Google Scholar] [CrossRef]
- Ke, C.; Xu, H.; Chen, Q.; Zhong, H.; Pan, C.W. Serum metabolic signatures of high myopia among older Chinese adults. Eye (Lond. Engl.) 2021, 35, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Ribelayga, C.; Mangel, S.C. A circadian clock and light/dark adaptation differentially regulate adenosine in the mammalian retina. J. Neurosci. Off. J. Soc. Neurosci. 2005, 25, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trier, K.; Munk Ribel-Madsen, S.; Cui, D.; Brøgger Christensen, S. Systemic 7-methylxanthine in retarding axial eye growth and myopia progression: A 36-month pilot study. J. Ocul. Biol. Dis. Inform. 2008, 1, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Meng, Y.F.; Xing, Q.; Tao, J.J.; Lu, J.; Wu, Y. Identification of lncRNAs involved in biological regulation in early age-related macular degeneration. Int. J. Nanomed. 2017, 12, 7589–7602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichenbach, A.; Bringmann, A. Purinergic signaling in retinal degeneration and regeneration. Neuropharmacology 2016, 104, 194–211. [Google Scholar] [CrossRef]
- Lin, W.J.; Chen, J.J. Class-imbalanced classifiers for high-dimensional data. Brief. Bioinform. 2013, 14, 13–26. [Google Scholar] [CrossRef] [Green Version]
- Blagus, R.; Lusa, L. Class prediction for high-dimensional class-imbalanced data. BMC Bioinform. 2010, 11, 523. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | %Missing | Training Set (n = 516) | Validation Set (n = 60) | %Missing |
|---|---|---|---|---|
| Age, years | 14.20 ± 3.07 | 12.95 ± 3.05 | ||
| height, cm | 155.20 ± 16.20 | 151.03 ± 19.91 | ||
| weight, kg | 50.00 (39.77, 60.40) | 48.30 (31.73, 56.23) | ||
| Body mass index, kg/ | 19.70 (17.73, 22.64) | 19.70 (17.53, 22.11) | ||
| Axial length, mm | 26.21 ± 1.15 | 25.60 (25.12, 26.73) | ||
| Anterior chamber depth, mm | 18.99 | 3.80 ± 0.22 | 3.81 ± 0.23 | |
| Central corneal thickness, um | 18.80 | 540.00 (518.00, 563.50) | 536.90 ± 35.37 | |
| Lens thickness, mm | 22.29 | 3.37 (3.28, 3.48) | 3.34 ± 0.16 | 40.00 |
| spherical power, diopters | −6.00 (−7.00, −5.25) | −5.25 (−6.31, −3.94) | ||
| cylindrical power, diopters | −1.25 (−2.25, −0.75) | −0.75 (−1.50, −0.50) | ||
| Spherical equivalent, diopters | −6.88 (−8.13, −5.88) | −6.06 (−7.25, −4.34) | ||
| Mean radius of curvature, mm | 7.77 ± 0.26 | 7.80 ± 0.25 | ||
| Pupil distance, mm | 60.00 (57.00, 63.00) | 60.10 ± 4.27 | ||
| Female (%) | 267 (51.74) | 29 (48.33) | ||
| Macular lesions (%) | 185 (35.85) | 13 (21.67) | ||
| Fundus tessellation (FT) (%) | 153 (29.88) | 12 (20.00) | ||
| Diffuse chorioretinal atrophy (%) | 32 (0.63) | 1 (1.67) | ||
| High myopia (%) | 135 (26.16) | 12 (20.00) |
| Characteristic | Controls (n = 331) | Myopic Retinopathy (n = 185) | H/t | p |
|---|---|---|---|---|
| Age, years | 13.34 (11.62, 15.78) | 15.97 (13.63, 17.65) | 47.990 | <0.001 |
| height, cm | 155.00 (142.00, 163.00) | 162.25 (154.00, 170.50) | 33.600 | <0.001 |
| weight, kg | 46.40 (35.45, 57.20) | 53.80 (47.10, 64.10) | 31.128 | <0.001 |
| Body mass index, kg/ | 19.14 (17.22, 22.38) | 20.26 (18.73, 23.26) | 15.349 | <0.001 |
| Axial length, mm | 25.87 ± 1.03 | 26.82 ± 1.10 | −9.567 | <0.001 |
| Anterior chamber depth, mm | 3.81 ± 0.21 | 3.80 ± 0.24 | 0.310 | 0.757 |
| Central corneal thickness | 538.50 (518.00, 563.00) | 543.00 (519.00, 564.00) | 0.660 | 0.417 |
| Lens thickness, mm | 3.36 (3.28, 3.47) | 3.38 (3.28, 3.50) | 0.484 | 0.487 |
| spherical power, diopters | −5.75 (−6.50, −4.75) | −6.75 (−8.00, −5.75) | 55.802 | <0.001 |
| cylindrical power, diopters | −1.25 (−2.25, −0.75) | −1.50 (−2.25, −1.00) | 2.824 | 0.093 |
| Spherical equivalent, diopters | −6.50 (−7.56, −5.50) | −7.63 (−8.88, −6.50) | 47.867 | <0.001 |
| Mean radius of curvature, mm | 7.73 ± 0.24 | 7.83 ± 0.26 | −4.240 | <0.001 |
| Pupil distance, mm | 59.00 (56.00, 62.00) | 61.00 (58.00, 63.00) | 22.035 | <0.001 |
| Female% | 179 (54.08) | 88 (47.57) | 1.763 | 0.184 |
| Male% | 152 (45.92) | 97 (52.43) | ||
| Mild to moderate myopia% | 272 (71.39) | 109 (28.61) | 32.033 | <0.001 |
| High myopia% | 59 (43.70) | 76 (56.30) |
| Metabolite | Citric Acid ↑ | Proline ↑ | Hypoxanthine ↓ | Stearic Acid ↓ |
|---|---|---|---|---|
| Hit | Ke (2020) | Najjar (2021) | Liu (2020) | Liu (2020) |
| Case | 40 HM | 18 chicks with monocular FD (BEW light) | 57 PM | |
| Control | 40 mild myopes | 18 chicks with monocular FD (3900 K SW LED light) | 81 cataract patients | |
| Age (case) | ≥60 | - | 55.32 ± 14.49 | |
| Age (control) | match | - | 65.83 ± 11.94 | |
| Patients vs. Controls | Increased | Increased | Decreased | Increased |
| Biofluid | Serum | vitreous and retinas | Serum | Serum |
| Technique Employed | GC-TOF-MS | LC-MS | GC-TOF-MS | |
| Evaluation standard | PLS-DA (VIP > 1.0) and t-test (p < 0.05) | PLS-DA and OPLS-DA | OPLS-DA (VIP > 1.0), t-test (p < 0.05), and FC > 1.2 or <0.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, X.-W.; Yang, J.-L.-X.; Li, D.-L.; Tao, Y.-J.; Ke, C.-F.; Zhang, B.; Liu, S.; Cheng, T.-Y.; Wang, T.-X.; Xu, X.; et al. Machine Learning-Based Integration of Metabolomics Characterisation Predicts Progression of Myopic Retinopathy in Children and Adolescents. Metabolites 2023, 13, 301. https://doi.org/10.3390/metabo13020301
Hou X-W, Yang J-L-X, Li D-L, Tao Y-J, Ke C-F, Zhang B, Liu S, Cheng T-Y, Wang T-X, Xu X, et al. Machine Learning-Based Integration of Metabolomics Characterisation Predicts Progression of Myopic Retinopathy in Children and Adolescents. Metabolites. 2023; 13(2):301. https://doi.org/10.3390/metabo13020301
Chicago/Turabian StyleHou, Xiao-Wen, Jin-Liu-Xing Yang, Dan-Lin Li, Yi-Jin Tao, Chao-Fu Ke, Bo Zhang, Shang Liu, Tian-Yu Cheng, Tian-Xiao Wang, Xun Xu, and et al. 2023. "Machine Learning-Based Integration of Metabolomics Characterisation Predicts Progression of Myopic Retinopathy in Children and Adolescents" Metabolites 13, no. 2: 301. https://doi.org/10.3390/metabo13020301