
Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
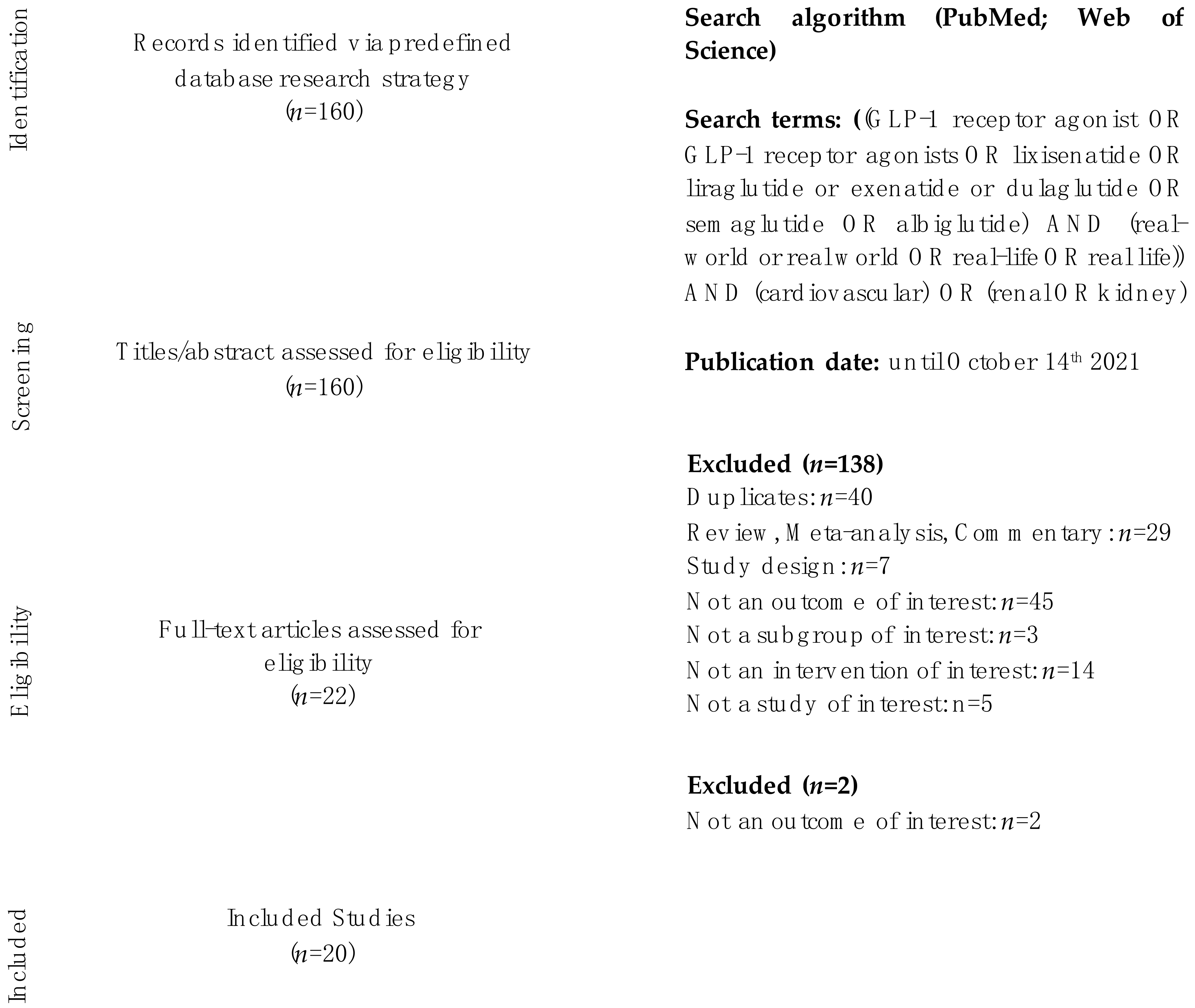
2. Materials and Methods
3. Results
3.1. Glucagon-like Peptide-1 Receptor Agonists (GLP-1RA) and Cardiovascular Outcomes in Real-World Studies
3.1.1. Atherosclerosis and Cardiovascular Risk Factors
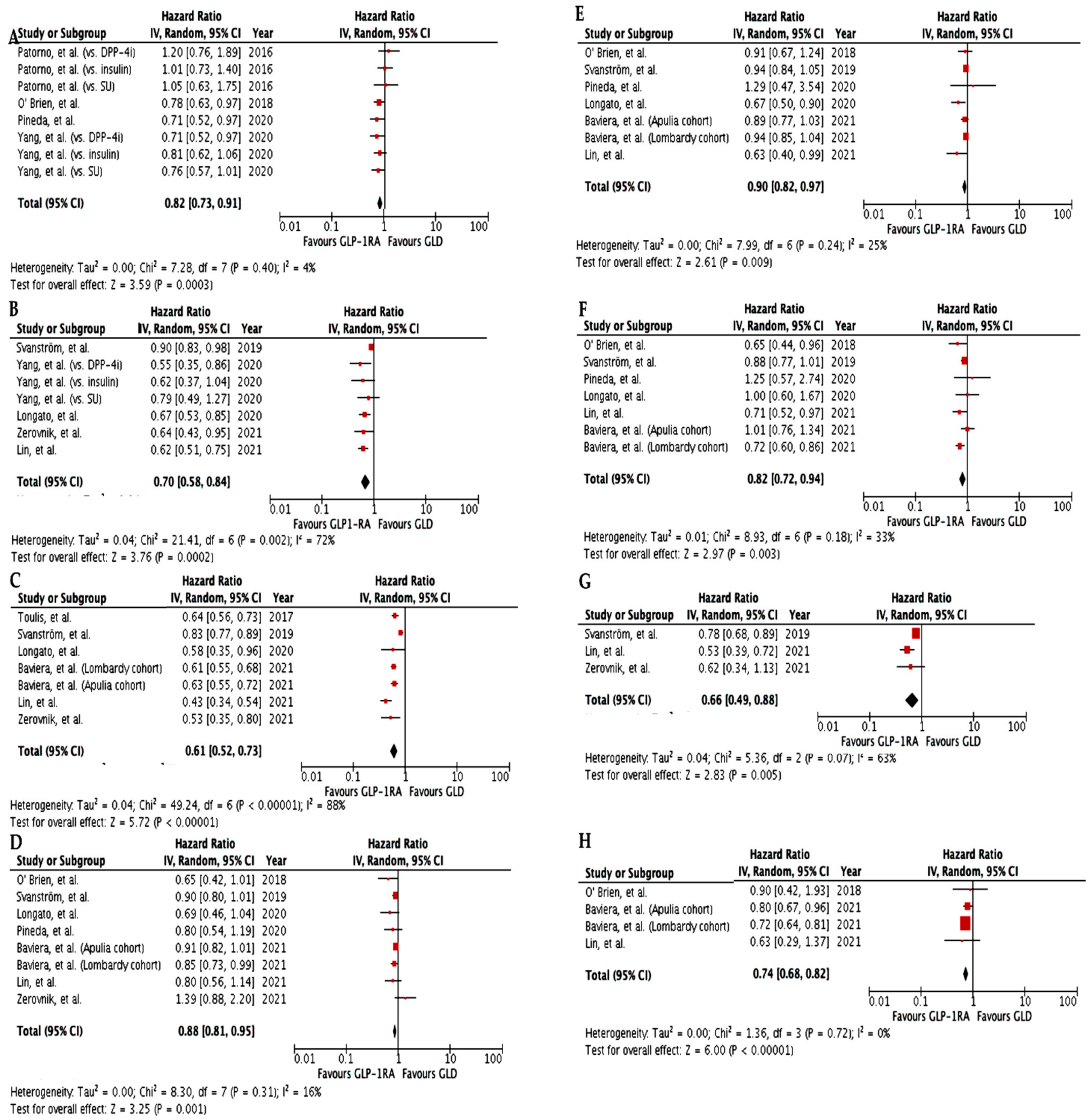
3.1.2. Cardiovascular Outcomes in Real-World Studies Comparing Patients Initiating Glucagon-like Peptide-1 Receptor Agonists (GLP-1RA) vs. Conventional Glucose-Lowering Drugs
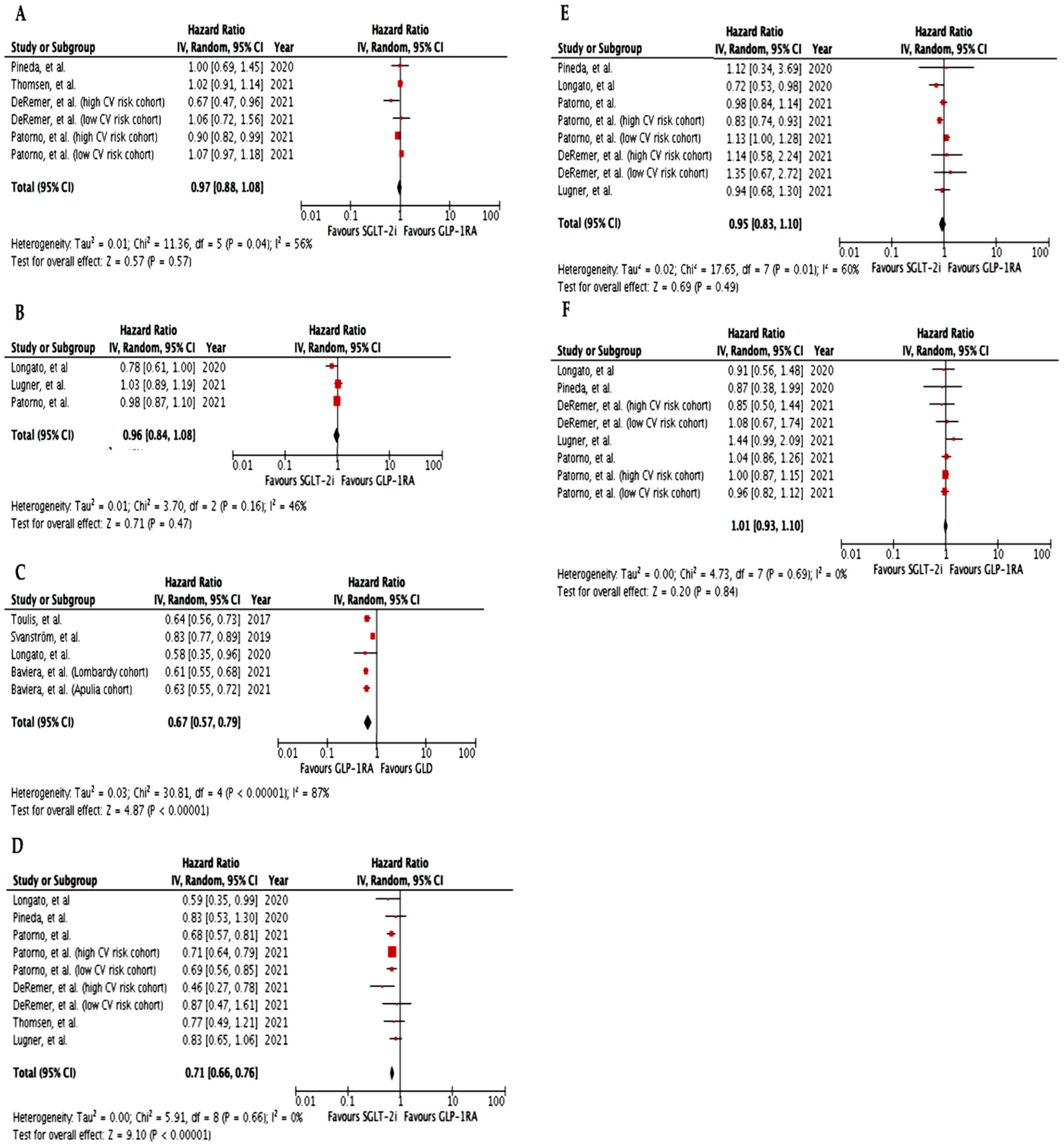
3.1.3. Cardiovascular Outcomes in Real-World Studies Comparing Patients Initiating Glucagon-like Peptide-1 Receptor Agonists (GLP-1RA) vs. Sodium-Glucose Transporter-2 Inhibitors (SGLT-2i)
3.2. Glucagon-like Peptide-1 Receptor Agonists (GLP-1RA) and Renal Outcomes in Real-World Studies
4. Discussion
5. Conclusions
Future Perspectives
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Mol, P.G.M.; Thompson, A.; Heerspink, H.J.L.; Leufkens, H.G.M. Precision medicine in diabetes and diabetic kidney disease: Regulatory considerations. Diabetes Obes. Metab. 2018, 20, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Seeger, J.D.; Nunes, A.; Loughlin, A.M. Using RWE research to extend clinical trials in diabetes: An example with implications for the future. Diabetes Obes. Metab. 2020, 22, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Sciannameo, V.; Berchialla, P.; Orsi, E.; Lamacchia, O.; Morano, S.; Querci, F.; Consoli, A.; Avogaro, A.; Fadini, G.P. The DARWIN-T2D study Enrolment criteria for diabetes cardiovascular outcome trials do not inform on generalizability to clinical practice: The case of glucagon-like peptide-1 receptor agonists. Diabetes Obes. Metab. 2020, 22, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Morieri, M.L.; Avogaro, A.; Fadini, G.P. Long-Acting Injectable GLP-1 Receptor Agonists for the Treatment of Adults with Type 2 Diabetes: Perspectives from Clinical Practice. Diabetes Metab. Syndr. Obesity Targets Ther. 2020, 13, 4221–4234. [Google Scholar] [CrossRef] [PubMed]
- Bray, J.J.H.; Foster-Davies, H.; Salem, A.; Hoole, A.L.; Obaid, D.R.; Halcox, J.P.J.; Stephens, J.W. Glucagon-like peptide-1 receptor agonists improve biomarkers of inflammation and oxidative stress: A systematic review and meta-analysis of randomised controlled trials. Diabetes Obes. Metab. 2021, 23, 1806–1822. [Google Scholar] [CrossRef] [PubMed]
- Giorgino, F.; Caruso, I.; Moellmann, J.; Lehrke, M. Differential indication for SGLT-2 inhibitors versus GLP-1 receptor agonists in patients with established atherosclerotic heart disease or at risk for congestive heart failure. Metabolism 2019, 104, 154045. [Google Scholar] [CrossRef] [PubMed]
- Anholm, C.; Kumarathurai, P.; Pedersen, L.R.; Samkani, A.; Walzem, R.L.; Nielsen, O.W.; Kristiansen, O.P.; Fenger, M.; Madsbad, S.; Sajadieh, A.; et al. Liraglutide in combination with metformin may improve the atherogenic lipid profile and decrease C-reactive protein level in statin treated obese patients with coronary artery disease and newly diagnosed type 2 diabetes: A randomized trial. Atherosclerosis 2019, 288, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, E.; Waller, H.L.; Sargeant, J.A.; Webb, M.A.; Htike, Z.Z.; McCann, G.P.; Gulsin, G.; Khunti, K.; Yates, T.; Henson, J.; et al. Effects of liraglutide versus sitagliptin on circulating cardiovascular biomarkers, including circulating progenitor cells, in individuals with type 2 diabetes and obesity: Analyses from the LYDIA trial. Diabetes Obes. Metab. 2021, 23, 1409–1414. [Google Scholar] [CrossRef]
- Ussher, J.R.; Greenwell, A.A.; Nguyen, M.; Mulvihill, E.E. Cardiovascular Effects of Incretin-Based Therapies: Integrating Mechanisms With Cardiovascular Outcome Trials. Diabetes 2022, 71, 173–183. [Google Scholar] [CrossRef]
- Rizzo, M.; Rizvi, A.A.; Patti, A.M.; Nikolic, D.; Giglio, R.V.; Castellino, G.; Li Volti, G.; Caprio, M.; Montalto, G.; Provenzano, V.; et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: An 18-month prospective study. Cardiovasc. Diabetol. 2016, 15, 162. [Google Scholar] [CrossRef] [Green Version]
- Nikolic, D.; Giglio, R.V.; Rizvi, A.A.; Patti, A.M.; Montalto, G.; Maranta, F.; Cianflone, D.; Stoian, A.P.; Rizzo, M. Liraglutide Reduces Carotid Intima-Media Thickness by Reducing Small Dense Low-Density Lipoproteins in a Real-World Setting of Patients with Type 2 Diabetes: A Novel Anti-Atherogenic Effect. Diabetes Ther. 2020, 12, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Frison, V.; Simioni, N.; Marangoni, A.; Balzano, S.; Vinci, C.; Zenari, L.; De Moliner, L.; Tadiotto, F.; D’Ambrosio, M.; Confortin, L.; et al. Clinical Impact of 5 Years of Liraglutide Treatment on Cardiovascular Risk Factors in Patients with Type 2 Diabetes Mellitus in a Real-Life Setting in Italy: An Observational Study. Diabetes Ther. 2018, 9, 2201–2208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciresi, A.; Vigneri, E.; Radellini, S.; Pantò, F.; Giordano, C. Liraglutide Improves Cardiovascular Risk as an Add-on to Metformin and Not to Insulin Secretagogues in Type 2 Diabetic Patients: A Real-life 48-Month Retrospective Study. Diabetes Ther. 2017, 9, 363–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirani, M.; Favacchio, G.; Serone, E.; Lucisano, G.; Rossi, M.C.; Berra, C.C. Liraglutide and cardiovascular outcomes in a real world type 2 diabetes cohort. Pharmacol. Res. 2018, 137, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Brixner, D.I.; McAdam-Marx, C.; Ye, X.; Boye, K.S.; Nielsen, L.L.; Wintle, M.; Misurski, D.; Fabunmi, R. Six-month outcomes on A1C and cardiovascular risk factors in patients with type 2 diabetes treated with exenatide in an ambulatory care setting. Diabetes Obes. Metab. 2009, 11, 1122–1130. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Lee, M.M.Y.; Kristensen, S.L.; Branch, K.R.H.; Del Prato, S.; Khurmi, N.S.; Lam, C.S.P.; Lopes, R.D.; McMurray, J.J.V.; Pratley, R.E.; et al. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of randomised trials. Lancet Diabetes Endocrinol. 2021, 9, 653–662. [Google Scholar] [CrossRef]
- Pineda, E.D.; Lia, I.-C.; Godley, P.J.; Michel, J.B.; Rascati, K. Cardiovascular outcomes among patients with type 2 diabetes newly initiated on sodium-glycose cotransporter-2 inhibitors, glucagon-like peptide-1 receptor agonists, and other antidiabetic medications. J. Manag. Care Spec. Pharm. 2020, 26, 610–618. [Google Scholar]
- Yang, C.-T.; Yang, C.-Y.; Ou, H.-T.; Kuo, S. Comparative cardiovascular safety of GLP-1 receptor agonists versus other glucose-lowering agents in real-world patients with type 2 diabetes: A nationwide population-based cohort study. Cardiovasc. Diabetol. 2020, 19, 83. [Google Scholar] [CrossRef]
- O’Brien, M.J.; Karam, S.L.; Wallia, A.; Kang, R.H.; Cooper, A.J.; Lancki, N.; Moran, M.R.; Liss, D.T.; Prospect, T.A.; Ackermann, R.T. Association of second-line antidiabetic medications with cardiovascular events among insured adults with type 2 diabetes. JAMA Netw. Open 2018, 1, e186125. [Google Scholar] [CrossRef]
- Patorno, E.; Everett, B.M.; Goldfine, A.B.; Glynn, R.J.; Liu, J.; Gopalakrishnan, C.; Kim, S.C. Comparative cardiovascular safety of glucagon-like peptide-1 receptor agonists versus other antidiabetic drugs in routine care: A cohort study. Diabetes Obes. Metab. 2016, 18, 755–765. [Google Scholar] [CrossRef]
- Longato, E.; Di Camillo, B.; Sparacino, G.; Tramontan, L.; Avogaro, A.; Fadini, G.P. Better cardiovascular outcomes of type 2 diabetic patients treated with GLP-1 receptor agonists versus DPP-4 inhibitors in clinical practice. Cardiovasc. Diabetol. 2020, 19, 74. [Google Scholar] [CrossRef] [PubMed]
- Svanström, H.; Ueda, P.; Melbye, M.; Eliasson, B.; Svensson, A.-M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Pasternak, B. Use of liraglutide and risk of major cardiovascular events: A register-based cohort study in Denmark and Sweden. Lancet Diabetes Endocrinol. 2018, 7, 106–114. [Google Scholar] [CrossRef]
- Lin, D.S.-H.; Lee, J.-K.; Chen, W.-J. Major adverse cardiovascular and limb events in patients with diabetes treated with GLP-1 receptor agonists vs DPP-4 inhibitors. Diabetologia 2021, 64, 1949–1962. [Google Scholar] [CrossRef] [PubMed]
- Zerovnik, S.; Kos, M.; Locatelli, I. Cardiovascular morbidity and mortality in patients with type 2 diabetes using novel antidiabetic medicines as add-on therapy: An observational real-world study. BMJ Open 2021, 11, e051549. [Google Scholar] [CrossRef]
- Baviera, M.; Genovese, S.; Lepore, V.; Colacioppo, P.; Robusto, F.; Tettamanti, M.; D’Ettorre, A.; Avanzini, F.; Fortino, I.; Nicolucci, A.; et al. Lower risk of death and cardiovascular events in patients with diabetes initiating glucagon-like peptide-1 receptor agonists or sodium-glucose cotransporter-2 inhibitors: A real-world study in two Italian cohorts. Diabetes Obes. Metab. 2021, 23, 1484–1495. [Google Scholar] [CrossRef]
- Toulis, K.; Hanif, W.; Saravanan, P.; Willis, B.; Marshall, T.; Kumarendran, B.; Gokhale, K.; Ghosh, S.; Cheng, K.; Narendran, P.; et al. All-cause mortality in patients with diabetes under glucagon-like peptide-1 agonists: A population-based, open cohort study. Diabetes Metab. 2017, 43, 211–216. [Google Scholar] [CrossRef]
- Dhatariya, K.; Bain, S.C.; Buse, J.B.; Simpson, R.; Tarnow, L.; Kaltoft, M.S.; Stellfeld, M.; Tornøe, K.; Pratley, R.E.; the LEADER Publication Committee on behalf of the LEADER Trial Investigators. The impact of liraglutide on diabetes-related foot ulceration and associated complications in patients with type 2 diabetes at high risk for cardiovascular events: Results from the LEADER trial. Diabetes Care 2018, 41, 2229–2235. [Google Scholar] [CrossRef] [Green Version]
- Alkhezi, O.S.; Alsuhaibani, H.A.; Alhadyab, A.A.; Alfaifi, M.E.; Alomrani, B.; Aldossary, A.; Alfayez, O.M. Heart failure outcomes and glucagon-like peptide-1 receptor agonists: A systematic review of observational studies. Prim. Care Diabetes 2021, 15, 761–771. [Google Scholar] [CrossRef]
- American Diabetes Association. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44, S111–S124. [Google Scholar] [CrossRef]
- DeRemer, C.E.; Vouri, S.M.; Guo, J.; Donahoo, W.T.; Winterstein, A.G.; Shao, H. Comparing cardiovascular benefits between GLP-1 receptor agonists and SGLT2 inhibitors as an add-on to metformin among patients with type 2 diabetes: A retrospective cohort study. J. Diabetes Compl. 2021, 35, 107972. [Google Scholar] [CrossRef]
- Patorno, E.; Htoo, P.T.; Glynn, S.R.J.; Schneeweiss, S.; Wexler, D.J.; Pawar, A.; Bessette, B.L.G.; Chin, B.K.; Everett, B.M.; Kim, S.C. Sodium–Glucose Cotransporter-2 inhibitors versus Glucagon-like Peptide-1 receptor Agonists and the risk for cardiovascular outcomes in routine care patients with diabetes across categories of cardiovascular disease. Ann. Intern. Med. 2021, 174, 1528–1541. [Google Scholar] [CrossRef] [PubMed]
- Lugner, M.; Sattar, N.; Miftaraj, M.; Ekelund, J.; Franzén, S.; Svensson, A.-M.; Eliasson, B. Cardiorenal and other diabetes related outcomes with SGLT-2 inhibitors compared to GLP-1 receptor agonists in type 2 diabetes: Nationwide observational study. Cardiovasc. Diabetol. 2021, 20, 67. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, R.W.; Knudsen, J.S.; Kahlert, J.; Baggesen, L.M.; Lajer, M.; Holmgaard, P.H.; Vedin, O.; Ustyugova, A.; Sørensen, H.T. Cardiovascular events, acute hospitalizations, and mortality in patients with type 2 diabetes mellitus who initiate empagliflozin versus liraglutide: A comparative effectiveness study. J. Am. Heart Assoc. 2021, 10, e019356. [Google Scholar] [CrossRef] [PubMed]
- Nørgaard, C.H.; Starkopf, L.; Gerds, T.A.; Vestergaard, P.; Bonde, A.N.; Fosbøl, E.; Køber, L.; Wong, N.D.; Torp-Pedersen, C.; Lee, C.J.-Y. Cardiovascular outcomes with GLP-1 receptor agonists vs. SGLT-2 inhibitors in patients with type 2 diabetes. Eur. Hear. J.-Cardiovasc. Pharmacother. 2021, pvab053. [Google Scholar] [CrossRef] [PubMed]
- Patorno, E.; Pawar, A.; Bessette, L.G.; Kim, D.H.; Dave, C.; Glynn, R.J.; Munshi, M.N.; Schneeweiss, S.; Wexler, D.J.; Kim, S.C. Comparative effectiveness and safety of Sodium–Glucose cotransporter 2 inhibitors versus Glucagon-like peptide 1 receptor agonists in older adults. Diabetes Care 2021, 44, 826–835. [Google Scholar] [CrossRef]
- Longato, E.; Di Camillo, B.; Sparacino, G.; Gubian, L.; Avogaro, A.; Fadini, G.P. Cardiovascular outcomes of type 2 diabetic patients treated with SGLT-2 inhibitors versus GLP-1 receptor agonists in real-life. BMJ Open Diabetes Res. Care 2020, 8, e001451. [Google Scholar] [CrossRef]
- Ueda, P.; Svanström, H.; Melbye, M.; Eliasson, B.; Svensson, A.-M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Pasternak, B. Sodium glucose cotransporter 2 inhibitors and risk of serious adverse events: Nationwide register based cohort study. BMJ 2018, 363, k4365. [Google Scholar] [CrossRef] [Green Version]
- Pasternak, B.; Wintzell, V.; Eliasson, B.; Svensson, A.-M.; Franzén, S.; Gudbjörnsdottir, S.; Hveem, K.; Jonasson, C.; Melbye, M.; Svanström, H.; et al. Use of Glucagon-Like Peptide 1 Receptor Agonists and Risk of Serious Renal Events: Scandinavian Cohort Study. Diabetes Care 2020, 43, 1326–1335. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Botros, F.T.; Riddle, M.C.; Rydén, L.; et al. Dulaglutide and renal outcomes in type 2 diabetes: An exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 2019, 394, 131–138. [Google Scholar] [CrossRef]
- Rondinelli, M.; Rossi, A.; Gandolfi, A.; Saponaro, F.; Bucciarelli, L.; Adda, G.; Molinari, C.; Montefusco, L.; Specchia, C.; Rossi, M.C.; et al. Use of Liraglutide in the Real World and Impact at 36 Months on Metabolic Control, Weight, Lipid Profile, Blood Pressure, Heart Rate, and Renal Function. Clin. Ther. 2016, 39, 159–169. [Google Scholar] [CrossRef]
- Boye, K.S.; Mody, R.; Wu, J.; Lage, M.J.; Botros, F.T.; Woodward, B. Effects of Dulaglutide and Insulin Glargine on Estimated Glomerular Filtration Rate in a Real-world Setting. Clin. Ther. 2018, 40, 1396–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boye, K.S.; Botros, F.T.; Haupt, A.; Woodward, B.; Lage, M.J. Glucagon-Like Peptide-1 Receptor Agonist Use and Renal Impairment: A Retrospective Analysis of an Electronic Health Records Database in the U.S. Population. Diabetes Ther. 2018, 9, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Krentz, A.J.; Deanfield, J.; Rydén, L. Evolution of Type 2 Diabetes Management from a Glucocentric Approach to Cardio-Renal Risk Reduction: The New Paradigm of Care. Drugs 2021, 81, 1373–1379. [Google Scholar] [CrossRef]
- Caruso, I.; Cignarelli, A.; Natalicchio, A.; Perrini, S.; Laviola, L.; Giorgino, F. Commentary: Glucose control: Not just a bystander in GLP-1RA-mediated cardiovascular protection. Metabolism 2020, 109, 154272. [Google Scholar] [CrossRef]
- Verma, S.; McMurray, J.J.V. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstein, H.C.; Sattar, N.; Rosenstock, J.; Ramasundarahettige, C.; Pratley, R.; Lopes, R.D.; Lam, C.S.; Khurmi, N.S.; Heenan, L.; Del Prato, S.; et al. Cardiovascular and Renal Outcomes with Efpeglenatide in Type 2 Diabetes. N. Engl. J. Med. 2021, 385, 896–907. [Google Scholar] [CrossRef]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular outcomes with Ertugliflozin in type 2 diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef]
- Longato, E.; Di Camillo, B.; Sparacino, G.; Tramontan, L.; Avogaro, A.; Fadini, G.P. Cardiovascular effectiveness of human-based vs. exendin-based glucagon like peptide-1 receptor agonists: A retrospective study in patients with type 2 diabetes. Eur. J. Prev. Cardiol. 2020, 28, 22–29. [Google Scholar] [CrossRef]
- Caruso, I.; Cignarelli, A.; Giorgino, F. Heterogeneity and Similarities in GLP-1 Receptor Agonist Cardiovascular Outcomes Trials. Trends Endocrinol. Metab. 2019, 30, 578–589. [Google Scholar] [CrossRef]
- Giorgino, F.; Penfornis, A.; Pechtner, V.; Gentilella, R.; Corcos, A. Adherence to antihyperglycemic medications and glucagon-like peptide 1-receptor agonists in type 2 diabetes: Clinical consequences and strategies for improvement. Patient Prefer. Adherence 2018, 12, 707–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carls, G.S.; Tuttle, E.; Tan, R.-D.; Huynh, J.; Yee, J.; Edelman, S.V.; Polonsky, W.H. Understanding the Gap Between Efficacy in Randomized Controlled Trials and Effectiveness in Real-World Use of GLP-1 RA and DPP-4 Therapies in Patients with Type 2 Diabetes. Diabetes Care 2017, 40, 1469–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerci, B.; Charbonnel, B.; Gourdy, P.; Hadjadj, S.; Hanaire, H.; Marre, M.; Vergès, B. Efficacy and adherence of glucagon-like peptide-1 receptor agonist treatment in patients with type 2 diabetes mellitus in real-life settings. Diabetes Metab. 2019, 45, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.Y. Why Choose Between SGLT2 Inhibitors and GLP1-RA When You Can Use Both? Circulation 2021, 143, 780–782. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | N | FU (yrs) | bCVD (%) | Comparators | GLP-1RA | CV Composite Endpoint * | MACE | CV Death | All-Cause Death | Stroke | ACS/MI | PAD | HHF |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baviera, et al., 2021 | 18,716 a; 9772 b | 3.9 a; 3.7 b | 11.8–12.1 a 11.9–12.9 b | MET, SU, glinides, TZD, acarbose, DPP-4i | - | - | - | - | 0.61 (0.56–0.65)a 0.63 (0.55–0.71)b | 0.72 (0.60–0.87) a 1.01 (0.76–1.33)b | 0.94 (0.85–1.04) a 0.89 (0.77–1.03) b | 0.72 (0.64–0.82) a 0.80 (0.67–0.98)b | 0.91 (0.82–1.01) a 0.85 (0.73–1.00) b |
| Zerovnic, et al., 2021 | 855 vs. 3817 | 2.5–3.2 | 6 | DPP-4i | 44.9%Lira, 32.6%Dula, 17.5%Exe, 4.9%Lixi | - | 0.64 (0.43–0.97) | 0.62 (0.34–1.14) | 0.53 (0.35–0.79) | - | - | - | 1.39 (0.88–2.21) |
| Lin, et al., 2021 | 4460 vs. 13,380 | 2.3–3.2 | 20.2 | DPP-4i | - | - | 0.62 (0.51–0.76) | 0.53 (0.39–0.73) | 0.43 (0.34–0.54) | 0.71 (0.52–0.96) | 0.63 (0.40–0.97) | 0.63 (0.29–1.35) | 0.80 (0.56–1.13) |
| Pineda, et al., 2020 | 815 | 1 | 14.4–23.1 | MET, SU, glinides, TZD, acarbose, DPP-4i, insulin | - | 0.71 (0.52–0.90) | - | - | - | 1.25 (0.57–2.73) | 1.29 (0.47–3.57) | - | 0.80 (0.54–1.17) |
| Yang, et al., 2020 | 1893 c, 1829 d, 1367 e | 1.5–2 | 14.9–14.7 c 14.7–17.0 d 16.5–18.1 e | DPP-4i c, SU d, insulin e | - | 0.73 (0.57–0.96)c0.76 (0.57–1.00)d0.81 (0.62–1.07)e | 0.55 (0.35–0.86)c 0.79 (0.49–1.26)d 0.62 (0.37–1.02)e | - | - | - | - | - | - |
| Longato, et al., 2020 | 2807 | 1.5 | 13.7–15.1 | DPP-4i | Exe, Lira, Lixi, Dula | - | 0.67 (0.53–0.86) | - | 0.58 (0.35–0.96) | 1.00 (0.60–1.68) | 0.67 (0.50–0.91) | - | 0.69 (0.46–1.04) |
| Svanström, et al., 2019 | 23,402 | 3.3 | 81.0 | DPP-4i | Lira | - | 0.90 (0.83–0.98) | 0.78 (0.68–0.91) | 0.83 (0.77–0.90) | 0.88 (0.77–1.01) | 0.94 (0.84–1.06) | - | 0.90 (0.80–1.03) |
| O’Brien, et al., 2018 | 11,351 vs. 28,898 | 1.3 | 5.5 | DPP-4i | - | 0.78 (0.63–0.96) | - | - | - | 0.65 (0.44–0.97) | 0.91 (0.67–1.24) | 0.90 (0.42–1.95) | 0.65 (0.42–1.02) |
| Toulis, et al., 2017 | 8345 vs. 16,541 | 2.6 | 21.8–20.4 | Conventional GLD | 55%Lira, 42%Exe, 3%Lixi | - | - | - | 0.64 (0.56–0.74) | - | - | - | - |
| Patorno, et al., 2016 | 35,534 c, 28,138 d, 47,068 e | 0.5–0.8 | ~20 | DPP-4i c, SU d, insulin e | 67.1%ExeBID, 28.3%Lira, 4.6%ExeQW | 1.20 (0.76–1.89) c 1.05 (0.63–1.74) d 1.01 (0.73–1.41) e | - | - | - | - | - | - | - |
| Study | N | FU (yrs) | bCVD(%) | Comparators | GLP-1RA | CV Composite Endpoint * | MACE | CV Death | All-Cause Death | Stroke | ACS/MI | PAD | HF |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| § Patorno, et al., 2021 | 45,047 | 0.5 | 45.2 | SGLT-2i (76.9%Cana, 13.1%Dapa, 11.1%Empa) | 58.7% Lira, 23.5% Exe, 14.8% Dula, 3.0% Albi | - | 0.98 (0.87–1.10) | 0.83 (0.64–1.07) | 0.95 (0.81–1.11) | 1.04 (0.86–1.27) | 0.98 (0.84–1.16) | - | 0.68 (0.57–0.80) |
| § DeRemer, et al., 2021 | 4829 vs. 7082 | n.a. | Subgroup 1: 0 Subgroup 2: 100 | SGLT-2i (Empa, Cana) | Exe, Lira, Albi, Dula | Subgroup 1: 1.06 (0.72–1.49) Subgroup 2: 0.67 (0.47–0.96) | - | - | - | Subgroup 1: 1.08 (0.67–1.75) Subgroup 2: 0.85 (0.50–1.70) | Subgroup 1: 1.35 (0.67–2.71) Subgroup 2: 1.14 (0.58–2.15) | - | Subgroup 1: 0.87 (0.47–1.61) Subgroup 2: 0.46 (0.27–0.79) |
| # Nørgaard, et al., 2021 | 8913 vs. 5275 | n.a. | n.a. | SGLT-2i | - | - | 5.6% (5.2–6.1) vs. 5.6% (4.8–6.3) | - | - | 2.5% (2.2–2.9) 2.6% (2.2–3.1) | 2.1% (1.8–2.4) vs. 2.1% (1.8–2.4) | - | 1.7% (1.5–2.0) vs. 1.8% (1.2–2.5) |
| § Patorno, et al., 2021 | Cohort 1: 133,139 Cohort 2: 52,901 | 0.6 | Cohort 1: 0 Cohort 2: 100 | SGLT-2i (Cana, Dapa, Empa) | Albi, Dula, Exe, Lira | Cohort 1: 1.07 (0.97–1.18) Cohort 2: 0.90 (0.82–0.98) | - | - | Cohort 1: 1.01 (0.87–1.17) Cohort 2: 0.88 (0.79–0.99) | Cohort 1: 0.96 (0.82–1.13) Cohort 2: 1.00 (0.87–1.15) | Cohort 1: 1.13 (1.00–1.28) Cohort 2: 0.83 (0.74–0.93) | - | Cohort 1: 0.69 (0.56–0.85) Cohort 2: 0.71 (0.64–0.79) |
| § Thomsen, et al., 2021 | 12,706 vs. 14,498 | 1.1 | 30 | SGLT-2i (Empa) | Lira | 1.02 (0.91–1.14) | - | - | 0.93 (0.89–0.98) | - | - | - | 0.77 (0.49–1.20) |
| § Lugner, et al., 2021 | 9648 vs. 12,097 | 1.7–1.1 | 15.8–17.0 | SGLT-2i (56.6%Empa, 43.2% Dapa, 0.2% Cana) | 75.1% Lira, 16.3% Dula, 6.4% ExeQW | - | 1.03 (0.89–1.21) | 1.00 (0.47–2.13) | 0.78 (0.61–1.01) | 1.44 (0.99–2.08) | 0.94 (0.68–1.3) | 1.68 (1.04–2.72) | 0.83 (0.65–1.07) |
| § Longato, et al., 2020 | 8596 | 1.08 | 18 | SGLT-2i (50% Empa, 40% Dapa, 10% Cana) | 48% Dula, 34% Lira, 14% Exe, 4% Lixi | - | 0.78 (0.61–0.99) | - | 0.74 (0.43–1.29) | 0.91 (0.56–1.48) | 0.72 (0.53–0.98) | - | 0.59 (0.35–0.99) |
| § Pineda, et al., 2020 | 947 | 1 | 12.8–12.0 | SGLT-2i | - | 1.00 (0.69–1.44) | - | - | - | 0.87 (0.38–1.97) | 1.12 (0.34–3.68) | - | 0.83 (0.53–1.30) |
| Boye et al. | Boye et al. | Lugner et al. | Pasternak et al. | ||
|---|---|---|---|---|---|
| Main Baseline Features | N | 5932 | 2366 | 21,781 | 77,462 |
| GLP-1RA | - | Dulaglutide | 75.1% Liraglutide 16.3% Dulaglutide 6.4% Exenatide QW | 92.5% Liraglutide 6.2% Exenatide 0.7% Lixisenatide 0.6% Dulaglutide | |
| Comparator | Other GLD | Insulin Glargine | SGLT-2i (56.6% Empagliflozin 43.2% Dapagliflozin 0.2% Canagliflozin) | DPP-4i | |
| Follow-up (yrs) | 1 | 1 | 1.7–1.1 | 3.0 | |
| Mean age (yrs) | 59.2 | 59.7 | 60.5 | 59.3 | |
| Female (%) | 52.0 | 51.1 | 37.5 | 40.7 | |
| Mean diabetes duration (yrs) | - | - | 7.5 | - | |
| Mean HbA1c (%) | 8.4 | 8.3 | 8.3 | - | |
| Mean eGFR (mL/min/1.73 m2) | 82.1 | 83.7 | 91.6 | - | |
| eGFR <60 mL/min/1.73 m2 (%) | 19.4 | 18.2 | - | 4.6 | |
| Mean albuminuria (mg/L) | - | - | - | - | |
| Microalbuminuria (%) | - | - | 20.6 | - | |
| Macroalbuminuria (%) | - | - | 4.3 | - | |
| Renal Outcomes | Change in albuminuria (mean (95% CI)) | - | - | - | - |
| New onset MA (HR (95% CI)) | - | - | 0.89 (0.77–1.04) | - | |
| Change in eGFR (mL/min/1.73 m2) | −0.80 vs. −1.03 p = 0.0005 | −0.4 vs. −0.9 p = 0.0024 | - | - | |
| ≥30% eGFR reduction | 2.19% vs. 3.14% p < 0.0001 | 3.3% vs 4.1%; p < 0.0001 | 0.92 (0.68–1.25) § | - | |
| ≥40% eGFR reduction (HR (95% CI)) # | - | - | 0.94 (0.62–1.43) | - | |
| Composite renal Outcome * (HR (95% CI)) # | - | - | 0.98 (0.92–1.05) | 0.76 (0.68–0.85)/0.60 (0.49–0.74) | |
| Renal replacement therapy (HR (95% CI)) # | - | - | - | 0.73 (0.62–0.87)/0.42 (0.29–0.62) | |
| Hospitalization for renal events (HR (95% CI)) # | - | - | - | 0.73 (0.65–0.83)/0.63 (0.50–0.78) | |
| Renal death (HR (95% CI)) # | - | - | - | 0.72 (0.48–1.10)/0.66 (0.24–1.49) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, I.; Cignarelli, A.; Sorice, G.P.; Natalicchio, A.; Perrini, S.; Laviola, L.; Giorgino, F. Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies. Metabolites 2022, 12, 183. https://doi.org/10.3390/metabo12020183
Caruso I, Cignarelli A, Sorice GP, Natalicchio A, Perrini S, Laviola L, Giorgino F. Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies. Metabolites. 2022; 12(2):183. https://doi.org/10.3390/metabo12020183
Chicago/Turabian StyleCaruso, Irene, Angelo Cignarelli, Gian Pio Sorice, Annalisa Natalicchio, Sebastio Perrini, Luigi Laviola, and Francesco Giorgino. 2022. "Cardiovascular and Renal Effectiveness of GLP-1 Receptor Agonists vs. Other Glucose-Lowering Drugs in Type 2 Diabetes: A Systematic Review and Meta-Analysis of Real-World Studies" Metabolites 12, no. 2: 183. https://doi.org/10.3390/metabo12020183