
The Role of Kynurenine and Its Metabolites in Comorbid Chronic Pain and Depression


Abstract
:1. Introduction
2. Epidemiology of Comorbid Chronic Pain and Depression
3. Neural Mechanisms Linking Chronic Pain and Depression
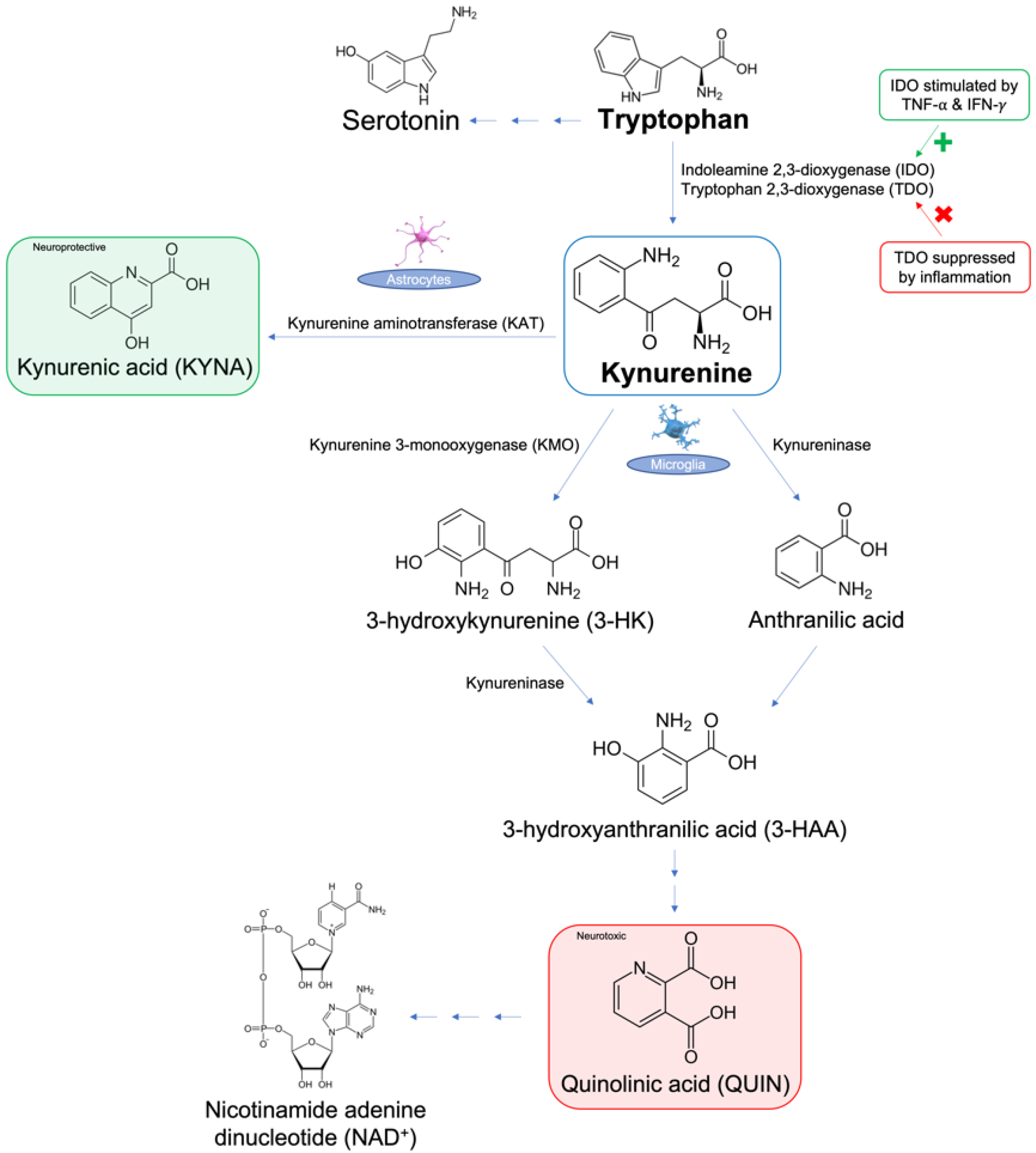
4. Kynurenine Pathway and Chronic Pain
5. Kynurenine Pathway and Depression
6. Kynurenine Metabolites in Chronic Pain and Depression
7. Kynurenine Metabolites in Animal Studies
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pitcher, M.H.; Von Korff, M.; Bushnell, M.C.; Porter, L. Prevalence and Profile of High-Impact Chronic Pain in the United States. J. Pain. 2019, 20, 146–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dydyk, A.M.; Conermann, T. Chronic Pain; StatPearls: Treasure Island, FL, USA, 2022; pp. 1–25. [Google Scholar]
- Yong, R.J.; Mullins, P.M.; Bhattacharyya, N. Prevalence of chronic pain among adults in the United States. Pain 2022, 163, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Roughan, W.H.; Campos, A.I.; García-Marín, L.M.; Cuellar-Partida, G.; Lupton, M.K.; Hickie, I.B.; Medland, S.E.; Wray, N.R.; Byrne, E.M.; Ngo, T.T.; et al. Comorbid Chronic Pain and Depression: Shared Risk Factors and Differential Antidepressant Effectiveness. Front. Psychiatry 2021, 12, 643609. [Google Scholar] [CrossRef] [PubMed]
- Orhurhu, V.; Olusunmade, M.; Akinola, Y.; Urits, I.; Salisu Orhurhu, M.; Viswanath, O.; Hirji, S.; Kaye, A.D.; Simopoulos, T.; Gill, J.S. Depression Trends in Patients with Chronic Pain: An Analysis of the Nationwide Inpatient Sample. Pain Physician 2019, 22, 487–494. [Google Scholar] [CrossRef]
- Ford, D.E.; Erlinger, T.P. Depression and C-reactive protein in US adults: Data from the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2004, 164, 1010–1014. [Google Scholar] [CrossRef] [Green Version]
- Noble, R.E. Depression in women. Metabolism 2005, 54, 49–52. [Google Scholar] [CrossRef]
- Ettman, C.K.; Cohen, G.H.; Vivier, P.M.; Galea, S. Savings, home ownership, and depression in low-income US adults. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1211–1219. [Google Scholar] [CrossRef]
- Leung, C.W.; Epel, E.S.; Willett, W.C.; Rimm, E.B.; Laraia, B.A. Household food insecurity is positively associated with depression among low-income supplemental nutrition assistance program participants and income-eligible nonparticipants. J. Nutr. 2015, 145, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Rayner, L.; Hotopf, M.; Petkova, H.; Matcham, F.; Simpson, A.; McCracken, L.M. Depression in patients with chronic pain attending a specialised pain treatment centre: Prevalence and impact on health care costs. Pain 2016, 157, 1472–1479. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 26 September 2022).
- Agüera-Ortiz, L.; Failde, I.; Mico, J.A.; Cervilla, J.; López-Ibor, J.J. Pain as a symptom of depression: Prevalence and clinical correlates in patients attending psychiatric clinics. J. Affect. Disord. 2011, 130, 106–112. [Google Scholar] [CrossRef]
- Amtmann, D.; Cook, K.F.; Jensen, M.P.; Chen, W.H.; Choi, S.; Revicki, D.; Cella, D.; Rothrock, N.; Keefe, F.; Callahan, L.; et al. Development of a PROMIS item bank to measure pain interference. Pain 2010, 150, 173–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Heer, E.W.; Gerrits, M.M.; Beekman, A.T.; Dekker, J.; van Marwijk, H.W.J.; de Waal, M.W.M.; Spinhoven, P.; Penninx, B.W.J.H.; van der Feltz-Cornelis, C.M. The association of depression and anxiety with pain: A study from NESDA. PLoS ONE 2014, 9, e115077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gelaye, B.; Williams, M.A.; Lemma, S.; Deyessa, N.; Bahretibeb, Y.; Shibre, T.; Wondimagegn, D.; Lemenih, A.; Fann, J.R.; Vander Stoep, A.; et al. Diagnostic validity of the composite international diagnostic interview (CIDI) depression module in an East African population. Int. J. Psychiatry Med. 2013, 46, 387–405. [Google Scholar] [CrossRef] [Green Version]
- van Hecke, O.; Hocking, L.J.; Torrance, N.; Campbell, A.; Padmanabhan, S.; Porteous, D.J.; McIntosh, A.M.; Burri, A.V.; Tanaka, H.; Williams, F.M.K.; et al. Chronic pain, depression and cardiovascular disease linked through a shared genetic predisposition: Analysis of a family-based cohort and twin study. PLoS ONE 2017, 12, e0170653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheng, J.; Liu, S.; Wang, Y.; Cui, R.; Zhang, X. The Link between Depression and Chronic Pain: Neural Mechanisms in the Brain. Neural Plast. 2017, 2017, 9724371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ménard, C.; Hodes, G.E.; Russo, S.J. Pathogenesis of depression: Insights from human and rodent studies. Neuroscience 2016, 321, 138–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.F.; Peng, W.; Sweeney, J.A.; Jia, Z.Y.; Gong, Q.Y. Brain structure alterations in depression: Psychoradiological evidence. CNS Neurosci. Ther. 2018, 24, 994–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandya, M.; Altinay, M.; Malone, D.A., Jr.; Anand, A. Where in the brain is depression? Curr. Psychiatry Rep. 2012, 14, 634–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinoza-Oyarce, D.A.; Shaw, M.E.; Alateeq, K.; Cherbuin, N. Volumetric brain differences in clinical depression in association with anxiety: A systematic review with meta-analysis. J. Psychiatry Neurosci. 2020, 45, 406–429. [Google Scholar] [CrossRef]
- Kang, H.J.; Voleti, B.; Hajszan, T.; Rajkowska, G.; Stockmeier, C.A.; Licznerski, P.; Lepack, A.; Majik, M.S.; Jeong, L.S.; Banasr, M.; et al. Decreased expression of synapse-related genes and loss of synapses in major depressive disorder. Nat. Med. 2012, 18, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Baliki, M.N.; Chialvo, D.R.; Geha, P.Y.; Levy, R.M.; Harden, R.N.; Parrish, T.B.; Apkarian, A.V. Chronic pain and the emotional brain: Specific brain activity associated with spontaneous fluctuations of intensity of chronic back pain. J. Neurosci. 2006, 26, 12165–12173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, A.K.; Kavelaars, A.; Heijnen, C.J.; Dantzer, R. Neuroinflammation and comorbidity of pain and depression. Pharmacol. Rev. 2013, 66, 80–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef] [Green Version]
- Campos, A.C.P.; Antunes, G.F.; Matsumoto, M.; Pagano, R.L.; Martinez, R.C.R. Neuroinflammation, Pain and Depression: An Overview of the Main Findings. Front. Psychol. 2020, 11, 1825. [Google Scholar] [CrossRef] [PubMed]
- Castro-Portuguez, R.; Sutphin, G.L. Kynurenine pathway, NAD+ synthesis, and mitochondrial function: Targeting tryptophan metabolism to promote longevity and healthspan. Exp. Gerontol. 2020, 132, 110841. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, F.; Candido, K.D.; Knezevic, N.N. The Role of the Kynurenine Signaling Pathway in Different Chronic Pain Conditions and Potential Use of Therapeutic Agents. Int. J. Mol. Sci. 2020, 21, 6045. [Google Scholar] [CrossRef]
- Ogyu, K.; Kubo, K.; Noda, Y.; Iwata, Y.; Tsugawa, S.; Omura, Y.; Wada, M.; Tarumi, R.; Plitman, E.; Moriguchi, S.; et al. Kynurenine pathway in depression: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2018, 90, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Savitz, J. The kynurenine pathway: A finger in every pie. Mol. Psychiatry 2020, 25, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Staats-Pires, A.; Tan, V.X.; Heng, B.; Guillemin, G.J.; Latini, A. Kynurenine and Tetrahydrobiopterin Pathways Crosstalk in Pain Hypersensitivity. Front. Neurosci. 2020, 14, 620. [Google Scholar] [CrossRef] [PubMed]
- Barjandi, G.; Louca-Jounger, S.; Löfgren, M.; Bileviciute-Ljungar, I.; Kosek, E.; Ernberg, M. Plasma tryptophan and kynurenine in females with temporomandibular disorders and fibromyalgia-An exploratory pilot study. J. Oral Rehabil. 2020, 47, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.M.; Bao, C.H.; Wu, Y.; Liang, S.H.; Wang, D.; Wu, L.Y.; Huang, Y.; Liu, H.R.; Wu, H.G. Tryptophan-kynurenine metabolism: A link between the gut and brain for depression in inflammatory bowel disease. J. Neuroinflamm. 2021, 18, 135. [Google Scholar] [CrossRef] [PubMed]
- Pope, J.E.; Fishman, M.A.; Gunn, J.A.; Cotten, B.M.; Hill, M.M.; Deer, T.R. Cross-Validation of the Foundation Pain Index with PROMIS-29 in Chronic Pain Patients. J. Pain Res. 2021, 14, 2677–2685. [Google Scholar] [CrossRef] [PubMed]
- Groven, N.; Reitan, S.K.; Fors, E.A.; Guzey, I.C. Kynurenine metabolites and ratios differ between Chronic Fatigue Syndrome, Fibromyalgia, and healthy controls. Psychoneuroendocrinology 2021, 131, 105287. [Google Scholar] [CrossRef]
- Erhardt, S.; Lim, C.; Linderholm, K.; Janelidze, S.; Lindqvist, D.; Samuelsson, M.; Lundberg, K.; Postolache, T.T.; Traskman-Bendz, L.; Guillemin, G.J.; et al. Connecting inflammation with glutamate agonism in suicidality. Neuropsychopharmacology 2013, 38, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Kanchanatawan, B.; Sirivichayakul, S.; Thika, S.; Ruxrungtham, K.; Carvalho, A.F.; Geffard, M.; Anderson, G.; Noto, C.; Ivanova, R.; Maes, M. Physio-somatic symptoms in schizophrenia: Association with depression, anxiety, neurocognitive deficits and the tryptophan catabolite pathway. Metab. Brain Dis. 2017, 32, 1003–1016. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.J.; Huang, X.F.; Newell, K.A. The kynurenine pathway in major depression: What we know and where to next. Neurosci. Biobehav. Rev. 2021, 127, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.M.; Pocivavsek, A.; Nicholson, J.D.; Notarangelo, F.M.; Langenberg, P.; McMahon, R.P.; Kleinman, J.E.; Hyde, T.M.; Stiller, J.; Postolache, T.T.; et al. Reduced kynurenine pathway metabolism and cytokine expression in the prefrontal cortex of depressed individuals. J. Psychiatry Neurosci. 2016, 41, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Réus, G.Z.; Jansen, K.; Titus, S.; Carvalho, A.F.; Gabbay, V.; Quevedo, J. Kynurenine pathway dysfunction in the pathophysiology and treatment of depression: Evidences from animal and human studies. J. Psychiatr. Res. 2015, 68, 316–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, M.; Török, N.; Tóth, F.; Szabó, Á.; Vécsei, L. Co-Players in Chronic Pain: Neuroinflammation and the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 897. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.S.; Ogbechi, J.; Clanchy, F.I.; Williams, R.O.; Stone, T.W. IDO and Kynurenine Metabolites in Peripheral and CNS Disorders. Front. Immunol. 2020, 11, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojewska, E.; Piotrowska, A.; Makuch, W.; Przewlocka, B.; Mika, J. Pharmacological kynurenine 3-monooxygenase enzyme inhibition significantly reduces neuropathic pain in a rat model. Neuropharmacology 2016, 102, 80–91. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, J.C.; André, C.; Wang, Y.; Lawson, M.A.; Szegedi, S.S.; Lestage, J.; Castanon, N.; Kelley, K.W.; Dantzer, R. Interferon-gamma and tumor necrosis factor-alpha mediate the upregulation of indoleamine 2,3-dioxygenase and the induction of depressive-like behavior in mice in response to bacillus Calmette-Guerin. J. Neurosci. 2009, 29, 4200–4209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.F.; Wang, J.; Han, J.F.; Guo, J.; Xie, Z.M.; Pan, W.; Yang, J.J.; Sun, K.J. Acute single dose of ketamine relieves mechanical allodynia and consequent depression-like behaviors in a rat model. Neurosci. Lett. 2016, 631, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Dantzer, R.; Budac, D.P.; Walker, A.K.; Mao-Ying, Q.L.; Lee, A.W.; Heijnen, C.J.; Kavelaars, A. Peripheral indoleamine 2,3-dioxygenase 1 is required for comorbid depression-like behavior but does not contribute to neuropathic pain in mice. Brain Behav. Immun. 2015, 46, 147–153. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Patient Population | Patient Demographics | Assessments/Diagnosis Methods | Patients with Comorbid Disorder |
|---|---|---|---|---|
| Orhurhu et al., 2019 [5] PMID 31561661 | 9.3 million inpatients with ICD-9/10 diagnosis of chronic pain | Mean age: 59 67.5% female | ICD-9, ICD-10 for both chronic pain and depression | 2.2 million patients (22.9%) with comorbid depression |
| Rayner et al., 2016 [10] PMID 26963849 | 1204 chronic pain patients referred to a specialty outpatient pain management unit | Median age: 47 67% female | Depression (diagnosis and severity) assessed using the PHQ-9 | 407 patients (33.8%) with comorbid severe MDD 256 (21.3%) with comorbid moderate MDD 69 (5.7%) with comorbid mild MDD |
| Aguera-Ortiz et al., 2011 [13] PMID 21055826 | 3566 patients attending outpatient psychiatric facilities | Mean age: 49.4 71.3% female | Depression diagnosed based on the DSM-IV-TR, intensity assessed by the 17-item Hamilton depression scale Pain assessed by survey questions, pain intensity assessed by VAS | 2107 patients (59.1%) with depression also reported pain |
| de Heer et al., 2014 [15] PMID 25330004 | 2981 patients recruited from the community, primary care providers, and specialized mental health care facilities | Mean age: 41.9 66.4% female | Depression/anxiety diagnosed via DSM-IV-based CIDI, severity of depression assessed via QIDS-SR, severity of anxiety assessed via BAI Pain assessed using the 7-item CPG Scale | 396 (13.3%) with current diagnosis of depression, 543 (18.2%) with current diagnosis of anxiety, 762 (25.6%) with current diagnosis of both depression and anxiety, 628 (21.1%) with remitted disorder 80% of patients with CPG 4 pain also had a current diagnosis of depression (14.3%), anxiety (13.5%), or both (52.1%) |
| Study | Morbidity | Sample Type/Test | Number of Patients | Main Findings |
|---|---|---|---|---|
| Barjandi et al., 2019 [33] PMID: 31545529 | Fibromyalgia and temporomandibular disorders myalgia | Venous blood tests and ELISA tests | 113 total: 17 temporomandibular disorders myalgia; 40 fibromyalgia; 56 healthy controls | Negative correlation between Trp ratio and pain intensity Positive correlation between kynurenine/Trp ratio and pain intensity |
| Groven et al., 2021 [36] PMID: 34090138 | Chronic fatigue syndrome and fibromyalgia | Venous blood tests | 160 total: 48 chronic fatigue syndrome; 58 fibromyalgia; 54 healthy controls | Fibromyalgia: low KYNA Chronic fatigue syndrome: low KYNA/QUIN ratio Confirming the neurotoxicity and neuroprotective aspects of QUIN and KYNA, respectively |
| Erhardt et al., 2013 [37] PMID: 23299933 | Depression and suicide attempt survivors | Cerebrospinal fluid tests | 100 total: 64 suicide attempt survivors; 36 healthy controls | Low KYNA levels Elevated QUIN levels, at 300% of healthy controls Confirming the neurotoxicity and neuroprotective aspects of QUIN and KYNA, respectively |
| Brown et al., 2021 [39] PMID: 34029552 | Depression | Postmortem brain tissues | 45 | Low TNF-α and IFN-γ Low kynurenine activity suggesting the necessity of inflammation to observe kynurenine elevation in depression |
| Pope et al., 2021 [35] PMID: 34512007 | Depression, anxiety, and fatigue | Urine tests | 298 | Depression patients had worse pain scores than the general population 87.2% had abnormal QUIN and KYNA levels |
| Kanchanatawan et al., 2017 [38] PMID: 28258445 | Schizophrenia | Plasma molecular studies | 124 total: 84 schizophrenia; 40 healthy controls | 53.75% had somatic symptoms (muscle pain) Depression and anxiety tightly connected to physical symptoms High activity against QUIN Low activity against KYNA Consistent with the pattern observed in other studies |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Athnaiel, O.; Ong, C.; Knezevic, N.N. The Role of Kynurenine and Its Metabolites in Comorbid Chronic Pain and Depression. Metabolites 2022, 12, 950. https://doi.org/10.3390/metabo12100950
Athnaiel O, Ong C, Knezevic NN. The Role of Kynurenine and Its Metabolites in Comorbid Chronic Pain and Depression. Metabolites. 2022; 12(10):950. https://doi.org/10.3390/metabo12100950
Chicago/Turabian StyleAthnaiel, Onella, Charmaine Ong, and Nebojsa Nick Knezevic. 2022. "The Role of Kynurenine and Its Metabolites in Comorbid Chronic Pain and Depression" Metabolites 12, no. 10: 950. https://doi.org/10.3390/metabo12100950