

Postpartum Depression and Health: Role of Perceived Social Support among Pakistani Women

 , , ,
, , , 
Abstract
:1. Introduction
- There would be a relationship between postpartum depression, insomnia, mental health, physical health, and perceived social support among Pakistani women.
- Postpartum depression would be a significant predictor of insomnia, mental health, physical health, and perceived social support.
- Social support would be a significant predictor of postpartum depression, mental health, and physical health.
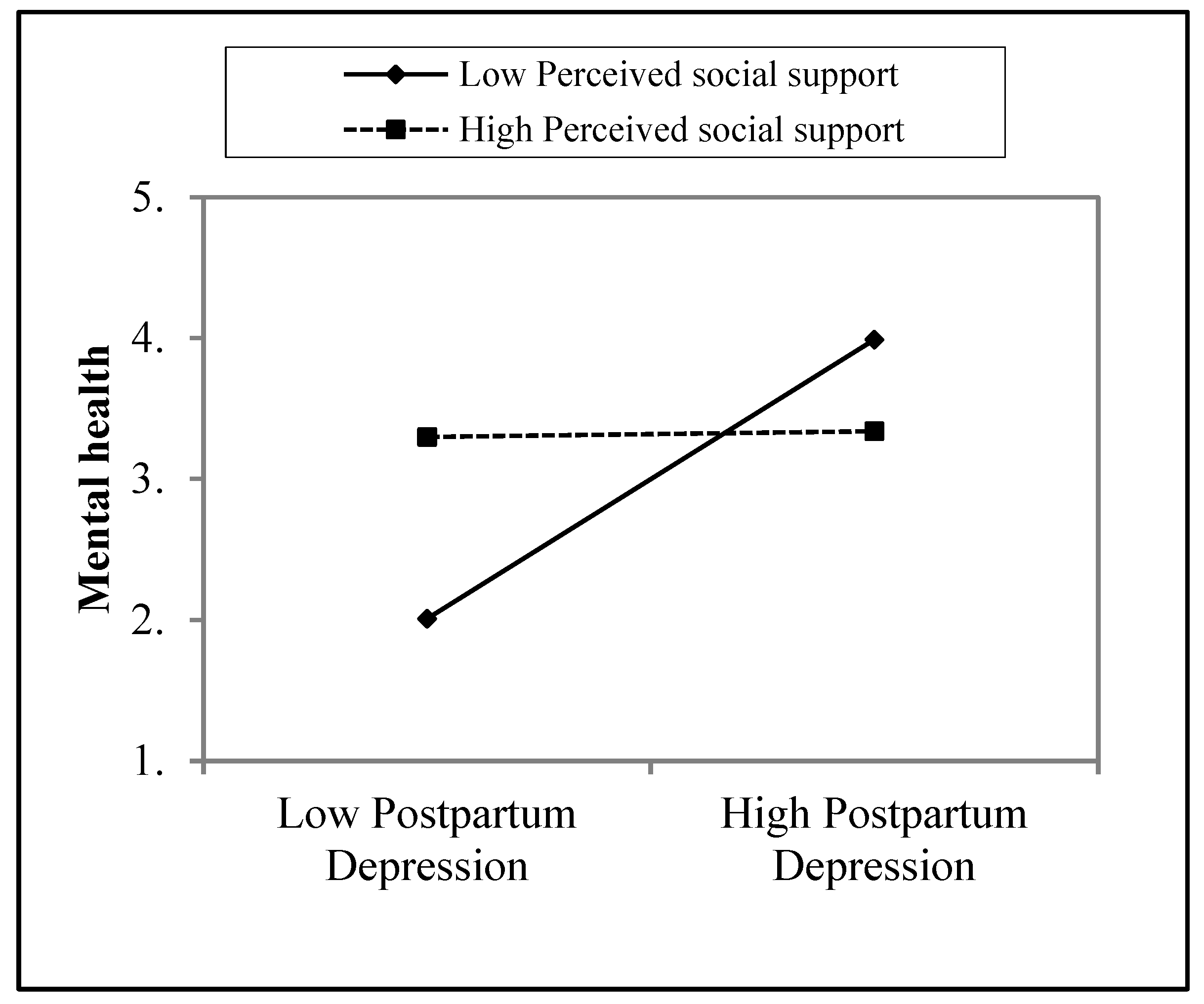
- There would be a moderating role of social support in the relationship between postpartum depression and mental health.
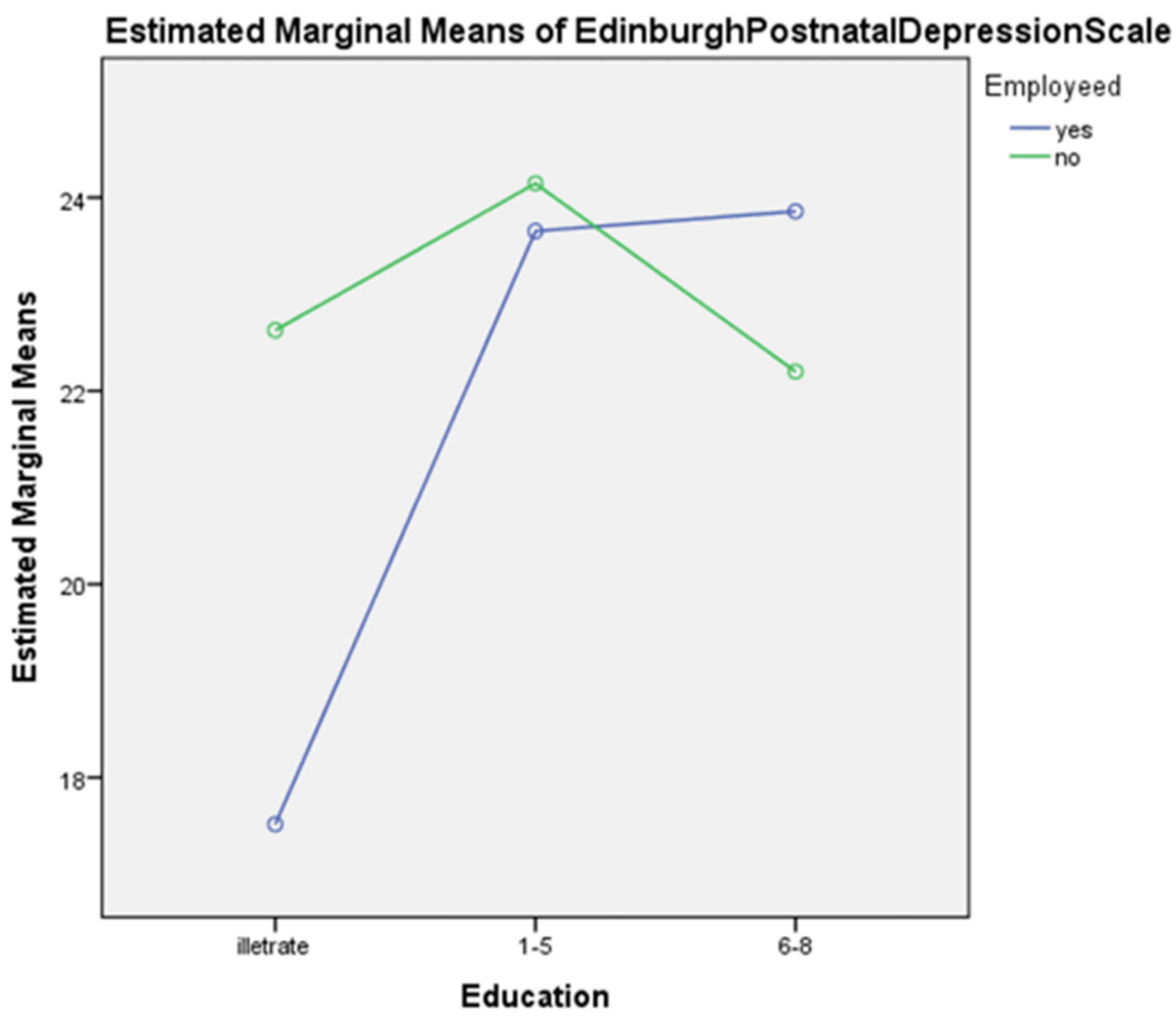
- Employed women who are uneducated would have more postpartum depression compared to educated unemployed women.
2. Methods
2.1. Materials and Procedures
2.2. Ethics
2.3. Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, E.J.; Park, J.S. Development of a prediction model for postpartum depression: Based on the mediation effect of antepartum depression. J. Korean Acad. Nurs. 2015, 45, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Association/APA, A.P. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®®); American Psychiatric Pub: Washington DC, USA, 2013. [Google Scholar]
- Taylor, S.E. Social support: A review. In The Oxford Handbook of Health Psychology; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Personal. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Aliani, R.; Khuwaja, B. Epidemiology of Postpartum Depression in Pakistan: A Review of Literature. Natl. J. Health Sci. 2017, 2, 24–30. [Google Scholar] [CrossRef]
- Gulamani, S.S.; Shaikh, K.; Chagani, J. Postpartum depression in Pakistan: A neglected issue. Nurs. Women’s Health 2013, 17, 147–152. [Google Scholar] [CrossRef]
- Jiang, Y.; Tang, Y.R.; Xie, C.; Yu, T.; Xiong, W.J.; Lin, L. Influence of sleep disorders on somatic symptoms, mental health, and quality of life in patients with chronic constipation. Medicine 2017, 96, e6093. [Google Scholar] [CrossRef] [PubMed]
- John, V.G. Predictors of Postpartum Depression among Women in Karachi, Pakistan. Predictors of Postpartum Depression among Women in Karachi, Pakistan, 1. 2017. Available online: http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=129592988&lang=es&site=ehost-live&scope=site (accessed on 19 November 2021).
- Shah, S.; Lonergan, B. Frequency of postpartum depression and its association with breastfeeding: A cross-sectional survey at immunization clinics in Islamabad, Pakistan. J. Pak. Med. Assoc. 2017, 67, 1151–1156. [Google Scholar]
- Marques, M.; Bos, S.; Soares, M.J.; Maia, B.; Pereira, A.T.; Valente, J.; Gomes, A.A.; Macedo, A.; Azevedo, M.H. Is insomnia in late pregnancy a risk factor for postpartum depression/depressive symptomatology? Psychiatry Res. 2011, 186, 272–280. [Google Scholar] [CrossRef]
- Dørheim, S.K.; Garthus-Niegel, S.; Bjorvatn, B.; Eberhard-Gran, M. Personality and Perinatal Maternal Insomnia: A Study Across Childbirth. Behav. Sleep Med. 2016, 14, 34–48. [Google Scholar] [CrossRef]
- Sivertsen, B.; Petrie, K.J.; Skogen, J.C.; Hysing, M.; Eberhard-Gran, M. Insomnia before and after childbirth: The risk of developing postpartum pain—A longitudinal population-based study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 210, 348–354. [Google Scholar] [CrossRef] [Green Version]
- Iranpour, S.; Kheirabadi, G.R.; Esmaillzadeh, A.; Heidari-Beni, M.; Maracy, M.R. Association between sleep quality and postpartum depression. J. Res. Med. Sci. 2016, 21, 110. [Google Scholar] [CrossRef]
- Dørheim, S.K.; Bjorvatn, B.; Eberhard-Gran, M. Can insomnia in pregnancy predict postpartum depression? A longitudinal, population-based study. PLoS ONE 2014, 9, e94674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okun, M.L.; Buysse, D.J.; Hall, M.H. Identifying insomnia in early pregnancy: Validation of the Insomnia Symptoms Questionnaire (ISQ) in pregnant women. J. Clin. Sleep Med. 2015, 11, 645–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivertsen, B.; Hysing, M.; Dørheim, S.K.; Eberhard-Gran, M. Trajectories of maternal sleep problems before and after childbirth: A longitudinal population-based study. BMC Pregnancy Childbirth 2015, 15, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stickley, A.; Leinsalu, M.; DeVylder, J.E.; Inoue, Y.; Koyanagi, A. Sleep problems and depression among 237 023 community-dwelling adults in 46 low- and middle-income countries. Sci. Rep. 2019, 9, 12011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shao, B.; Song, B.; Feng, S.; Lin, Y.; Du, J.; Shao, H.; Chi, Z.; Yang, Y.; Wang, F. The relationship of social support, mental health, and health-related quality of life in human immunodeficiency virus-positive men who have sex with men: From the analysis of canonical correlation and structural equation model: A cross-sectional study. Medicine 2018, 97, e11652. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, F.; Zarghami, M. Effect of postpartum depression on women’s mental and physical health four years after childbirth. East. Mediterr. Health J. 2018, 24, 1002–1009. [Google Scholar] [CrossRef]
- Hornby, T.G.; Holleran, C.L. Sleep matters. J. Neurol. Phys. Ther. 2014, 38, 170–171. [Google Scholar] [CrossRef]
- Kita, L.E. Investigating the Relationship between Sleep and Postpartum Depression. Ph.D. Thesis, Bournemouth University, Poole, UK, 2013. [Google Scholar]
- Miloseva, L.; Vukosavljevic-Gvozden, T.; Richter, K.; Milosev, V.; Niklewski, G. Perceived social support as a moderator between negative life events and depression in adolescence: Implications for prediction and targeted prevention. EPMA J. 2017, 8, 237–245. [Google Scholar] [CrossRef] [Green Version]
- Norhayati, M.N.; Nik Hazlina, N.H.; Asrenee, A.R.; Wan Emilin WM, A. Magnitude and risk factors for postpartum symptoms: A literature review. J. Affect. Disord. 2015, 175, 34–52. [Google Scholar] [CrossRef] [Green Version]
- Bukhari, S.R.; Afzal, F. Perceived Social Support predicts Psychological Problems among University Students. Int. J. Indian Psychol. 2017, 4, 18–27. [Google Scholar]
- Dağ, İ.; Şen, G. The mediating role of perceived social support in the relationships between general causality orientations and locus of control with psychopathological symptoms. Eur. J. Psychol. 2018, 14, 531–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kofman, Y.B.; Eng, Z.E.; Busse, D.; Godkin, S.; Campos, B.; Sandman, C.A.; Wing, D.; Yim, I.S. Cortisol reactivity and depressive symptoms in pregnancy: The moderating role of perceived social support and neuroticism. Biol. Psychol. 2019, 147, 107656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yim, I.S.; Stapleton LR, T.; Guardino, C.M.; Hahn, J.; Schetter, C.D.; Behavior, S.; Angeles, L. Depression: Systematic Review and Call for Integration. Annu. Rev. Clin. Psychol. 2015, 11, 99–137. [Google Scholar] [CrossRef] [Green Version]
- Kwok SY, C.L.; Yeung DY, L.; Chung, A. The moderating role of perceived social support on the relationship between physical functional impairment and depressive symptoms among Chinese nursing home elderly in Hong Kong. Sci. World J. 2011, 11, 1017–1026. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.; Cacciatore, A.; Giordano, R.; La Rosa, B. Postpartum period: Three distinct but continuous phases. J. Prenat. Med. 2010, 4, 22. [Google Scholar]
- Dawn, Child Marriage Bill Referred to Senate Body. 2018. Available online: https://senate.gov.pk/uploads/documents/1551158734_957.pdf (accessed on 19 November 2021).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression: Development of the 10-item Edinburgh Postnatal Depression scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [Green Version]
- Teissèdre, F.; Chabrol, H. Detecting Women at Risk for Postnatal Depression Using the Edinburgh Postnatal Depression Scale at 2 to 3 Days Postpartum. Can. J. Psychiatry 2004, 49, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Angst, J.; Gamma, A.; Ajdacic, V.; Eich, D.; Rössler, W. Prevalence, Course, and Comorbidity of Insomnia and Depression in Young Adults. Sleep 2008, 31, 473–480. [Google Scholar] [CrossRef]
- Stewart, D.; Bowers, L.; Simpson, A.; Ryan, C.; Tziggili, M. Manual restraint of adult psychiatric inpatients: A literature review. J. Psychiatr. Ment. Health Nurs. 2009, 16, 749–757. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.E.; Chideya, S.; Cubbin, C.; Williams, B.; Dekker, M.; Braveman, P. Should health studies measure wealth?: A systematic review. Am. J. Prev. Med. 2007, 33, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Tambag, H.; Turan, Z.; Tolun, S.; Can, R. Perceived social support and depression levels of women in the postpartum period in Hatay, Turkey. Niger. J. Clin. Pract. 2018, 21, 1525–1530. [Google Scholar] [CrossRef]
- Gan, Y.; Xiong, R.; Song, J.; Xiong, X.; Yu, F.; Gao, W.; Hu, H.; Zhang, J.; Tian, Y.; Gu, X.; et al. The effect of perceived social support during early pregnancy on depressive symptoms at 6 weeks postpartum: A prospective study. BMC Psychiatry 2019, 19, 232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaezi, A.; Soojoodi, F.; Banihashemi, A.T.; Nojomi, M. The association between social support and postpartum depression in women: A cross sectional study. Women Birth. 2019, 32, e238–e242. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.W.; Park, M.; Wallace, J.P. The impact of perceived social support, loneliness, and physical activity on quality of life in South Korean older adults. J. Sport Health Sci. 2016, 7, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eom, C.S.; Shin, D.W.; Kim, S.Y.; Yang, H.K.; Jo, H.S.; Kweon, S.S.; Kang, Y.S.; Kim, J.H.; Cho, B.L.; Park, J.H. Impact of perceived social support on the mental health and health-related quality of life in cancer patients: Results from a nationwide, multicenter survey in South Korea. Psycho-Oncology 2013, 22, 1283–1290. [Google Scholar] [CrossRef]
- Yoo, H.; Shin, D.W.; Jeong, A.; Kim, S.Y.; Yang, H.K.; Kim, J.S.; Lee, J.E.; Oh, J.H.; Park, E.C.; Park, K.; et al. Perceived social support and its impact on depression and health-related quality of life: A comparison between cancer patients and general population. Jpn. J. Clin. Oncol. 2017, 47, 728–734. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Zhu, H.; Zhang, B.; Cai, T. Perceived social support as moderator of perfectionism, depression, and anxiety in college students. Soc. Behav. Personal. 2013, 41, 1141–1152. [Google Scholar] [CrossRef]
- Itzick, M.; Kagan, M.; Tal-Katz, P. Perceived social support as a moderator between perceived discrimination and subjective well-being among people with physical disabilities in israel. Disabil. Rehabil. 2018, 40, 2208–2216. [Google Scholar] [CrossRef] [PubMed]
- Azad, R.; Fahmi, R.; Shrestha, S.; Joshi, H.; Hasan, M.; Khan AN, S.; Chowdhury MA, K.; Arifeen, S.E.L.; Billah, S.M. Prevalence and risk factors of postpartum depression within one year after birth in urban slums of Dhaka, Bangladesh. PLoS ONE 2019, 14, e0215735. [Google Scholar] [CrossRef] [Green Version]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Variables | f | % | |
|---|---|---|---|
| Age | 16–25 years | 169 | 52.8 |
| 26–35 | 151 | 47.2 | |
| Education | Illiterate | 102 | 31.9 |
| 1–5 class | 126 | 39.4 | |
| 6–8 class | 92 | 28.8 | |
| Delivery type | C-section | 207 | 64.7 |
| Normal delivery | 113 | 35.3 | |
| Newborn gender | Boy | 157 | 49.1 |
| Girl | 163 | 50.9 | |
| Employed | Yes | 154 | 48.1 |
| No | 166 | 51.9 | |
| Family system | Nuclear | 252 | 78.8 |
| Joint | 68 | 21.3 | |
| Number of Children | 0–4 children | 267 | 83.4 |
| 5–10 children | 53 | 16.6 | |
| Number of Daughters | 0 daughter | 103 | 32.2 |
| 1–3 daughters | 134 | 41.9 | |
| 4–6 daughters | 83 | 25.9 | |
| Number of Sons | 0 Son | 40 | 12.5 |
| 1–3 sons | 173 | 54.1 | |
| 4–6 sons | 107 | 33.4 | |
| Socioeconomic Status | High economic status | 70 | 21.9 |
| Moderate economic status | 124 | 38.8 | |
| Low economic status | 126 | 39.4 |
| Variables | M | SD | α | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 PPD | 22.56 | 4.84 | 0.92 | - | −0.24 *** | −0.03 | 0.45 *** | −0.38 *** | −0.21 *** | −0.34 *** | −31 *** |
| 2 INS | 25.4 | 3.49 | 0.56 | - | −0.08 | −0.14 * | 0.17 * | 0.12 | 0.09 | 0.16 * | |
| 3 MH | 26.2 | 4.85 | 0.79 | - | −0.04 | 0.01 | 0.18 ** | −0.02 | −0.06 | ||
| 4 PH | 22.98 | 3.3 | 0.59 | - | −0.23 *** | −0.20 ** | −0.22 ** | −0.15 * | |||
| 5 PSS | 41.17 | 5.24 | 0.71 | - | 0.69 *** | 0.78 *** | 0.83 *** | ||||
| 6 FM | 15.86 | 1.6 | 0.29 | - | 0.51 *** | 0.32 *** | |||||
| 7 FR | 13.05 | 2.07 | 0.49 | - | 0.38 *** | ||||||
| 8 SO | 12.86 | 3.04 | 0.81 | - |
| Variable | INS | PH | MH | PSS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | R2 | F | β | R2 | F | β | R2 | F | β | R2 | F | |
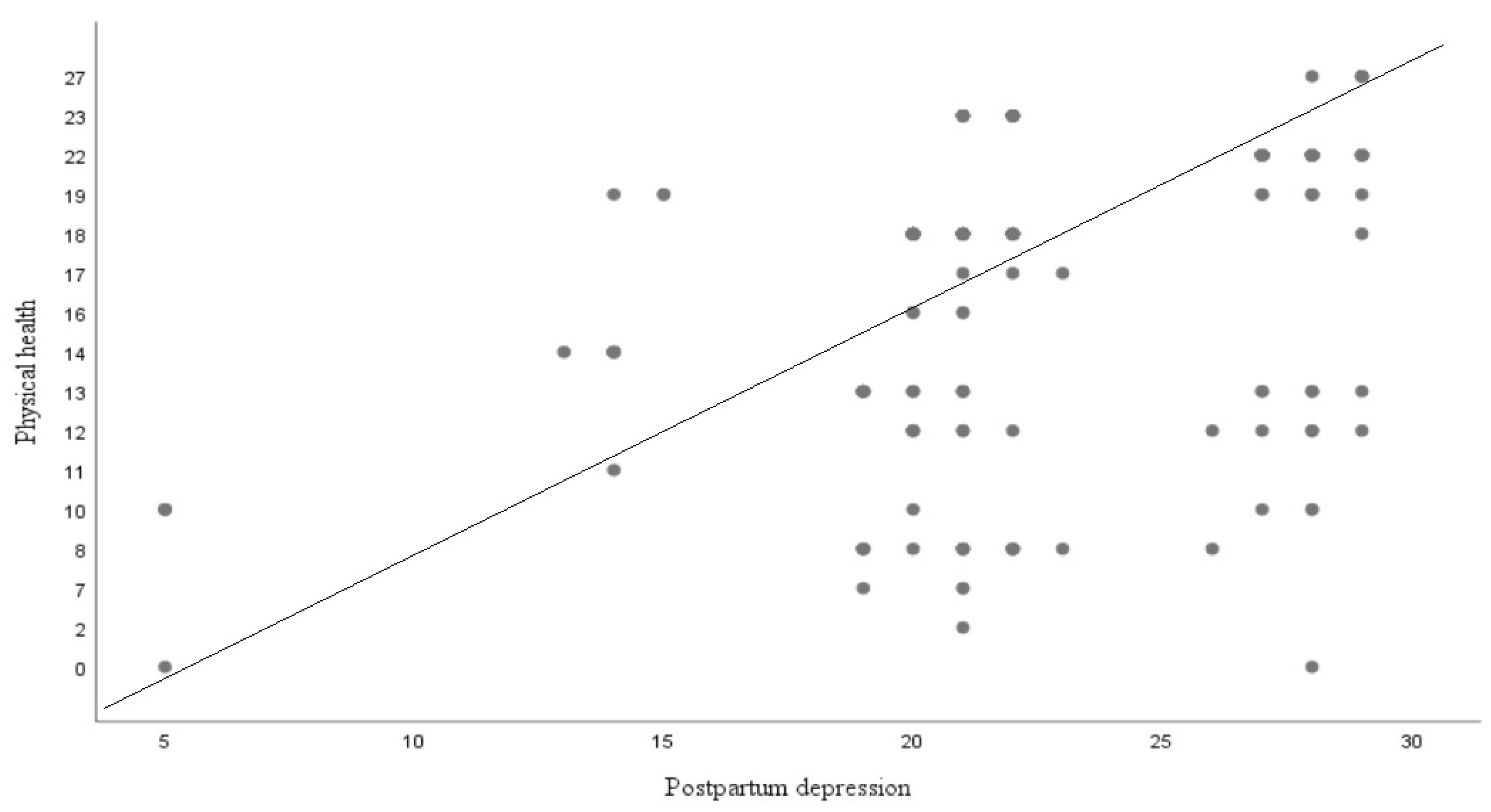
| PPD | −0.24 *** | 0.06 | 13.82 | 0.21 *** | 0.45 | 56.73 | −0.03 | 0.00 | 0.26 | −0.38 *** | 0.14 | 36.81 |
| Predictor Variables | PPD | INS | MH | PH | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | R2 | F | β | R2 | F | β | R2 | F | β | R2 | F | |
| PST | −0.38 *** | 0.14 | 36.81 | 0.16 * | 0.02 | 6.41 | 0.01 | 0.00 | 0.04 | −0.23 *** | 0.05 | 12.67 |
| FM | −0.21 ** | 0.04 | 10.59 | 0.12 | 0.01 | 3.30 | 0.18 ** | 0.03 | 8.04 | −0.20 ** | 0.04 | 9.04 |
| FR | −0.33 *** | 0.11 | 28.37 | 0.09 | 0.01 | 2.15 | −0.08 | 0.00 | 0.07 | −0.22 ** | 0.04 | 11.34 |
| SO | −0.31 *** | 0.09 | 23.03 | 0.15 * | 0.02 | 5.65 | −0.06 | 0.00 | 0.84 | −0.14 * | 0.01 | 4.78 |
| Models | R2 | β | F |
|---|---|---|---|
| Model 1 | 0.00 | 0.26 | |
| (PPD) | −0.03 | ||
| Model 2 | 0.00 | 0.13 | |
| (PPD) | −0.03 | ||
| (PSS) | 0.00 | ||
| Model 3 | 0.03 | 2.67 | |
| (PPD) | 0.99 ** | ||
| (PSS) | 0.32 * | ||
| (PPD)*(PSS) | −0.97 ** | ||
| Total R2 | 0.03 |
| Sources | SS | MS | F | Partial η2 |
|---|---|---|---|---|
| Education | 598.59 | 299.30 | 15.34 *** | 0.125 |
| Employment | 90.78 | 90.78 | 4.64 * | 0.021 |
| Education * Employment | 396.18 | 196.09 | 10.04 *** | 0.086 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamshaid, S.; Malik, N.I.; Ullah, I.; Saboor, S.; Arain, F.; De Berardis, D. Postpartum Depression and Health: Role of Perceived Social Support among Pakistani Women. Diseases 2023, 11, 53. https://doi.org/10.3390/diseases11020053
Jamshaid S, Malik NI, Ullah I, Saboor S, Arain F, De Berardis D. Postpartum Depression and Health: Role of Perceived Social Support among Pakistani Women. Diseases. 2023; 11(2):53. https://doi.org/10.3390/diseases11020053
Chicago/Turabian StyleJamshaid, Samrah, Najma Iqbal Malik, Irfan Ullah, Sundas Saboor, Fauzia Arain, and Domenico De Berardis. 2023. "Postpartum Depression and Health: Role of Perceived Social Support among Pakistani Women" Diseases 11, no. 2: 53. https://doi.org/10.3390/diseases11020053