
The Association of Combined Per- and Polyfluoroalkyl Substances and Metals with Allostatic Load Using Bayesian Kernel Machine Regression


1
Department of Built Environment, North Carolina A&T State University, Greensboro, NC 27411, USA
2
Environmental Health and Disease Laboratory, North Carolina A&T State University, Greensboro, NC 27411, USA
*
Author to whom correspondence should be addressed.
Diseases 2023, 11(1), 52; https://doi.org/10.3390/diseases11010052
Submission received: 28 January 2023
/
Revised: 1 March 2023
/
Accepted: 19 March 2023
/
Published: 22 March 2023
Abstract
:Background/Objective: This study aimed to investigate the effect of exposure to per- and polyfluoroalkyl substances (PFAS), a class of organic compounds utilized in commercial and industrial applications, on allostatic load (AL), a measure of chronic stress. PFAS, such as perfluorodecanoic acid (PFDE), perfluorononanoic acid (PFNA), perfluorooctane sulfonic acid (PFOS), perfluoroundecanoic acid (PFUA), perfluorooctanoic acid (PFOA), and perfluorohexane sulfonic acid (PFHS), and metals, such as mercury (Hg), barium (Ba), cadmium (Cd), cobalt (Co), cesium (Cs), molybdenum (Mo), lead (Pb), antimony (Sb), thallium (TI), tungsten (W), and uranium (U) were investigated. This research was performed to explore the effects of combined exposure to PFAS and metals on AL, which may be a disease mediator. Methods: Data from the National Health and Nutrition Examination Survey (NHANES) from 2007 to 2014 were used to conduct this study on persons aged 20 years and older. A cumulative index of 10 biomarkers from the cardiovascular, inflammatory, and metabolic systems was used to calculate AL out of 10. If the overall index was ≥ 3, an individual was considered to be chronically stressed (in a state of AL). In order to assess the dose-response connections between mixtures and outcomes and to limit the effects of multicollinearity and other potential interaction effects between exposures, Bayesian kernel machine regression (BKMR) was used. Results: The most significant positive trend between mixed PFAS and metal exposure and AL was revealed by combined exposure to cesium, molybdenum, PFHS, PFNA, and mercury (posterior inclusion probabilities, PIP = 1, 1, 0.854, 0.824, and 0.807, respectively). Conclusions: Combined exposure to metals and PFAS increases the likelihood of being in a state of AL.
1. Introduction
1.1. Background
The totality of exposures people endure throughout their lives and how those exposures affect health have been referred to as the exposome [1]. Although certain environmental exposures might lead to unfavorable health outcomes, little is understood about how these factors interact or synergize to affect the stress response system [2]. This is especially critical to understand when exposure to metals is mixed with exposure to per- and polyfluoroalkyl substances (PFAS).
The negative consequences of PFAS and mixed metals may be deleterious. They could have a long-term effect on the impacted populations’ social, educational, and economic advancement [3,4]. In many environments with high levels of chronic stress, several metals and PFAS co-exist at moderate to high levels.
Individuals maintain physiological balance through allostasis, which involves adjusting bodily characteristics to meet environmental requirements. Homeostasis describes health as a state in which all physiological parameters function within non-changing setpoints. Allostasis, on the other hand, states that there are no setpoints and that the demands of the moment will determine the normal values of markers. However, the body adjusts to the higher set point if the impediments persist [5]. When the setpoint is changed, people are said to be in a state of allostatic load. Allostatic load (AL), an index of persistent physiological stress, is the biological consequence of stress. AL depends on the assumption that repetitive activation of the hypothalamic-pituitary-adrenal (HPA) axis affects multiple organ systems [5,6,7,8].
The wear and tear on the body caused by ongoing exposure to stressors can be measured by AL, which combines markers from systems within the human body to form a comprehensive biological stress index. An adult’s well-being is negatively impacted by psychosocial stresses, such as poverty, racial inequality, lack of access to resources, and water and food insecurity, which may be combined with environmental factors to increase AL within populations.
At the individual and population levels, real-world human exposure to stressors is extraordinarily varied and temporally dynamic. Humans are constantly exposed to intricate chemical combinations of PFAS, metals, and other environmental pollutants [9,10]. Data analytics techniques provide a novel way to analyze the combined risk of various exposures in order to develop methodologies to properly identify and evaluate their impact on indices of stress, such as AL, because we do not fully understand the combinational nature of these exposures [11].
1.2. Human Exposure Pathways to PFAS and Metals
According to the Agency for Toxic Substances and Disease Registry at the Centers for Disease Control and Prevention (CDC), metals such as cadmium (Cd), arsenic (As), lead (Pb), and mercury (Hg) are among the top 10 most toxic substances. Most people are exposed to metals through ingestion (through water and food), inhalation (through cigarette smoke or industrial products), or skin contact (through paint or soil) [12]. For example, As comes in two forms: the inorganic form is highly toxic, while the organic form is not. Most people are exposed to inorganic As, which is found in soil and groundwater, through drinking water, often from unregulated private wells. Most people are exposed to organic arsenic, which is found in fish and shellfish, through ingestion [13]. In the United States, people of different races, ethnicities, and socioeconomic backgrounds experience widely varying degrees of exposure. For example, non-Hispanic blacks have higher Pb exposure than non-Hispanic whites [14].
Humans most commonly absorb toxic PFAS through their diets [15]. Inhalation of air or dust containing PFAS particles is another route of exposure. Over the past decade, there has been extensive research on the dangers of PFAS exposure for people’s health. The CDC, for example, has set limits on PFAS concentrations in drinking water (70 ppt for PFOA and PFOS).
PFAS spreads through many sites, including landfills and sites where PFAS has been processed. E-waste sites, for example, leach PFAS into groundwater, soil, and air, while wastewater treatment plants (WWTPs) release PFAS-laden effluent into rivers, lakes, and farms [16]. PFAS from treated or untreated effluent enters sewers, rivers, lakes, and oceans through aquatic ecosystems, making water the ultimate repository of PFAS in the environment [2].
Pregnant and parturient women, elderly people, children, and neonates are the most vulnerable to PFAS exposure, which can cause thyroid, lung, kidney, reproductive organ, metabolic, brain, and behavior disorders, obesity, type 2 diabetes, proteinuria, hematuria, immunosuppression, and adverse pregnancy outcomes [17].
1.3. Bayesian Kernel Machine Regression (BKMR): A Mechanism for Monitoring Multiple Environmental Exposures
Bobb et al. introduced Bayesian kernel machine regression (BKMR) for analyzing mixtures within the R statistical program [18]. By using the (bkmr) package for the R programming language, BKMR was created to estimate the health effects of pollutant mixtures and is used for toxicological, epidemiological, and other applications. It does this by using procedures from Gaussian predictive methods or hierarchical variable selection [18,19]. The estimation of health outcomes of the mixtures under kernel function is modeled on the exposure variables by adjusting for potential covariates or cofounder factors [20]. These procedures can address the possible collinearity of the mixtures’ components and test the exposures’ overall health effects [21].
Ultimately, BKMR modeling is a technique that (1) models the exposures and outcomes comprehensively, (2) evaluates the components of chemicals independently of the independent–dependent function, (3) evaluates the effects of mixtures of chemicals, and (4) distinguishes the necessary chemical mixtures for any dataset that is simulated [19,21]. BKMR is also used to solve the challenges encountered when evaluating the health impacts of chemical mixtures (i.e., PFAS and metals). In epidemiological and toxicological studies, BKMR helps solve problems such as collinearity and strong correlations between exposures [22]. BKMR uses variable selection that produces and estimates posterior inclusion probabilities (PIPs) values, which measure the values of variable importance for each exposure in a mixture [18,20].
This study using BKMR hypothesizes that exposure to metals and PFAS is associated with high levels of AL. PFAS and metals were chosen due to the unique opportunity to assess combined exposures to organic and inorganic contaminants, the extensive research on both groups of contaminants with National Health and Nutrition Examination Survey (NHANES) data, and the vast historical and emerging research related to these contaminants. To test this hypothesis, data from the NHANES were used to identify the factors most critical in combined exposures to PFAS and metals.
2. Materials and Methods
2.1. Study Cohort and Design
Data from the NHANES 2007–2014 of adults aged 20 years and over were utilized in this investigation. This dataset is a representative sample of non-institutionalized people residing in all 50 U.S. states and the District of Columbia. The U.S. Centers for Disease Control and Prevention (CDC) collected the data, which are available in two-year cycles and include multi-year, stratified, multi-stage, and clustered samples. The population of the United States is represented by the statistics for four cycles within 2007–2014.
Selected individuals in the NHANES underwent a physical examination and an interview. The participants’ blood was extracted, and samples were sent to a laboratory for evaluation.
On the NHANES website of the CDC, additional descriptions and information about the study, as well as the steps and processes involved in data collection, are provided.
The association between the various PFAS/metals concentrations and AL levels was examined using weighted data in order to produce sample estimates, which reflect how many people in the U.S. population one individual represents.
2.2. PFAS and Metals Measurements
There were two examination sessions each day. Exams in the morning, afternoon, or evening were randomly assigned to participants. After fasting for nine hours, participants were instructed to consume 75 g of dextrose (10 oz. of glucose solution) within 10 min after the initial blood draw. After the first blood draw was taken, a second blood sample was taken [23].
2.2.1. PFAS Quantification
At the mobile examination center (MEC), the CDC gathered blood samples for laboratory analysis to evaluate serum for PFAS. Polypropylene or polyethylene containers were used to store the serum samples. The vials were subsequently shipped to several laboratories across the country. Sample analysis was performed at every survey location under the same conditions, owing to the controlled environments at separate facilities.
In order to concentrate the analytes (PFAS) in a solid-phase extraction column, one aliquot of 50 mL of serum was injected into a commercial column switching system after being diluted with formic acid.
High-performance liquid chromatography was used to separate the analytes from one another and the other serum constituents.
A negative-ion Turbo Ion Spray (TIS) ionization source was utilized for detection and quantification (DOQ). Tandem mass spectrometry was used to change liquid-phase ions into gas-phase ions, utilizing a variation of the electrospray ionization source.
These PFAS can be quickly detected in human serum using this technique, with detection limits in the low parts per billion (ppb or ng/mL) range [24].
An imputed value was placed in the analyte results field for analytes with analytic results below the lower limit of detection; 0.10/square root of 2 = 0.07 was the lower limit of detection divided by the square root of 2. Thus, the LOD for each PFAS was 0.10 or 0.07.
2.2.2. Metals Quantification
Inductively coupled mass spectrometry (ICP-MS) measured metals in diluted whole blood. ICP-MS is a validated technique for analyzing metals in biological media.
All data set metal analytes had the same detection limits. An imputed fill value was placed in the analyte results field for analytes below the lower limit of detection using the equation: lower limit of detection divided by the square root of 2 [23].The NHANES Laboratory Procedures Manual describes specimen collection and processing in detail [24]. The National Center for Environmental Health (NCEH) of the CDC’s Division of Laboratory Sciences performed metal assays on whole blood samples for the NHANES 2007–2014. Blood metals were identified and quantified using the inductively coupled plasma mass spectrometry method No. ITB0001A.
2.3. Determining Allostatic Load Levels
This study’s AL was determined using physiological evaluations of 10 health indicators or biomarkers. The biomarkers included systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol (TC), high-density lipoprotein (HDL) cholesterol, glycosylated hemoglobin (HbA1c), albumin (Alb), triglycerides (TG), body mass index (BMI), creatinine clearance (CLCR), and C-reactive protein (CRP). Measures of AL were determined by calculating the cutoffs for various biomarkers based on their distribution within the database. All biomarkers were transformed into quartiles based on the data distribution. The top 25% of the distribution for each marker was designated as high risk for (1) C-reactive protein (CRP), (2) triglycerides (TG), (3) total cholesterol (TC), (4) systolic blood pressure (SBP), (5) diastolic blood pressure (DBP), (6) body mass index, and (7) glycosylated hemoglobin. For the other markers where high risk is determined by lower values, the bottom 25% of the distribution was used. These markers included (1) urinary albumin (Alb), (2) creatinine clearance (CLCR), and (3) high-density lipoprotein (HDL) cholesterol. High risk for each marker was assigned a value of 1, with low risk assigned a value of 0 to obtain a total AL index out of 10. An AL value greater than 3/10 was considered elevated, as indicated by the prior work of the team and others [2,25,26,27].
2.4. Data Analysis
We used BKMR with the hierarchical variable selection method due to highly correlated variables and collinearity in the datasets. We utilized the BKMR model in the R program using the R package (bkmr) to simulate the dataset. In this study, the model evaluated the impacts of mixtures or multipollutant exposures (e.g., PFAS and metals such as cadmium, cobalt, cesium, molybdenum, lead, etc.) by comparing the implementation of statistical and characteristics methods using the (kmbayes) function.
BKMR Modeling for Binary Outcomes
Combining data sources from various samples, including probability and nonprobability samples, is appropriate when using Bayesian inference. The use of Bayesian inference has various benefits. It first enables the estimation of complicated models and the quantification of uncertainty measurements.
The likelihood function can be used to analyze sample units based on probability.
As the probability sample size grows, it is primarily set up to give these units priority in the posterior calculations. Third, it enables posterior estimates to be more effective and efficient than estimates obtained from tiny probability-only samples, with less uncertainty [19,28].
We implemented kernel machine regression (KMR) for binary outcomes, as follows:
where h is a flexible function of the predictor variables zi1, ..., ziM, x is a vector of covariates (β is the corresponding vector of coefficients), and h is the cumulative distribution function (CDF) for the standard normal distribution. The outcome Yi is a binary (0/1) variable. Predictors z were the exposure variables, and h(.) was the exposure-response function. A kernel machine representation was used to model the function h in order to capture complex, non-additive, non-linear exposure-response interactions.
Φ − 1(P(Yi = 1)) = h(zi1, …, ziM) + βxi, I = 1, …, n
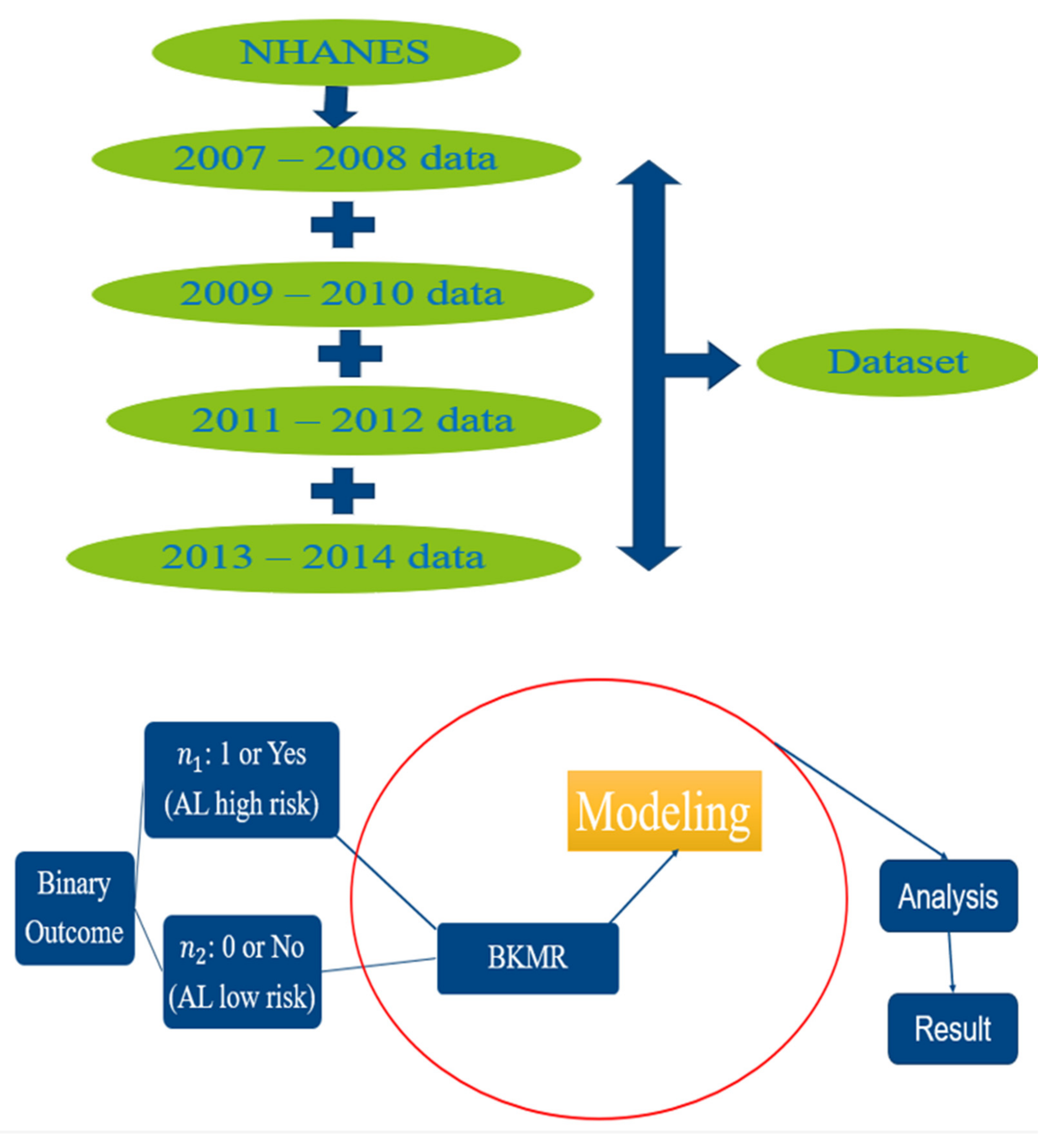
The outcome variable in this study was AL. AL index values ≥ 3 were considered high risk, with values < 3 considered low risk. Those who were high risk were assigned a 1 in the dataset, while those who were low risk were assigned a 0. Binary outcomes were performed by applying the BKMR package using the probit model for convenience of computation and to overcome some of the issues that may arise in the dataset, such as collinearity under Bayesian inference [29]. Posterior inclusion probabilities (PIPs), which offer a gauge of the variable importance of each exposure, were extracted and plotted. All models were adjusted for sex, age, smoking, physical activity, ethnicity, occupation, income, alcohol consumption, education, birthplace, and time in the U.S. The analysis within this study was conducted using R software, version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria). A flow chart containing all the steps performed in the analysis can be found in Figure 1 below.
3. Results
Table 1 below provides the posterior inclusion probabilities (PIPs), which measure the percentage of the data that backs the inclusion of exposure or variable in the model. In other words, it quantifies the variable significance to be included within the model. The exposures to be included in the model were PFNA, PFUA, PFOA, PFHS, mercury, cesium, and molybdenum.
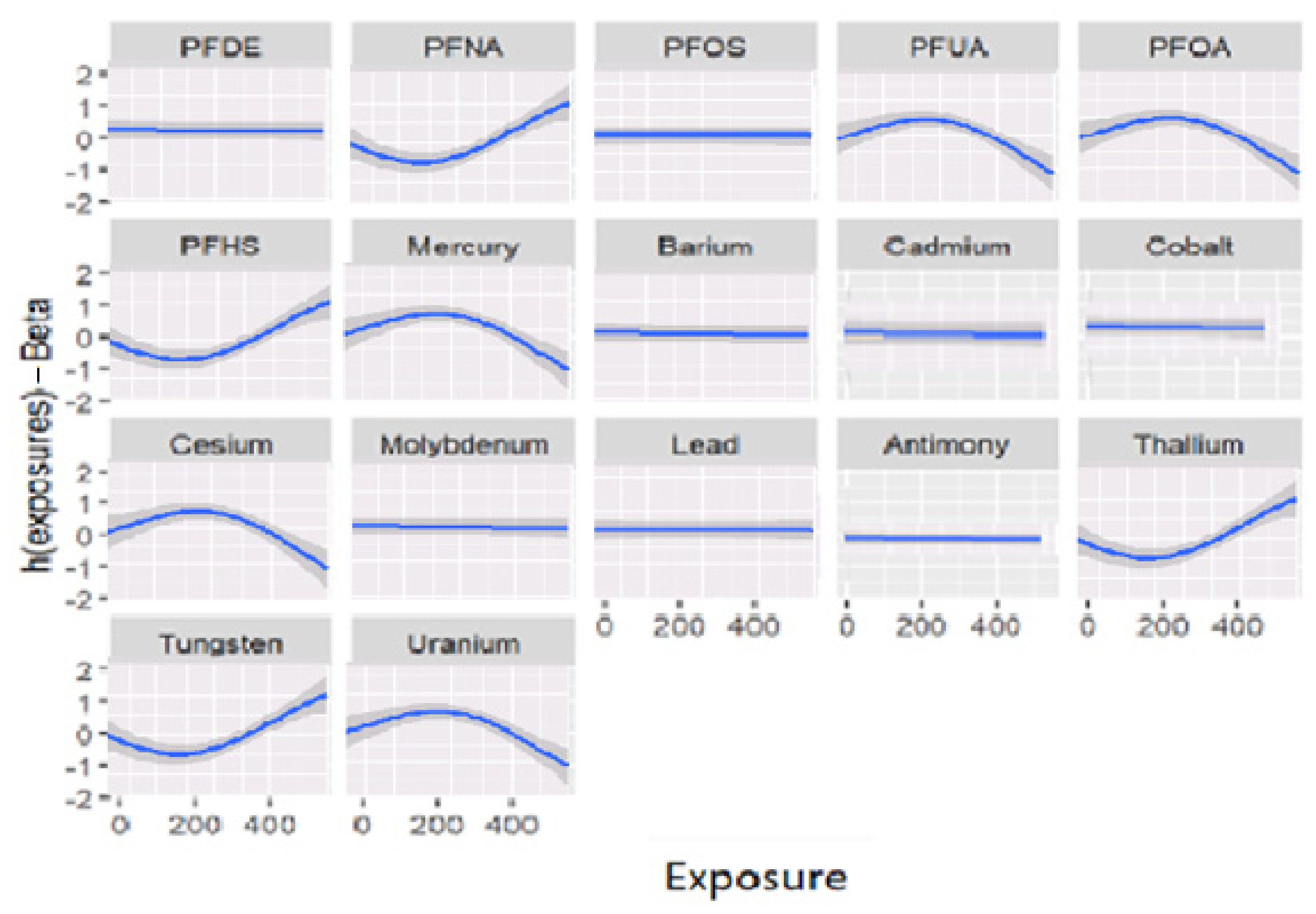
Figure 2 shows the association between the response variable and each individual exposure included in the model, which is known as the univariate relationship. The other exposures were fixed at their median values, and the covariates were fixed as constant. This figure shows that the association of some variables is not significant or has no association with the outcome. In other words, Figure 2 below shows the univariate independent-response association (each individual independent and dependent—AL association) by fixing the remaining exposures to their median, with the covariates being constant. The associations in Figure 2 present the relationship of exposures with responses when the model is adjusted for covariates (sex, age, smoking, physical activity, ethnicity, occupation, income, alcohol consumption, education, birthplace, and time in the U.S.). For instance, exposure to PFNA, PFUA, PFOA, PFHS, mercury, cesium, thallium, tungsten, and uranium are associated with AL, with some of these contaminants having sharper inclines, indicating different levels of exposure. Uphill on the graphs represents a higher level of exposure, and downhill shows lower levels of exposure. In other words, concentration values increase and decrease depending on the amount of exposure.
In Table 2, the PIPs with the highest values are explored using critical sociodemographic and behavioral variables. The six highest PIPs were molybdenum, cesium, mercury, PFNA, PFOA, and PFHS.
Table 3 explores mean AL levels by ethnicity and age group. This was performed to give context to the results. The results indicated that both ethnicity and age are significantly related to AL.
Table 4 explores the correlation between all the critical environmental exposures in this study. The results demonstrate that the strongest correlation exists between cesium and mercury.
4. Discussion
The main PFAS have extensive half-lives in humans and are physiologically and biologically persistent. The gap in the body of knowledge on the impact of environmental pollutants on stress and health is partly filled by attempting to understand the relationship between the cumulative physiological burden of stress (AL) and PFAS and metals [30]. This is especially true because stressors are constantly present in people’s lives, and the cumulative effect on health is apparent when resilience is lacking [30,31].
BKMR provides a way to address the potential multicollinearity among numerous PFAS and metal exposures, which cannot be resolved using traditional regression modeling. Based on a comprehensive analysis of the NHANES 2007–2014 data, we assessed the relationships between metal and PFAS exposures and AL among a nationally representative sample of adults. The study’s findings supported the main hypothesis, which stated that exposure to a combination of PFAS and metals is strongly linked to AL. This expands prior work by the team, which found that metals and PFAS are associated with AL using simpler modeling techniques [2,30].
In this study, combined exposure analyses of PFAS and metals showed a significant positive association between mixed PFAS and metal exposure and AL, to which cesium, molybdenum, PFHS, PFNA, and mercury contributed the most (PIP = 1, 1, 0.854, 0.824, and 0.807, respectively). In addition, the correlation between selected metals and PFAS (Table 4), with some negatively and others positively associated, suggests that the relationships between these factors are varied and require dynamic modeling techniques to capture the combined relationship appropriately. In the BKMR model, a substantial positive association between combined metal and PFAS exposure and AL existed for PFNA, PFUA, PFHS, thallium, and tungsten.
The univariate relationship between AL and each exposure in the model is depicted in Figure 2. All other exposures and covariates were held constant at their respective median values. The results demonstrated which variables, in combination, were not significantly associated with AL. These models were adjusted for confounding factors, and the associations between exposures and responses became clear. Exposures to PFNA, PFUA, PFOA, PFHS, mercury, cesium, thallium, tungsten, and uranium, to name a few, are all associated with AL; some of the graphs had steeper slopes than others, reflecting the fact that there were varying degrees of association between variables.
The molecular processes or toxicological pathways that underlie the relationships between human exposure to PFAS and metals and AL are not fully understood. The means by which exposure to PFAS and metals brings forth adverse health outcomes may be via AL. Simply put, AL may be the mediator between exposure to multiple contaminants and adverse health outcomes [2,32], such as heart disease, high blood pressure, metabolic syndrome, obesity, and arthritis [33].
Table 2 shows that the mean levels of the contaminants of interest varied by ethnicity; for example, Asians had high mean levels of molybdenum, cesium, and PFUA, with values of 65.9, 537, and 0.26, respectively. Blacks had higher mean mercury levels, and Whites had higher PFOA and PFHS levels than the other groups. These varied exposure levels by ethnicity speak to the variability of the contaminants of interest and the dynamism of exposure in various environments.
Within our results, compared to those of the White, Asian, and Hispanic ethnicities, non-Hispanic Blacks had greater rates of high AL. Table 2 and Table 3 demonstrate that across all age groups, high stressors in addition to lower levels of resilient behavior, such as physical activity, exist. This may play a role in adverse health outcomes driven by AL.
Understanding the social implications of AL may help explain some of the results of this study. For instance, many ethnic groups in the U.S. experience prejudice, face poor wage employment disproportionately, and are susceptible to chronic stress [34]. In the context of multiple environmental exposures, these factors may play a role in promoting AL. When this is intertwined with inadequate healthcare, the health burden on communities exposed to combinations of exposures and health outcomes is vast [34]. Non-Hispanic Whites in the US often have lower levels of AL than minority ethnic groups, as demonstrated in Table 3, across all age groups [35]. This may partly explain the lower disease burden within this group compared to the other groups.
Age is a critical variable in AL levels, with younger people typically having lower AL levels than older persons [36]. Our results, as shown in Table 3, confirm this. Continuous stressor exposure over the course of a lifetime can promote inflammation and oxidative stress, which can lead to physiological impairment and promote disease [37]. Among these is cardiovascular disease, the leading killer in the U.S. and in the world [38]. As people become older, their biological sensitivities to chronic stress vary, and the body’s physiological response system also changes naturally. As a result, biological regulation may deteriorate over time, which may result in an unhealthy physical state. This scenario has the potential to cause mortality over time, especially in elderly people [35].
The literature on AL by sex varies. Some research has shown that AL levels are often lower in men who hold professional positions, such as managers and directors. On the contrary, Rogers et al. reported that men with higher levels of education are likely to have higher AL [39]. According to several studies, women who obtained higher levels of education and simultaneously held professional jobs as managers had a higher prevalence of AL [40]. People who experience continual stress due to issues such as unemployment and poverty are more likely to engage in excessive drinking, smoking, and eating, which leads to obesity, poor sleep, and, of course, increased AL [41]; our results in Table 2 and Table 3 support this.
According to a study by Petrovic et al., drinking, smoking, and eating too much sodium were all associated with a higher risk of developing AL. Meanwhile, physical activity and a vegetarian diet were linked to a reduction in AL [40]; our results in Table 2 support these findings.
Very few laboratory studies have examined combined exposure to PFAS and metals. Therefore, future experimental and human investigations are required to further corroborate our findings and to investigate the probable mechanism for the health impacts of PFAS and metal exposure on AL, given the dearth of laboratory data and the cross-sectional design of our study. The limitation of this design means that temporality cannot be inferred. A longitudinal study would offer better insight into these exposures and health outcomes.
5. Conclusions
PFAS and other toxicants, such as metals, interact in the human body to produce AL. The mixture of PFAS and metals is critical to understand, as they may, in combination, bring forth adverse health outcomes via AL. When PFAS are found in the body alongside metals, our results indicate that their combined toxicity needs to be considered, with cesium, molybdenum, mercury, PFHS, and PFNA especially being of concern. More research is required into this matter. Research into the levels of exposure to multiple pollutants required to bring about AL must be explored if we are to gain an understanding of the real-world mixture concentrations that bring forth disease. This is of paramount significance for at-risk communities because their members lack the resources to effectively manage stress and/or avoid exposure to environmental contaminants.
Author Contributions
Conceptualization, E.O.-G.; methodology, T.B. and E.O.-G.; formal analysis, T.B. and E.O.-G.; investigation, T.B. and E.O.-G.; resources, E.O.-G.; data curation, T.B. and E.O.-G.; writing—original draft preparation, T.B.; writing—review and editing, T.B. and E.O.-G.; supervision, E.O.-G.; project administration, E.O.-G.; funding acquisition, E.O.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by NHLBI grant R25 HL105400 and the BCSP Foundation.
Institutional Review Board Statement
This study did not require IRB approval because de-identified secondary data were used. In the collection of the data by the Centers for Disease Control and Prevention, the study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Centers for Disease Control and Prevention.
Informed Consent Statement
Not applicable.
Data Availability Statement
The NHANES dataset is publicly available online, accessible at cdc.gov/nchs/nhanes/index.htm (accessed on 12 January 2023).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wild, C.P. The exposome: From concept to utility. Int. J. Epidemiol. 2012, 41, 24–32. [Google Scholar] [CrossRef]
- Bashir, T.; Obeng-Gyasi, E. The Association between Multiple Per- and Polyfluoroalkyl Substances’ Serum Levels and Allostatic Load. Int. J. Environ. Res. Public Health 2022, 19, 5455. [Google Scholar] [CrossRef] [PubMed]
- Szyf, M.; McGowan, P.; Meaney, M.J. The social environment and the epigenome. Environ. Mol. Mutagen. 2008, 49, 46–60. [Google Scholar] [CrossRef] [PubMed]
- Caplin, A.; Ghandehari, M.; Lim, C.; Glimcher, P.; Thurston, G. Advancing environmental exposure assessment science to benefit society. Nat. Commun. 2019, 10, 1236. [Google Scholar] [CrossRef] [Green Version]
- Juster, R.-P.; McEwen, B.S.; Lupien, S.J. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci. Biobehav. Rev. 2010, 35, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Utumatwishima, J.N.; Baker, R.L.; Bingham, B.A.; Chung, S.T.; Berrigan, D.; Sumner, A.E. Stress Measured by Allostatic Load Score Varies by Reason for Immigration: The Africans in America Study. J. Racial Ethn. Health Disparities 2018, 5, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Cacioppo, J.T.; Berntson, G.G.; Adolphs, R.; Carter, C.S.; Davidson, R.J.; McClintock, M.; McEwen, B.S.; Meaney, M.; Schacter, D.L.; Sternberg, E.M.; et al. Protective and Damaging Effects of Stress Mediators. N. Engl. J. Med. 1998, 338, 171–179. [Google Scholar] [CrossRef] [Green Version]
- Duong, M.T.; Bingham, B.A.; Aldana, P.C.; Chung, S.T.; Sumner, A.E. Variation in the Calculation of Allostatic Load Score: 21 Examples from NHANES. J. Racial Ethn. Health Disparities 2016, 4, 455–461. [Google Scholar] [CrossRef]
- de Hollander, A.E.M.; Melse, J.M.; Lebret, E.; Kramers, P.G.N. An Aggregate Public Health Indicator to Represent the Impact of Multiple Environmental Exposures. Epidemiology 1999, 10, 606–617. [Google Scholar] [CrossRef] [Green Version]
- Su, F.; Zeeshan, M.; Xiong, L.-H.; Lv, J.-Y.; Wu, Y.; Tang, X.-J.; Zhou, Y.; Ou, Y.-Q.; Huang, W.-Z.; Feng, W.-R.; et al. Co-exposure to perfluoroalkyl acids and heavy metals mixtures associated with impaired kidney function in adults: A community-based population study in China. Sci. Total Environ. 2022, 839, 156299. [Google Scholar] [CrossRef] [PubMed]
- Bobb, J.F.; Henn, B.C.; Valeri, L.; Coull, B.A. Statistical software for analyzing the health effects of multiple concurrent exposures via Bayesian kernel machine regression. Environ. Health 2018, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Tchounwou, P.B.; Yedjou, C.G.; Patlolla, A.K.; Sutton, D.J. Heavy metal toxicity and the environment. Mol. Clin. Environ. Toxicol. 2012, 3, 133–164. [Google Scholar]
- Stone, J.; Sutrave, P.; Gascoigne, E.; Givens, M.B.; Fry, R.C.; Manuck, T.A. Exposure to toxic metals and per- and polyfluoroalkyl substances and the risk of preeclampsia and preterm birth in the United States: A review. Am. J. Obstet. Gynecol. MFM 2021, 3, 100308. [Google Scholar] [CrossRef] [PubMed]
- Obeng-Gyasi, E.; Roostaei, J.; Gibson, J.M. Lead Distribution in Urban Soil in a Medium-Sized City: Household-Scale Analysis. Environ. Sci. Technol. 2021, 55, 3696–3705. [Google Scholar] [CrossRef] [PubMed]
- Genualdi, S.; Beekman, J.; Carlos, K.; Fisher, C.M.; Young, W.; DeJager, L.; Begley, T. Analysis of per- and poly-fluoroalkyl substances (PFAS) in processed foods from FDA’s Total Diet Study. Anal. Bioanal. Chem. 2021, 414, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Tansel, B. PFAS use in electronic products and exposure risks during handling and processing of e-waste: A review. J. Environ. Manag. 2022, 316, 115291. [Google Scholar] [CrossRef]
- Garg, S.; Kumar, P.; Mishra, V.; Guijt, R.; Singh, P.; Dumée, L.F.; Sharma, R.S. A review on the sources, occurrence and health risks of per-/poly-fluoroalkyl substances (PFAS) arising from the manufacture and disposal of electric and electronic products. J. Water Process Eng. 2020, 38, 101683. [Google Scholar] [CrossRef]
- Bobb, J.F.; Valeri, L.; Henn, B.C.; Christiani, D.C.; Wright, R.O.; Mazumdar, M.; Godleski, J.J.; Coull, B.A. Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 2015, 16, 493–508. [Google Scholar] [CrossRef] [Green Version]
- George, E.I.; McCulloch, R.E. Approaches for Bayesian variable selection. Stat. Sin. 1997, 7, 339–373. [Google Scholar]
- Stafoggia, M.; Breitner, S.; Hampel, R.; Basagaña, X. Statistical Approaches to Address Multi-Pollutant Mixtures and Multiple Exposures: The State of the Science. Curr. Environ. Health Rep. 2017, 4, 481–490. [Google Scholar] [CrossRef]
- Sun, Z.; Tao, Y.; Li, S.; Ferguson, K.K.; Meeker, J.D.; Park, S.K.; Batterman, S.A.; Mukherjee, B. Statistical strategies for constructing health risk models with multiple pollutants and their interactions: Possible choices and comparisons. Environ. Health 2013, 12, 85. [Google Scholar] [CrossRef] [Green Version]
- Bobb, J. Introduction to Bayesian Kernel Machine Regression and the bkmr R Package. 2017. Available online: https://jenfb.github.io/bkmr/overview.html (accessed on 16 February 2023).
- Centers for Disease Control and Prevention. Laboratory Procedure Manual for Perfluoroalkyl and Polyfluoroalkyl Substances (NHANES 2013−2014); (Method No. 6304.06); CDC: Atlanta, GA, USA, 2014. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2013-2014/labmethods/PFAS_H_MET.pdf (accessed on 16 February 2023).
- Mottaleb, M.A.; Petriello, M.C.; Morris, A.J. High-Throughput UHPLC-MS/MS Measurement of Per- and Poly-Fluorinated Alkyl Substances in Human Serum. J. Anal. Toxicol. 2020, 44, 339–347. [Google Scholar] [CrossRef]
- Obeng-Gyasi, E.; Obeng-Gyasi, B. Chronic Stress and Cardiovascular Disease among Individuals Exposed to Lead: A Pilot Study. Diseases 2020, 8, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeng-Gyasi, E. Cumulative Effects of Low-Level Lead Exposure and Chronic Physiological Stress on Hepatic Dysfunction—A Preliminary Study. Med. Sci. 2020, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Bashir, T.; Asiseh, F.; Jefferson-Moore, K.; Obeng-Gyasi, E. The Association of Per- and Polyfluoroalkyl Substances Public Health Serum Levels and Allostatic Load by Country of Birth and the Length of Time in the United States. Int. J. Environ. Res. Public Health 2022, 19, 9438. [Google Scholar] [CrossRef]
- Sakshaug, J.W.; Wiśniowski, A.; Ruiz, D.A.P.; Blom, A.G. Supplementing Small Probability Samples with Nonprobability Samples: A Bayesian Approach. J. Off. Stat. 2019, 35, 653–681. [Google Scholar] [CrossRef] [Green Version]
- Scott, J.G.; Berger, J.O. Bayes and empirical-Bayes multiplicity adjustment in the variable-selection problem. Ann. Stat. 2010, 38, 2587–2619. [Google Scholar] [CrossRef] [Green Version]
- Rodriquez, E.J.; Livaudais-Toman, J.; Gregorich, S.E.; Jackson, J.S.; Nápoles, A.M.; Pérez-Stable, E.J. Relationships between allostatic load, unhealthy behaviors, and depressive disorder in U.S. adults, 2005–2012 NHANES. Prev. Med. 2018, 110, 9–15. [Google Scholar] [CrossRef]
- Wadhwa, P.D.; Culhane, J.F.; Rauh, V.; Barve, S.S.; Hogan, V.; Sandman, C.A.; Hobel, C.J.; Chicz-DeMet, A.; Dunkel-Schetter, C.; Garite, T.J.; et al. Stress, infection and preterm birth: A biobehavioural perspective. Paediatr. Périnat. Epidemiol. 2001, 15, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Logan, J.G.; Barksdale, D.J. Allostasis and allostatic load: Expanding the discourse on stress and cardiovascular disease. J. Clin. Nurs. 2008, 17, 201–208. [Google Scholar] [CrossRef]
- Mattei, J.; Demissie, S.; Falcon, L.M.; Ordovas, J.M.; Tucker, K. Allostatic load is associated with chronic conditions in the Boston Puerto Rican Health Study. Soc. Sci. Med. 2010, 70, 1988–1996. [Google Scholar] [CrossRef] [Green Version]
- Nelson, K.M.; Reiber, G.; Kohler, T.; Boyko, E.J. Peripheral arterial disease in a multiethnic national sample: The role of conventional risk factors and allostatic load. Ethn. Dis. 2007, 17, 669. [Google Scholar] [PubMed]
- Slade, G.D.; Sanders, A.E.; By, K. Role of Allostatic Load in Sociodemographic Patterns of Pain Prevalence in the U.S. Population. J. Pain 2012, 13, 666–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obeng-Gyasi, E. Factors associated with elevated Per- and Polyfluoroalkyl substances serum levels in older adults. Aging Health Res. 2022, 2, 100086. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Johnston, M.; Hayward, M.; Seeman, T. Age differences in allostatic load: An index of physiological dysregulation. Exp. Gerontol. 2003, 38, 731–734. [Google Scholar] [CrossRef]
- Salazar, C.R.; Strizich, G.; Seeman, T.E.; Isasi, C.R.; Gallo, L.C.; Avilés-Santa, L.M.; Cai, J.; Penedo, F.J.; Arguelles, W.; Sanders, A.E.; et al. Nativity differences in allostatic load by age, sex, and Hispanic background from the Hispanic Community Health Study/Study of Latinos. SSM-Popul. Health 2016, 2, 416–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C.R.; Moore, J.X.; Gilmore, D.R.; Petersen, E.; Brooks, E.; Kennedy, C.; Thorpe, R.J. Investigation of Differences in Allostatic Load among Black Men by Level of Educational Attainment: High School Graduates Experience the Highest Levels of Stress. Int. J. Environ. Res. Public Health 2022, 19, 3580. [Google Scholar] [CrossRef]
- Petrovic, D.; Pivin, E.; Ponte, B.; Dhayat, N.; Pruijm, M.; Ehret, G.; Ackermann, D.; Guessous, I.; Younes, S.E.; Pechère-Bertschi, A.; et al. Sociodemographic, behavioral and genetic determinants of allostatic load in a Swiss population-based study. Psychoneuroendocrinology 2016, 67, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Flow chart for methodology.

Figure 2.
Univariate exposure-response functions and 95% confidence intervals for each metal and PFAS exposure, with others fixed at the median.
Figure 2.
Univariate exposure-response functions and 95% confidence intervals for each metal and PFAS exposure, with others fixed at the median.


{kind=link}
{kind=link}
Table 1.
Posterior inclusion probability (PIP) and comparison of four models (BKMR, Oracle, Linear, and True) of overall health effects on the response variable (AL) by exposures.
Table 1.
Posterior inclusion probability (PIP) and comparison of four models (BKMR, Oracle, Linear, and True) of overall health effects on the response variable (AL) by exposures.
| Overall Effects | ||||||
|---|---|---|---|---|---|---|
| Models | ||||||
| BKMR 1 | Oracle 2 | Linear 3 | TRUE 4 | |||
| 0.680 | −0.539 | −0.572 | −0.843 | |||
| Individual effect | ||||||
| Models | ||||||
| variable # | variable | PIP 5 | BKMR | Oracle | Linear | TRUE |
| 1 | PFDE | 0.700 | 0.068 | 0.153 | −0.693 | −1.784 |
| 2 | PFNA | 0.824 | 0.023 | 0.239 | 0.124 | 0.264 |
| 3 | PFOS | 0.651 | 0.087 | −0.131 | 0.032 | 0.059 |
| 4 | PFUA | 0.795 | 0.019 | 0.098 | 0.235 | −0.324 |
| 5 | PFOA | 0.754 | 0.033 | 0.955 | 0.015 | −0.021 |
| 6 | PFHS | 0.854 | 0.115 | −0.169 | −0.037 | −0.068 |
| 7 | Mercury | 0.807 | 0.022 | −0.278 | −0.084 | −0.144 |
| 8 | Barium | 0.719 | 0.014 | 0.427 | 0.033 | 0.054 |
| 9 | Cadmium | 0.727 | 0.390 | 0.356 | 0.114 | 0.199 |
| 10 | Cobalt | 0.706 | 0.022 | −0.038 | −0.169 | −0.273 |
| 11 | Cesium | 1.000 | 0.350 | 0.101 | 0.003 | 0.008 |
| 12 | Molybdenum | 1.000 | 0.238 | −0.386 | 0.004 | 0.006 |
| 13 | Lead | 0.674 | 0.035 | 0.736 | −0.008 | −0.036 |
| 14 | Antimony | 0.701 | 0.203 | −0.258 | 0.343 | 0.543 |
| 15 | Thallium | 0.749 | 0.044 | −0.163 | 0.419 | 0.663 |
| 16 | Tungsten | 0.762 | 0.012 | −0.195 | −0.349 | −0.689 |
| 17 | Uranium | 0.723 | 0.016 | −0.413 | 4.204 | 7.213 |
Note: 1 Bayesian kernel machine regression (BKMR); 2 Oracle model that uses glm (generalized linear model); 3 Linear model; 4 True model using all variables with no adjustment; 5 PIP (posterior inclusion probability), which quantifies the importance of the variable in variable selection.
Table 2.
Metals (molybdenum, cesium, and mercury) and PFAS (PFNA, PFOA, and PFHS) means by critical study variables.
Table 2.
Metals (molybdenum, cesium, and mercury) and PFAS (PFNA, PFOA, and PFHS) means by critical study variables.
| Metals and PFAS | ||||||
|---|---|---|---|---|---|---|
| Variable | Molybdenum | Cesium | Mercury | PFNA | PFOA | PFHS |
| Activities | Mean | |||||
| 1 day | 57.80 | 5.08 | 0.59 | 0.14 | 0.98 | 0.80 |
| 2 days | 76.70 | 4.72 | 0.62 | 0.13 | 0.89 | 0.77 |
| 3 days | 55.70 | 5.05 | 0.57 | 0.13 | 0.85 | 0.70 |
| 4 days | 45.30 | 5.20 | 1.33 | 0.12 | 0.84 | 0.72 |
| 5 days | 60.40 | 4.26 | 0.57 | 0.13 | 0.90 | 0.79 |
| 6 days | 40.10 | 3.56 | 0.44 | 0.13 | 1.00 | 0.82 |
| 7 days | 57.40 | 3.60 | 0.63 | 0.14 | 0.86 | 0.67 |
| Smoke | ||||||
| yes | 51.70 | 4.95 | 0.56 | 0.13 | 0.93 | 0.78 |
| no | 61.00 | 5.03 | 0.64 | 0.14 | 0.81 | 0.67 |
| AL | ||||||
| high | 67.54 | 5.35 | 0.60 | 0.13 | 0.83 | 0.73 |
| low | 49.45 | 4.73 | 0.61 | 0.13 | 0.88 | 0.71 |
| Ethnicity | ||||||
| Mexican | 59.10 | 5.07 | 0.58 | 0.09 | 0.78 | 0.59 |
| Black | 57.70 | 4.78 | 0.66 | 0.14 | 0.84 | 0.72 |
| White | 50.20 | 4.89 | 0.54 | 0.12 | 0.97 | 0.82 |
| Hispanic | 61.80 | 5.19 | 0.43 | 0.11 | 0.80 | 0.59 |
| Other and Asian | 65.90 | 5.37 | 0.60 | 0.26 | 0.65 | 0.60 |
| Sex | ||||||
| Female | 54.30 | 4.76 | 0.63 | 0.12 | 0.76 | 0.56 |
| Male | 59.90 | 5.23 | 0.58 | 0.14 | 0.97 | 0.88 |
Table 3.
AL means for ethnicities by age group.
| Age Groups | |||
|---|---|---|---|
| 20 to 39 | 40 to 59 | 60 and older | |
| Ethnicity | AL mean | ||
| Mexican | 2.9 | 3.49 | 3.58 |
| Black | 3.32 | 3.92 | 3.83 |
| White | 2.66 | 3.26 | 3.37 |
| Hispanic | 2.69 | 3.47 | 3.64 |
| Other and Asian | 2.63 | 3.08 | 3.13 |
Table 4.
Correlation between metals and PFAS variables.
| Metals and PFAS | ||||||
|---|---|---|---|---|---|---|
| PFNA | PFOA | PFHS | Cesium | Molybdenum | Mercury | |
| PFNA | 1.000 | 0.124 | 0.028 | 0.042 | −0.006 | 0.064 |
| PFOA | 0.124 | 1.000 | 0.327 | 0.003 | 0.032 | −0.032 |
| PFHS | 0.028 | 0.327 | 1.000 | 0.029 | −0.013 | −0.069 |
| Cesium | 0.042 | 0.003 | 0.029 | 1.000 | 0.320 | 0.438 |
| Molybdenum | −0.006 | 0.032 | −0.013 | 0.320 | 1.000 | 0.221 |
| Mercury | 0.064 | −0.032 | −0.069 | 0.438 | 0.221 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bashir, T.; Obeng-Gyasi, E. The Association of Combined Per- and Polyfluoroalkyl Substances and Metals with Allostatic Load Using Bayesian Kernel Machine Regression. Diseases 2023, 11, 52. https://doi.org/10.3390/diseases11010052
AMA Style
Bashir T, Obeng-Gyasi E. The Association of Combined Per- and Polyfluoroalkyl Substances and Metals with Allostatic Load Using Bayesian Kernel Machine Regression. Diseases. 2023; 11(1):52. https://doi.org/10.3390/diseases11010052
Chicago/Turabian StyleBashir, Tahir, and Emmanuel Obeng-Gyasi. 2023. "The Association of Combined Per- and Polyfluoroalkyl Substances and Metals with Allostatic Load Using Bayesian Kernel Machine Regression" Diseases 11, no. 1: 52. https://doi.org/10.3390/diseases11010052
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.