2.1. Animals
According to the requirements of the Chinese Pharmacopoeia and WHO regulations, we selected Macaca mulatta (over 1.5 kg) as the test animal, which were provided by the Beijing Institute of Xieerxin Biology Resource (Beijing, China) and Xiangcheng Longrui Experimental Animal Co., Ltd. (Henan, China). We selected monkeys before the test and isolated them for 6 weeks. After blood sampling and testing, we ensured that the monkeys did not carry tuberculosis, B virus, foam virus (FV) or other acute infectious diseases, and there were no neutralizing antibodies against poliovirus in serum. Type I and type III were immunized in 14 and 22 heads of monkeys, respectively, to ensure that the effective number of monkeys after the test was not less than 11 and 18.
All animals were housed in a room maintained at 16–26 °C with an alternating 12 h light/dark cycle (AM. 7:00–PM. 19:00). Food and water were autoclaved. The operation process of animal experiment conforms to the national Regulations on the Administration of Experimental Animals and has been reviewed by the Ethics Committee of Experimental Animal Welfare of Beijing Company. The manufacturers of experimental animals have obtained the production license of experimental animals approved by the Beijing Municipal Science Committee and the domestication and breeding license of wild animals approved by the Beijing Landscaping Bureau.
All efforts were made to minimize animal pain and suffering and the number of animals used during the experiments.
2.3. Methods
MNVT is widely used in the detection of attenuated live vaccines. As an important standard for judging neurovirulence, this method has been used in vaccine quality control in the pharmaceutical industry for more than 50 years. Since 1996, all the experimental steps were carried out in accordance with the requirements of the WHO Regulations for the Manufacture and Testing of Live Attenuated Oral Polio Vaccine and the Pharmacopoeia of the People’s Republic of China (current edition).
The experiment was divided into a vaccine group to be tested and a reference vaccine group. The number of effective monkeys in each group of type I should be more than 11, and the number of effective monkeys of type III should be more than 18. The group of reference and vaccine to be tested should be carried out in parallel. All animals were injected between the first and second lumbar vertebrae, and each monkey was injected with 0.1 mL of sample (the virus content should be 6.5~7.5 LgCCID50/mL).
Spinal cord injection can make the virus directly invade the central nervous system (CNS) tissue. After vaccination, it is observed for 17–22 consecutive days, and the daily feed intake (normal; feed intake 1/2; feed intake 1/3; feed intake waste), fecal conditions (fecal formation; fecal beach; fecal porridge) and motor status (normal climbing; hind limbs unable to move; limbs unable to move) were recorded. If an animal dies during clinical observation, the animal shall be dissected to further confirm the cause of death, and the number of animals killed during observation shall not exceed one quarter before the experiment can be established.
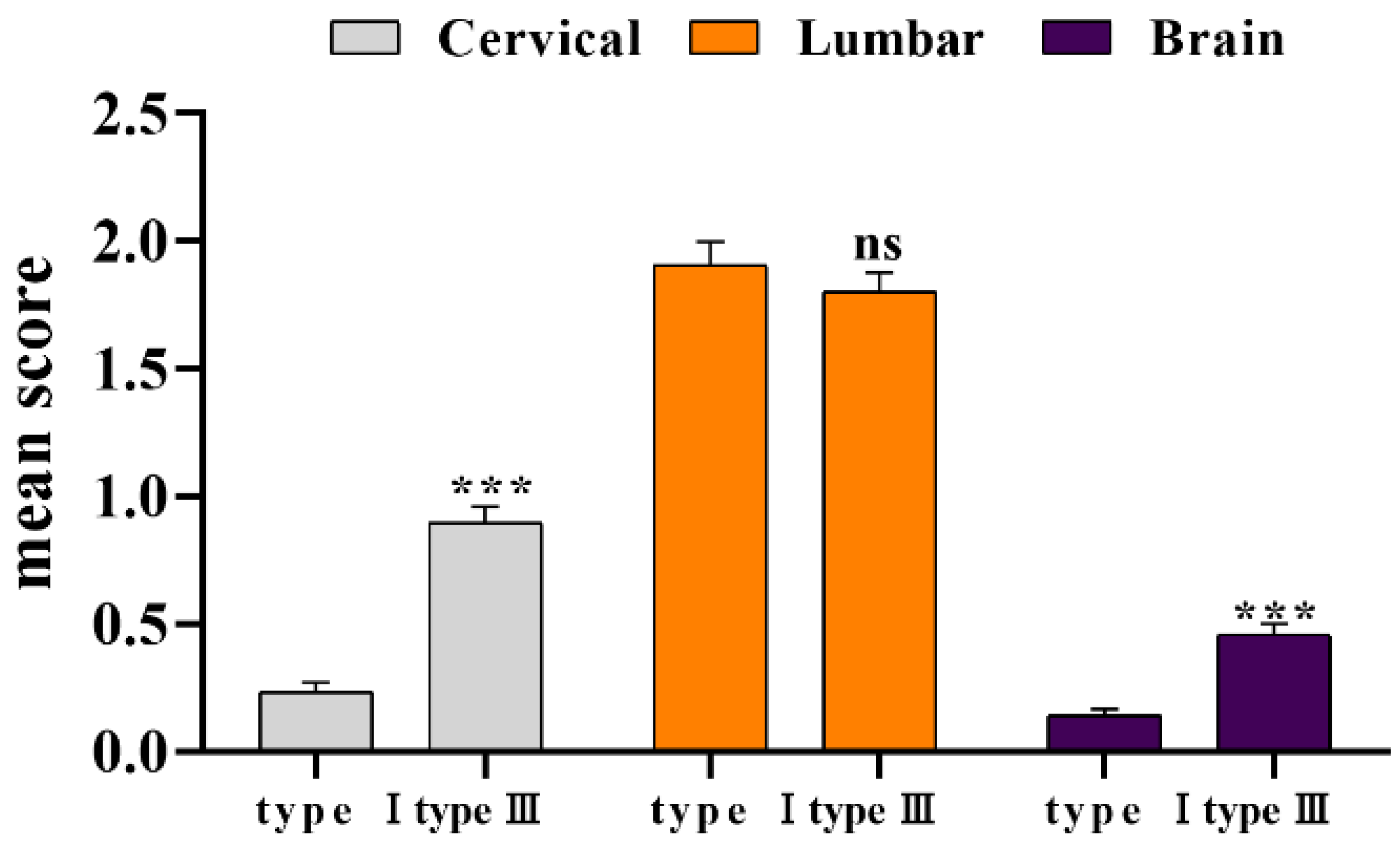
At the end of observation period, sections of the CNS of monkeys were taken for histological examination, and the thickness of the sections was 10–15 μm. Five pathological sections were prepared from each animal, resulting in a total of 29 tissues: 10 tissues from the cervical enlargement, 12 tissues from the lumbar enlargement, 1 from the cerebellum, 1 from the pons, 2 from the medulla oblongata, 2 from the midbrain, 2 from the cortex, and 2 from the thalamus. The specific distribution is as follows:
Slice 1: Swollen neck, 10 slices.
Slice 2: Waist puffed, 12 slices.
Slice 3: 1 section of cerebellum and pontine and 2 sections of medulla oblongata.
Slice 4: Midbrain and cortex, 3 slices.
Slice 5: Thalamus, 1 slice.
After fixation, staining and depigmentation, the pathological sections were prepared, and the lesions in each monkey were observed by microscopic examination and counted using a 4-level scoring method. The scoring process was performed independently by the same experimenter and criteria were as follows:
Score 1: Only cellular invasion like perivascular cufflike leukocyte aggregates; Low, moderate or high cellular invasion by non-neural lesions (which alone would not be sufficient to indicate a positive monkey).
Score 2: Cellular infiltration and little neuronal damage.
Score 3: Cell invasion and extensive neuronal damage.
Score 4: Massive neuronal damage with or without cell invasion.
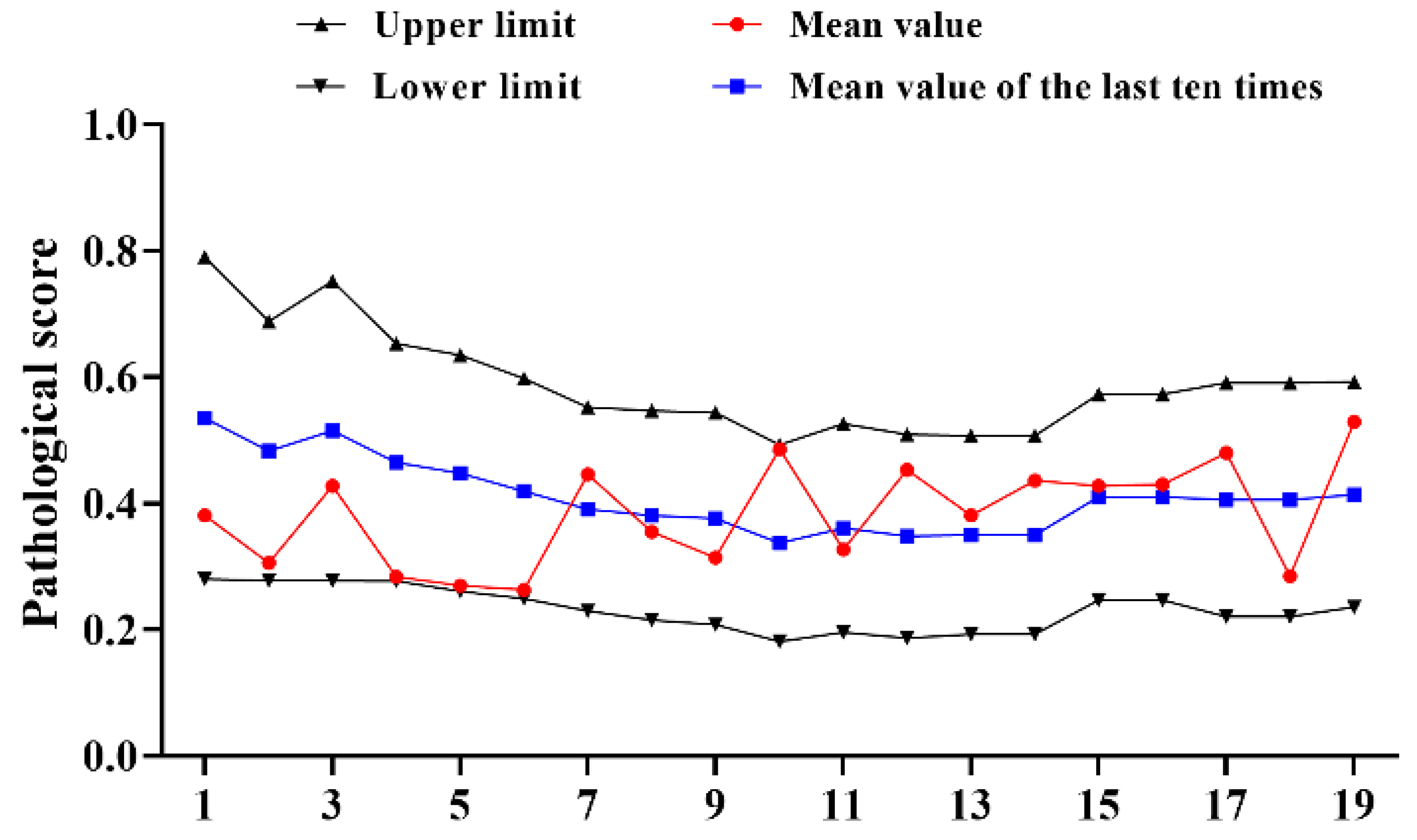
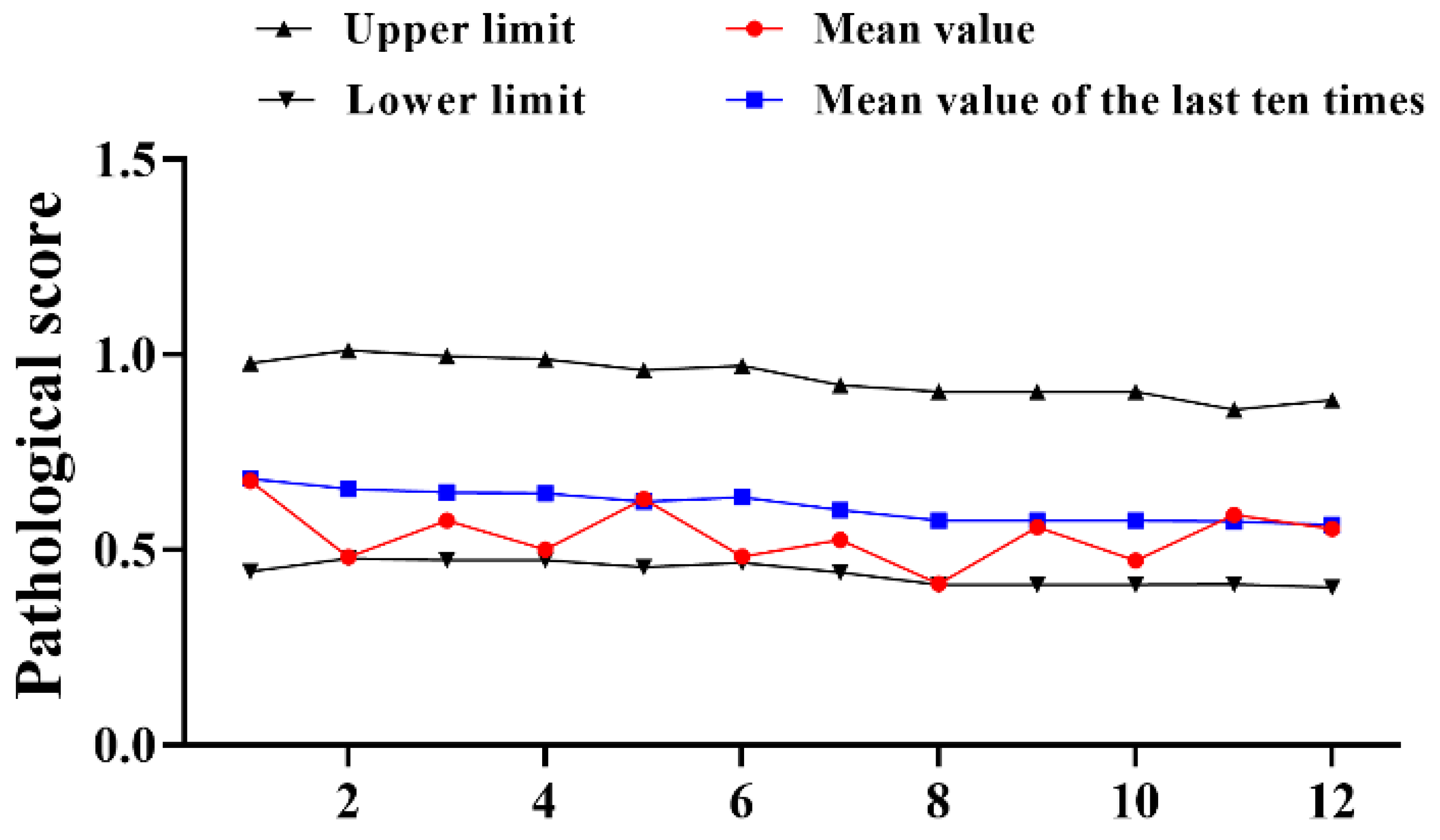
Of concern is that monkeys with neuronal damage in slices, but without a needle track should be considered valid monkeys. Trauma-induced damage in sections without specific pathological changes was not considered valid. Sections could not be included in the scoring if the damage on the sections was a result of trauma and not specific viral damage. Pathological sections were scored by scoring method to determine the activity of virus-induced neuropathy. When the mean value of the reference vaccine was between the upper and lower limits, the vaccine to be tested can be judged to be qualified based on the respective standard values. If the mean value of the vaccine to be tested exceeds the upper and lower limits, the experimental result does not hold.
The mean value of the reference lesion, the total within test error (s2) and combined sample standard deviation (s) were calculated using the sampling error of the statistical mean. The upper limit of type I was calculated as M+s, the lower limit was calculated as M-s, the upper limit of type III was calculated in the same way as type I, and the lower limit comes from M-s/2.
The acceptability constant (C value) was the difference between the average lesion score of the vaccine to be tested and the average lesion score of the reference vaccine. The calculation method is as follows: , , . The results were judged as follows: the average lesion score () of the vaccine to be tested was compared with the average lesion score () of the reference product, if , the vaccine was qualified, otherwise it is unqualified; requires it to be retested and recalculated after the retest. If , it will be judged unqualified.






{kind=link}
{kind=link}
{kind=link}