1. Introduction
The blood flow, to and from the heart, is regulated by the cardiovascular system, which is composed of a complex set of muscles and vessels that must ensure adequate flux for the proper functioning of all organs in the body [
1].
The heart–brain axis is a key part of the cardiovascular system, and failure to supply blood to this area results in the inhibition or disruption of the functioning of the entire body [
2,
3].
The cerebral venous return occurs mainly through the internal jugular vein (IJV) when the subject is in the supine position [
4]. The waveform describing the temporal changes in pressure within this vessel is called the jugular venous pulse (JVP) and it is among the main parameters for monitoring cardiac function [
5].
Moreover, knowledge of the JVP parameter is of extreme interest outside the clinical study of cardiovascular disorders [
6]. Studies conducted by several research groups, including the University of Ferrara, have suggested potential links between cardiovascular dysfunction and the onset of central-nervous-system-related disorders [
7,
8,
9,
10]. To date, unfortunately, there is still insufficient knowledge about the physiology of the venous compartment; therefore, attempts at a cause-and-effect correlation between phenomena are often difficult to validate [
11,
12].
The activity of the nervous system is influenced by multiple factors, such as posture and breathing, and their changes significantly alter blood flows and pressures within vessels [
13]. For these reasons, the study of the hemodynamics of the brain, and particularly the study of its drainage through the IJV, is one of the most interesting strands of current scientific research in the medical field.
The possibility of studying in vivo the dynamics of the cerebral venous return is limited for several reasons. On the one hand, there is a problem related to the instrumentation useful for investigating the fluid dynamics of such a complex system. Noninvasive instruments (e.g., pulse oximeters) are obviously desirable, but their measurement accuracy is limited for this investigation [
14]. Conversely, more precise invasive instruments (e.g., sensors attached to cannulas) inevitably affect the measurement itself [
15]. For these reasons, it is critically important to develop in silico and in vitro simulation environments to improve the ability of health operators on using noninvasive instruments for carrying out investigations on physical factors that regulate blood flow in the circulatory system [
16,
17].
Ultrasound is a widely used technique that allows both the imaging and acquisition of information about the dynamics of the vascular system without the use of ionizing radiation, and at a very low cost. Its main drawback is that it is a highly operator-dependent technique [
18]. Therefore, it is necessary to have tools to enable healthcare operators to be adequately trained to carry out ultrasound investigations.
The use of ultrasound examination is rapidly increasing in acute care specialties because of the evolution of point-of-care ultrasonography: a novel patient’s bedside approach for diagnostic purposes [
19].
In cardiovascular emergencies, where the needs of rapid assessments are strongly prominent, ultrasound-assisted examination is a promising trend [
20]. Therefore, the JVP parameter can be used by cardiologists as an indicator to diagnose heart failure.
The assessment of the JVP can be obtained by recording the changes in the cross-sectional area of the IJV with the ultrasound scanner [
21], but it requires a highly qualified healthcare provider. Nowadays, there is a shortage of professional sonographers [
22], so it is of paramount importance to accelerate the learning process for such operators.
Training physicians is of great interest because it allows them to acquire the necessary skills to perform adequate examinations, as well as the ability to identify the presence of interesting details on the images [
23]. In sonography, image acquisition is complex and operator-dependent: the quality of a scan may reflect the degree of training and there is a significant learning curve [
24,
25]. Good transducer placement and orientation plus familiarity with ultrasound anatomy are required. It has previously been demonstrated that simulations may provide an efficient way of training [
26], for example, to hold and place the probe properly, and to assess device parameters during scans [
27,
28].
The use of skill trainer devices is particularly required for the sonographer community, for providing constant training without waiting for the availability of patients and without jeopardizing their health [
29]. Ultrasound training systems have been proposed in [
30,
31]; they mostly consist of software applications that exploit pre-acquired images that are not suitable for echo-doppler training, because of the lack of haptic feedback.
The proposed research aims to develop a mechatronic system for the assessment of cardiovascular function using standardized, inexpensive, and reliable data acquisition methods. The mechatronic system consists of a hemodynamic circuit connected to a manikin designed to simulate vessels and soft tissues of the human neck. Such a manikin is made of materials that can replicate the characteristics of human tissues with respect to ultrasound, i.e., tissue echogenicity. The data for the proper implementation of the hemodynamic circuit, aimed at reproducing the blood flow of clinical interest, are first simulated on MATLAB, version R2022b.
The entire hemodynamic circuit is developed to verify the proper functioning of ultrasound equipment, in use by medical personnel, who perform investigations of cardiovascular function. As a natural consequence, the mechatronic cardiovascular system aims to become a tool for training medical personnel.
2. Materials and Methods
2.1. Hemodynamic Circuit Hardware
For the development of the hemodynamic circuit, a fully customized gear-pump–servomotor combination is used. The Dayton 4KHH8 gear pump (Grainger, Inc., Lake Forest, IL, USA) has a rated maximum continuous output flux of 302 mL s
−1. It is a positive displacement pump, which means that the output flow is minimally affected by downstream pressure. Compared to rotodynamic pumps, the gear pumps exhibit smaller variations in output flow under varying downstream loading conditions [
32]. In this way, a wide variety of manikins can be placed downstream of the pump without losing efficiency. The gear pump can also generate negative flows by changing the direction of motion of the motor. Unlike the piston pumps, they can be operated continuously and do not need complex tubing connections or valves for switching flow directions. This gear pump was already used for similar research purposes as reported in [
32]. The pump and all the materials used to connect it with the manikin are selected to avoid reactivity with the working-blood-mimicking fluid used in this study [
33].
A closed-loop NEMA 34 stepper motor is chosen. This motor generates approximately 0.81 hp at 1725 RPM, up to 300 mL s−1 of flow at physiologic pressures, and enables the pump to handle waveforms with steep acceleration.
A closed-loop stepper driver (model: CL86T, input voltage: 48 V, maximum output current: 8.2 A) regulates the motor. It accepts clock and direction digital signals from a microcontroller as control inputs.
The motor and the pump shafts are coupled through a SC 040 ServoClass Double Flex Couplings Zero-Max, Inc., Plymouth, MN, USA (operating torque: 10 NM, maximum speed: 10,000 rpm, tightening torque: 3.4 Nm) to allow small parallel and angular misalignments while ensuring zero backlash.
A 10 mm inner-diameter high-pressure PVC tubing is used to connect the reservoir, pump, and manikin sections. The low compliance of this tube minimizes the flow waveform distortion while the large inner diameter minimizes the flow resistance.
Flow measurements are critical to ensure the generation of realistic waveforms; thus, the ultrasonic clamp-on flow meter SONOFLOW CO.55/120 V2.0, SONOTEC GmbH, Halle, Germany (measurement principle: ultrasound, outer/inner tubing diameters: 14/10 mm, measurement range: 1.2–12 L min–1 ± 2%, output: 4–20 mA current loop, housing: aluminum) is included in the hemodynamic circuit to perform accurate and timely flow measurement. Such a non-invasive sensor can provide high-accuracy measurements in dynamic conditions without any contact with the fluid.
To implement the motor control loop and to acquire data from the flow meter, an Arduino Zero board, Arduino S.r.l., Monza, Italy (microcontroller: 32-Bit Arm Cortex, operating voltage: 3.3 V, 20 digital I/O pins, flash memory: 256 KB) is selected, and the values of the measured flow are transmitted in real time to a PC via a serial communication protocol to log data for post-processing purposes.
2.2. Manikin
Existing ultrasound manikins can be organic-based, e.g., agarose-gel-based, but the choice of these materials is not recommended, due to their poor durability [
34].
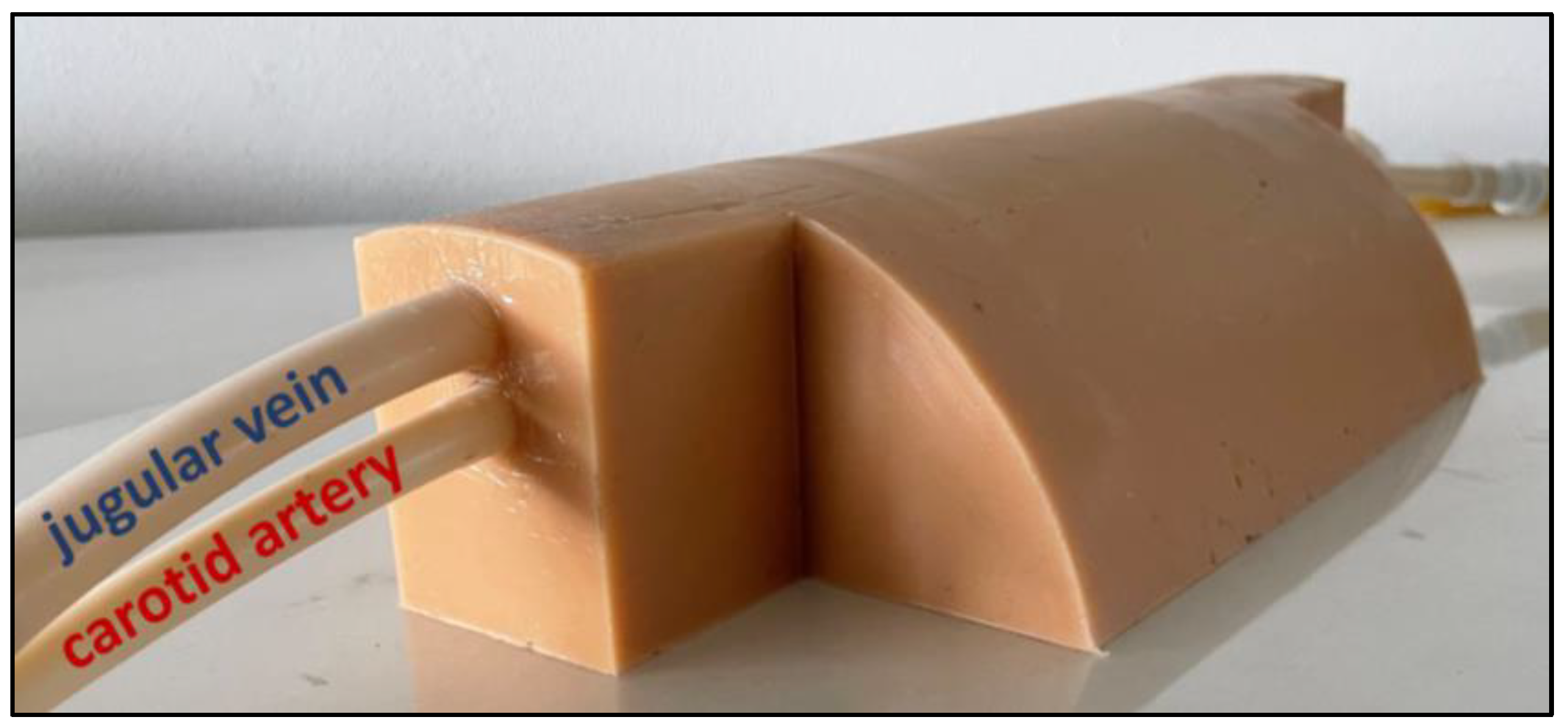
In this work, we opt for a silicone-based material to make the ultrasound manikin prototype. The manikin is developed in collaboration with the ACMIT Gmbh company, Austria. It emulates a human neck but includes only the two main blood vessels, i.e., jugular vein and carotid artery, as clearly visible in
Figure 1.
The vessels are just cavities in the silicone to guarantee a proper transmission/reflection of the ultrasound wave. The external tubes, too rigid to emulate a vessel, are only used to connect the cavities to the circulation pumps. The length of the manikin is far enough to achieve laminar flow.
The manikin material is ultrasound-compatible and emulates the stiffness of the neck area, so mimicking as much as possible the different collapsibility of arteries and veins. Moreover, the manikin comes close to real tissue with biomechanical parameters to save the vessels’ geometry, their relative distance, and the distance with the manikin upper surface.
2.3. Hemodynamic Circuit Design in MATLAB/Simulink Simulation Environment
The design of the mechatronic hemodynamic system that reproduces in vitro human blood flows is first simulated using the Matlab/Simulink simulation environment (MathWorks, Inc., Natick, MA, USA), version R2022b. The purpose of the simulation is to test the capability of the hardware in generating a flow similar to the ideal JVP waveform, for different values of heart rate.
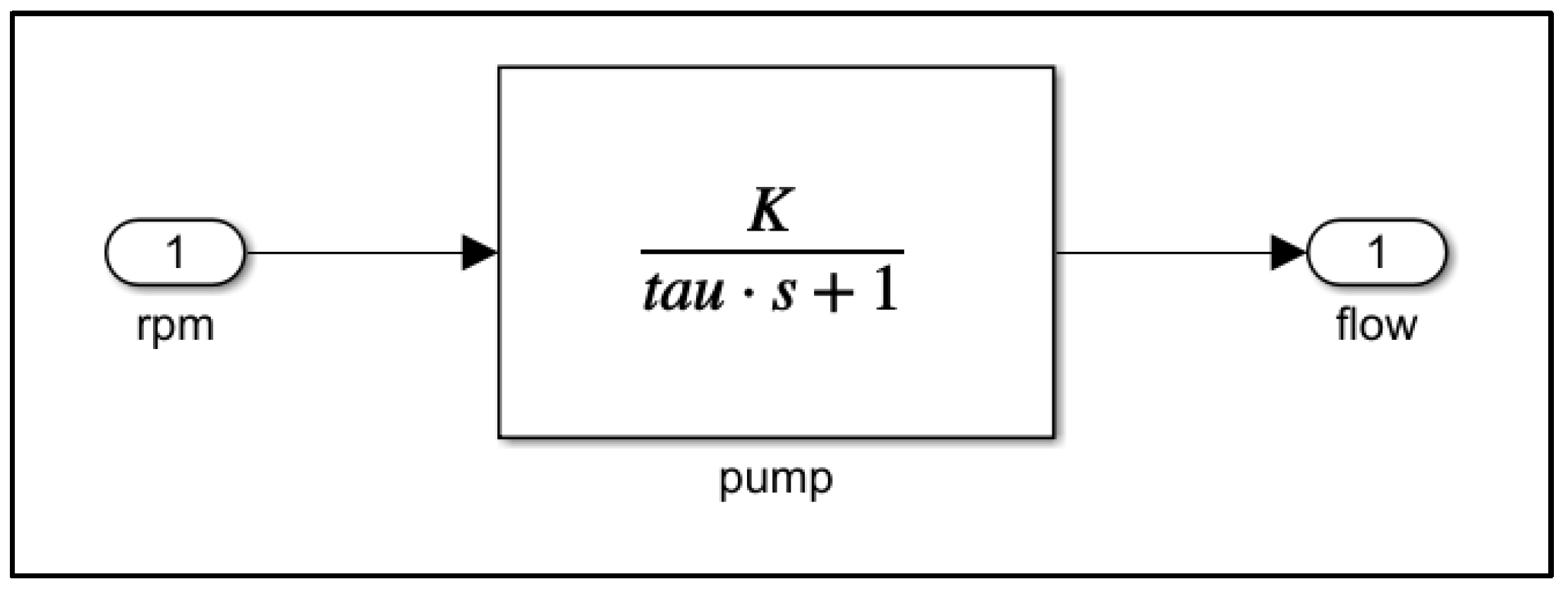
From the point of view of control systems theory, the motor and the pump can be considered as a single dynamical system that transforms the motor setpoint velocity (system input) into a blood flow (system output) with first-order dynamics, introducing a settling time proportional to the system time constant
τ. In particular, the adopted transfer function of the motor/pump system is:
where
is the Laplace transformation variable and
is the theoretical proportional coefficient that relates the motor rotational speed to the flow generated by the pump. Its value, i.e.,
= 0.0035, is experimentally calculated in regime conditions. In addition, the time constant
is empirically tuned to introduce a settling time of 0.3 s in the step response. Such a value is experimentally obtained by measuring the settling time of the real pump in the tracking of a unitary step flow reference signal.
Figure 2 shows the Simulink transfer function block associated with the motor/pump system.
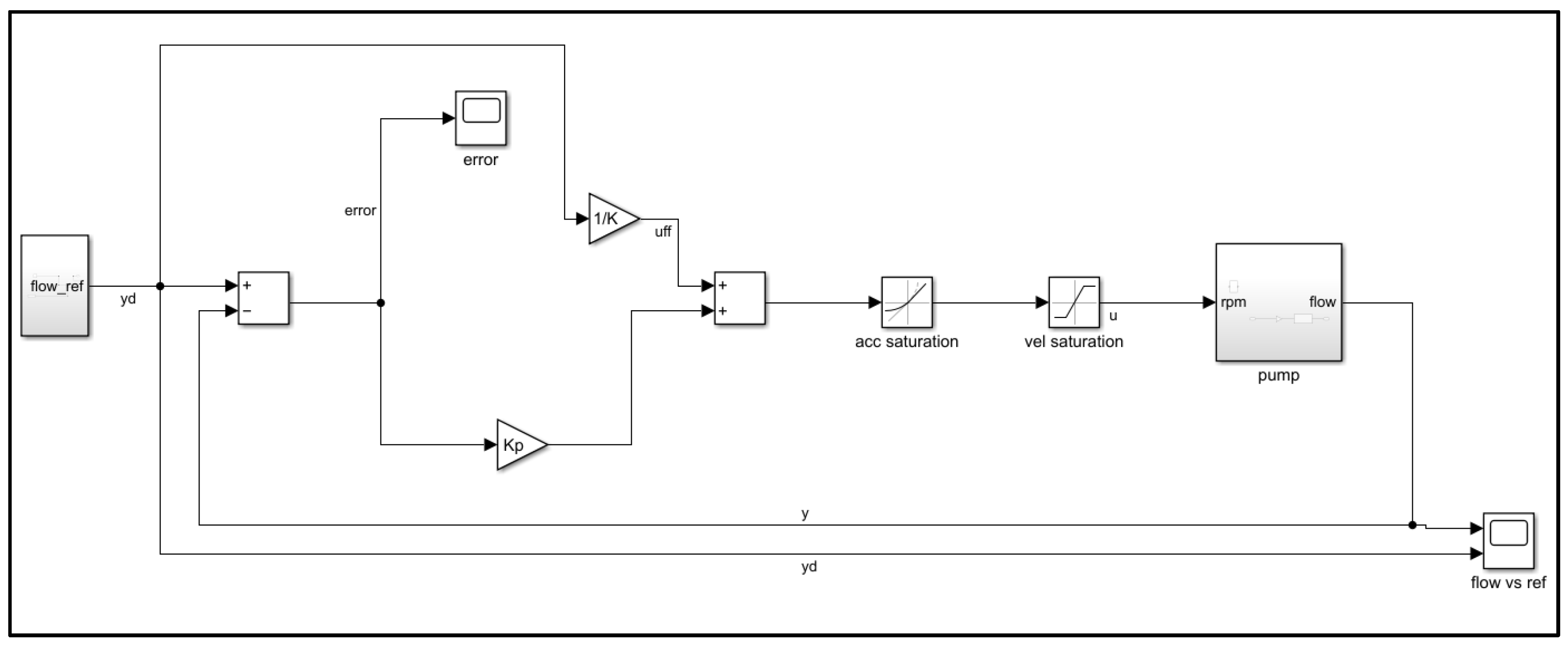
With the aim of tracking a desired flow reference signal, such a dynamical system can be controlled with a proportional regulator with feedforward, so the motor/pump input signal becomes as follows:
where
represents the time in seconds;
is the motor/pump input, i.e., the motor velocity setpoint;
is the proportional regulator gain;
is the tracking error, i.e.,
with
as the desired flow and
as the actual flow; and
is the feedforward term added to the input with the aim of deleting the steady-state error and is computed as:
.
Finally, saturations on the motor/pump input and on its rate change are inserted into the control loop to take into account the physical capabilities of the motor drive. The proportional regulator gain
is empirically tuned to rapidly track the reference signal with the minimal intervention of input saturations. The overall control loop is depicted in
Figure 3.
The results of the simulations show that even if the desired flow reference signal is not perfectly tracked, a realistic flow can still be generated, up to a heart rate of 70 bpm. For higher heart rates, the delay introduced by the motor/pump system prevents the generation of a realistic flow.
Figure 4 shows the comparison between the desired flow and the generated flow in a 10 s simulation. The rapid variation in the reference signal is not perfectly tracked by the motor, due to the first-order dynamics of the system and the velocity/acceleration constraints that introduce a finite settling time, so the local peak values of the reference curve are smoothed. However, the main three positive peaks of the curve are still present in the generated flow, implying a realistic behavior.
3. Results
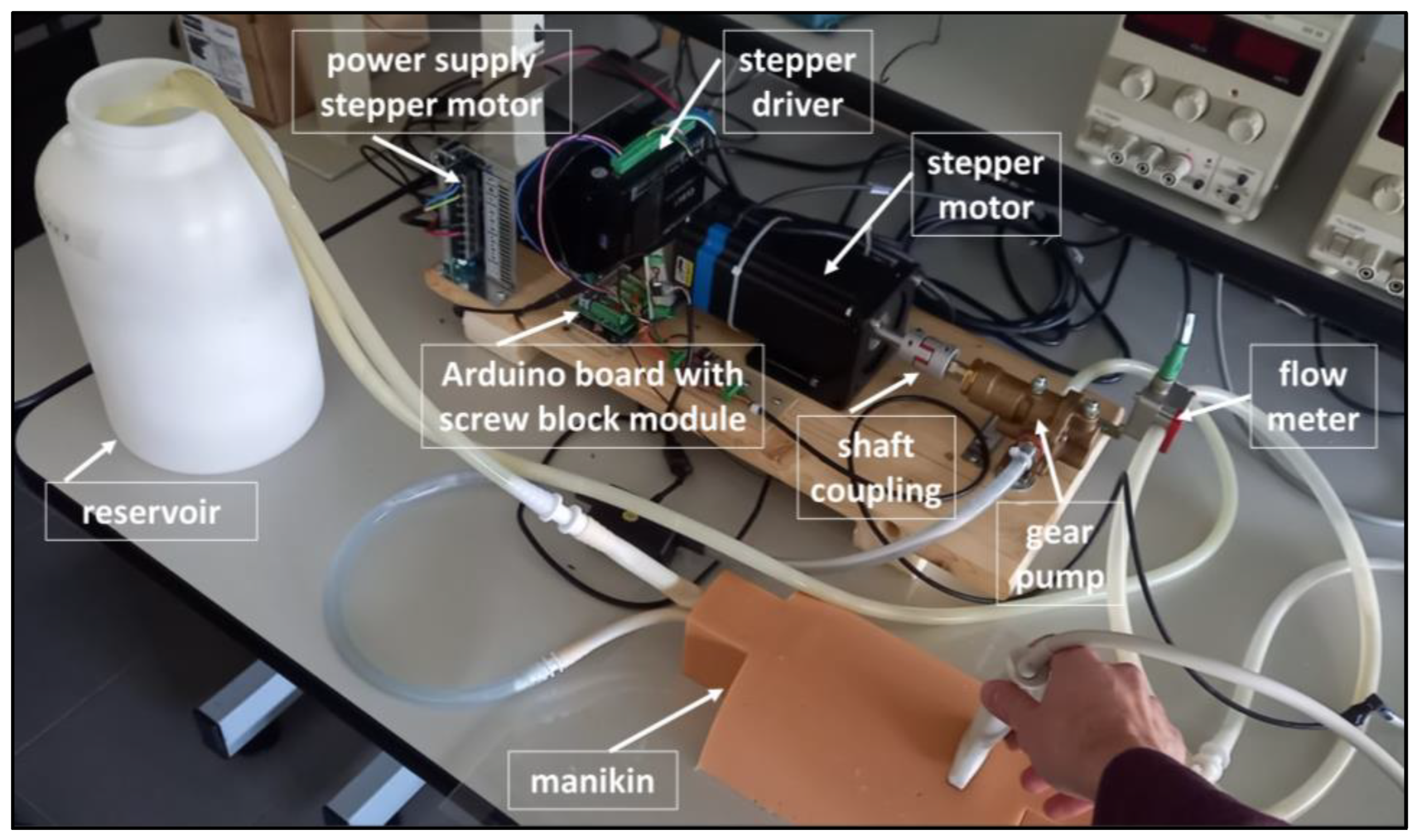
The hemodynamic circuit was assembled at the Laboratory on Intelligent Robotics and Automation of the Department of Engineering, University of Ferrara.
Figure 5 shows a user performing the echo-doppler ultrasound examination on the manikin connected to the proposed mechatronic hemodynamic circuit. The names of the main parts of the circuit are also shown in
Figure 5 to aid the reader’s understanding.
The silicone-based manikin used in the experiment replaces the body part of the neck, and the doppler fluid used in the circuit is formulated to mimic the acoustic and physical properties of human blood [
33].
The aim of the experiments was to compare the actual flow passage through the manikin with echo-doppler measurements carried out by using an ultrasound scanner, i.e., My-LabAlpha system with linear array probe SL1543 (Esaote S.p.a., Genova, Italy).
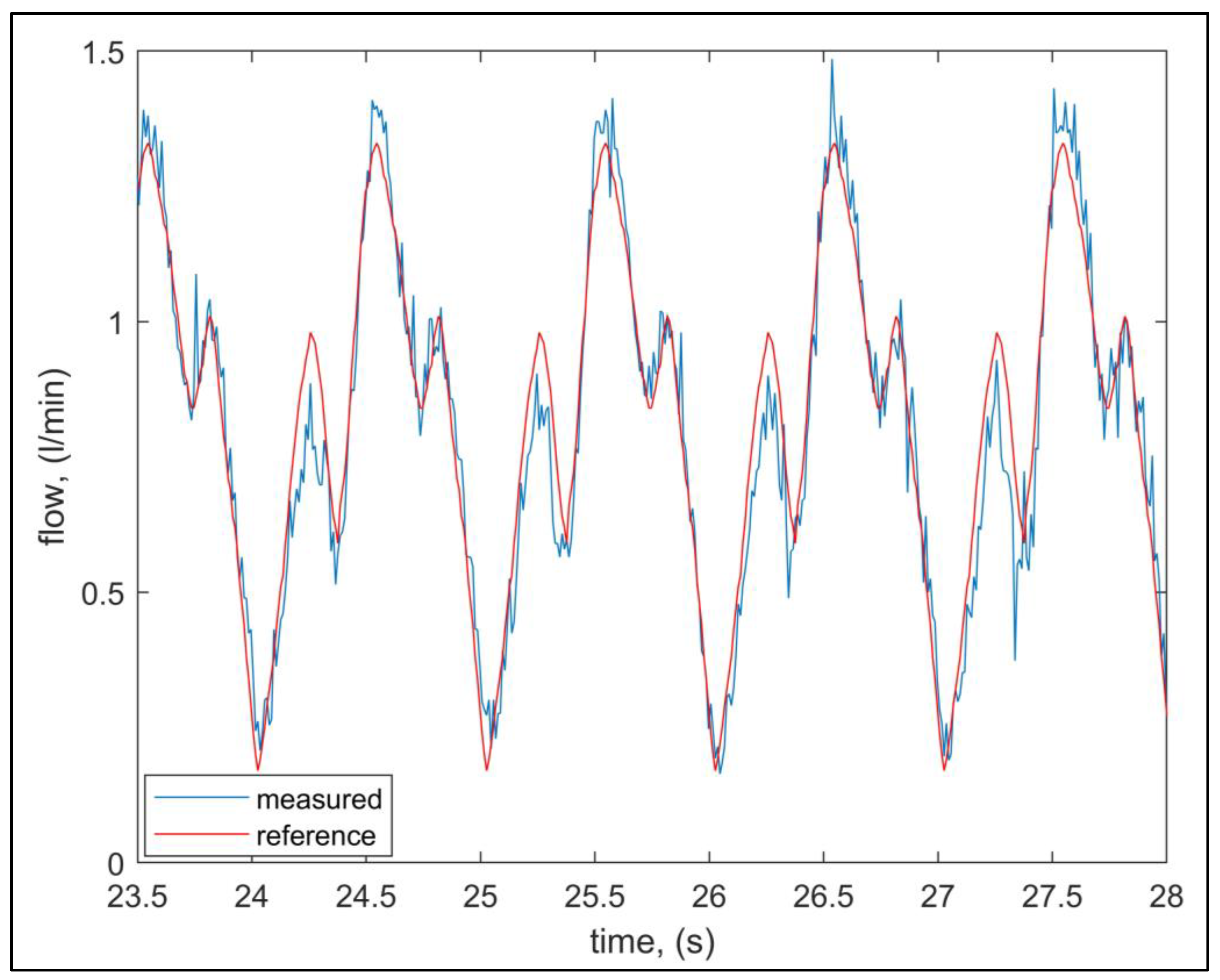
The experimental phase of this work was then divided into two parts. First, experiments were carried out to verify the capabilities of the control loop of the hemodynamic circuit to track the ideal JVP waveform obtained with the simulations. As depicted in
Figure 6, the mechatronic system generates a flow suitably close to the ideal one unless a delay that does not affect the purpose of the application is present. The generated flow was measured in the hemodynamic circuit with the flow meter.
In
Figure 6, the delay introduced by the mechatronic system was removed so that the two curves could be better compared. The measured signal faithfully follows the reference signal, and this ensures that the proposed hemodynamic circuit works properly.
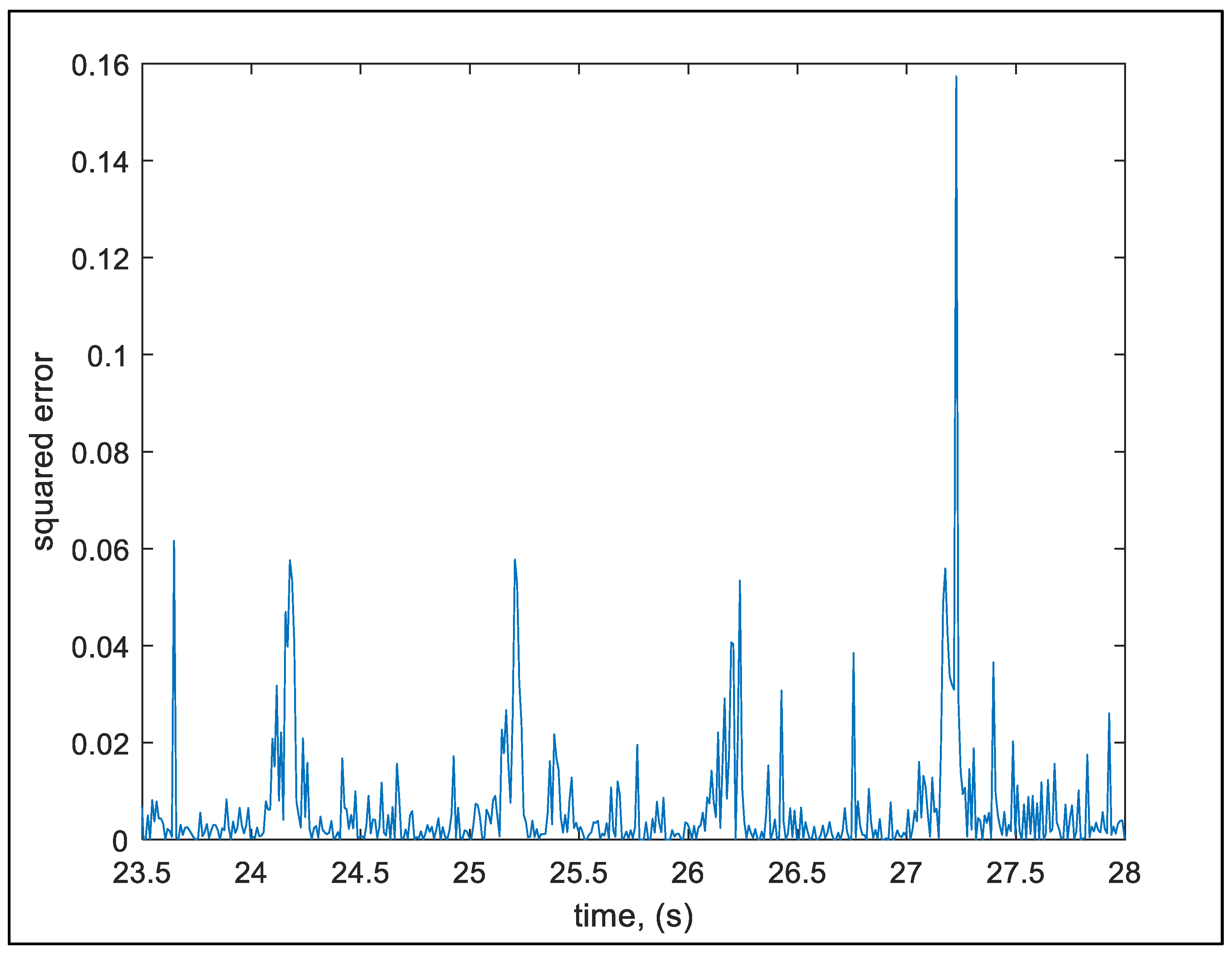
In order to better analyze the dynamic performance of the proposed system, the squared error
was computed as the squared difference between the reference
and the measured flow
:
The graph of
Figure 7 shows the computed squared error in several control loop periods. In particular, it can be noticed that the peak values of the squared error correspond to the faster variation in the reference signal that cannot be perfectly tracked, due to the physical capabilities and the acceleration limits of the motor/pump system. However, the overall Root-Mean-Squared Error (RMSE) is 0.109 L min
−1. Such a value is negligible if compared to the typical flow variations that can be observed considering different human anatomies.
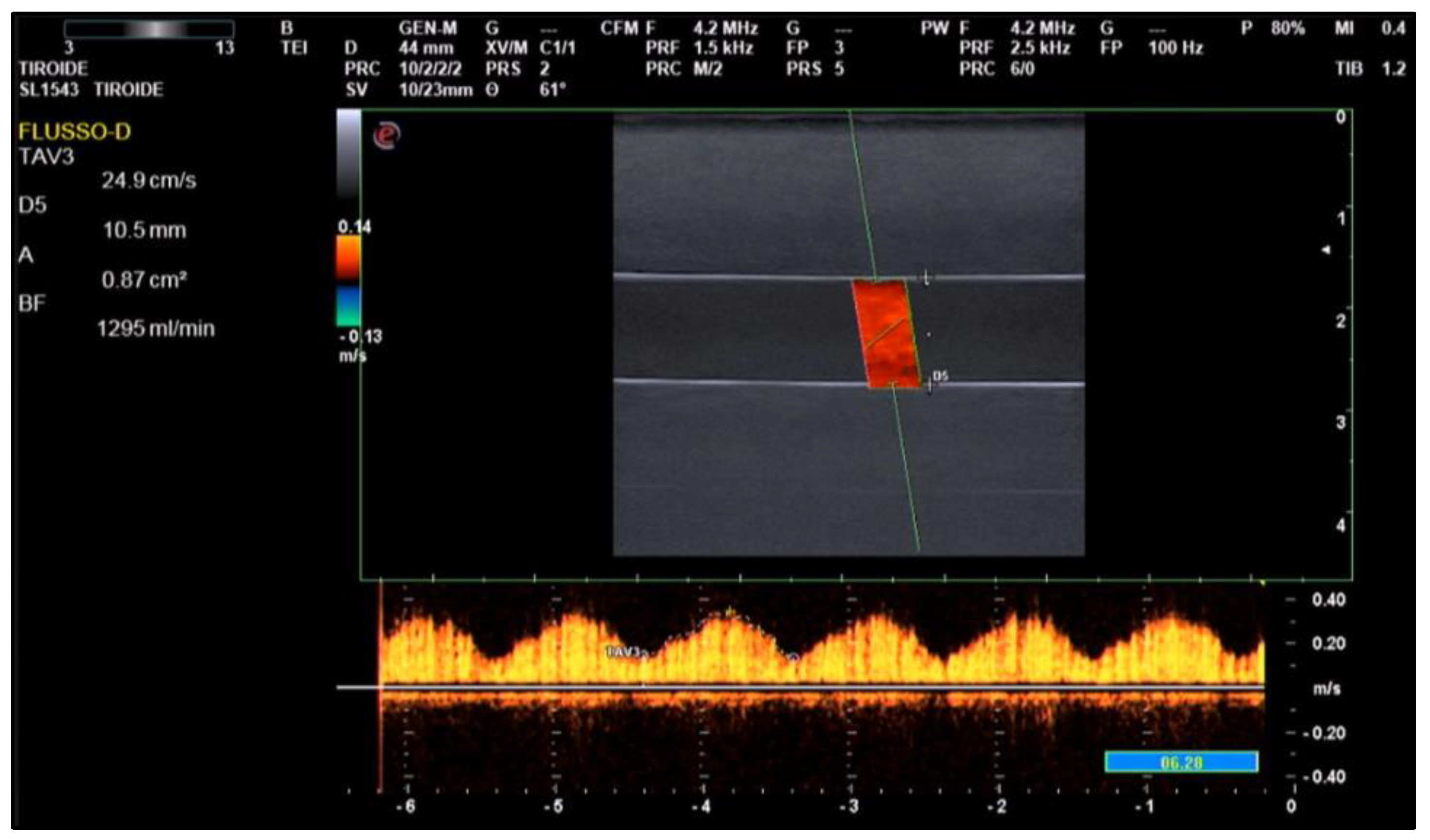
Again, experiments were carried out with the aim to compare the average value of the flow measured by the ultrasound scanner, on a certain number of periods, with the actual average flow generated by the proposed system and measured by the flow meter. The results of the obtained flow show that the echo-doppler measurements are always larger, in amplitude, than the actual average flow. Particularly, a set of 20 echo-doppler measurements on one JVP period results in an average value of 1.25 L min−1, while the actual average flow actuated by the pump is 0.92 L min−1.
Figure 8 shows a screenshot of an echo-doppler measurement.
The larger value obtained for the flow measured with the echo-doppler compared to that given with the flow meter is because medical ultrasound scanners are calibrated to consider a sound propagation speed of 1540 m s−1, which is equal to the average speed of sound propagation in the human body. Conversely, the manikin used in this experiment is based on a silicone-based material for which the speed-of-sound value is lower than that assumed by the ultrasound scanner, resulting in a distortion in the calculation of vessel wall spacing.
4. Discussion
The proposed mechatronic cardiovascular simulation system is designed to train the user in terms of the physical interaction between the ultrasound probe and the patient tissue and vein. Indeed, the proposed system generates a realistic ultrasound visualization reacting to the user probe positioning and to the applied forces. It is currently set to be a facilitating tool for learning ultrasound examination in the neck area, and particularly on the IJV. Waveforms of other circulatory pressures can also be generated with the simulator, so the ultrasound investigation may vary from case to case.
This system enables effective use of the entire apparatus in high-fidelity-simulation scenarios. Indeed, a typical emergency scenario is represented by means of two separated environments: the director room, where the instructor manages the parameters to be investigated, and the simulation room, where the trainee examines the manikin representing the patient. It is often required for the trainee to have no contact with the trainer during the session, but the instructor can observe the scene and modify the desired waveform, which is loaded in the software that drives the hydraulic pump, so the desired flow can be generated on the manikin, at the point where the trainee should put the probe. Then, the trainee uses the probe to perform the ultrasound examination on the manikin. This mainly considers the hand–eye coordination in the simultaneous actions of moving the probe and interpreting the visualized view to perform a diagnosis.
The results obtained in the experimental phase imply a high uniformity for the JVP waveform generated on each cycle. Our pump design performs equal to or better than previous studies and most commercial systems in terms of realistic flow accuracy [
35,
36,
37] because the design of the control software allows for individual needs, with the possibility of adding emergency scenarios, such as vascular disease. In addition, the system can be arranged to be portable, and we estimate that it would take an experienced technician about 5 h to configure the entire hardware and software, including the time for assembly, machining, and writing the code for motor control and signal handling. The total cost, including all parts and machining, is less than 2000 EUR.
A further application of our system may involve the training of AI algorithms [
38,
39,
40] for the implementation of autonomous diagnostic tools.
The proposed system has several nontechnical advantages:
It takes less than 1 min from when the desired waveform is specified for the pump to produce an accurate replica;
After the initial setup, no additional human intervention is necessary;
The pump can be completely controlled by computational programs.
This ability for automation is a useful feature for experimental setups where large numbers of flow waveforms are desired (e.g., in vitro flows through the same anatomical location under various conditions that affect the flow pulse amplitude). Both scientific investigation and clinical training would benefit significantly from this automation capability.
5. Conclusions
In this study, we successfully designed, built, and tested a mechatronic cardiovascular simulation system for jugular venous echo-doppler training. The system was also designed to learn how to safely use ultrasound equipment. The proposed setup is much more convenient than commercial systems useful for simulating blood flow in the jugular vein, and it is ideal for vascular simulation, in general. It can be used as a training tool to accelerate the learning process and confidence of novice sonographers, and its use is convenient for point-of-care ultrasound deployment because the whole system is easily transportable and has a low cost. In the future, the proposed system could be used when proceeding with ultrasound guidance for venous catheter insertion and to evaluate arterial catheter insertion performance.
To conclude, it is possible to state that the cardiovascular ultrasound simulation systems offer new possibilities for the training of sonographers. Indeed, the use of these tools allows the improvement of psychomotor skills for proper hand–eye coordination in the generation of ultrasound images, and then to transfer the skills acquired during simulations to real patients. In addition, learning the basics on manikins rather than in a clinical setting reduces patient and learner anxiety.
The challenge of implementing a procedure based on ultrasound simulation, on a large scale in medical residency programs, requires the development of a variety of teaching methods, and the use of the proposed mechatronic cardiovascular simulation system represents one of them.

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







