


IoT-Based Motorbike Ambulance: Secure and Efficient Transportation

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
- The first step includes a 5G-wireless mesh network and splits it into VLANs, and each VLAN represents an independent wireless sub-network.
- The second step is writing a middleware application that handles the network and determines the closest end-to-end convenient access point using an appropriate algorithm to ensure that the patient is transported urgently to the nearest hospital.
- Third, the middleware transmits information to the network and monitors emergency motorbike information in the protected sockets layer to ensure the maximum degree of secure communication using the cryptography method. The ant colony hypothesis, one of the SWARM optimization methods recently used to solve short-tracking path problems, is proposed for quick access to the closest medical center.
2. Preliminaries
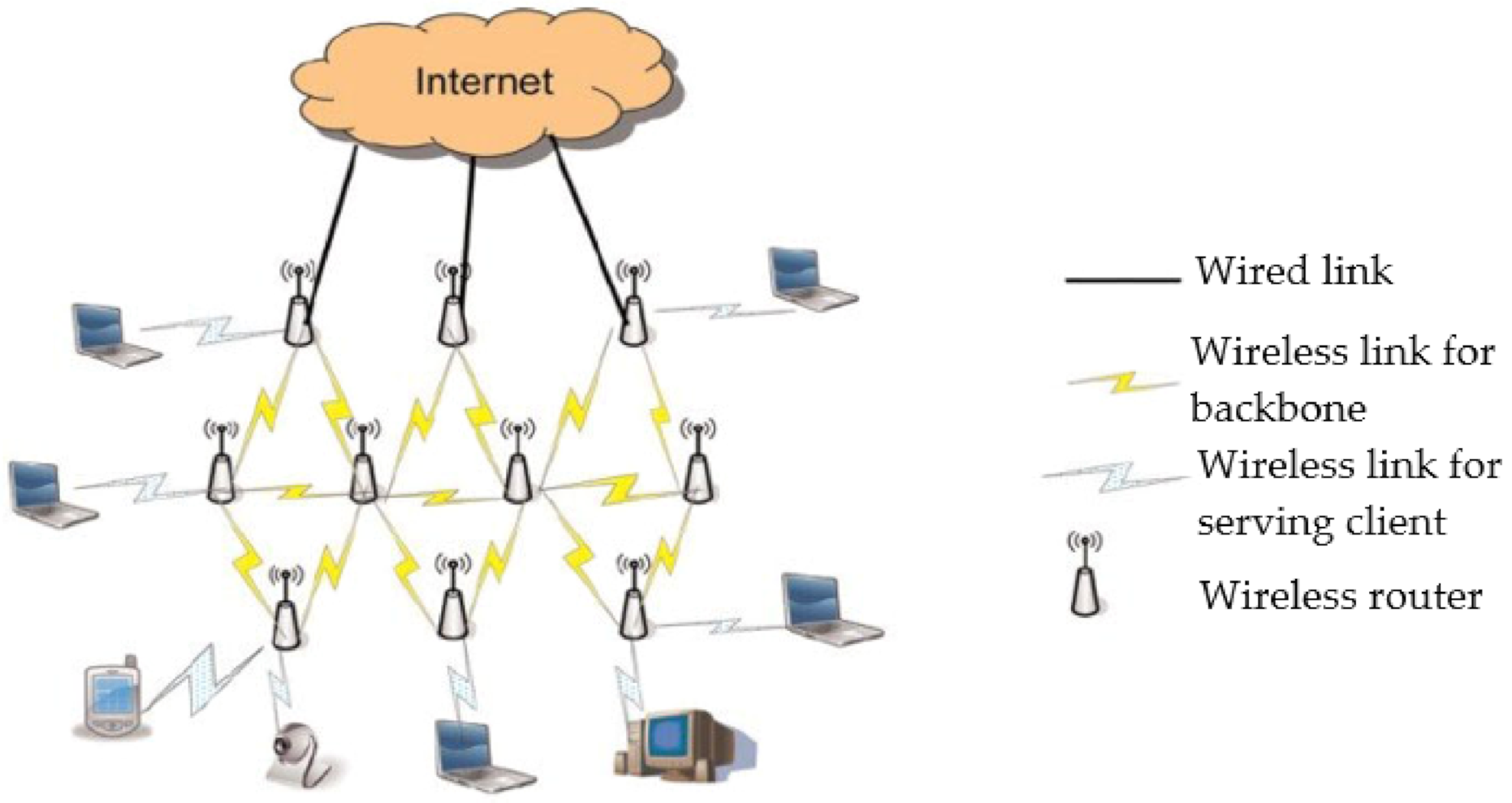
2.1. 5G-Wireless Networks and IoT
2.2. Vehicle Social Networks
2.3. Telemedicine Services Based on WMNs
2.4. Intelligent Ant Colony Optimization (ACO)
2.5. Transport Layer Security (TLS)
2.6. OMNeT++
3. The Proposed System
- The motorbike’s SWARM computing algorithm is programmed to find the best way.
- Middleware is more reliable than any other Ad-Hoc middleware network because of the proposed encryption approach added to the TCP/IP network layer.
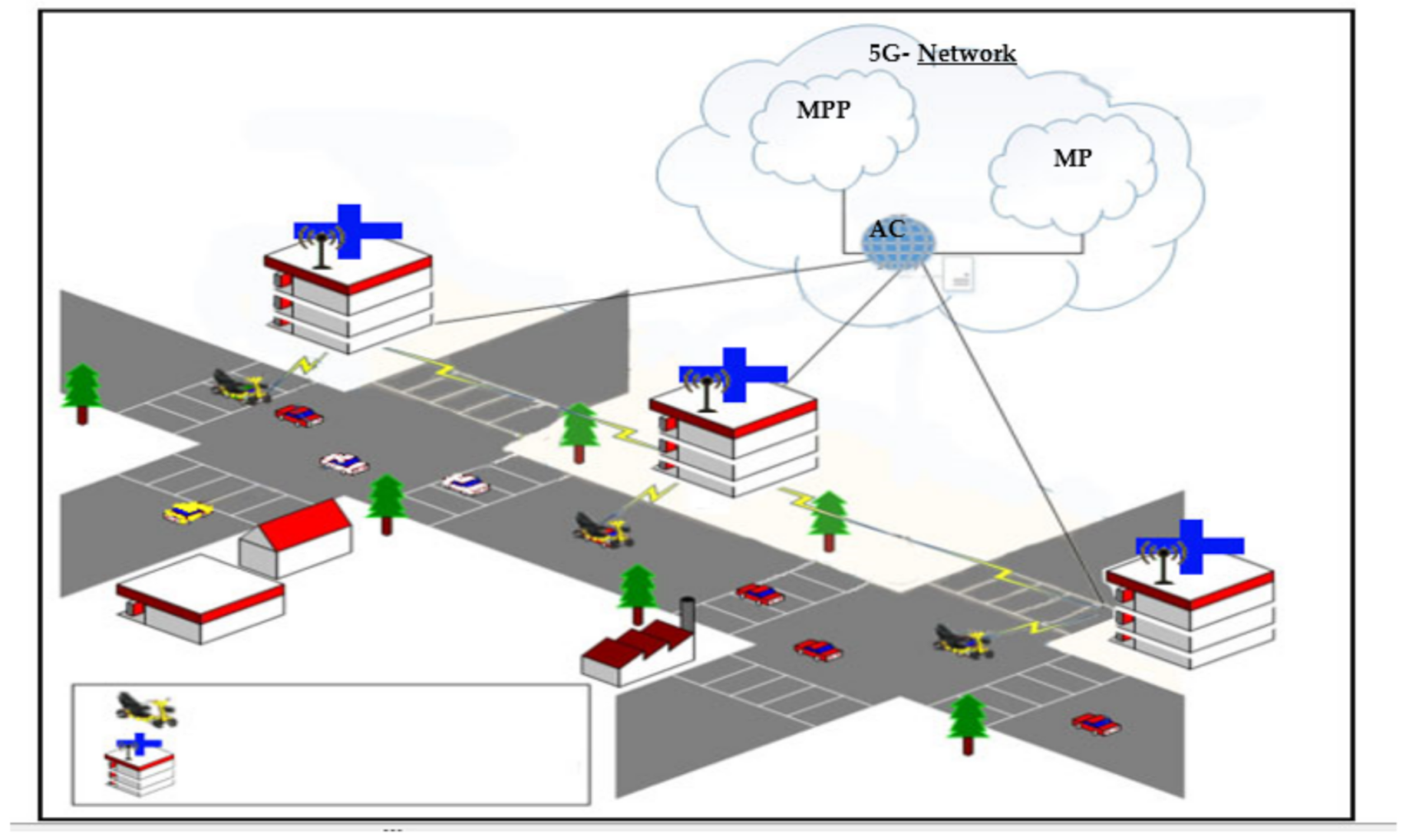
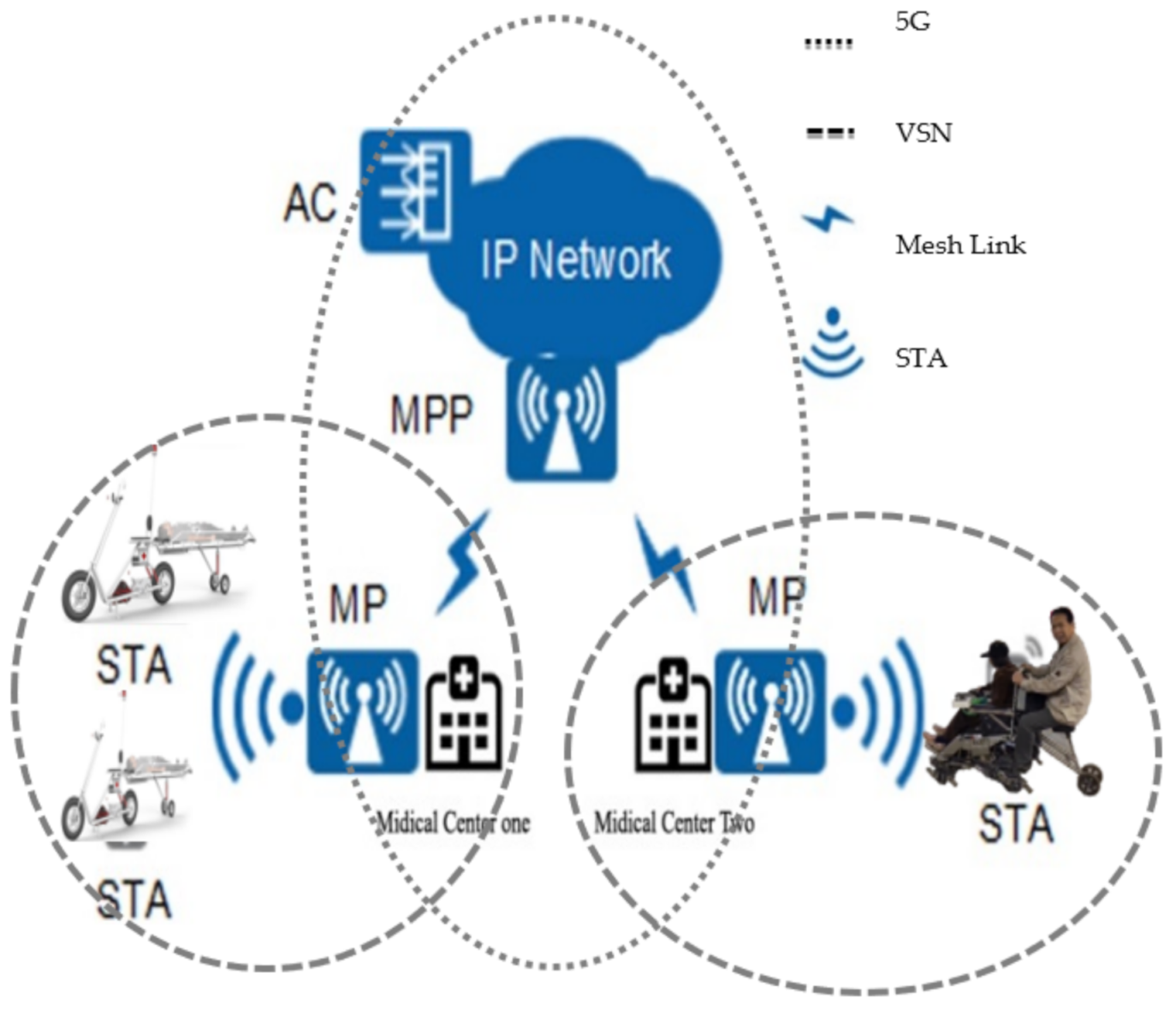
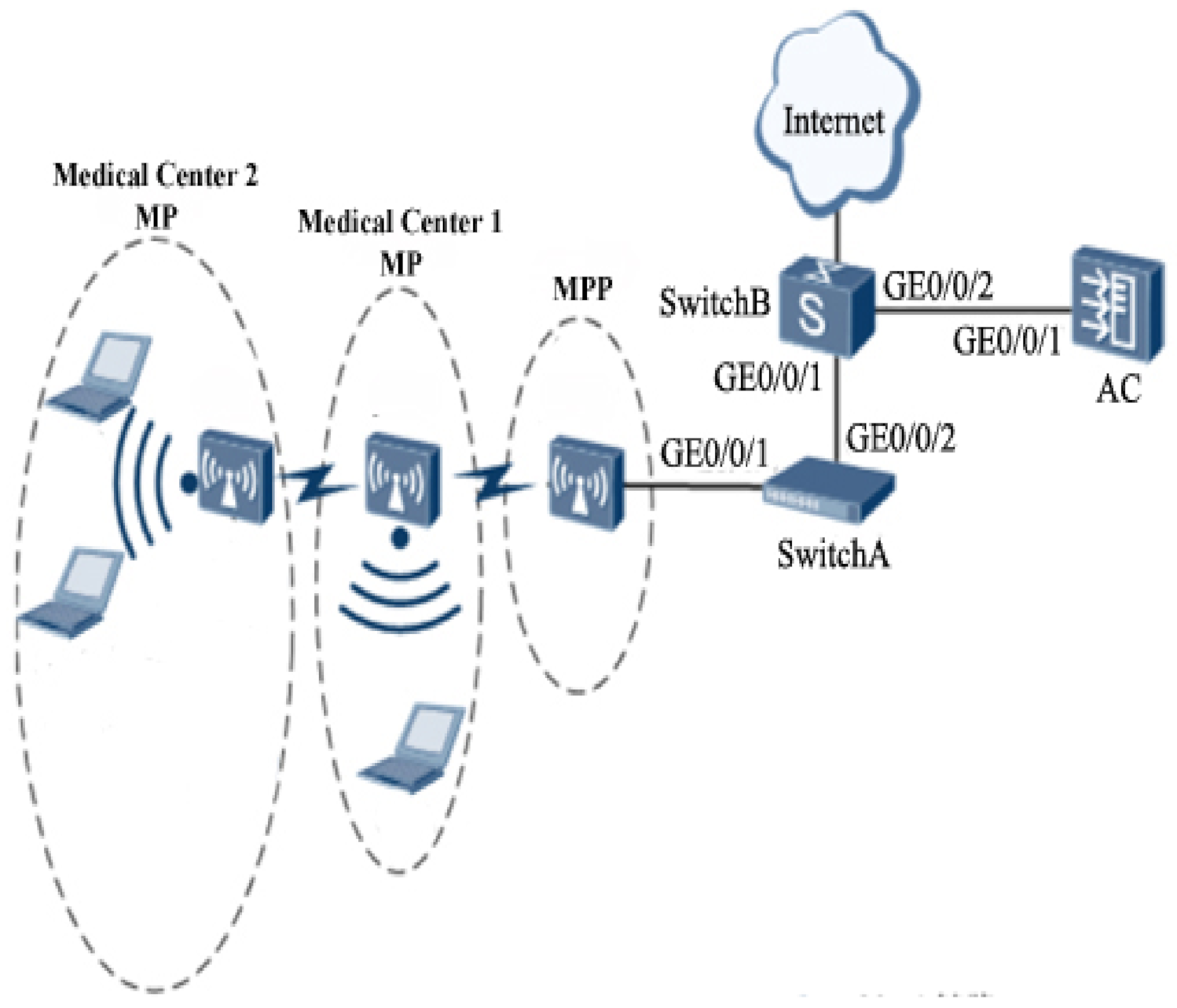
3.1. Network Architecture
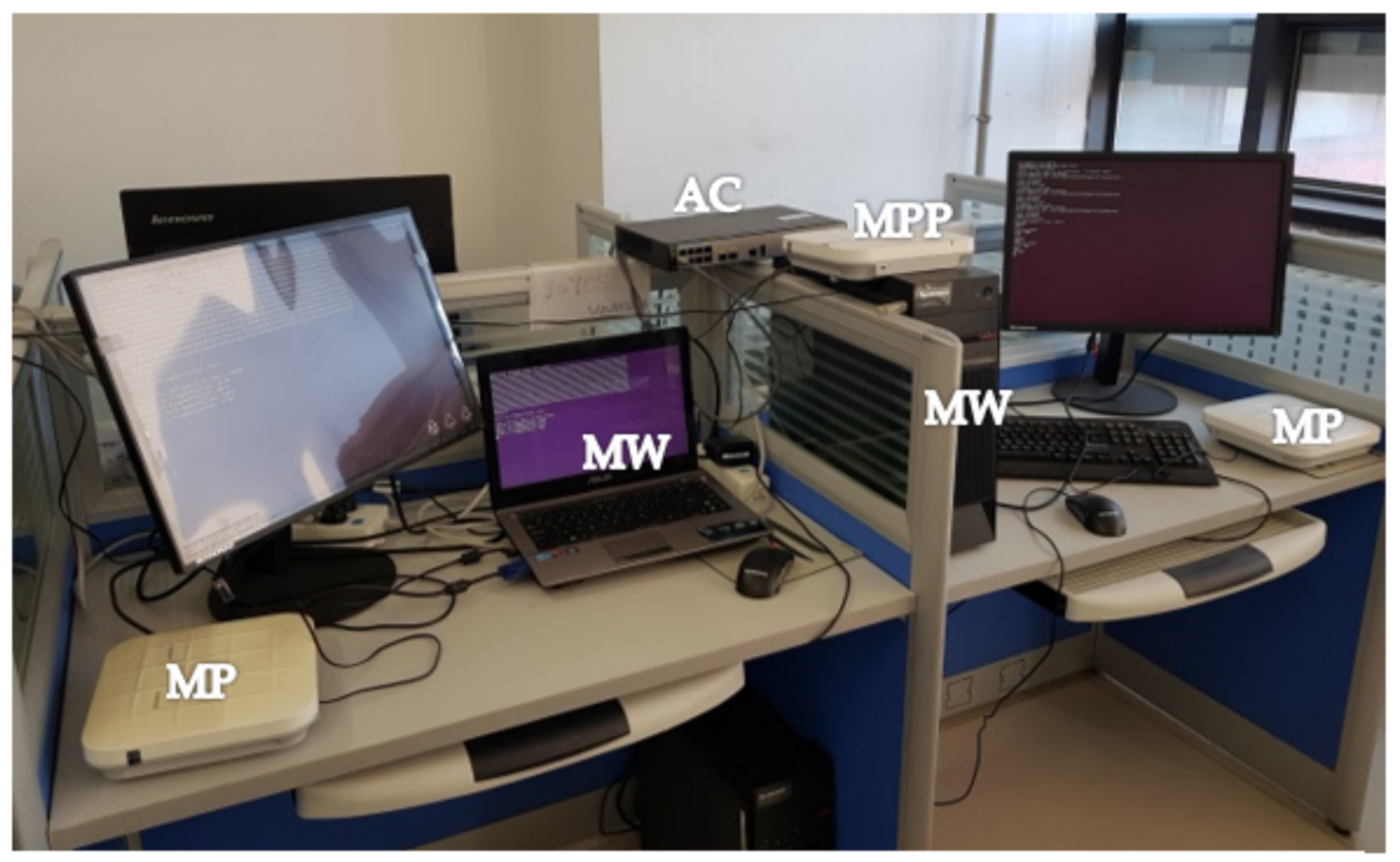
- MP is a wireless network internal connection point that can perform automatic path finding and packet forwarding.
- MPP is an external connection point that can join the WMN or other network types.
- AC is a controller configured to ensure continuous packet forwarding and high reliability.
3.2. The Proposed Delivery Algorithm
| Algorithm 1. Ant colony optimization |
| 01. Input: sub-networks’ throughput. 02. Output: Compute the best throughput for ambulance motorcycles, then the fast network path can follow to achieve efficiency. 03. Initialize the number of network nodes, n, and other parameters. 04. While (the end criterion is not met) do 05. t = t + 1; 06. For k = 1 to n 07. The ambulance motorbike is positioned on a starting node; 08. For m = 2 to hospital node number 09. Send test signals into hospitals according to the probabilistic transition rules; 10. Append return throughput that is calculated according to Equation (1); 11. End for 12. Compute for each hospital node according to Equation (2); 13. Compute the highest throughput according to Equation (3); 14. End for 15. Update the trail throughput for nodes concerning the time; 16. Compute and update the best solution; 17. End while. |
- The problem has to be correctly defined, allowing the middleware to change the solutions incrementally by use of probabilistic transformation rules depending on the amount of throughput in the trail.
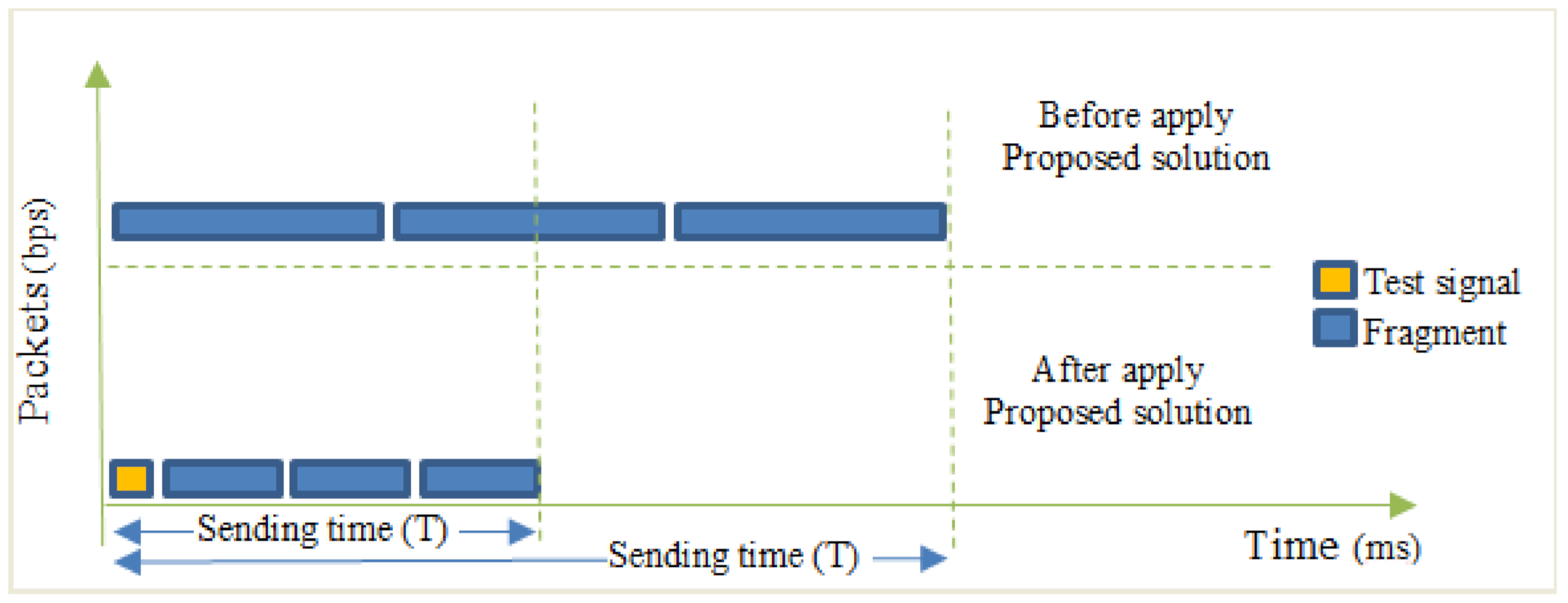
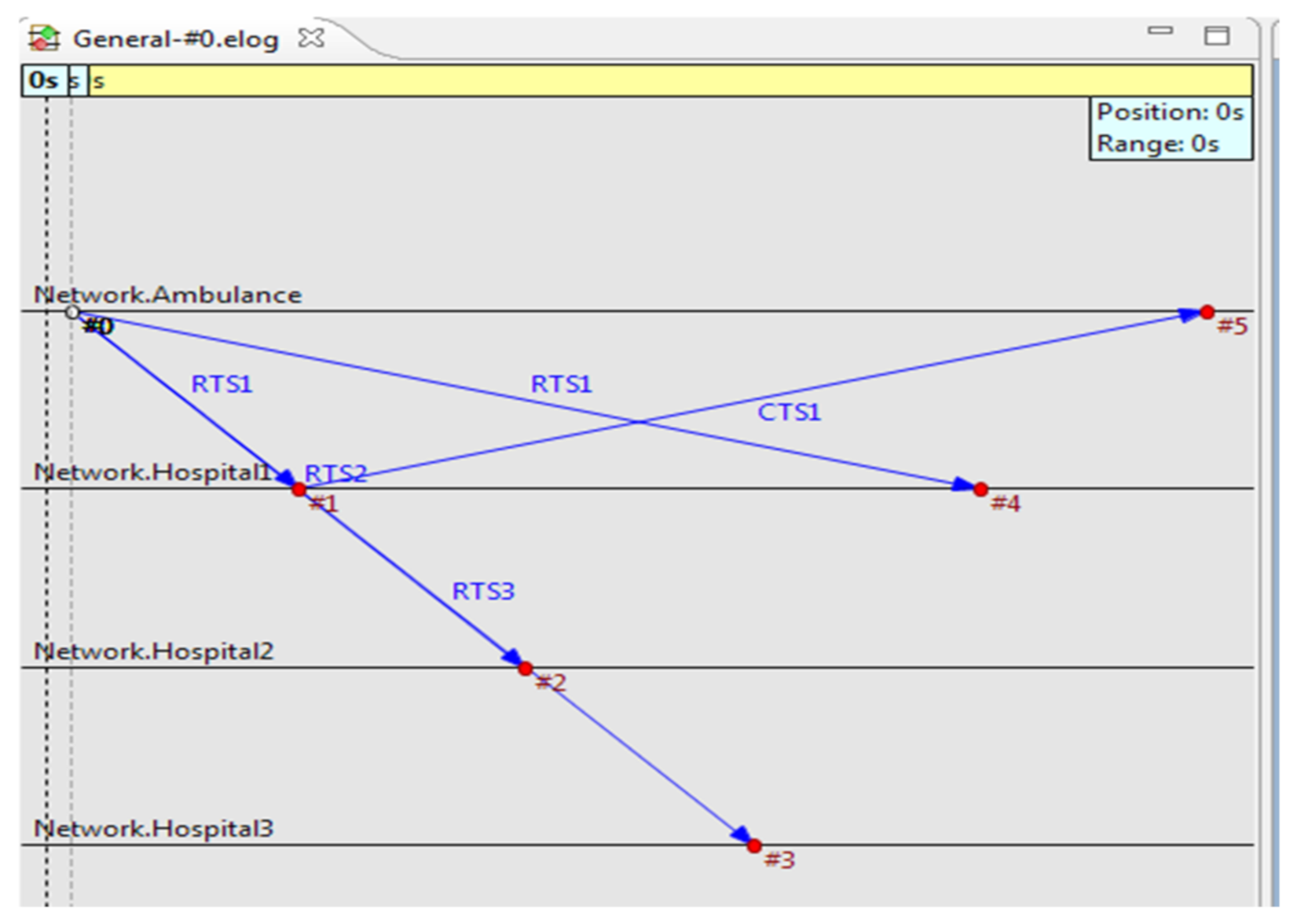
- Give a test signal in various directions and check the highest throughput. Based on the throughput, the device may recommend a link. The machine then redirects all data transfers to the maximum throughput connectivity with the respective hospitals.
- The description and measurement of the production are shown in Equation (1):
- RT, real throughput.
- RTT, round-trip time.
- RWIN, receive window size.
- Describe the heuristic function (η) that calculates the consistency of components that could be applied to the current partial solution to estimate the output.
- The rule set for the output is defined, which calculates how to change the output value (t).
- The probabilistic conversion rule is developed to concentrate on the heuristic function value (η) and the throughput used to create a fast-track assessment approach.
- The likelihood of paths is given in Equation (2):
- , is the feasible neighborhood of the router that the telemedicine project has covered.
- , is the throughput value on the edge (i, j) at the time t.
- is a priori available heuristic information on the edge (i, j) at the time t.
- α is the weight of the throughput.
- β is the weight of the heuristic information.
- The output value at the edge (i, j) at the time (t) is given by Equation (3):
- is the throughput trail evaporation rate (0 < t < 1).
- n is the number of servers.
- is a constant for throughput updating.
3.3. The Proposed Authentication Scheme
| Algorithm 2. Authentication |
|
4. System Implementation
5. Performance Analysis
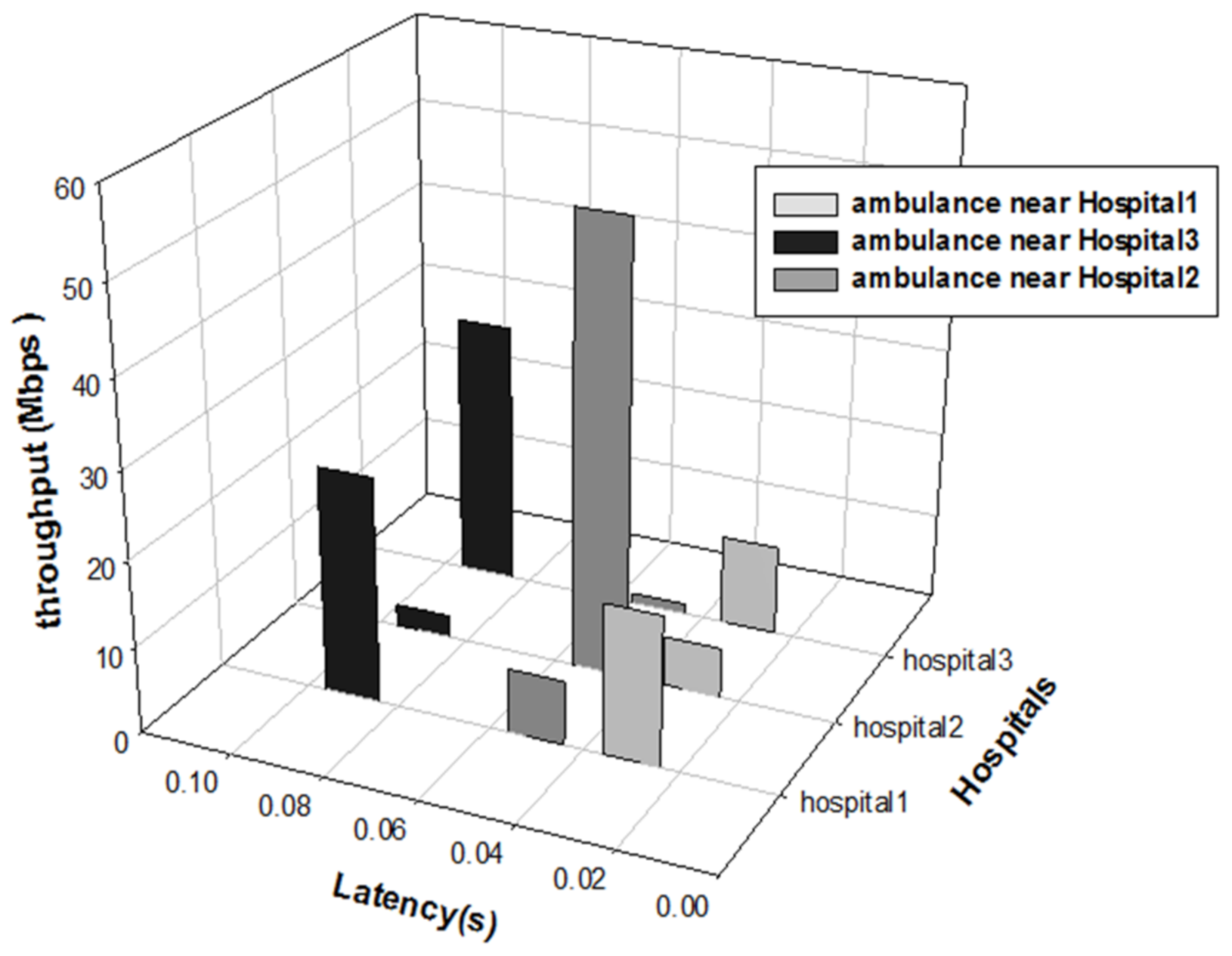
5.1. Throughput Analysis
5.2. Simulation
5.3. Security Analysis
6. Conclusions and Outlook
- The first stage includes a 5G-wireless mesh network and split it into VLANs, where each VLAN represents an independent wireless sub-network.
- The second stage is writing a middleware application that handles the network and determines the closest end-to-end convenient access point using an appropriate algorithm to ensure that the patient is transported urgently to the nearest hospital.
- The third stage is the middleware transmits information to the network and monitors emergency motorbike information in the protected sockets layer to ensure that the maximum degree of secure communication is achieved using the cryptography method. The ant colony hypothesis, one of the SWARM optimization methods recently used to solve short-tracking path problems, was proposed for quick access to the closest medical center.
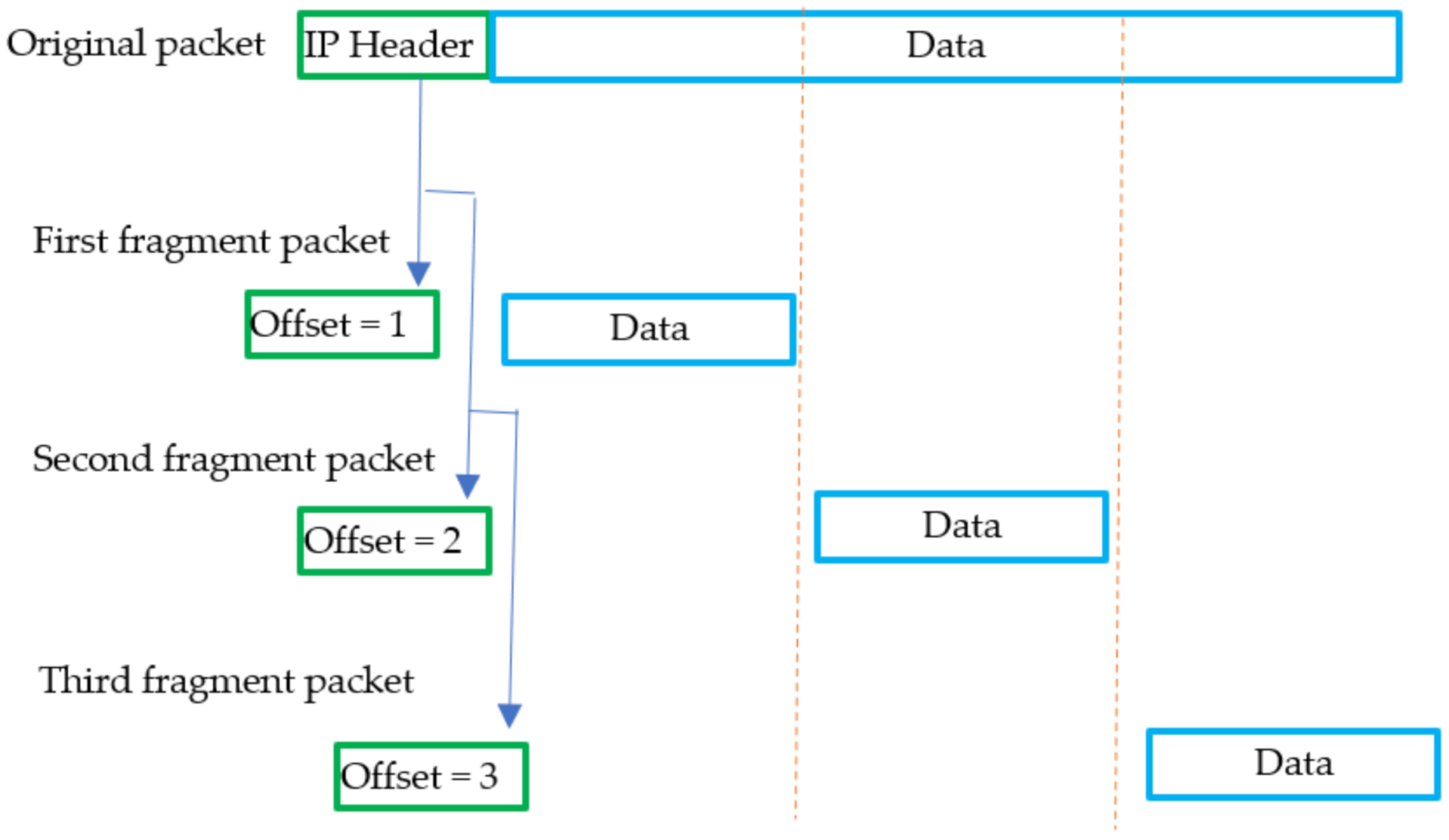
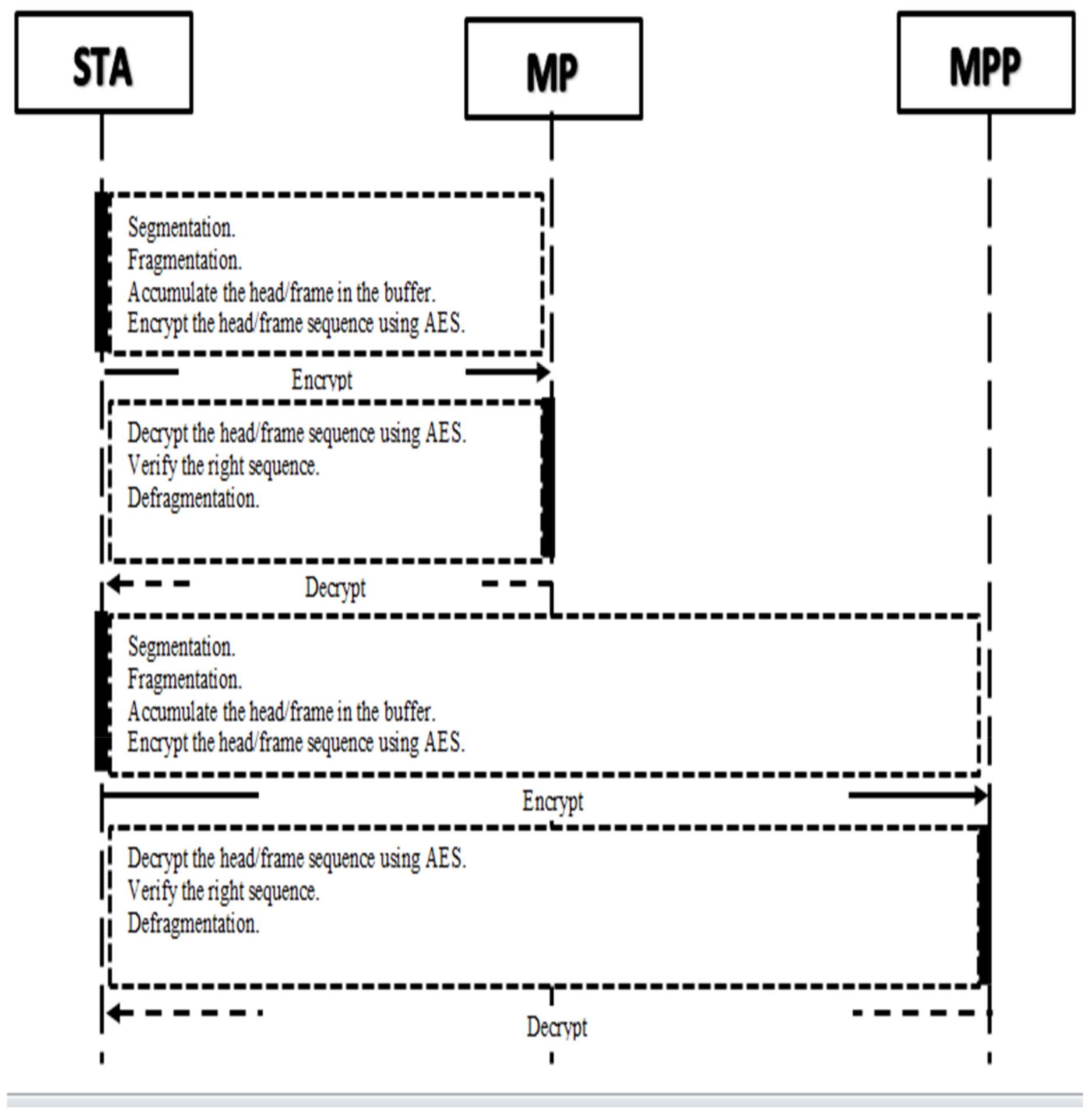
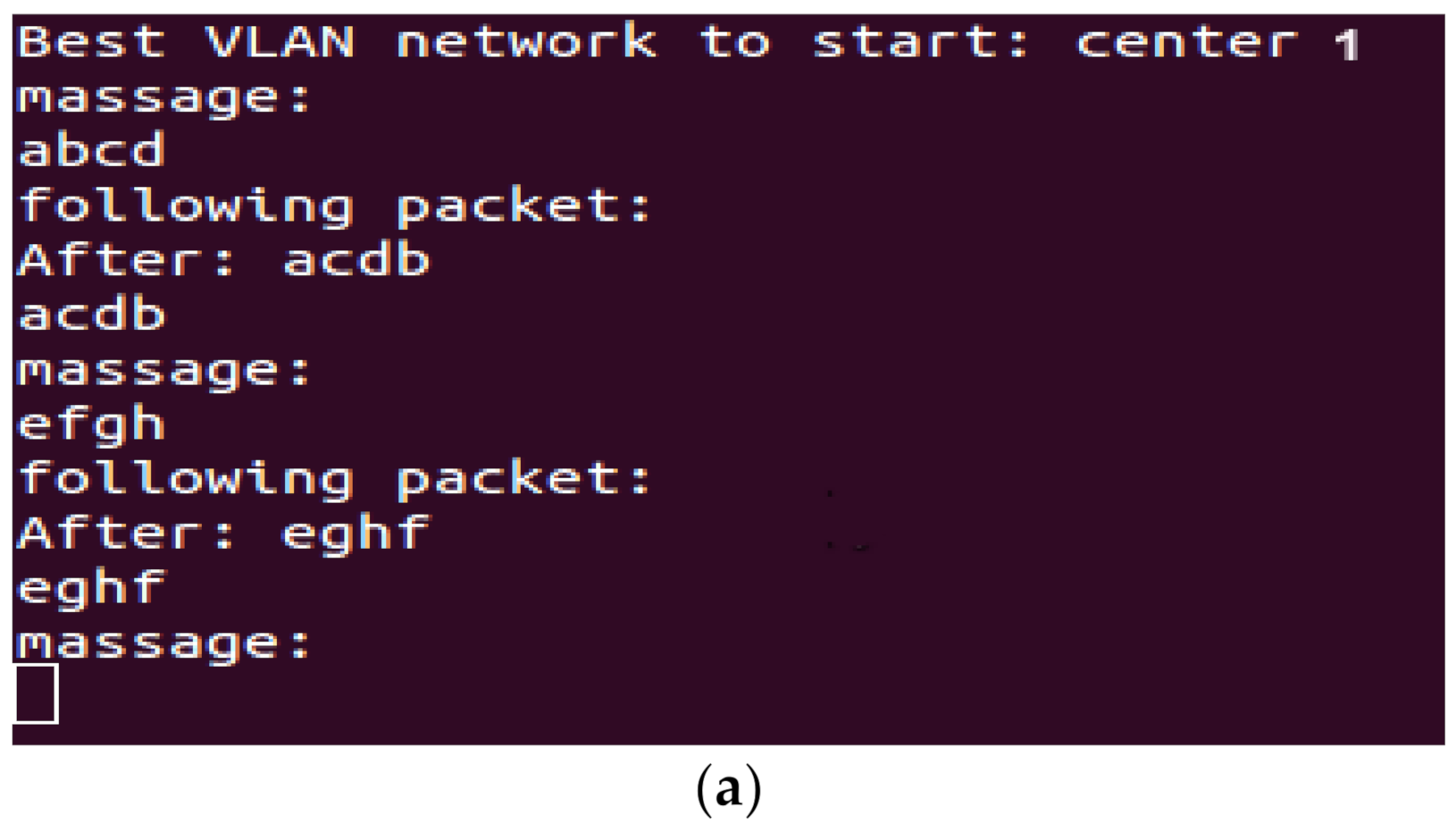
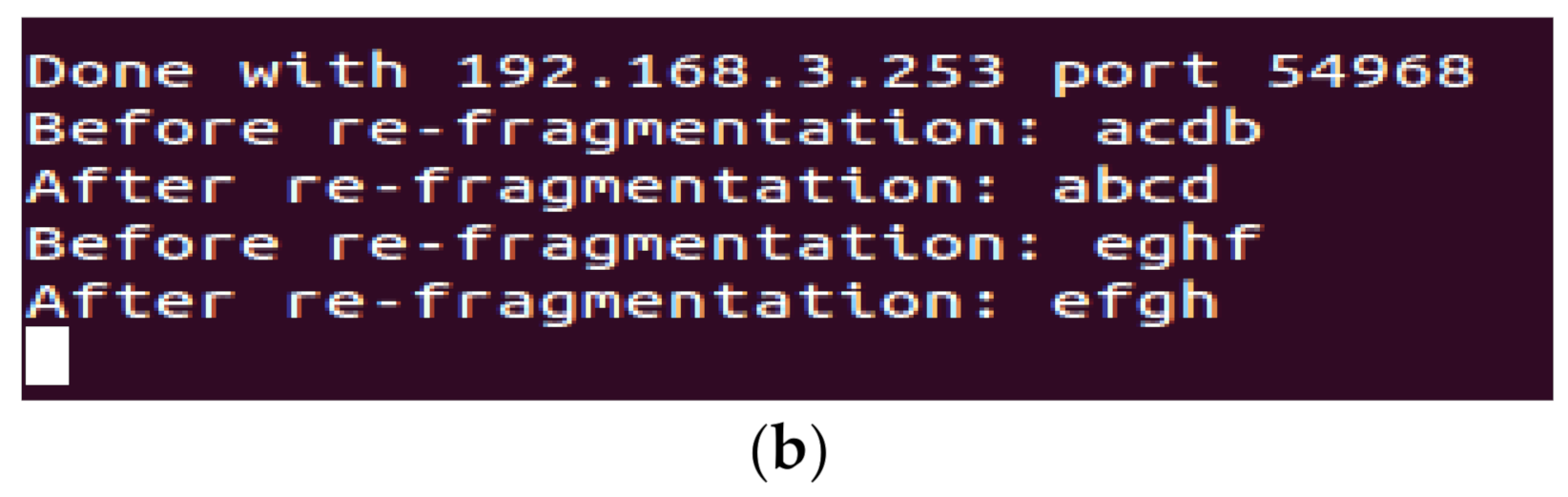
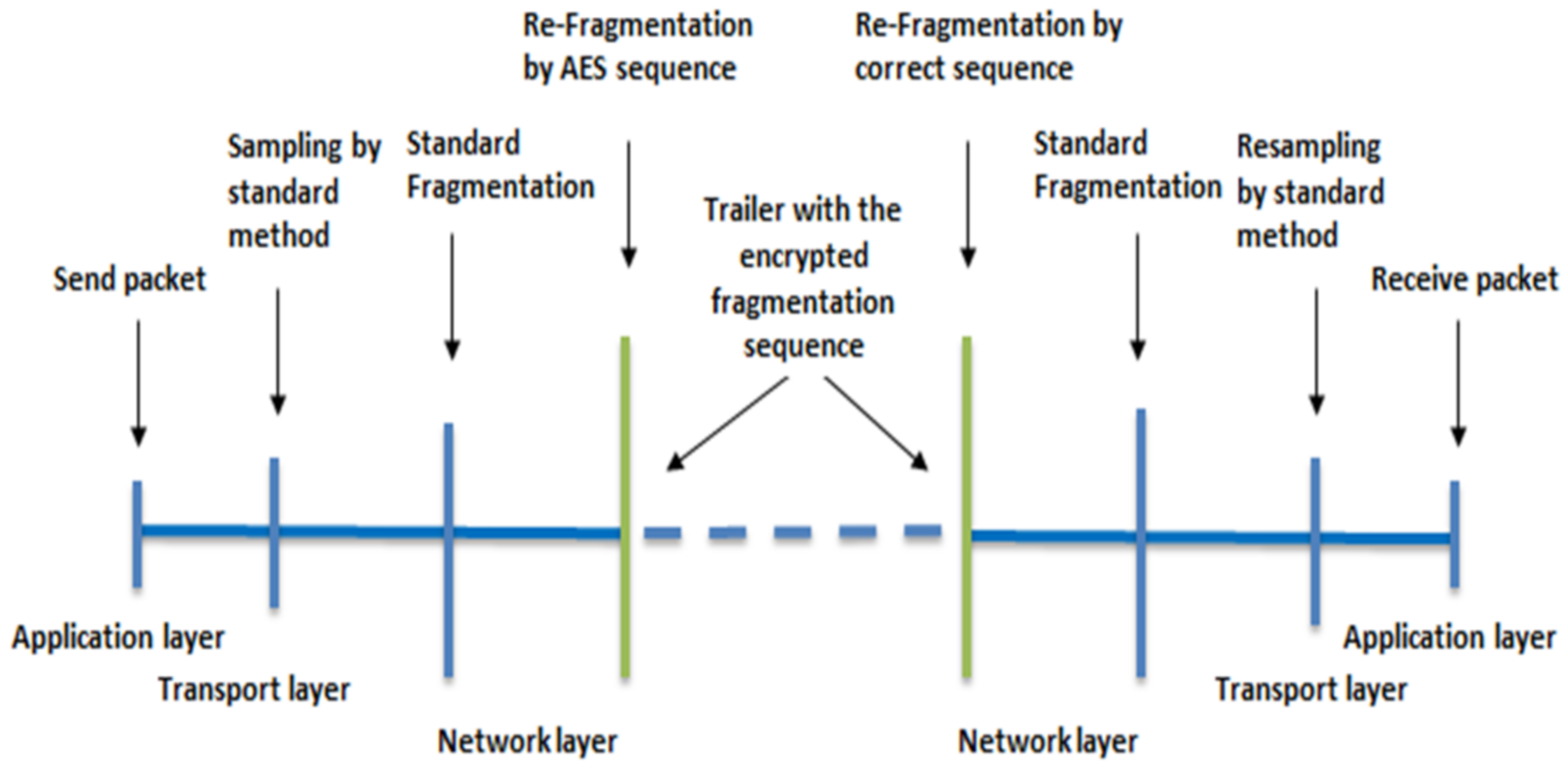
- The fourth stage is security employing the Rijndael encryption to reassemble sequence fragments in the network layer, which was built as a challenge for the authentication part.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Han, Y.; Li, A.; Stevens, A.; Xiao, J.; Yu, J.; Jiang, Z. Improving access to Healthcare Services through an in-Depth Understanding of Telemedicine in China. Value Health 2018, 21, S20. [Google Scholar] [CrossRef]
- Husebø, A.M.L.; Storm, M.; Ødegård, A.; Wegener, C.; Aakjær, M.; Pedersen, A.L.; Østergaard, M.B.; Willumsen, E. Exploring Social Innovation (SI) within the Research Contexts of Higher Education, Healthcare, and Welfare Services—A Scoping Review. Nord. J. Soc. Res. 2021, 12, 72–110. [Google Scholar] [CrossRef]
- Kenoui, M.; Belgacem, K.; Chaffa, G.; Bouderbala, F.Z.; Lakhneche, R.; Oudjoudi, I. First Steps Toward a Full-Web National Telemedicine Portal. In Proceedings of the 2020 2nd International Workshop on Human-Centric Smart Environments for Health and Well-being (IHSH), Boumerdes, Algeria, 9–10 February 2021; pp. 154–159. [Google Scholar]
- Peterson, S. Telehealth in Rural Healthcare. Ph.D. Thesis, The College of St. Scholastica, Duluth, MN, USA, 2021. [Google Scholar]
- Dalmida, S.G.; Foster, P.P.; Mugoya, G.C.; Kirkpatrick, B.; Kraemer, K.R.; Bonner, F.; Merritt, J.; Martinez, L.A. A Community-Engaged, Team-Based Approach to HIV Care and Research in the Mostly Rural Deep South. J. Community Engagem. Scholarsh. 2021, 14, 23. [Google Scholar] [CrossRef]
- Shalom, E.; Goldstein, A.; Ariel, E.; Sheinberger, M.; Jones, V.; Van Schooten, B.; Shahar, Y. Distributed Application of Guideline-Based Decision Support through Mobile Devices: Implementation and Evaluation. arXiv 2021, arXiv:2102.11314. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.J.; Irfan, M.; Jhanjhi, N.Z.; Hussain, K.; Humayun, M. Performance Enhancement in Wireless Body Area Networks with Secure Communication. Wirel. Pers. Commun. 2021, 116, 1–22. [Google Scholar] [CrossRef]
- Ghawy, M.Z.; Amran, G.A.; AlSalman, H.; Ghaleb, E.; Khan, J.; AL-Bakhrani, A.A.; Alziadi, A.M.; Ali, A.; Ullah, S.S. An Effective Wireless Sensor Network Routing Protocol Based on Particle Swarm Optimization Algorithm. Wirel. Commun. Mob. Comput. 2022, 2022, 13. [Google Scholar] [CrossRef]
- Oh Nelson, H. Doctor–Patient Relationship. Wiley Blackwell Companion Med. Sociol. 2021, 495–515. [Google Scholar] [CrossRef]
- Alsamhi, S.H.; Afghah, F.; Sahal, R.; Hawbani, A.; Al-qaness, M.A.; Lee, B.; Guizani, M. Green Internet of Things Using UAVs in B5G Networks: A Review of Applications and Strategies. Ad Hoc Netw. 2021, 117, 102505. [Google Scholar] [CrossRef]
- Garg, D.; Sharma, D.K.; Mani, P.; Kaushik, B.K. A Comprehensive Survey on the Internet of Things (IoT) in Healthcare. In The Role of the Internet of Things (IoT) in Biomedical Engineering: Present Scenario and Challenges; Apple Academic Press: Waretown, NJ, USA, 2022; p. 157. [Google Scholar]
- Li, M.; Lukyanenko, A.; Ou, Z.; Ylä-Jääski, A.; Tarkoma, S.; Coudron, M.; Secci, S. Multipath Transmission for the Internet: A Survey. IEEE Commun. Surv. Tutor. 2016, 18, 2887–2925. [Google Scholar] [CrossRef]
- Kotenko, I.V.; Kolomeets, M.; Chechulin, A.; Chevalier, Y. A Visual Analytics Approach for the Cyber Forensics Based on Different Views of the Network Traffic. J. Wirel. Mob. Networks Ubiquitous Comput. Dependable Appl. 2018, 9, 57–73. [Google Scholar]
- Choudhary, G.; Kim, J.; Sharma, V. Security of 5G-Mobile Backhaul Networks: A Survey. arXiv 2019, arXiv:1906.11427. [Google Scholar]
- Kotenko, I.V.; Saenko, I.; Kushnerevich, A. Parallel Big Data Processing System for Security Monitoring in Internet of Things Networks. J. Wirel. Mob. Networks Ubiquitous Comput. Dependable Appl. 2017, 8, 60–74. [Google Scholar] [CrossRef]
- Majeed, A.; Zia, T.A. Multi-Layer Network Architecture for Supporting Multiple Applications in Wireless Sensor Networks. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2017, 8, 36–56. [Google Scholar]
- De La Torre, G.; Rad, P.; Choo, K.-K.R. Driverless Vehicle Security: Challenges and Future Research Opportunities. Future Gener. Comput. Syst. 2020, 108, 1092–1111. [Google Scholar] [CrossRef]
- Sanchez-Iborra, R.; Gómez, J.S.; Santa, J.; Fernández, P.J.; Skarmeta, A.F. Integrating LP-WAN Communications within the Vehicular Ecosystem. J. Internet Serv. Inf. Secur. 2017, 7, 45–56. [Google Scholar]
- Panayides, A.S.; Pattichis, M.S.; Pantziaris, M.; Constantinides, A.G.; Pattichis, C.S. The Battle of the Video Codecs in the Healthcare Domain-a Comparative Performance Evaluation Study Leveraging VVC and AV1. IEEE Access 2020, 8, 11469–11481. [Google Scholar] [CrossRef]
- Shen, Y.; Zhang, H.; Fan, Y.; Lee, A.P.; Xu, L. Smart Health of Ultrasound Telemedicine Based on Deeply Represented Semantic Segmentation. IEEE Internet Things J. 2020, 8, 16770–16778. [Google Scholar] [CrossRef]
- Abu-Rmaileh, M.; Osborn, T.; Gonzalez, S.R.; Yuen, J.C. The Use of Live Streaming Technologies in Surgery: A Review of the Literature. Ann. Plast. Surg. 2022, 88, 122–127. [Google Scholar] [CrossRef]
- Rezaeibagha, F.; Mu, Y. Practical and Secure Telemedicine Systems for User Mobility. J. Biomed. Inform. 2018, 78, 24–32. [Google Scholar] [CrossRef]
- Kane-Gill, S.L.; Rincon, F. Expansion of Telemedicine Services: Telepharmacy, Telestroke, Teledialysis, Tele–Emergency Medicine. Crit. Care Clin. 2019, 35, 519–533. [Google Scholar] [CrossRef]
- Swaraja, K.; Meenakshi, K.; Kora, P. An Optimized Blind Dual Medical Image Watermarking Framework for Tamper Localization and Content Authentication in Secured Telemedicine. Biomed. Signal Process. Control 2020, 55, 101665. [Google Scholar]
- Khan, W.U.; Li, X.; Ihsan, A.; Khan, M.A.; Menon, V.G.; Ahmed, M. NOMA-Enabled Optimization Framework for next-Generation Small-Cell IoV Networks under Imperfect SIC Decoding. IEEE Trans. Intell. Transp. Syst. 2021, 1–10. [Google Scholar] [CrossRef]
- Huang, S.; Gui, J.; Wang, T.; Li, X. Joint Mobile Vehicle–UAV Scheme for Secure Data Collection in a Smart City. Ann. Telecommun. 2021, 76, 559–580. [Google Scholar] [CrossRef]
- Jameel, F.; Khan, W.U.; Kumar, N.; Jäntti, R. Efficient Power-Splitting and Resource Allocation for Cellular V2X Communications. IEEE Trans. Intell. Transp. Syst. 2020, 22, 3547–3556. [Google Scholar] [CrossRef]
- Khan, W.U.; Nguyen, T.N.; Jameel, F.; Jamshed, M.A.; Pervaiz, H.; Javed, M.A.; Jäntti, R. Learning-Based Resource Allocation for Backscatter-Aided Vehicular Networks. IEEE Trans. Intell. Transp. Syst. 2021, 1–5. [Google Scholar] [CrossRef]
- Khan, W.U.; Ihsan, A.; Nguyen, T.N.; Javed, M.A.; Ali, Z. NOMA-Enabled Backscatter Communications for Green Transportation in Automotive-Industry 5.0. IEEE Trans. Ind. Inform. 2022. [Google Scholar] [CrossRef]
- Wang, T.; Li, G.; Ding, J.; Miao, Q.; Li, J.; Wang, Y. 5G Spectrum: Is China Ready? IEEE Commun. Mag. 2015, 53, 58–65. [Google Scholar] [CrossRef]
- Rahim, A.; Kong, X.; Xia, F.; Ning, Z.; Ullah, N.; Wang, J.; Das, S.K. Vehicular Social Networks: A Survey. Pervasive Mob. Comput. 2018, 43, 96–113. [Google Scholar] [CrossRef]
- Ahmad, N.A.; Kidam, K.; Mohsin, R. Wireless Mesh Network Infrastructure and Communication Challenges in Emergency Response. In AIP Conference Proceedings; AIP Publishing LLC: Melville, NY, USA, 2021; Volume 2401, p. 020002. [Google Scholar]
- Taleb, S.M.; Meraihi, Y.; Gabis, A.B.; Mirjalili, S.; Ramdane-Cherif, A. Nodes Placement in Wireless Mesh Networks Using Optimization Approaches: A Survey. Neural Comput. Appl. 2022, 1–37. [Google Scholar] [CrossRef]
- Junior, N.D.S.R.; Vieira, M.A.; Vieira, L.F.; Gnawali, O. SplitPath: High Throughput Using Multipath Routing in Dual-Radio Wireless Sensor Networks. Comput. Netw. 2022, 207, 108832. [Google Scholar]
- Thirugnanasambandam, K.; Rajeswari, M.; Bhattacharyya, D.; Kim, J. Directed Artificial Bee Colony Algorithm with Revamped Search Strategy to Solve Global Numerical Optimization Problems. Autom. Softw. Eng. 2022, 29, 1–31. [Google Scholar] [CrossRef]
- Valencia-Rodríguez, D.C.; Coello Coello, C.A. A Study of Swarm Topologies and Their Influence on the Performance of Multi-Objective Particle Swarm Optimizers. In International Conference on Parallel Problem Solving from Nature; Springer: Cham, Switzerland, 2020; pp. 285–298. [Google Scholar]
- Kumari, P.; Sahana, S.K. PSO-DQ: An Improved Routing Protocol Based on PSO Using Dynamic Queue Mechanism for MANETs. J. Inf. Sci. Eng. 2022, 38, 41–56. [Google Scholar]
- Gao, T.; Al-shammari, M.K.M. A Secure and Efficient System for Ambulance Vehicular Social Network Based on Re-Fragmentation and Swarm. IT CoNvergence PRActice INPRA 2018, 6, 1–8. [Google Scholar]
- Osman, O.M.; Kanona, M.E.A.; Hassan, M.K.; Elkhair, A.A.E.; Mohamed, K.S. Hybrid Multistage Framework for Data Manipulation by Combining Cryptography and Steganography. Bull. Electr. Eng. Inform. 2022, 11, 327–335. [Google Scholar] [CrossRef]
- Al-Shareeda, M.A.; Anbar, M.; Manickam, S.; Hasbullah, I.H. A Secure Pseudonym-Based Conditional Privacy-Preservation Authentication Scheme in Vehicular Ad Hoc Networks. Sensors 2022, 22, 1696. [Google Scholar] [CrossRef]
- Humayed, A.; Lin, J.; Li, F.; Luo, B. Cyber-Physical Systems Security—A Survey. IEEE Internet Things J. 2017, 4, 1802–1831. [Google Scholar] [CrossRef]
- Patel, R.L.; Pathak, M.J.; Nayak, A.J. Survey on Network Simulators. Int. J. Comput. Appl. 2018, 182, 21. [Google Scholar]
- Lee, E.A.; Seshia, S.A. Introduction to Embedded Systems: A Cyber-Physical Systems Approach; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Gopi, S.P.; Magarini, M.; Alsamhi, S.H.; Shvetsov, A.V. Machine Learning-Assisted Adaptive Modulation for Optimized Drone-User Communication in B5g. Drones 2021, 5, 128. [Google Scholar] [CrossRef]
- Younis, M.I.; Majeed, G.H. A Fully Computerized Method to Backup the Router Configuration File. Al-Khwarizmi Eng. J. 2007, 3, 89–100. [Google Scholar]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviations | Describes |
|---|---|
| VSN | Vehicle social network |
| ACO | Ant colony optimization |
| SSL | Secure socket layer |
| AES | Advanced encryption standard |
| IoT | Internet of Things |
| PEM | Personal ECG monitor |
| ECGs | Electrocardiogram |
| MHU | Mobile health unit |
| UTMB | University of Texas Medical Branch |
| TTHSC | Texas Tech Health Science Centre |
| MU | Medical unit |
| PU | Patient unit |
| BASN | Body area sensor networks |
| QoS | Quality of service |
| AVs | Autonomous vehicles |
| LP-WAN | Low power–wide area network |
| LZW | Lempel-Ziv-Welch |
| NOMA | Non-orthogonal multi-access |
| V2X | Vehicular-to-everything |
| VLANs | Virtual local area networks |
| IoV | Internal-of-vehicle |
| SN | Social Network |
| WMNs | Wireless mesh networks |
| WLAN | Wireless local area network |
| APs | Access points |
| AC | Access controller |
| TLS | Transport layer security |
| TL | Transport layer |
| GUI | Graphical user interface |
| NDF | Network diagnostics file |
| STA | Station |
| RTS | Request test signal |
| CTS | Conform test signal |
| MP | Mesh point |
| MPP | Mesh portal point |
| MSS | Maximum segment size |
| Device | Type | My Net | Radio | Configuration |
|---|---|---|---|---|
| AP1 | AP6010DN | 192.168.1.1/24 | Center1 | Channel 40 MHz-plus 157 |
| AP2 | AP6010DN | 192.168.2.1/24 | Center2 | Ap-region 102, 102, 103 |
| AP3 | AP6010DN | 192.168.3.1/24 | Center3 | Forward mode |
| AC | AC6605 | VLAN 100 | mesh1 | p/w: 12345678 |
| Scenario | Hospitals | Window Size (KB) | Round-Trip Latency (S) | Throughput (Mbps) |
|---|---|---|---|---|
| Near From Hospital 1 | Hospital 1 | 64 | 0.03 | 17.47626667 |
| Hospital 2 | 64 | 0.09 | 5.825422222 | |
| Hospital 3 | 64 | 0.05 | 10.48576 | |
| Near From Hospital 3 | Hospital 1 | 64 | 0.02 | 26.2144 |
| Hospital 2 | 64 | 0.2 | 2.62144 | |
| Hospital 3 | 64 | 0.017 | 30.84047059 | |
| Near From Hospital 2 | Hospital 1 | 64 | 0.07 | 7.489828571 |
| Hospital 2 | 64 | 0.01 | 52.4288 | |
| Hospital 3 | 64 | 0.44 | 1.191563636 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahmoud, H.H.; Alghawli, A.S.; Al-shammari, M.K.M.; Amran, G.A.; Mutmbak, K.H.; Al-harbi, K.H.; Al-qaness, M.A.A. IoT-Based Motorbike Ambulance: Secure and Efficient Transportation. Electronics 2022, 11, 2878. https://doi.org/10.3390/electronics11182878
Mahmoud HH, Alghawli AS, Al-shammari MKM, Amran GA, Mutmbak KH, Al-harbi KH, Al-qaness MAA. IoT-Based Motorbike Ambulance: Secure and Efficient Transportation. Electronics. 2022; 11(18):2878. https://doi.org/10.3390/electronics11182878
Chicago/Turabian StyleMahmoud, Halah Hasan, Abed Saif Alghawli, Marwan Kadhim Mohammed Al-shammari, Gehad Abdullah Amran, Khaled H. Mutmbak, Khaled H. Al-harbi, and Mohammed A. A. Al-qaness. 2022. "IoT-Based Motorbike Ambulance: Secure and Efficient Transportation" Electronics 11, no. 18: 2878. https://doi.org/10.3390/electronics11182878