


FPGA-Based Decision Support System for ECG Analysis



Abstract
:1. Introduction
- The development of an automatic classifier, which should be suitable as a decision support system;
- The soft real-time implementation of the classifier on FPGA for a low-cost/low-power device;
- The evaluation of CAD (software) and hardware performance;
- Comparative benchmarking for assessing the method validity
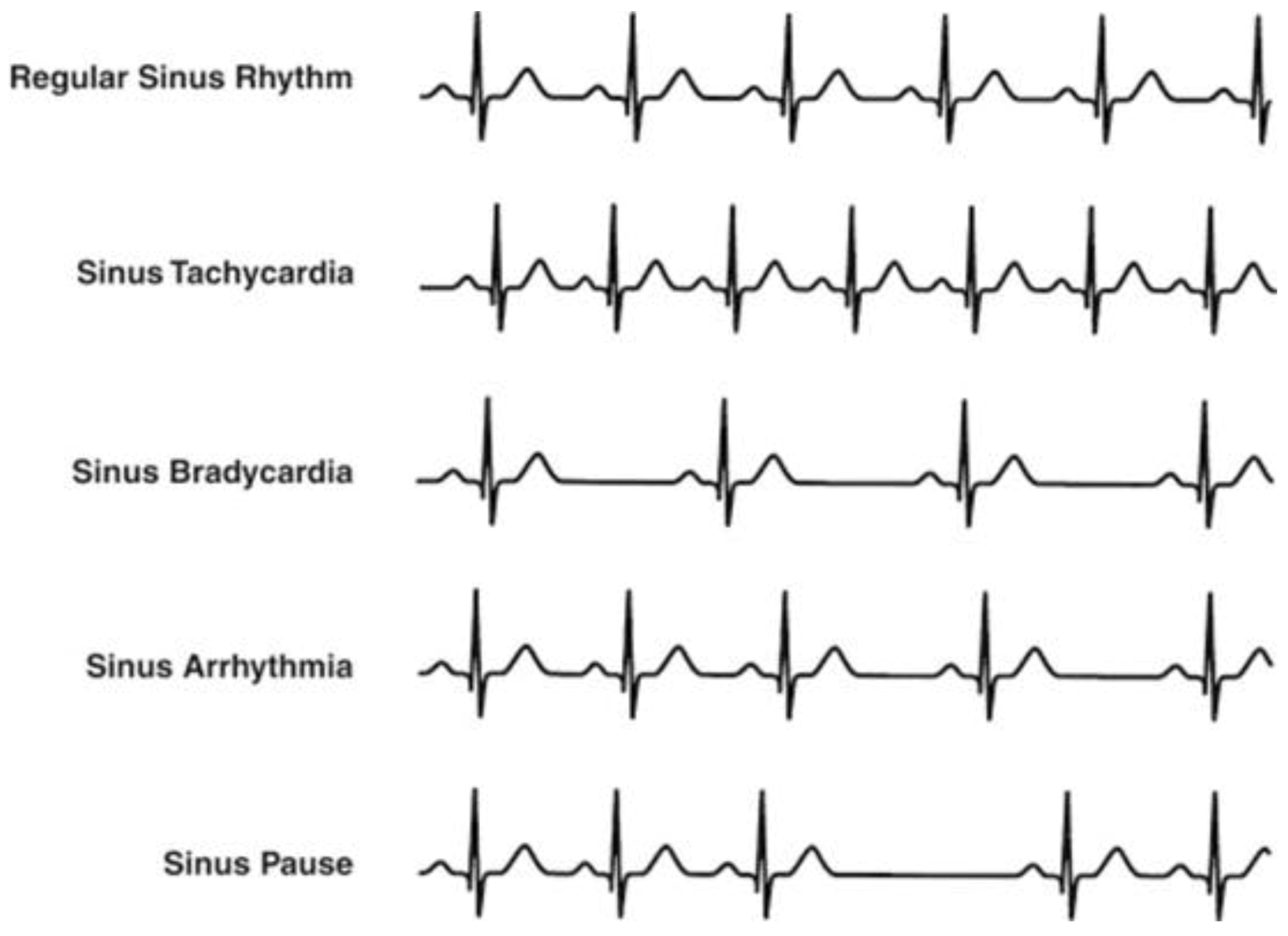
2. Implemented Diagnostic Procedure
- Arrhythmias;
- Tachycardia;
- Bradycardia;
- Arrhythmias in presence of tachycardia;
- Arrhythmias in presence of bradycardia;
- Irregular heartbeat, followed by tachycardia/bradycardia, succeeded by normal cardiac rhythm;
- Pulmonary embolism risk;
- Variations (lengthening) of the QT segment.
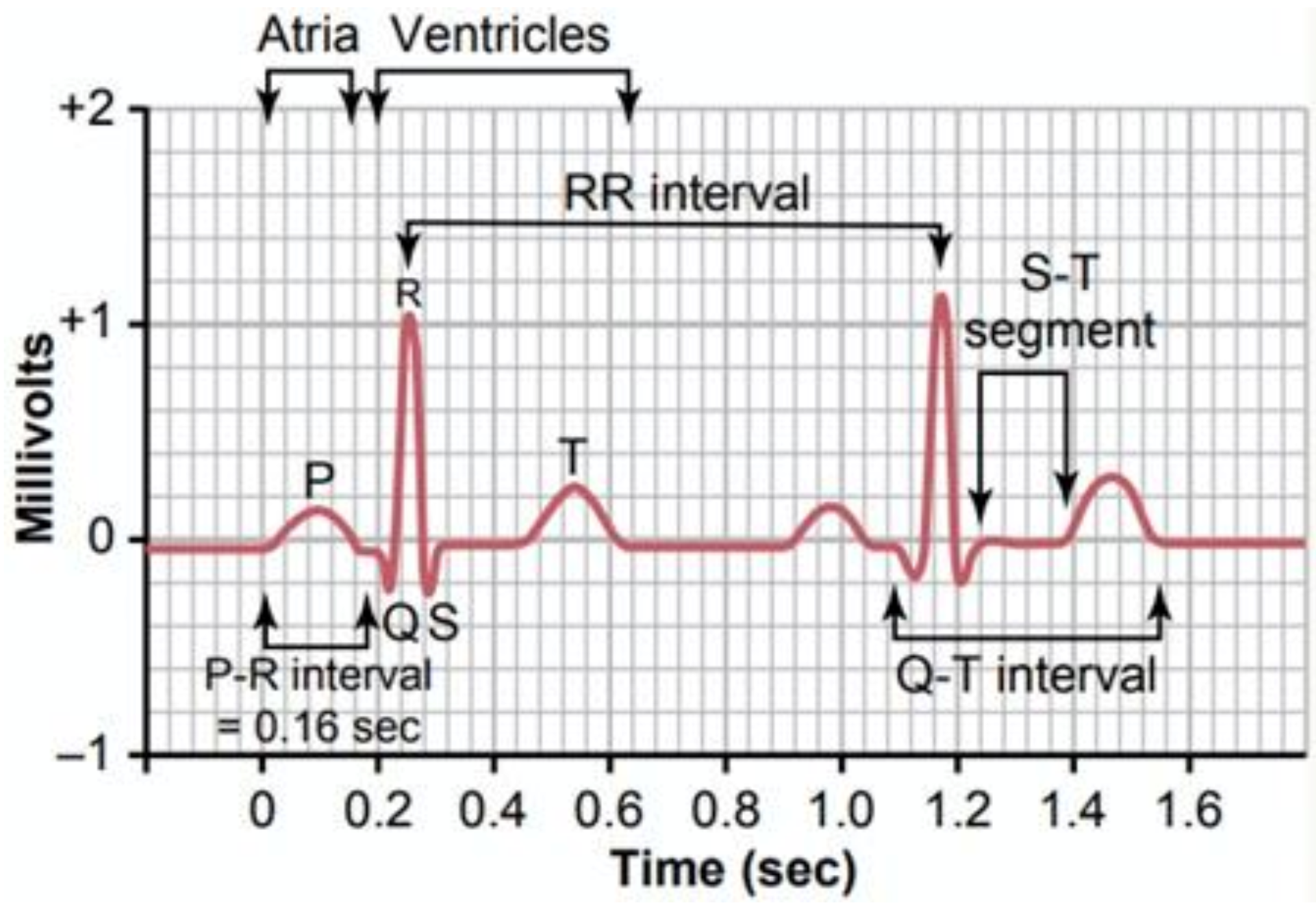
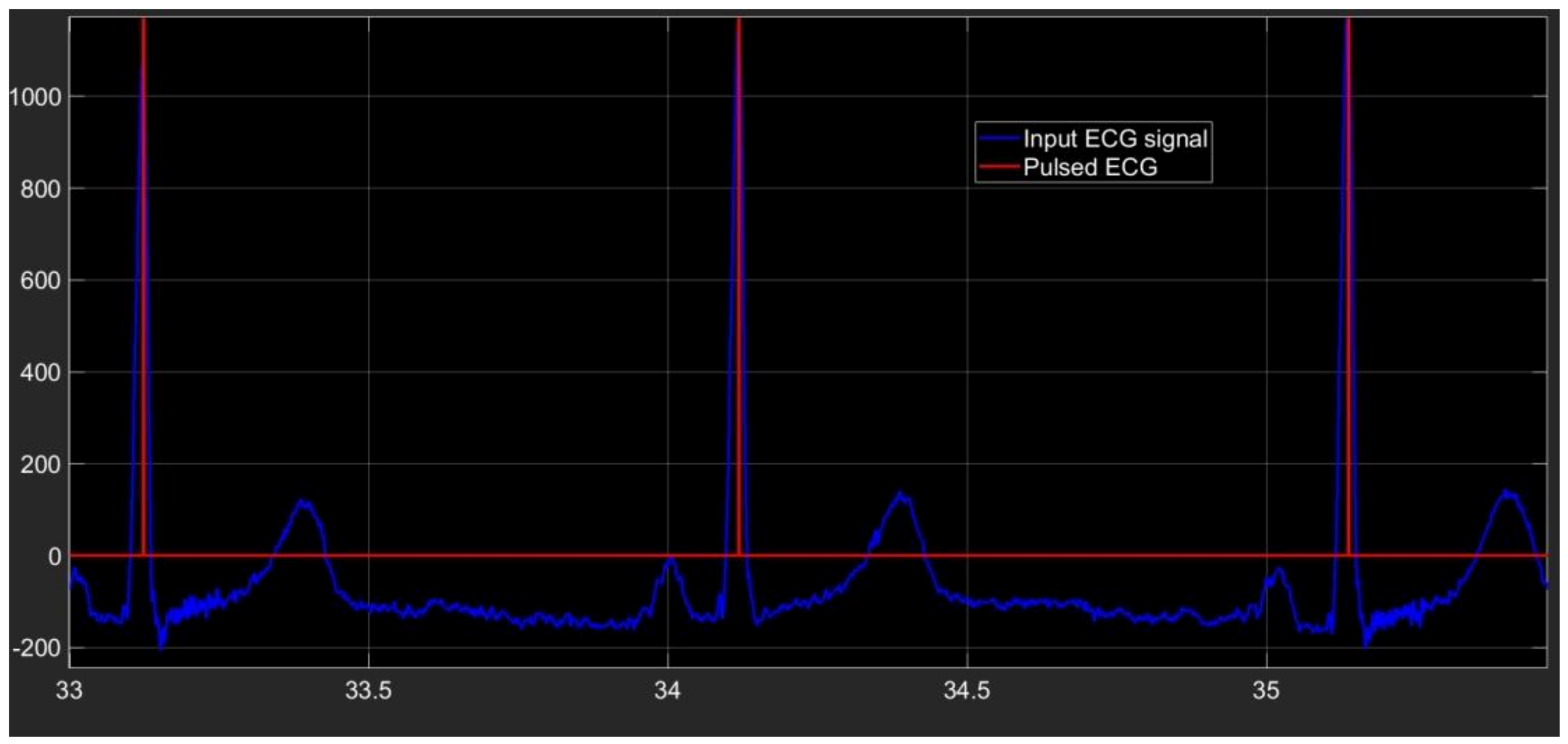
2.1. Preprocessing Phase
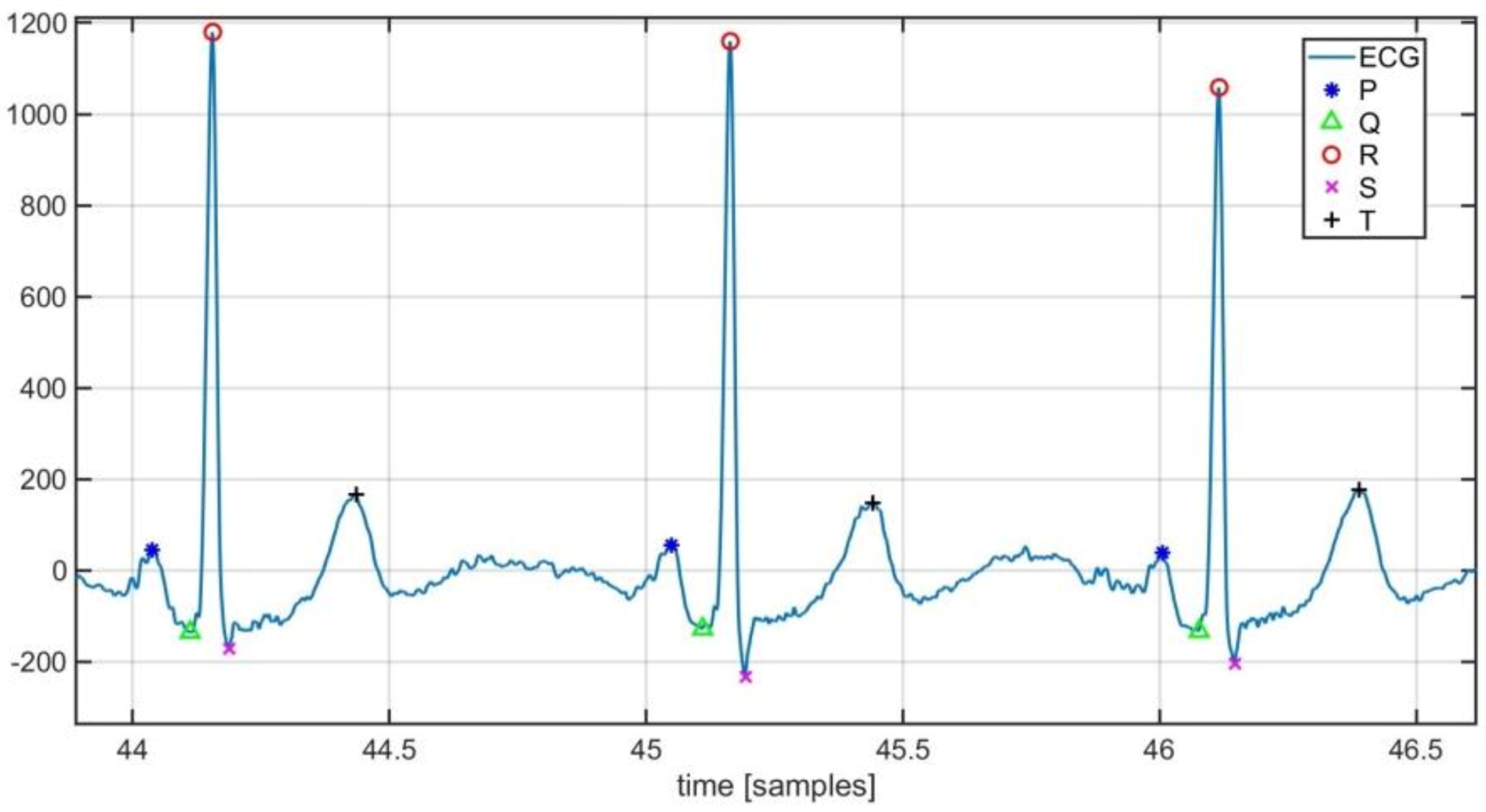
2.2. Segmentation
- ✓
- The S-wave by examining the ECG signal ranged between the ith R point and the middle of the ith cardiac cycle, looking for the minimum point. The following pseudo-code is used:for ii = 1:(length(peakRLocend)−1)[peakSMagend(ii)peakSLocend(ii)] = min ecg(peakRLocend(ii):(peakRLocend(ii) + (peakRLocend(ii + 1)-peakRLocend(ii))/2)));peakSLocend(ii) = peakRLocend(ii) + peakSLocend(ii);end
- ✓
- The T-wave by considering the ECG signal ranged between the ith S point and the middle of the ith cardiac cycle, looking for the maximum point. The following pseudo-code is used:for ii = 1:(length(peakRLocend)−1)[peakTMagend(ii)peakTLocend(ii)] = max (ecg(peakSLocend(ii):(peakRLocend(ii) + (peakRLocend(ii + 1)-peakRLocend(ii))/2)));peakTLocend(ii) = peakSLocend(ii) + peakTLocend(ii);end
- ✓
- The Q-wave by taking into account the portion of the ECG within the middle of the ith cardiac cycle and the (i + 1)th R peak according to the following pseudo-codefor ii = 1:(length(peakRLocend)−1)[peakQMagend(ii)peakQLocend(ii)] = min (ecg((peakRLocend(ii) + (peakRLocend(ii + 1)-peakRLocend(ii))/2):(peakRLocend(ii + 1))));peakQLocend(ii) = peakRLocend(ii) + (peakRLocend(ii + 1)-peakRLocend(ii))/2 + peakQLocend(ii);end
- ✓
- The P-wave by seeking the maximum point in the ECG part ranged between the middle of the ith cardiac cycle and the Q-wave belonging to the ith cardiac cycle. The following pseudo-code is used:for ii = 1:length(peakQLocend)a = round((peakRLocend(ii + 1)-peakRLocend(ii))*2/3);[peakPMagend(ii)peakPLocend(ii)] = max (ecg((peakRLocend(ii) + a):(peakQLocend(ii))));peakPLocend(ii) = peakRLocend(ii) + a+peakPLocend(ii);end
2.3. Classification Phase
2.4. Adopted Database
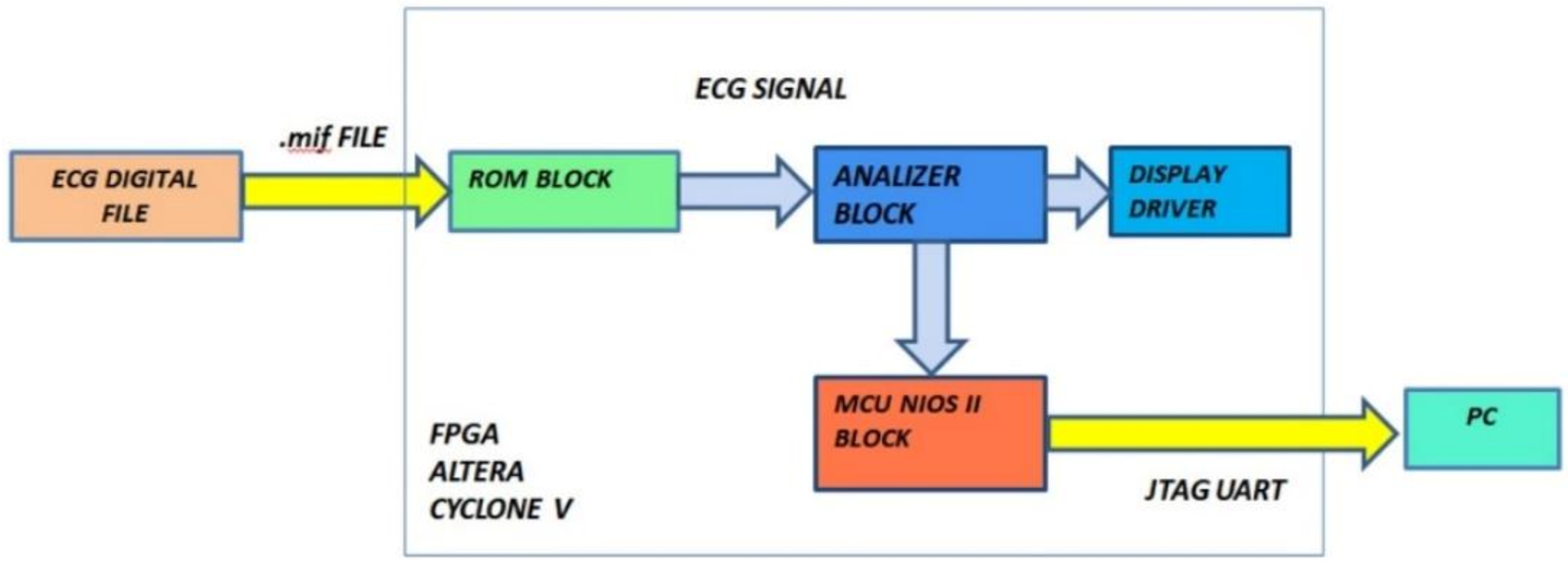
3. Hardware Architecture of the FPGA-Based Embedded System
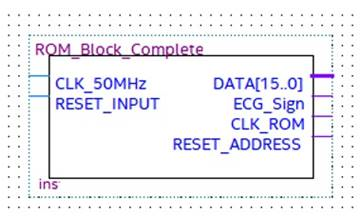
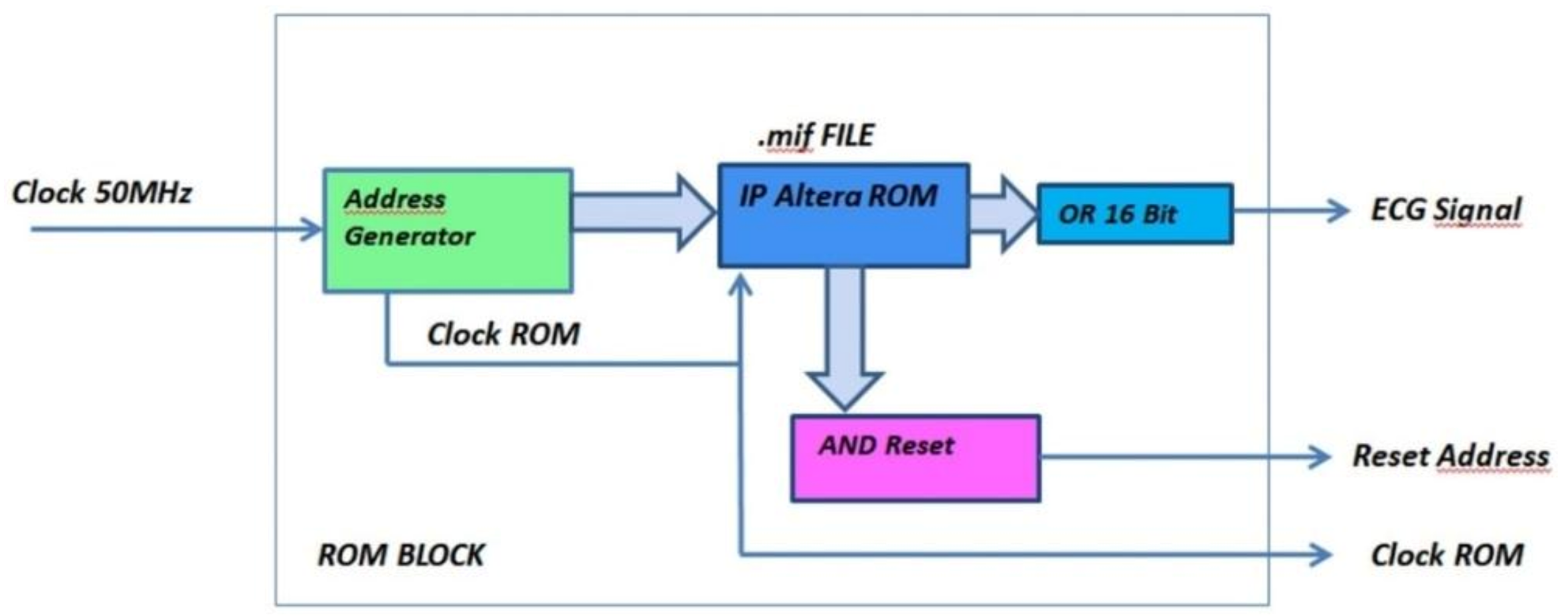
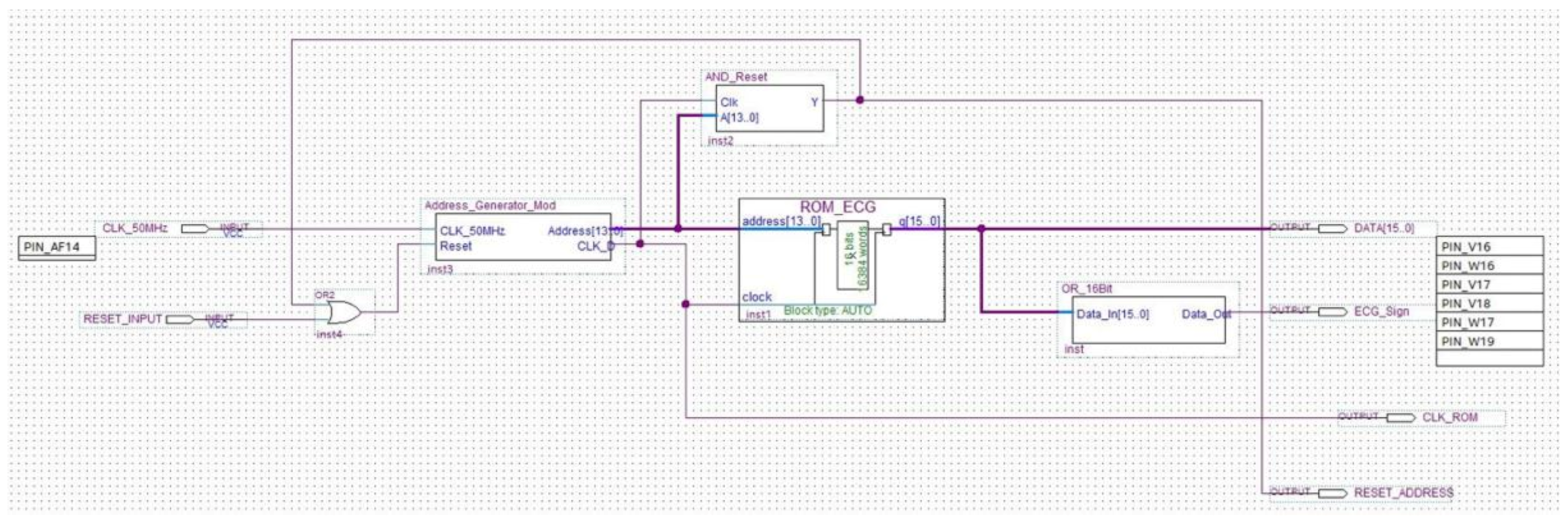
3.1. ROM Module
- -
- DATA [15…0], which is a 16-bit word pointed to by the address counter, which tests and checks the block operations;
- -
- ECG_Signal, which is the pulsed transformed ECG signal under test;
- -
- CLK_ROM, which is the timing signal of the ROM address counter;
- -
- Reset_Address, which is the reset signal generated after the whole ROM has analyzed, which stops the process.
- Address Generator: generates both the clock signal to accurately reproduce the ECG signal acquisition frequency and the 16-bit address for driving the ROM memory bank. The number of bits composing the address is equal to the bits forming the binary representation of the ECG sample amplitude;
- AND Reset: generates a reset signal as soon as the Address Generator counter has reached the binary value 1111111111111111. In such a situation, the analysis can be stopped because the ROM has been completely read and the whole signal has been processed;
- OR_16Bit: makes the logical sum on each of the 16-bit words stored into the ROM. According to the Boolean algebra, OR gate output is set at logical value 1 if at least one input is equal to 1, while a 0 output happens if all inputs are set at logical value 0. A logic 1 output occurs when a pulse (R peak) is recorded into the ROM block (being the OR inputs equal to 1111111111111111), and a logic 0 output takes place when no R peak is stored in the ROM (since the OR inputs are 0000000000000000). The analysis is so restricted to a single bit, which is the OR output instead of 16 bits, because only the moment at which the pulse occurs is relevant for diagnosis purpose. Pulse amplitude has no diagnostic relevance in this instance.
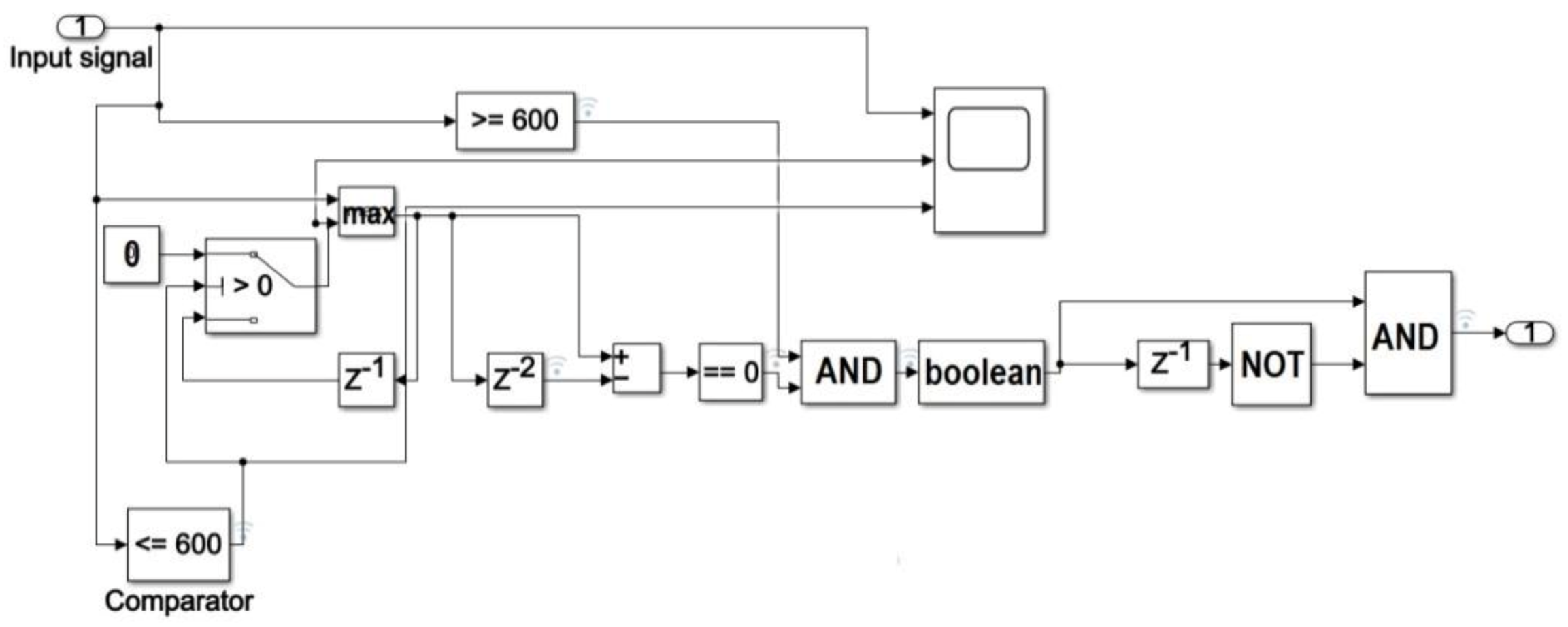
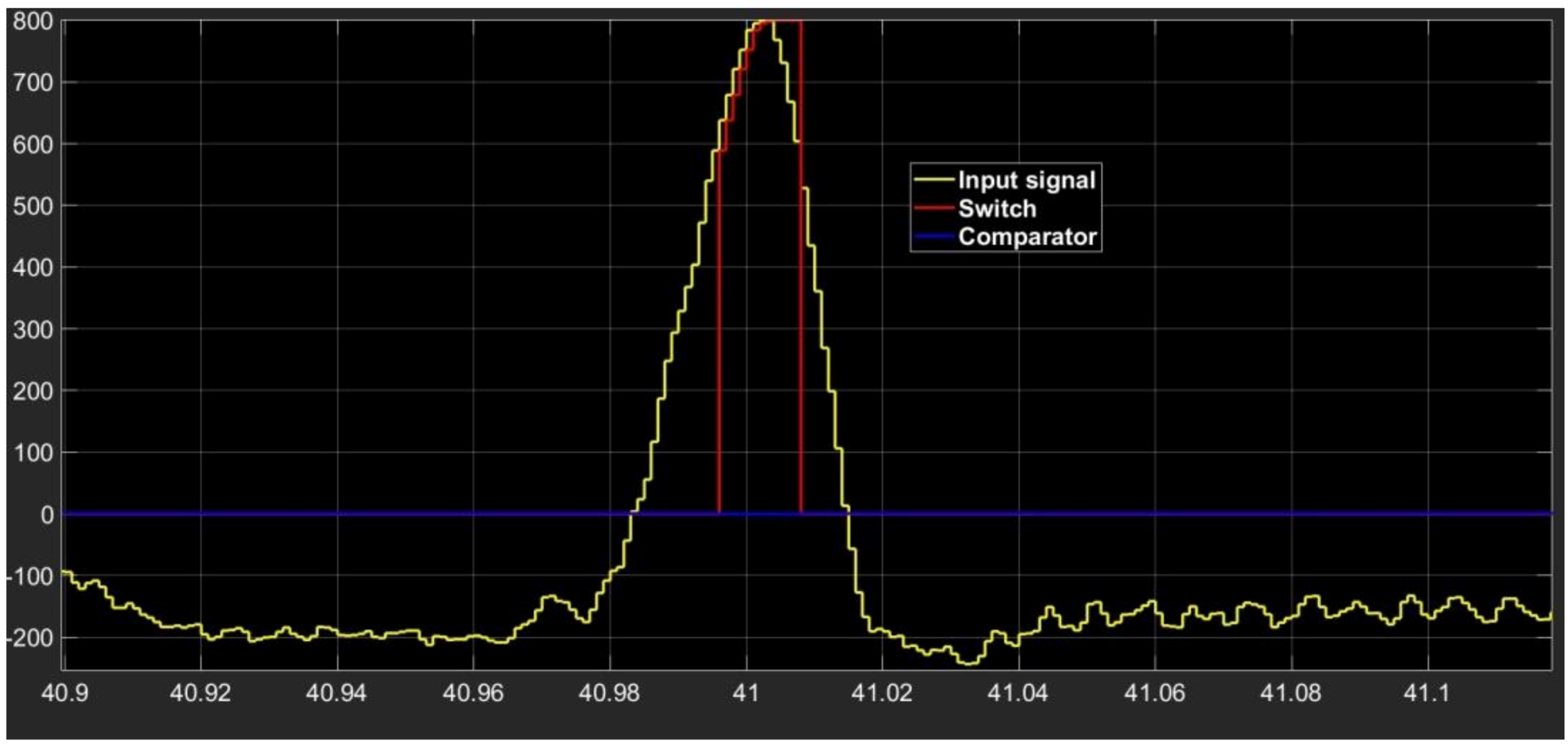
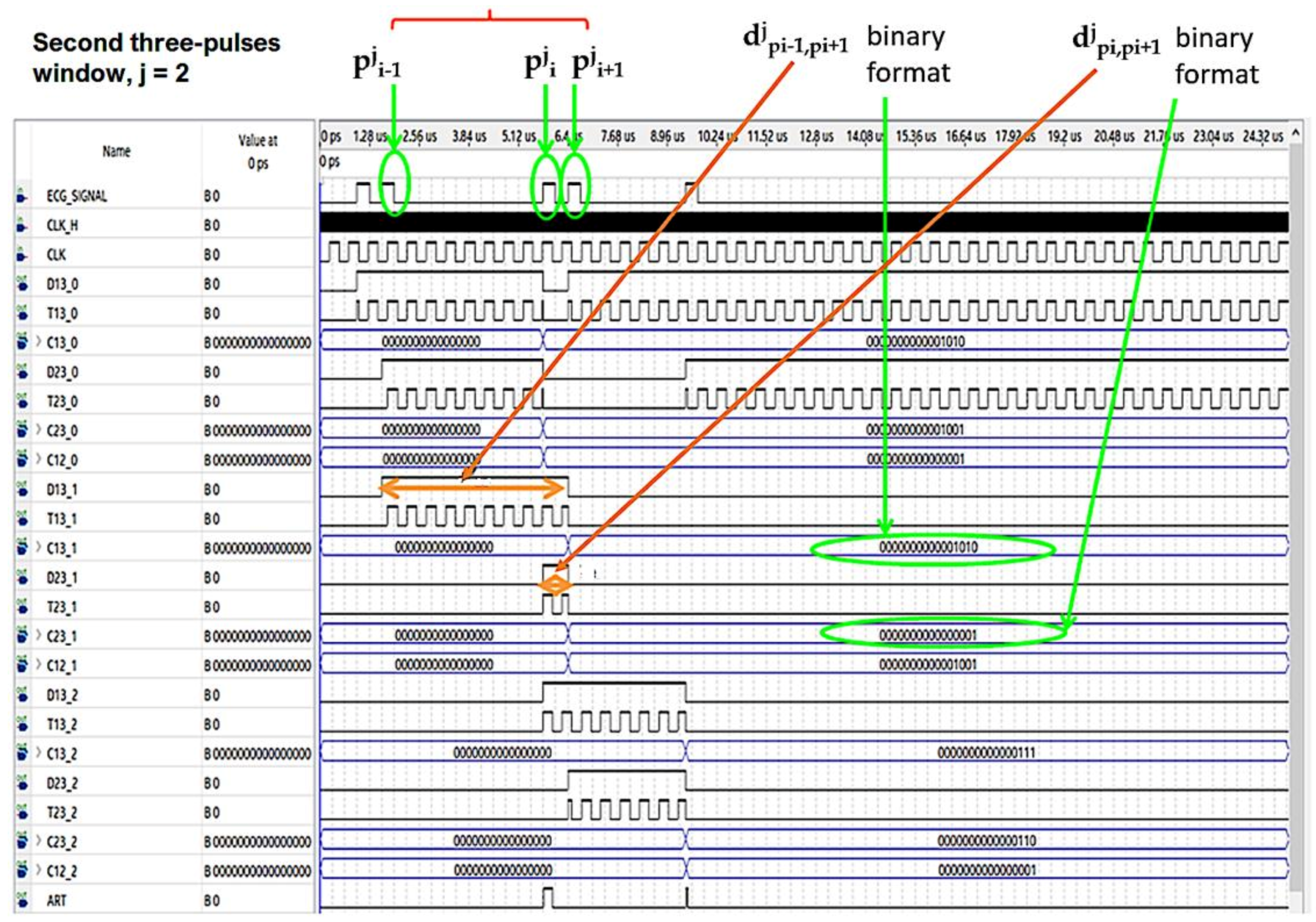
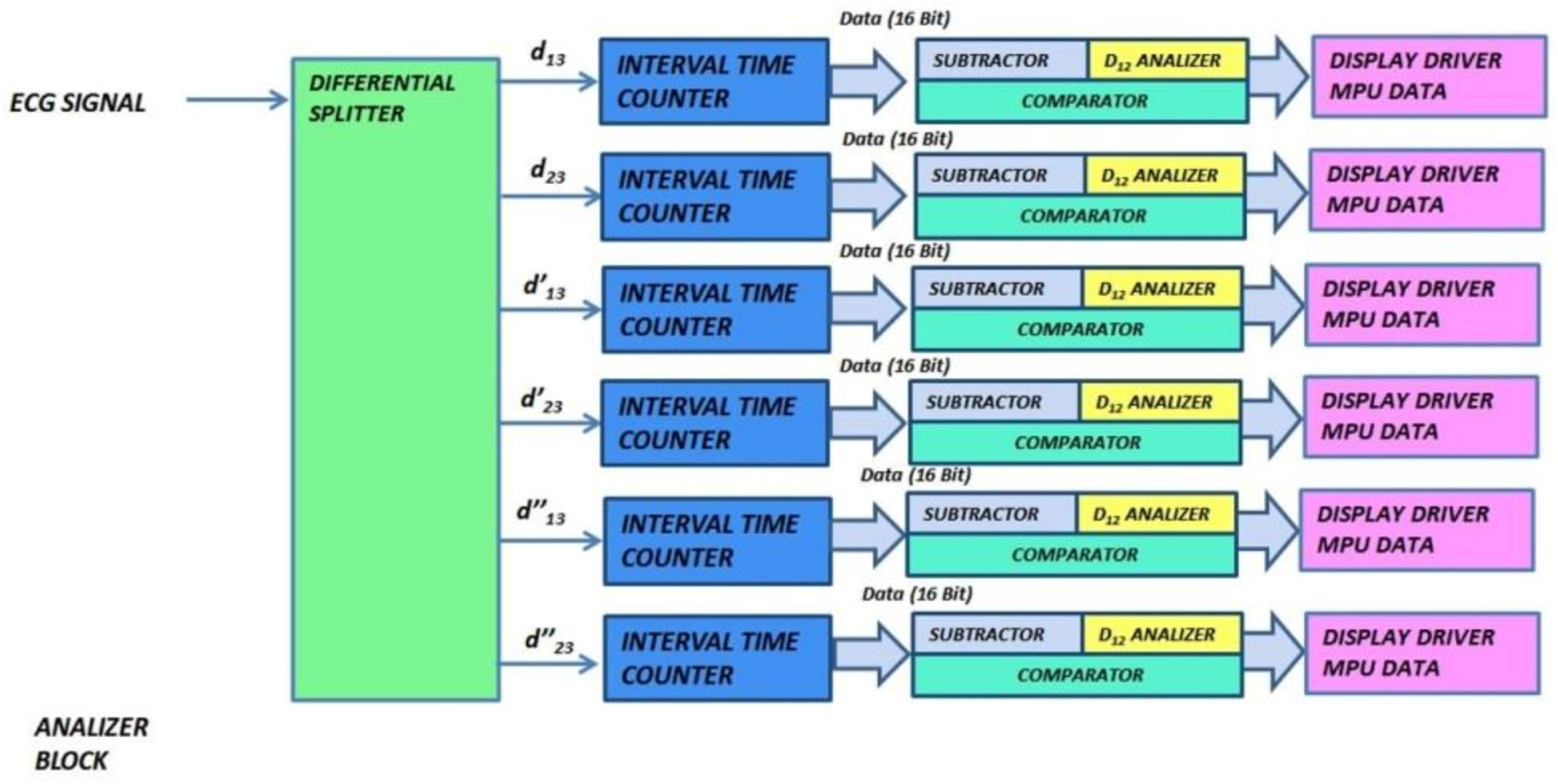
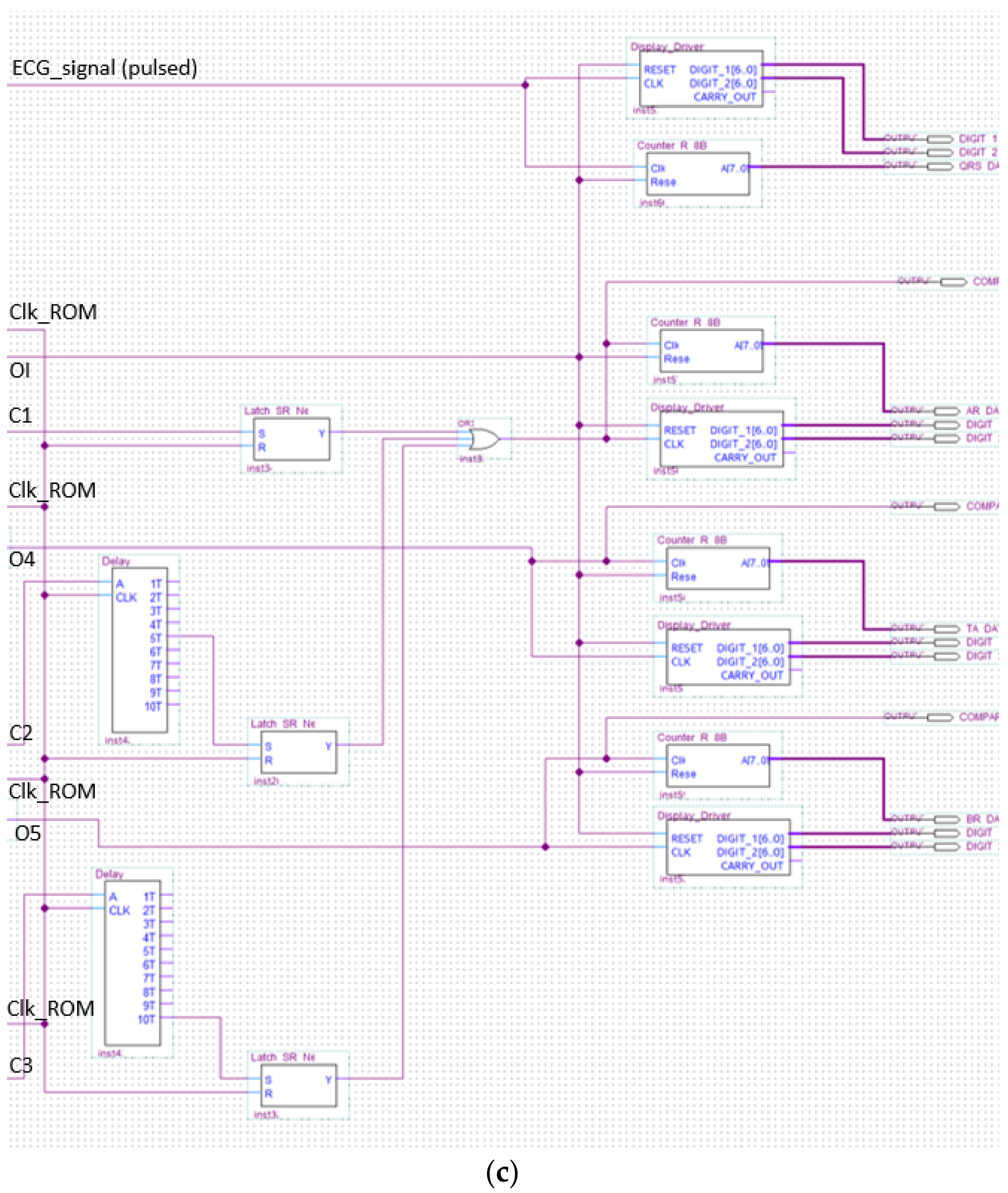
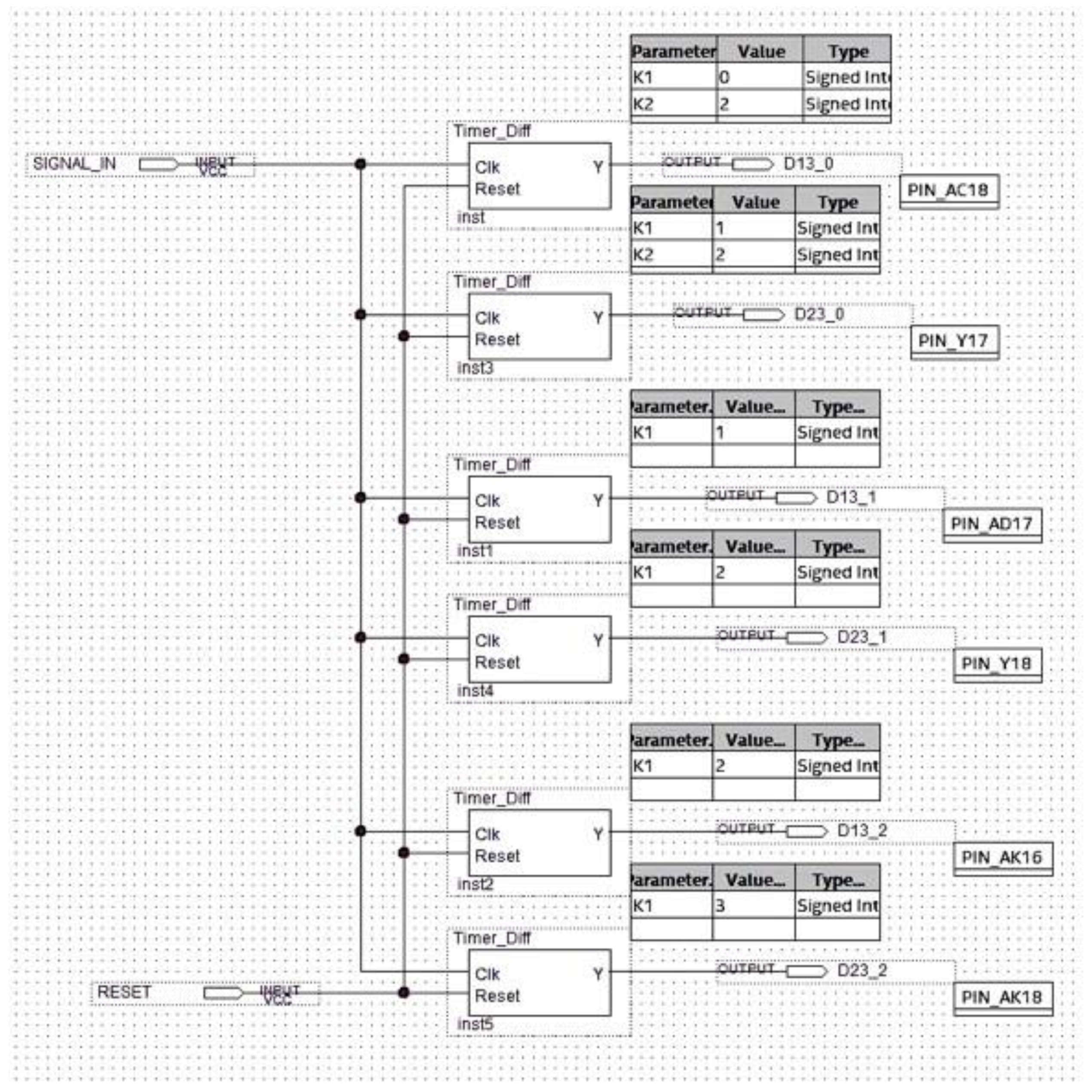
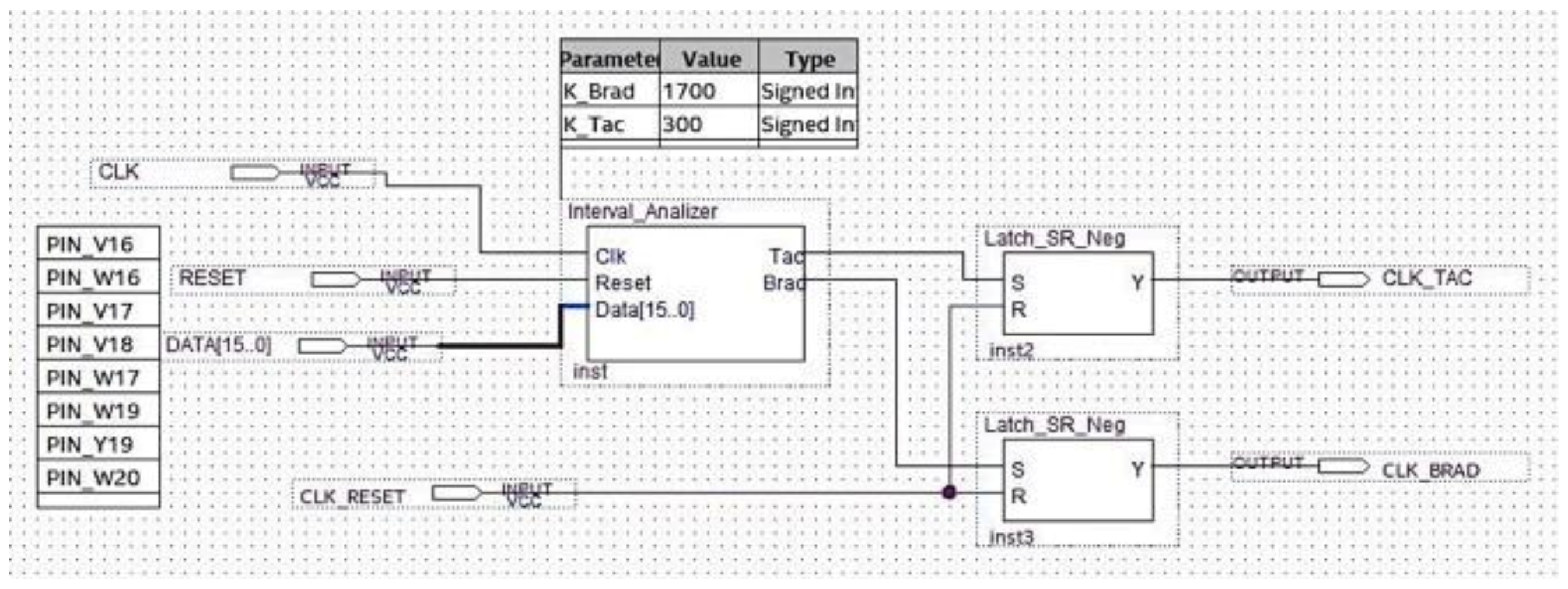
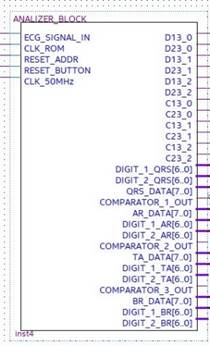
3.2. Analyzer Block Module
- ECG_SIGNAL_IN is the pulses-transformed ECG signal coming from the ROM Block in debug mode, otherwise coming from the preprocessing and R-peak detection block in real-time operating mode;
- CLK_ROM is the input to which the clock generated by the ROM memory block is applied for the system synchronization;
- Reset_Address is the reset signal provided by the ROM block;
- Reset_Button is the reset signal sent to the FPGA through a switch of the development board for functional check;
- CLK_50MHz is the reference signal clock generated by the development board.
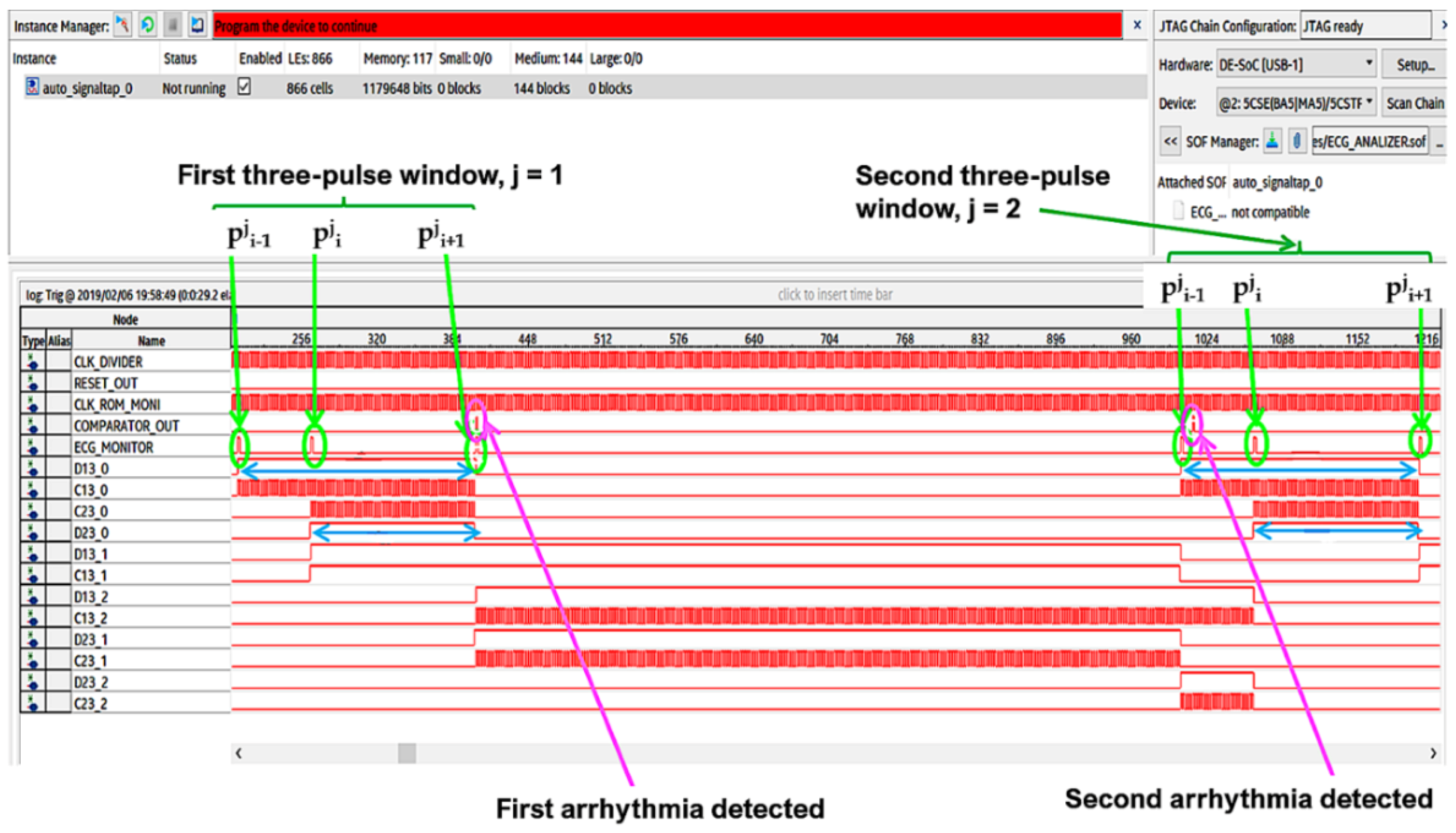
- D13_0, D13_1, and D13_2 are the signals generated by the differential splitter representing the distances djpi−1,pi+1, dj+1pi−1,pi+1, and dj+2pi−1,pi+1, respectively;
- D23_0, D23_1, and D23_2 are the signals generated by the differential splitter and representing the djpi,pi+1, dj+1pi,pi+1, and dj+2pi,pi+1, respectively;
- C13_0, C13_1, and C13_2 are the control signals for instrumental test of the system. They are generated by the Interval_Time_Counter and are expressed in 16-bit format. These signals represent the number of reference clock pulses counted in each window, which are D13_0, D13_1, and D13_2, respectively (that is the clock pulses counted by placing each of the signals D13_0, D13_1, and D13_2 in logic AND with the reference clock);
- C23_0, C23_1, and C23_2 are also control signals for the instrumental test of the system. They are generated by the Interval_Time_Counter and are expressed in 16-bit format. They represent the number of reference clock pulses counted in each window D23_0, D23_1, and D23_2, respectively (that is the clock pulses counted by placing each of the signals D23_0, D23_1, and D23_2 in logic AND with the reference clock);
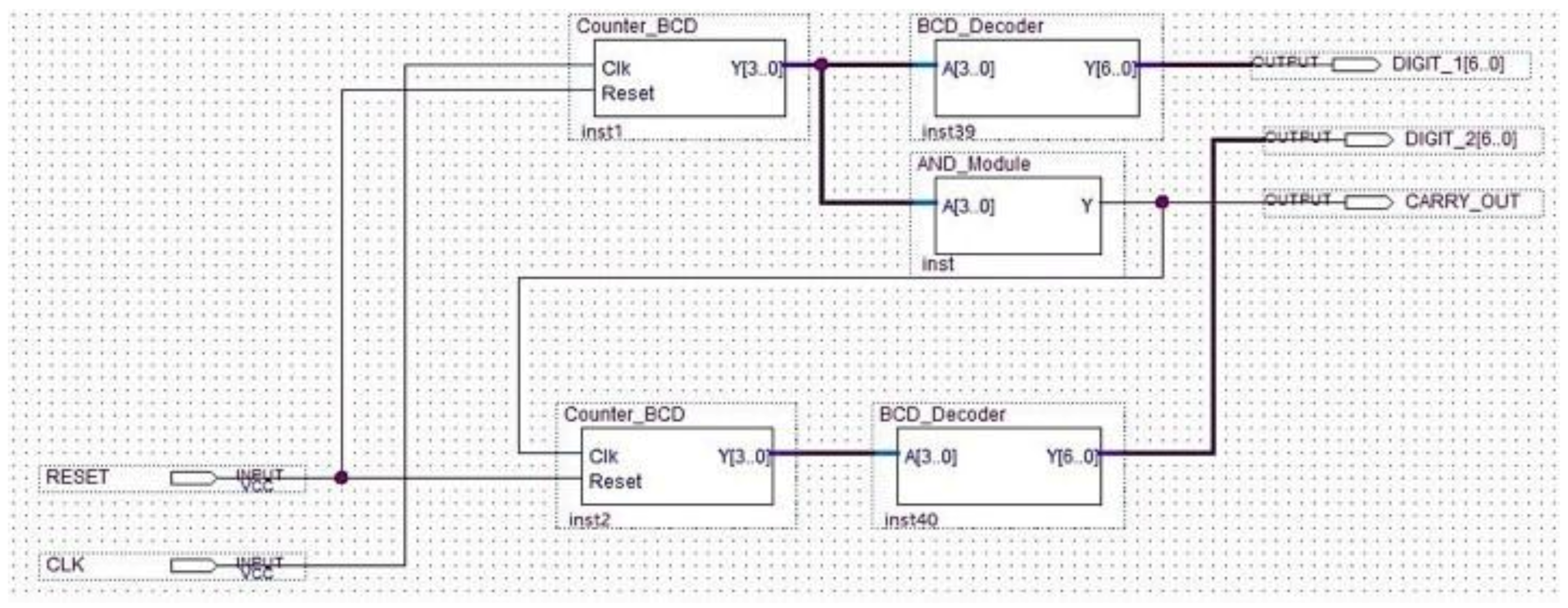
- DIGIT_1_QRS [6..0] and DIGIT_2_QRS [6..0], DIGIT_1_AR [6..0] and DIGIT_2_AR [6..0], DIGIT_1_TA [6..0] and DIGIT_2_TA [6..0], and DIGIT_1_BR [6..0] and DIGIT_2_BR [6..0] indicate the number of QRS, of arrhythmic, of tachycardic, and of bradycardic heartbeats detected, respectively. They are coded in binary-coded decimal (BCD) and visualized on the seven-segment display of the development board;
- QRS_DATA [7..0], AR_DATA [7..0], TA_DATA [7..0], and BR_DATA [7..0] are the 8-bit digital outputs that transmit the number of detected QRS, of arrhythmic, of tachycardic, and of bradycardic heartbeats to the data logger created with the FPGA-embedded processor;
- COMPARATOR OUT 1, 2, 3 are the output signals of the comparator inside the analyzer block, which are used as functional test outputs.
3.3. MCU Block
4. Implementation of the FPGA-Based Embedded System
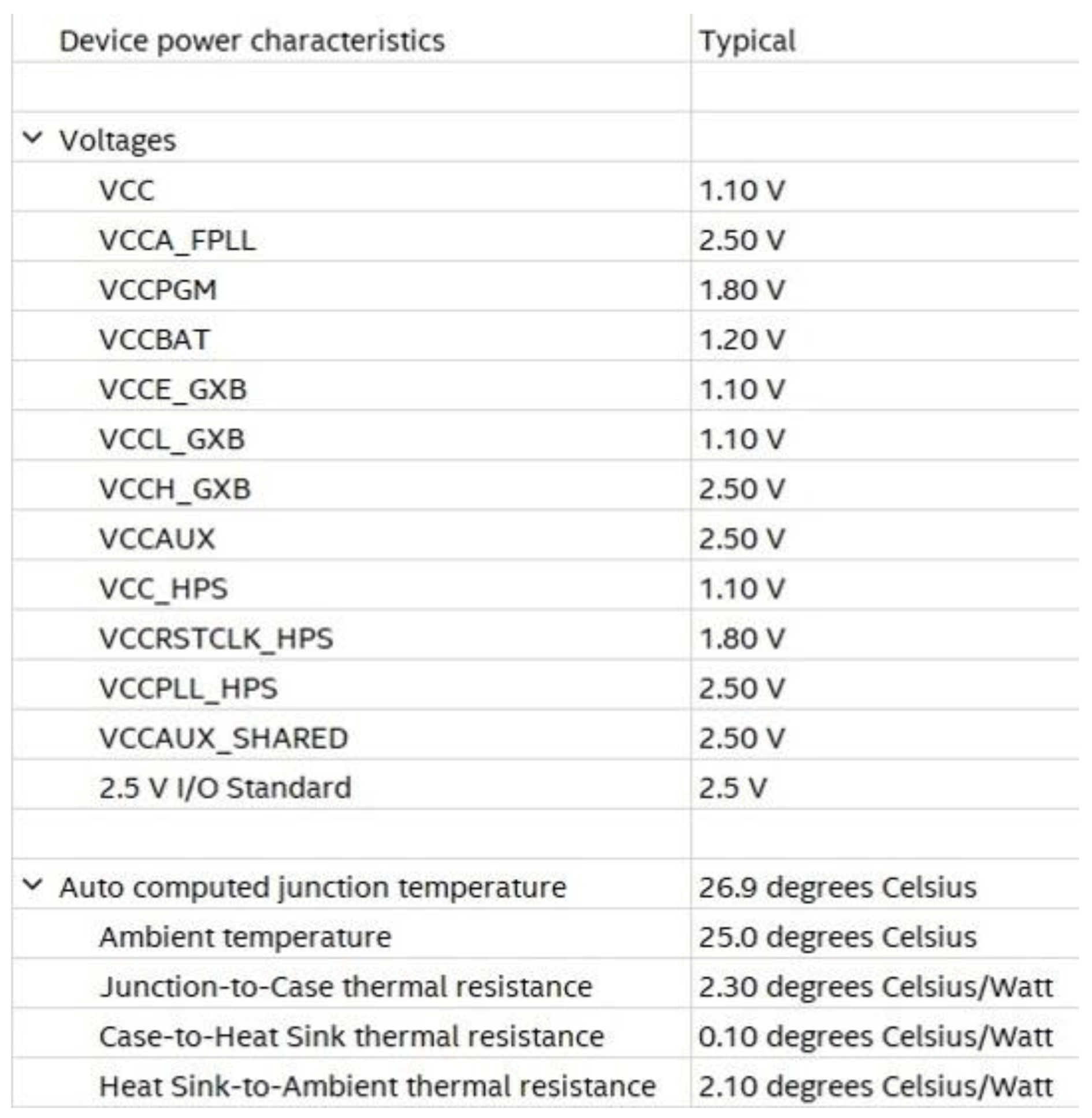
Efficiency of HW Design
- ➢
- Area occupancy and or amount of used hardware resources;
- ➢
- Operating speed;
- ➢
- Power consumption due to the system processing activity.
5. Results
5.1. Evaluation Parameters
5.2. Results of Matlab Simulations and FPGA Classifier Performance
6. Discussions
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gon, A.; Mukherjee, A. FPGA-Based Low-Cost Architecture for R-Peak Detection and Heart-Rate Calculation Using Lifting-Based Discrete Wavelet Transform. Circuits Syst. Signal Process 2023, 42, 580–600. [Google Scholar] [CrossRef]
- Rizzi, M.; D’Aloia, M. Computer aided system for breast cancer diagnosis. Biomed. Eng.-Appl. Basis Commun. 2014, 26, 1450033. [Google Scholar] [CrossRef]
- Karataş, F.; Koyuncu, İ.; Tuna, M.; Alçın, M.; Avcioglu, E.; Akgul, A. Design and implementation of arrhythmic ECG signals for biomedical engineering applications on FPGA. Eur. Phys. J. Spec. Top. 2022, 231, 869–884. [Google Scholar] [CrossRef]
- Guaragnella, C.; Rizzi, M.; Giorgio, A. Marginal Component Analysis of ECG Signals for Beat-to-Beat Detection of Ventricular Late Potentials. Electronics 2019, 8, 1000. [Google Scholar] [CrossRef] [Green Version]
- Lutfi, M.F. Ventricular late potential in cardiac syndrome X compared to coronary artery disease. BMC Cardiovasc. Disord. 2017, 17, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Al-Ani, M.S. ECG waveform classification based on P-QRS-t wave recognition, UHD. J. Sci. Technol. 2018, 2, 7–14. [Google Scholar] [CrossRef]
- Characteristics of the Normal Electrocardiogram. Available online: https://www.brainkart.com/article/Characteristics-of-the-Normal-Electrocardiogram_19237/ (accessed on 2 November 2022).
- Bsoul, A.A.R.; Ji, S.-Y.; Ward, K.; Najarian, K. Detection of P, QRS, and T Components of ECG using wavelet transformation. In Proceedings of the 2009 ICME International Conference on Complex Medical Engineering, Tempe, AZ, USA, 9–11 April 2009; pp. 1–6. [Google Scholar] [CrossRef]
- Rogers, B.; Schaffarczyk, M.; Clauß, M.; Mourot, L.; Gronwald, T. The Movesense Medical Sensor Chest Belt Device as Single Channel ECG for RR Interval Detection and HRV Analysis during Resting State and Incremental Exercise: A Cross-Sectional Validation Study. Sensors 2022, 22, 2032. [Google Scholar] [CrossRef]
- Esgalhado, F.; Batista, A.; Vassilenko, V.; Russo, S.; Ortigueira, M. Peak Detection and HRV Feature Evaluation on ECG and PPG Signals. Symmetry 2022, 14, 1139. [Google Scholar] [CrossRef]
- Liaqat, S.; Dashtipour, K.; Zahid, A.; Assaleh, K.; Arshad, K.; Ramzan, N. Detection of Atrial Fibrillation Using a Machine Learning Approach. Information 2020, 11, 549. [Google Scholar] [CrossRef]
- Mayapur, P. A Review on Detection and Performance Analysis on R-R Interval Methods for ECG. Int. J. Innov. Res. Sci. Eng. Technol. 2018, 7, 11019–11025. [Google Scholar] [CrossRef]
- Bin Obadi, A.; Soh, P.J.; Aldayel, O.; Al-Doori, M.H.; Mercuri, M.; Schreurs, D. A survey on vital signs detection using radar techniques and processing with FPGA implementation. IEEE Circuits Syst. Mag. 2021, 21, 41–74. [Google Scholar] [CrossRef]
- Tyagi, D.; Kumar, R. Rhythm Identification and Classification for Electrocardiogram Signals using Feature Cluster Framework Classifier. Int. J. Adv. Res. Eng. Technol. 2021, 12, 199–208. [Google Scholar] [CrossRef]
- Gowri Shankar, M.; Ganesh Babu, C. An Exploration of ECG Signal Feature Selection and Classification using Machine Learning Techniques. Int. J. Innov. Technol. Explor. Eng. 2020, 9, 797–804. [Google Scholar] [CrossRef]
- Arvanaghi, R.; Daneshvar, S.; Seyedarabi, H.; Goshvarpour, A. Fusion of ECG and ABP Signals Based on Wavelet Transform for Cardiac Arrhythmias Classification. Comput. Methods Programs Biomed. 2017, 151, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Mayapur, P. Classification of Arrhythmia from ECG Signals using MATLAB. Int. J. Eng. Manag. Res. 2018, 8, 115–129. [Google Scholar] [CrossRef]
- Gajowniczek, K.; Grzegorczyk, I.; Ząbkowski, T.; Bajaj, C. Weighted Random Forests to Improve Arrhythmia Classification. Electronics 2020, 9, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AAMI ECAR:1987. Recommended Practice for Testing and Reporting Performance Results of Ventricular Arrhythmia Detection Algorithms; Association for the Advancement of Medical Instrumentation: Arlington, VA, USA, 1987. [Google Scholar]
- ANSI/AAMI EC57:2012. Testing and reporting performance results of cardiac rhythm and ST segment measurement algorithms. Association for the Advancement of Medical Instrumentation: Arlington, VA, USA, 2012. [Google Scholar]
- Cardiac Arrhythmias. Available online: https://thoracickey.com/cardiac-arrhythmias-3/ (accessed on 2 November 2022).
- Saxena, S.; Vijay, R.; Saxena, G.; Pahadiya, P. Classification of Cardiac Signals with Automated R-Peak Detection Using Wavelet Transform Method. Wirel. Pers. Commun. 2022, 123, 655–669. [Google Scholar] [CrossRef]
- Maghfiroh, A.M.; Musvika, S.D.; Wakidi, L.F.; Amidi, L.; Sumber, S.; Mak’ruf, M.R.; Pudji, A.; Titisari, D. State-of-the-Art Method to Detect R-Peak on Electrocardiogram Signal: A Review. In Proceedings of the 1st International Conference on Electronics, Biomedical Engineering, and Health Informatics. Lecture Notes in Electrical Engineering; Triwiyanto, Nugroho, H.A., Rizal, A., Caesarendra, W., Eds.; Springer: Singapore, 2021; Volume 746. [Google Scholar] [CrossRef]
- Sabherwal, P.; Agrawal, M.; Singh, L. Automatic detection of the R peaks in single-lead ECG signal. Circuits Syst. Signal Process. 2017, 36, 4637–4652. [Google Scholar] [CrossRef]
- TerBekke, R.M.A.; Haugaa, K.H.; van den Wijngaard, A.; Bos, J.M.; Ackerman, M.J.; Edvardsen, T.; Volders, P.G.A. Electromechanical window negativity in genotyped long-QT syndrome patients: relation to arrhythmia risk. Eur. Heart J. 2015, 36, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Munshi, F.; Fontaine, J.M. Application of Electromechanical Window Negativity as an Arrhythmia Risk Correlate in Acquired Long QT Syndrome. JACC Case Rep. 2021, 15, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Rencuzogullari, I.; Çağdaş, M.; Karabağ, Y.; Karakoyun, S.; Çiftçi, H.; Gürsoy, M.O.; Karayol, S.; Çinar, T.; Tanik, O.; Hamideyin, S. A novel ECG parameter for diagnosis of acute pulmonary embolism: RS time RS time in acute pulmonary embolism. Am. J. Emerg. Med. 2019, 37, 1230–1236. [Google Scholar] [CrossRef]
- Gümüşdağ, A.; Burak, C.; Süleymanoğlu, M.; Yesin, M.; Tanık, V.O.; Karabağ, Y.; Çağdaş, M.; Rencüzoğulları, I. The predictive value of RS time for short term mortality in patients with acute pulmonary embolism. J. Electrocardiol. 2020, 62, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, A.; Guaragnella, C.; Rizzi, M. An Effective CAD System for Heart Sound Abnormality Detection. Circuits Syst. Signal Process. 2022, 41, 2845–2870. [Google Scholar] [CrossRef]
- Mirza, A.H.; Nurmaini, S.; Partan, R.U. Automatic Classification of 15 Leads ECG Signal of Myocardial Infarction Using One Dimension Convolutional Neural Network. Appl. Sci. 2022, 12, 5603. [Google Scholar] [CrossRef]
- Rizzi, M.; Guaragnella, C. Skin Lesion Segmentation Using Image Bit-Plane Multilayer Approach. Appl. Sci. 2020, 10, 3045. [Google Scholar] [CrossRef]
- Talukder, S.; Singh, R.; Bora, S.; Paily, R. An Efficient Architecture for QRS Detection in FPGA Using Integer Haar Wavelet Transform. Circuits Syst. Signal Process. 2020, 39, 3610–3625. [Google Scholar] [CrossRef]
- Liu, Y.; Dong, L.; Zhang, B.; Xin, Y.; Geng, L. Real Time ECG Classification System Based on DWT and SVM. In Proceedings of the 2020 IEEE International Conference on Integrated Circuits, Technologies and Applications, Nanjing, China, 23–25 November 2020; pp. 155–156. [Google Scholar] [CrossRef]
- Rizzi, M.; Guaragnella, C. A Decision Support System for Melanoma Diagnosis from Dermoscopic Images. Appl. Sci. 2022, 12, 7007. [Google Scholar] [CrossRef]
- Aqil, M.; Jbari, A.; Bourouhou, A. ECG Signal Denoising by Discrete Wavelet Transform. Int. J. Online Biomed. Eng. 2017, 13, 51–68. [Google Scholar] [CrossRef]
- Rizzi, M.; D’Aloia, M.; Castagnolo, B. A fully automatic system for detection of breast microcalcification clusters. J. Med. Biol. Eng. 2010, 30, 181–188. [Google Scholar]
- Ruha, A.; Sallinen, S.; Nissila, S. A real time microprocessor QRS detector system with a 1ms timing accuracy for the measurement of ambulatory HRV. IEEE Trans. Biomed. Eng. 1997, 44, 159–167. [Google Scholar] [CrossRef]
- Aritmie. Available online: http://www.medicinaurgenza.it/aritmie.html (accessed on 2 November 2022).
- Dahlberg, P.; Diamant, U.B.; Gilljam, T.; Rydberg, A.; Bergfeldt, L. QT correction using Bazett’s formula remains preferable in long QT syndrome type 1 and 2. Ann. Noninvasive Electrocardiol. 2021, 26, e12804. [Google Scholar] [CrossRef] [PubMed]
- Bousseljot, R.; Kreiseler, D.; Schnabel, A. Nutzung der EKG-Signaldatenbank CARDIODAT der PTB über das Internet. Biomed. Eng. 1995, 40, 317–318. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sološenko, A.; Petrėnas, A.; Paliakaitė, B.; Marozas, V.; Sörnmo, L. Model for Simulating ECG and PPG Signals with Arrhythmia Episodes (version 1.3.1). PhysioNet 2022. [Google Scholar] [CrossRef]
- DatabaseECG_Arrhythmia. Available online: https://drive.google.com/file/d/19DaROtBXEzpc2uZxSPaGQ2VkGPIq0YkU/view?usp=share_link(accessed on 2 November 2022).
- HDL Coder. Available online: https://www.mathworks.com/products/hdl-coder.html(accessed on 2 November 2022).
- FPGA designs with Verilog and SystemVerilog. Available online: https://www.academia.edu/42857396/FPGA_designs_with_Verilog_and_SystemVerilog?email_work_card=title (accessed on 2 November 2022).
- Video Intel® FPGA Rapidi. Available online: https://www.intel.it/content/www/it/it/programmable/support/training/demonstrations/online/embedded-processor.html?wapkw=nios%20II (accessed on 2 November 2022).
- FPGA ed FPGA SoC Intel®. Available online: https://www.intel.it/content/www/it/it/products/details/fpga.html(accessed on 2 November 2022).
- DE1-SoC Board. Available online: https://www.terasic.com.tw/cgi-bin/page/archive.pl?Language=English&CategoryNo=165&No=836#contents (accessed on 2 November 2022).
- Software Intel® Quartus® Prime. Available online: https://www.intel.it/content/www/it/it/software/programmable/quartus-prime/overview.html (accessed on 2 November 2022).
- Baratloo, A.; Hosseini, M.; Negida, A.; El Ashal, G. Part 1: Simple Definition and Calculation of Accuracy, Sensitivity and Specificity. Emergency 2015, 3, 48–49. [Google Scholar]
- Dinakarrao, S.M.P.; Jantsch, A.; Shafique, M. Computer-aided Arrhythmia Diagnosis with Bio-signal Processing: A Survey of Trends and Techniques. ACM Comput. Surv. 2020, 52, 1–37. [Google Scholar] [CrossRef]
- Rajani Kumaria, L.V.; Padma Saib, Y.; Balajic, N.; Viswada, K. FPGA Based Arrhythmia Detection. Procedia Comput. Sci. 2015, 57, 970–979. [Google Scholar] [CrossRef] [Green Version]
- Zairi, H.; Kedir Talha, M.; Meddah, K.; Ould Slimane, S. FPGA-based system for artificial neural network arrhythmia classification. Neural Comput. Appl. 2020, 32, 4105–4120. [Google Scholar] [CrossRef]
- Srivastava, R.; Kumar, B.; Alenezi, F.; Alhudhaif, A.; Althubiti, S.A.; Polat, K. Automatic Arrhythmia Detection Based on the Probabilistic Neural Network with FPGA Implementation. Math. Probl. Eng. 2022, 7564036. [Google Scholar] [CrossRef]
- Lim, H.W.; Hau, Y.W.; Othman, M.A.; Lim, C.W. Embedded system-on-chip design of atrial fibrillation classifier. In Proceedings of the 2017 International SoC Design Conference (ISOCC), Seoul, Republic of Korea, 5–8 November 2017; pp. 90–91. [Google Scholar] [CrossRef]
- Vinaykumar, S.; Thilagavathy, R. FPGA Implementation of Artificial Neural Network (ANN) for ECG Signal Classification. In Proceedings of the 2022 IEEE International IOT, Electronics and Mechatronics Conference (IEMTRONICS), Toronto, ON, Canada, 1–4 June 2022; pp. 1–6. [Google Scholar] [CrossRef]
- Desai, M.P.; Caffarena, G.; Jevtic, R.; Márquez, D.G.; Otero, A. A Low-Latency, Low-Power FPGA Implementation of ECG Signal Characterization Using Hermite Polynomials. Electronics 2021, 10, 2324. [Google Scholar] [CrossRef]
- Kripa, S.; Jebastine, J. Efficient FPGA-Based Design for Detecting Cardiac Dysrhythmias. In Intelligent Computing in Engineering. Advances in Intelligent Systems and Computing; Solanki, V., Hoang, M., Lu, Z., Pattnaik, P., Eds.; Springer: Singapore, 2020; Volume 1125. [Google Scholar] [CrossRef]
- Ghosh, R.; Tamil, L.S. Computation-efficient and compact FPGA design for a real-time wearable arrhythmia-detector. Biomed. Eng. Adv. 2021, 2, 100019. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Krichen, M. Anomalies Detection Through Smartphone Sensors: A Review. IEEE Sens. J. 2021, 21, 7207–7217. [Google Scholar] [CrossRef]
- Jabbar, R.; Fetais, N.; Krichen, M.; Barkaoui, K. Blockchain technology for healthcare: Enhancing shared electronic health record interoperability and integrity. Proceeding of the 2020 IEEE International Conference on Informatics, IoT, and Enabling Technologies (ICIoT), Doha, Qatar, 2–5 February 2020; pp. 310–317. [Google Scholar] [CrossRef]


























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nrms (mV) | Accuracy (%) |
|---|---|
| 0.02 | 99.20 |
| 0.04 | 99.20 |
| 0.06 | 99.20 |
| 0.08 | 99.20 |
| 0.1 | 98.80 |
| 0.4 | 97.60 |
| HW Used | Power Supply | Power Dissipation | Area Occupancy | Accuracy (%) | |
|---|---|---|---|---|---|
| Ref. [52] | Xilinx Spartan XC3S500 | NA | NA | 38% | 94.76 |
| Ref. [53] | Artix-7 | NA | NA | NA | 98.3 |
| Ref. [54] | Artix-7 | NA | NA | NA | 98.27 |
| Ref. [55] | Altera DE2-115 | NA | NA | NA | 95.3 |
| Ref. [56] | Artix-7 | NA | NA | NA | 86 |
| Ref. [57] | Artix-7 | 5 V | 28 mW | NA | NA |
| Ref. [58] | Xilinx Spartan 3 | NA | 280 mW | NA | 93.6 |
| Ref. [59] | Xilinx Spartan 6 | NA | 0.48 mW | 32% | 99.65 |
| Our system | Intel Cyclone V | 1.1 V | 5.70 mW | 6% | 99.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giorgio, A.; Guaragnella, C.; Rizzi, M. FPGA-Based Decision Support System for ECG Analysis. J. Low Power Electron. Appl. 2023, 13, 6. https://doi.org/10.3390/jlpea13010006
Giorgio A, Guaragnella C, Rizzi M. FPGA-Based Decision Support System for ECG Analysis. Journal of Low Power Electronics and Applications. 2023; 13(1):6. https://doi.org/10.3390/jlpea13010006
Chicago/Turabian StyleGiorgio, Agostino, Cataldo Guaragnella, and Maria Rizzi. 2023. "FPGA-Based Decision Support System for ECG Analysis" Journal of Low Power Electronics and Applications 13, no. 1: 6. https://doi.org/10.3390/jlpea13010006