
Structural Abnormalities in Brugada Syndrome and Non-Invasive Cardiac Imaging: A Systematic Review
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract

1. Introduction
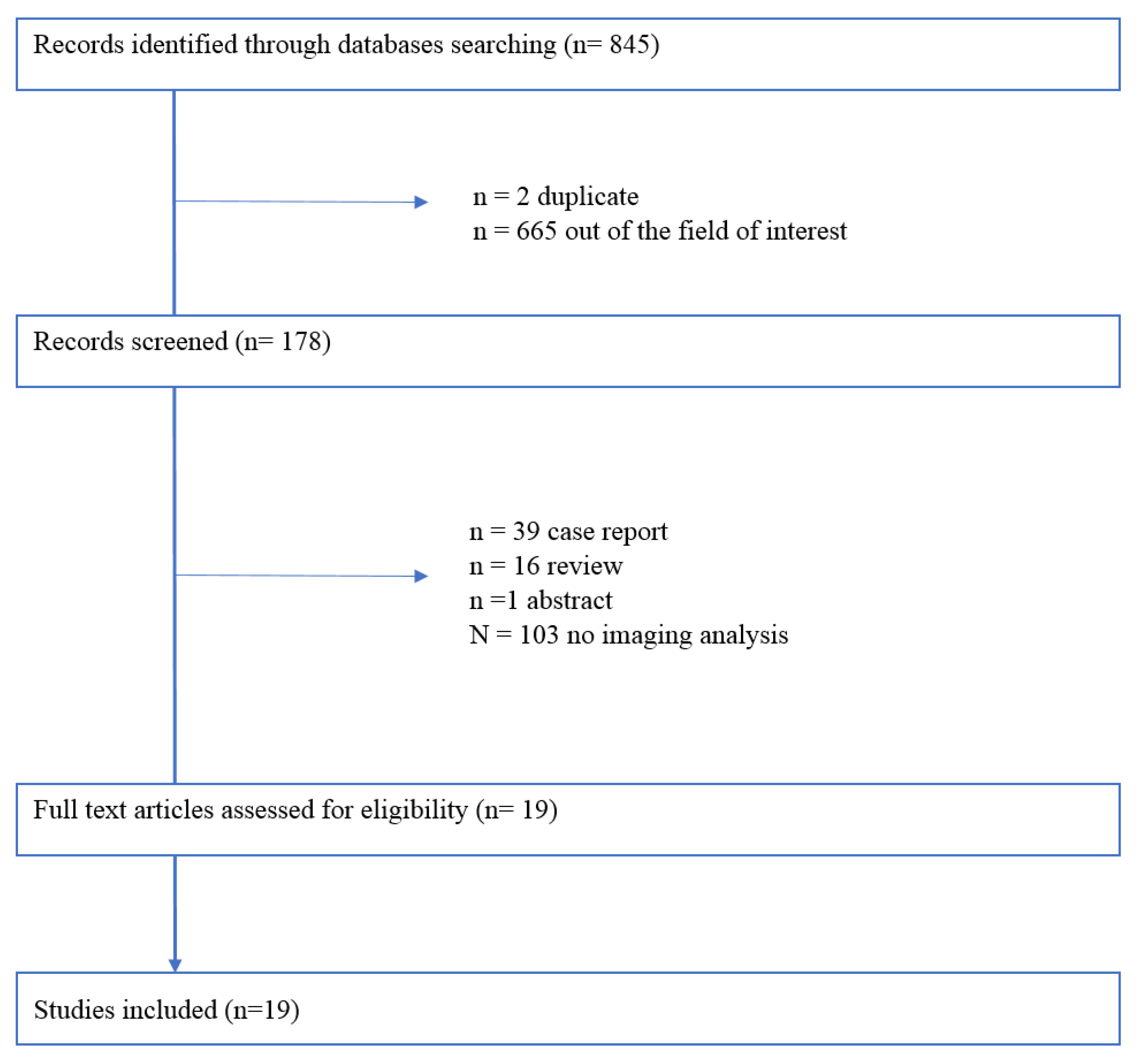
2. Methodological Considerations
3. Cardiac Imaging in BrS Patients
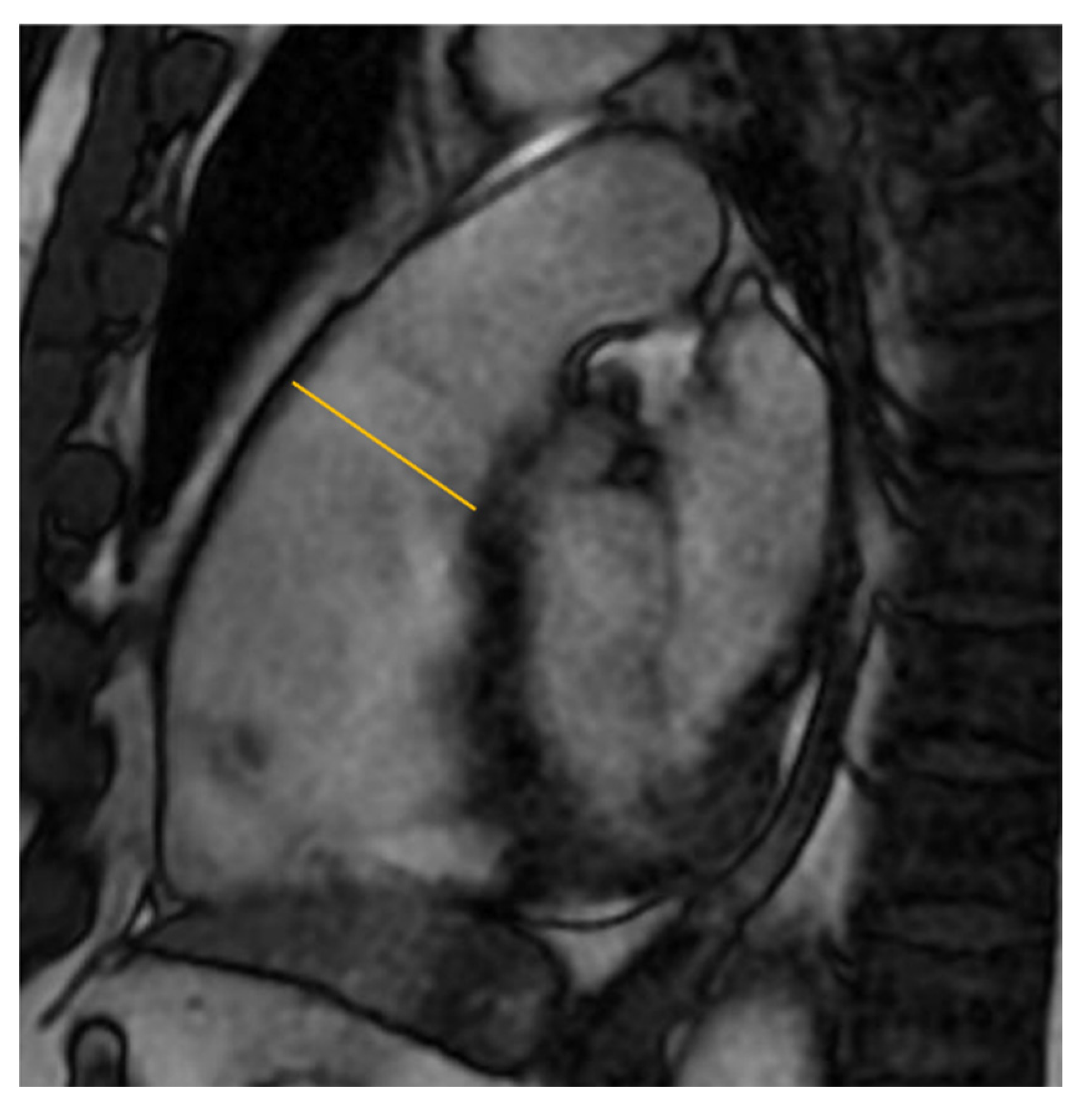
3.1. Right Ventricular Dilatation
3.2. Ejection Fraction
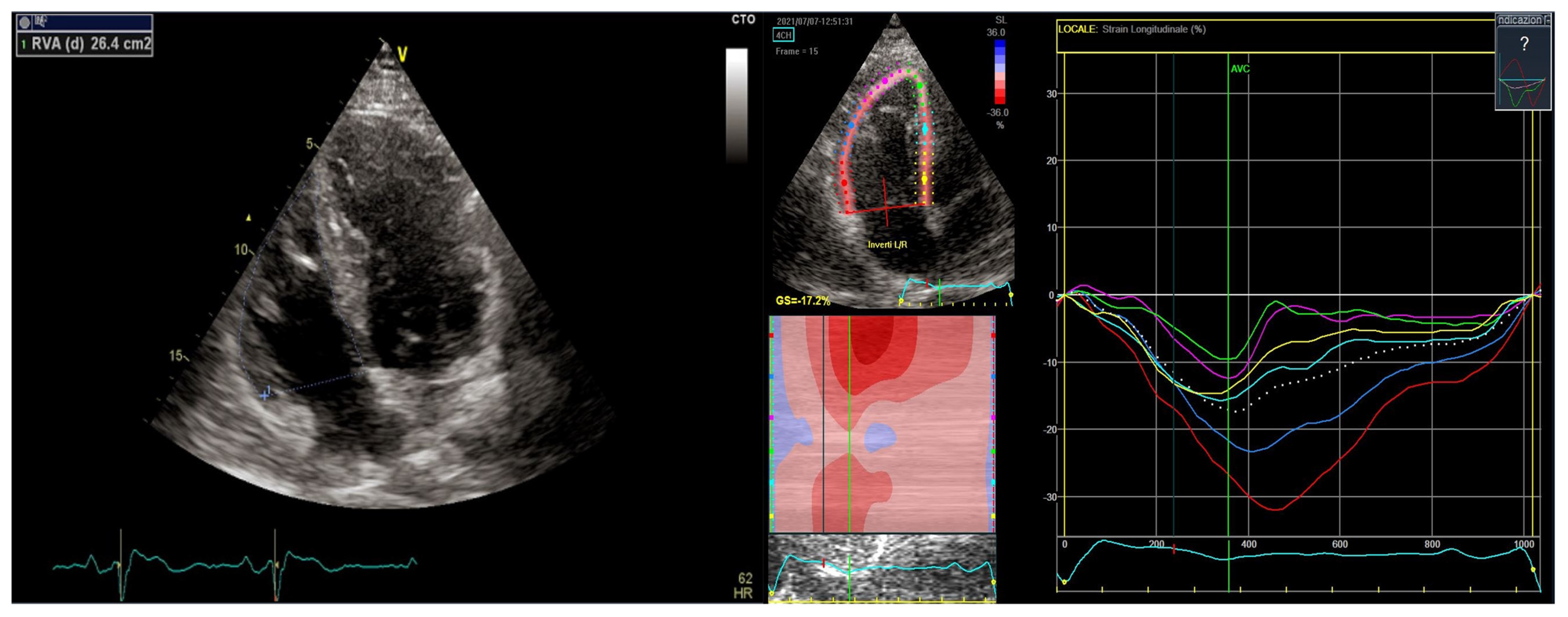
3.3. Speckle and Feature Tracking
3.4. Contraction Delay
3.5. Tissue Carachterization
3.6. Atrial Involvement
4. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brugada, J.; Campuzano, O.; Arbelo, E.; Sarquella-Brugada, G.; Brugada, R. Present Status of Brugada Syndrome: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 1046–1059. [Google Scholar] [CrossRef]
- Watanabe, H.; Minamino, T. Genetics of Brugada syndrome. J. Hum. Genet. 2016, 61, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Kapplinger, J.D.; Tester, D.J.; Alders, M.; Benito, B.; Berthet, M.; Brugada, J.; Brugada, P.; Fressart, V.; Guerchicoff, A.; Harris-Kerr, C.; et al. An international compendium of mutations in the SCN5A-encoded cardiac sodium channel in patients referred for Brugada syndrome genetic testing. Heart Rhythm 2010, 7, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Blomström-Lundqvist, C. 2015 European Society of Cardiology Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death summarized by co-chairs. Eur. Heart J. 2015, 36, 2757–2759. [Google Scholar] [CrossRef]
- Vitali, F.; Brieda, A.; Balla, C.; Pavasini, R.; Tonet, E.; Serenelli, M.; Ferrari, R.; Delise, P.; Rapezzi, C.; Bertini, M. Standard ECG in Brugada Syndrome as a Marker of Prognosis: From Risk Stratification to Pathophysiological Insights. J. Am. Heart Assoc. 2021, 10, e020767. [Google Scholar] [CrossRef]
- Milman, A.; Andorin, A.; Gourraud, J.B.; Postema, P.G.; Sacher, F.; Mabo, P.; Km, S.H.; Juang, J.J.M.; Maeda, S.; Takahashi, Y.; et al. Profile of patients with Brugada syndrome presenting with their first documented arrhythmic event: Data from the Survey on Arrhythmic Events in BRUgada Syndrome (SABRUS). Heart Rhythm 2018, 15, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Casado-Arroyo, R.; Berne, P.; Rao, J.Y.; Rodriguez-Manero, M.; Levinstein, M.; Conte, G.; Sera, J.; Namdar, M.; Ricciardi, D.; Chierchia, G.B.; et al. Long-Term Trends in Newly Diagnosed Brugada Syndrome: Implications for Risk Stratification. J. Am. Coll. Cardiol. 2016, 68, 614–623. [Google Scholar] [CrossRef] [PubMed]
- Papavassiliu, T.; Veltmann, C.; Doesch, C.; Haghi, D.; Germans, R.; Schoenberg, S.O.; van Rossum, A.C.; Schmpf, R.; Brade, J.; Wolpert, C.; et al. Spontaneous type 1 electrocardiographic pattern is associated with cardiovascular magnetic resonance imaging changes in Brugada syndrome. Heart Rhythm 2010, 7, 1790–1796. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleeijnen, J.; Moher, D.; et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiiatkowskii, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Bucciarelli-Ducci, C.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized cardiovascular magnetic resonance imaging (CMR) protocols: 2020 update. J. Cardiovasc. Magn. Reson. 2020, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Van Malderen, S.C.H.; Daneels, D.; Kerkhove, D.; Peeters, U.; Theuns, D.A.M.J.; Droogmans, S.; Van Camp, G.; Weytjens, C.; Biervliet, M.; Bonduelle, M.; et al. Prolonged Right Ventricular Ejection Delay in Brugada Syndrome Depends on the Type of SCN5A Variant—Electromechanical Coupling through Tissue Velocity Imaging as a Bridge between Genotyping and Phenotyping. Circ. J. 2017, 82, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Trevisan, F.; Bertini, M.; Balla, C.; Pestelli, G.; Luisi, A.; Smarrazzo, V.; Farnè, M.; Ferlini, A.; Gualandi, F.; Mele, D. Type 1 Brugada Pattern Is Associated with Echocardiography-Detected Delayed Right Ventricular Outflow Tract Contraction. J. Am. Coll. Cardiol. 2021, 77, 2865–2867. [Google Scholar] [CrossRef] [PubMed]
- Scheirlynck, E.; Van Malderen, S.; Motoc, A.; Lie, O.H.; de Asmunds, C.; Sieira, J.; Chierchia, G.B.; Brugada, P.; Cosyns, B.; Droogmans, S. Contraction alterations in Brugada syndrome; association with life-threatening ventricular arrhythmias. Int. J. Cardiol. 2020, 299, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Iacoviello, M.; Forleo, C.; Puzzovivo, A.; Nalin, I.; Guida, P.; Anacleiro, M.; Marangelli, V.; Sorrentino, S.; Monitillo, F.; Ciccone, M.M.; et al. Altered two-dimensional strain measures of the right ventricle in patients with Brugada syndrome and arrhythmogenic right ventricular dysplasia/cardiomyopathy. Eur. J. Echocardiogr. 2011, 12, 773–781. [Google Scholar] [CrossRef]
- Catalano, O.; Antonaci, S.; Moro, G.; Mussida, M.; Frascaroli, M.; Baldi, M.; Cobelli, F.; Baiardi, P.; Nastol, J.; Bloise, R.; et al. Magnetic resonance investigations in Brugada syndrome reveal unexpectedly high rate of structural abnormalities. Eur. Heart J. 2009, 30, 2241–2248. [Google Scholar] [CrossRef] [PubMed]
- Van Hoorn, F.; Campian, M.E.; Spijkerboer, A.; Blom, M.T.; Planken, N.; van Rossum, A.C.; de Bakker, J.M.T.; Wilde, A.A.M.; Groenink, M.; Tan, H.L. SCN5A mutations in Brugada syndrome are associated with increased cardiac dimensions and reduced contractility. PLoS ONE 2012, 7, e42037. [Google Scholar] [CrossRef] [PubMed]
- Rudic, B.; Schimpf, R.; Veltmann, C.; Doesch, C.; Tulumen, E.; Schoenberg, S.O.; Borggrefe, M.; Papaassiliu, T. Brugada syndrome: Clinical presentation and genotype-correlation with magnetic resonance imaging parameters. Europace 2016, 18, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Papavassiliu, T.; Wolpert, C.; Flüchter, S.; Schimpf, R.; Neff, W.; Haase, K.K.; Duber, C.; Borggrefe, M. Magnetic resonance imaging findings in patients with Brugada syndrome. J. Cardiovasc. Electrophysiol. 2004, 15, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Hohneck, A.; Overhoff, D.; Rutsch, M.; Rudic, B.; Tulumen, E.; Wolpert, C.; Hetjens, S.; Akin, I.; Borggrefe, M.; Papavassiliu, T. Risk stratification of patients with Brugada syndrome: The impact of myocardial strain analysis using cardiac magnetic resonance feature tracking. Hell. J. Cardiol. 2021, 62, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Gray, B.; Gnanappa, G.K.; Bagnall, R.D.; Femia, G.; Yeates, L.; Ingles, J.; Burns, C.; Puranik, R.; Grieve, S.M.; Semsaran, C.; et al. Relations between right ventricular morphology and clinical, electrical and genetic parameters in Brugada Syndrome. PLoS ONE 2018, 13, e0195594. [Google Scholar] [CrossRef] [PubMed]
- Bastiaenen, R.; Cox, A.T.; Castelletti, S.; Wijeyeratne, Y.D.; Colbeck, N.; Pakroo, N.; Ahmed, H.; Bunce, N.; Anderson, L.; Moon, J.C.; et al. Late gadolinium enhancement in Brugada syndrome: A marker for subtle underlying cardiomyopathy? Heart Rhythm 2017, 14, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Tessa, C.; Del Meglio, J.; Ghidini Ottonelli, A.; Diciotti, S.; Salvatori, L.; Magnacca, M.; Chioccioli, M.; Lera, J.; Vignali, C.; Casolo, G.; et al. Evaluation of Brugada syndrome by cardiac magnetic resonance. Int. J. Cardiovasc. Imaging 2012, 28, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Giusca, S.; Dambrauskaite, V.; Scheurwegs, C.; D’hooge, J.; Claus, P.; Herbots, L.; Magro, M.; Rademakers, F.; Meyns, B.; Delcroix, M.; et al. Deformation imaging describes right ventricular function better than longitudinal displacement of the tricuspid ring. Heart 2010, 96, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Muraru, D.; Parati, G.; Haugaa, K.; Voigt, J.U. How to do right ventricular strain. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 825–827. [Google Scholar] [CrossRef] [PubMed]
- Orwat, S.; Kempny, A.; Diller, G.P.; Bauerschmitz, P.; Bunck, A.C.; Maintz, D.; Radke, R.M.; Baumgartner, H. Cardiac magnetic resonance feature tracking: A novel method to assess myocardial strain. Comparison with echocardiographic speckle tracking in healthy volunteers and in patients with left ventricular hypertrophy. Kardiol. Pol. 2014, 72, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Kempny, A.; Fernández-Jiménez, R.; Orwat, S.; Schuler, P.; Bunck, A.C.; Maintz, D.; Baumgartner, H.; Diller, G.P. Quantification of biventricular myocardial function using cardiac magnetic resonance feature tracking, endocardial border delineation and echocardiographic speckle tracking in patients with repaired tetralogy of Fallot and healthy controls. J. Cardiovasc. Magn. Reson. 2012, 14, 32. [Google Scholar] [CrossRef]
- Prati, G.; Vitrella, G.; Allocca, G.; Muser, D.; Buttignoni, S.C.; Piccoli, G.; Morocutti, G.; Delise, P.; Pinamonti, B.; Proclemer, A.; et al. Right Ventricular Strain and Dyssynchrony Assessment in Arrhythmogenic Right Ventricular Cardiomyopathy: Cardiac Magnetic Resonance Feature-Tracking Study. Circ. Cardiovasc. Imaging 2015, 8, e003647. [Google Scholar] [CrossRef]
- Eitel, I.; Stiermaier, T.; Lange, T.; Rommel, K.P.; Koschalka, A.; Kowallick, J.T.; Lotz, J.; Kutty, S.; Gutberlet, M.; Hasenfus, G.; et al. Cardiac Magnetic Resonance Myocardial Feature Tracking for Optimized Prediction of Cardiovascular Events Following Myocardial Infarction. JACC Cardiovasc. Imaging 2018, 11, 1433–1444. [Google Scholar] [CrossRef]
- Romano, S.; Judd, R.M.; Kim, R.J.; Kim, H.W.; Klem, I.; Heitner, J.F.; Shah, D.J.; Jue, J.; White, B.E.; Indorkar, R.; et al. Feature-Tracking Global Longitudinal Strain Predicts Death in a Multicenter Population of Patients with Ischemic and Nonischemic Dilated Cardiomyopathy Incremental to Ejection Fraction and Late Gadolinium Enhancement. JACC Cardiovasc. Imaging 2018, 11, 1419–1429. [Google Scholar] [CrossRef]
- Buss, S.J.; Breuninger, K.; Lehrke, S.; Voss, A.; Galuschky, C.; Lossnitzer, D.; Andre, F.; Ehlermann, P.; Franke, J.; Taeger, T.; et al. Assessment of myocardial deformation with cardiac magnetic resonance strain imaging improves risk stratification in patients with dilated cardiomyopathy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 307–315. [Google Scholar] [CrossRef]
- Heermann, P.; Fritsch, H.; Koopmann, M.; Sporns, P.; Paul, M.; Heindel, W.; Schulze-Bahr, E.; Schulke, C. Biventricular myocardial strain analysis using cardiac magnetic resonance feature tracking (CMR-FT) in patients with distinct types of right ventricular diseases comparing arrhythmogenic right ventricular cardiomyopathy (ARVC), right ventricular outflow-tract tachycardia (RVOT-VT), and Brugada syndrome (BrS). Clin. Res. Cardiol. 2019, 108, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Mitroi, C.; García-Izquierdo, E.; García-Lunar, I.; Castro-Urda, V.; Toquero-Ramos, J.; Monivas-Palomero, V.; Mingo-Santos, S.; Cavero, M.A.; Brugada, J.; Fernandez-Lozano, I.; et al. Right ventricular function and dyssynchrony in Brugada syndrome: Highlighting the importance of the mechanical substrate in the right ventricular outflow tract. Int. J. Cardiol. 2021, 333, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Van Malderen, S.C.H.; Kerkhove, D.; Theuns, D.A.M.J.; Weytjens, C.; Droogmans, S.; Tanaka, K.; Daneels, D.; Van Dooren, S.; Meuwissen, M.; Bonduelle, M.; et al. Prolonged right ventricular ejection delay identifies high risk patients and greater differences in Brugada syndrome. Int. J. Cardiol. 2015, 191, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Toh, N.; Morita, H.; Nagase, S.; Miura, D.; Nishii, N.; Nakamura, K.; Ohe, T.; Kusano, K.F.; Ito, H. Atrial electrophysiological and structural remodeling in high-rick patients with Brugada syndrome: Assessment with electrophysiology and echocardiography. Heart Rhythm 2010, 7, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Isbister, J.C.; Gray, B.; Offen, S.; Yeates, L.; Naoum, C.; Medi, C.; Raju, H.; Semsarian, C.; Puranik, R.; Sy, R.W. Longitudinal assessment of structural phenotype in Brugada syndrome using cardiac magnetic resonance imaging. Heart Rhythm O2 2022, 18, 34–41. [Google Scholar] [CrossRef]
- Ciconte, G.; Monasky, M.M.; Santinelli, V.; Micaglio, E.; Vicedomini, G.; Anastasia, L.; Negro, G.; Borrelli, V.; Giannelli, L.; Santini, F.; et al. Brugada syndrome genetics is associated with phenotype severity. Eur. Heart J. 2021, 42, 1082–1090. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Echocardiography | Cardiac MRI | |
|---|---|---|
| RV dilatation | + | + |
| RVEF abnormality | + | + |
| RV strain value | + | + |
| Delayed RV contraction | + | -- |
| RV fatty infiltration | -- | + |
| RV LGE | -- | + |
| LVEF abnormality | + | + |
| Atrial enlargement | + | + |
| Incidence | Prognostic Implication | |
|---|---|---|
| RV dilatation | +++ | |
| RVEF abnormality | +++ | |
| RV strain value | +++ | + |
| Delayed RV contraction | +++ | + |
| RV fatty infiltration | + | |
| RV LGE | + | |
| LVEF abnormality | + | |
| Atrial enlargement | ++ |
| Authors | Population | CMR Findings |
|---|---|---|
| Catalano O et al. [16] | 30 BrS vs. 30 Hc | ↑ RV inflow tract diameter (p < 0.001) |
| ↑ RV inflow tract area (p = 0.050) | ||
| ↑ RVES volume (p = 0.031) | ||
| van Hoorn F et al. [17] | 138 BrS vs. 18 Hc | ↑RVOT diameter (p < 0.001) |
| ↑ RVES volume (p < 0.001) | ||
| Rudic B et al. [18] | 81 BrS vs. 30 Hc | ↑RVOT diameter (p < 0.01) |
| ↑ RVES volume (p < 0.01) | ||
| Papavassiliu T et al. [19] | 20 BrS vs. 20 Hc | ↑ RV outflow area (p = 0.018) |
| ↑ RVES volume (p = 0.3) | ||
| ↑ RVED volume (p = 0.08) | ||
| Hohneck A et al. [20] | 106 BrS vs. 25 Hc | ↑ RVES volume (p = 0.01) |
| ↑ RVOT area (p < 0.0001) | ||
| Gray B et al. [21] | 48 BrS vs. 48 Hc | ↑ RVOT volume (p < 0.0001) |
| Bastiaenen R et al. [22] | 78 BrS vs. 78 Hc | ↑ RVES volume (p = 0.038) |
| Authors | Population | RV CMR Findings | LV CMR Findings |
|---|---|---|---|
| Papavassiliu T et al. [19] | 20 BrS vs. 20 Hc | trend ↓ RVEF (p = 0.06) | x |
| Catalano O et al. [16] | 30 BrS vs. 30 Hc | RV motion abnormalities (p = 0.006) | x |
| ↓ motion of RVOT (p = 0.032) | |||
| Papavassiliu T et al. [8] | 69 BrS (26 sBrS + 43 diBrS) vs. 30 Hc | ↓ RVEF in sBrS (p < 0.05) | ↓ LVEF in sBrS (p < 0.05) |
| Rudic B et al. [18] | 81 BrS vs. 30 Hc | ↓ RVEF (p < 0.01) | trend ↓ LVEF (p = 0.07) |
| Gray B et al. [21] | 29 BrS vs. 29 Hc | ↓ RVEF (p = 0.002) | x |
| ↓ motion of RVOT (p < 0.0001) | |||
| Hohneck A et al. [20] | 106 BrS (34 sBrS + 72 diBrS) vs. 25 Hc | ↓ RVEF in sBrS vs. Hc (p < 0.0001) | x |
| van Hoorn F et al. [17] | 138 BrS (40 SCN5A+ and 98 SCN5a−) vs. 18 Hc | x | ↓ LVEF in SCN5A + (p < 0.001) |
| Tessa C. et al. [23] | 29 BrS vs. 29 Hc | x | x |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Raffele, M.; Di Domenico, A.; Balla, C.; Vitali, F.; Boccadoro, A.; Pavasini, R.; Micillo, M.; Cocco, M.; Campo, G.; Bertini, M.; et al. Structural Abnormalities in Brugada Syndrome and Non-Invasive Cardiac Imaging: A Systematic Review. Biology 2023, 12, 606. https://doi.org/10.3390/biology12040606
De Raffele M, Di Domenico A, Balla C, Vitali F, Boccadoro A, Pavasini R, Micillo M, Cocco M, Campo G, Bertini M, et al. Structural Abnormalities in Brugada Syndrome and Non-Invasive Cardiac Imaging: A Systematic Review. Biology. 2023; 12(4):606. https://doi.org/10.3390/biology12040606
Chicago/Turabian StyleDe Raffele, Martina, Assunta Di Domenico, Cristina Balla, Francesco Vitali, Alberto Boccadoro, Rita Pavasini, Marco Micillo, Marta Cocco, Gianluca Campo, Matteo Bertini, and et al. 2023. "Structural Abnormalities in Brugada Syndrome and Non-Invasive Cardiac Imaging: A Systematic Review" Biology 12, no. 4: 606. https://doi.org/10.3390/biology12040606