
Prevalence of Ponticulus Posticus and Migraine in 220 Orthodontic Patients: A Cross-Sectional Study
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
- ○
- with aura;
- ○
- without aura (formerly called classic and common migraine).
2. Materials and Methods
2.1. Study DesignSS
2.2. Setting (Setting, Locations and Relevant Dates, including Periods of Recruitment, Exposure, Follow-Up and Data Collection)
2.3. Participants
2.4. Exclusion Criteria
- ○
- Age under 18;
- ○
- Non-Italian nationality;
- ○
- Low-quality images (e.g., due to patient movement);
- ○
- Incomplete region of interest (ROI);
- ○
- Head congenital anomalies or syndromic pathologies;
- ○
- Anamnesis positive for trauma or surgery of the neck;
- ○
- Anamnesis positive for traumatic injury or concussion of the brain;
- ○
- Anamnesis positive for more than 1 type of primary headache;
- ○
- Anamnesis positive for comorbidity with other medical conditions (e.g., epilepsy, diabetes mellitus, underlying hypertension, cerebrovascular diseases or other neurodegenerative disorders);
- ○
- Anamnesis positive for psychiatric conditions (anxiety disorders, schizophrenia bipolar disorders or major depressive disorders) [13];
- ○
- Inability to provide a detailed history.
2.5. Diagnosis of Migraine
2.6. CBCT Scans
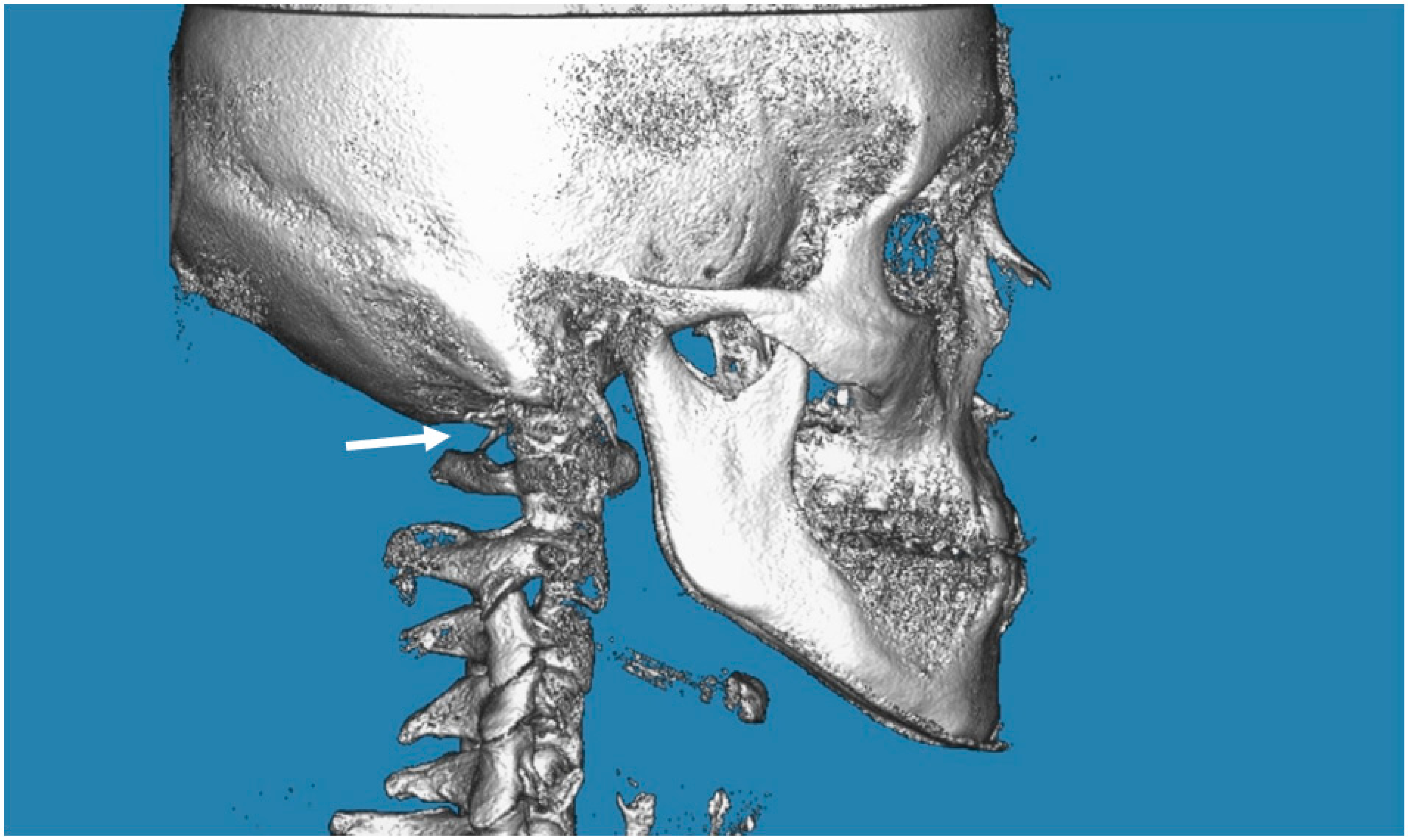
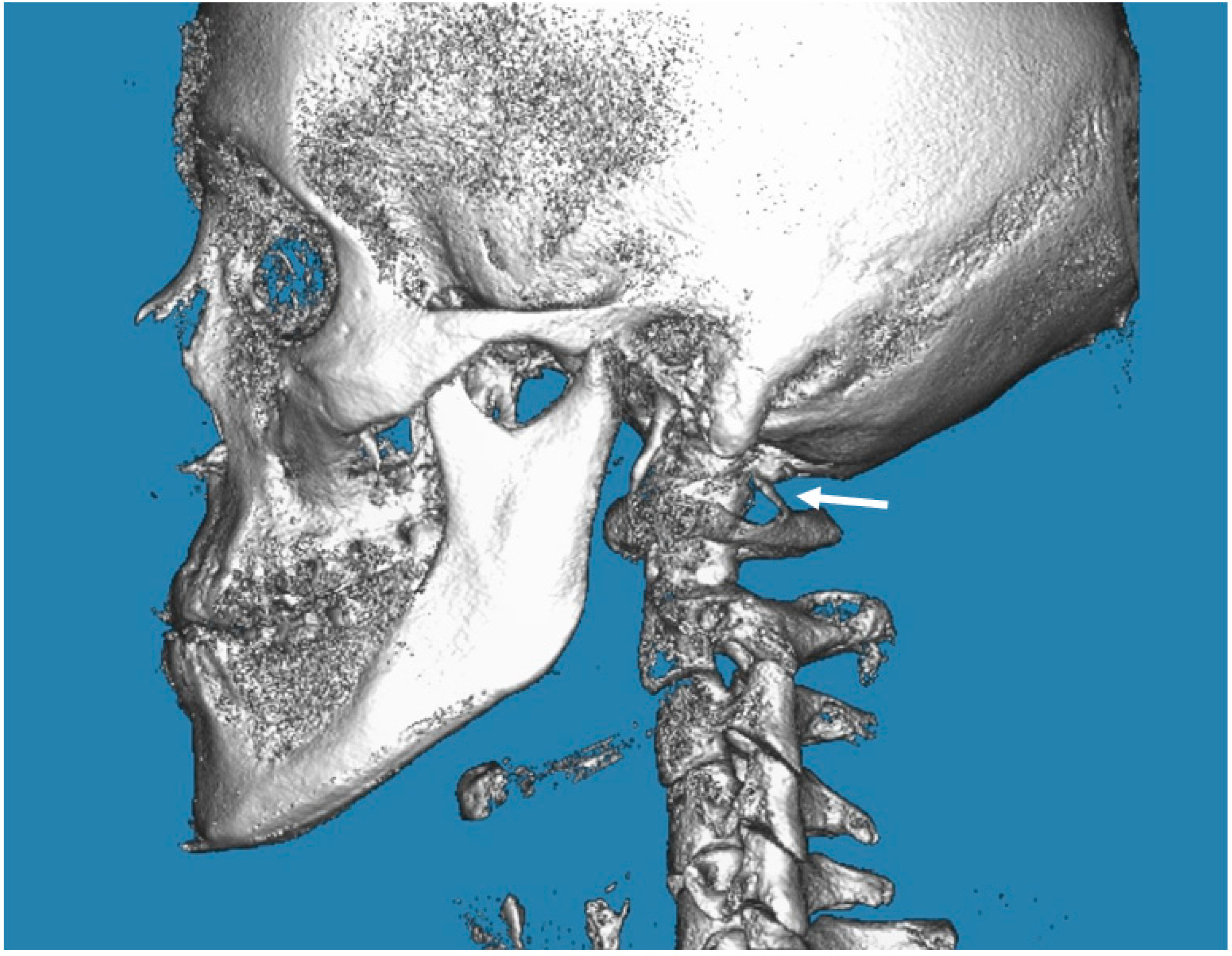
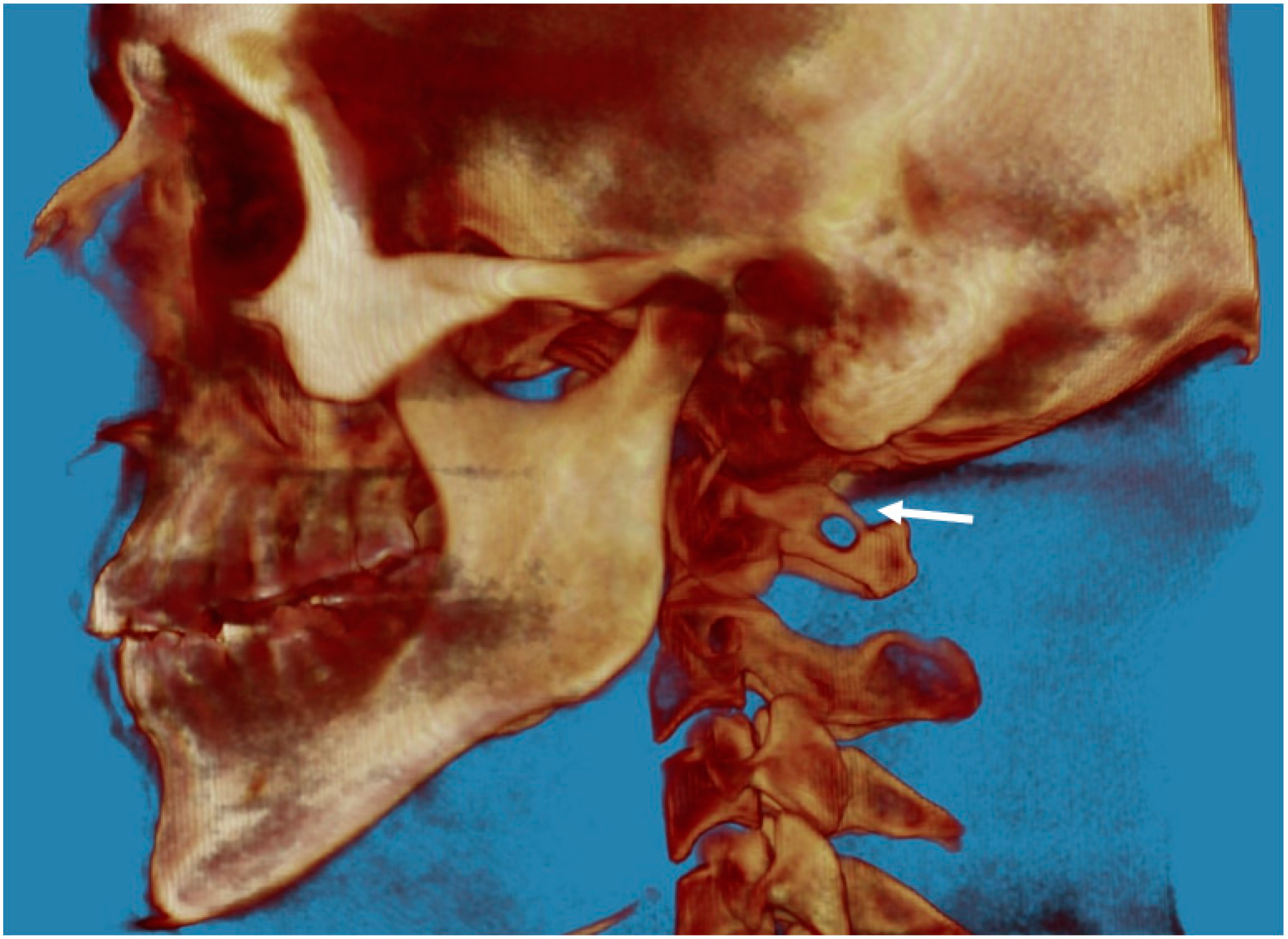
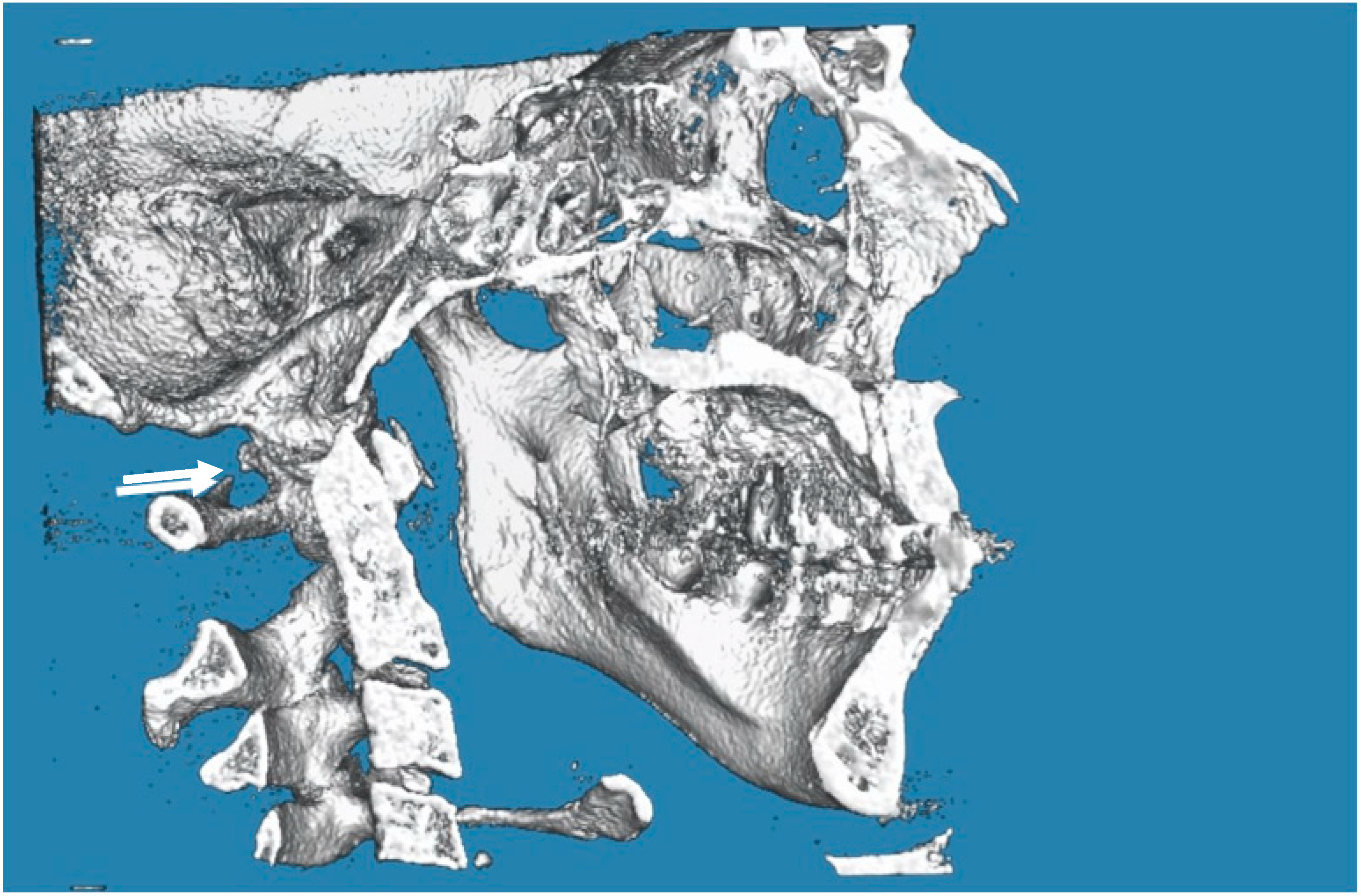
2.7. Evaluation of PP
2.8. Error Method
2.9. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tassoker, M.; Kok, H.; Ozcan, S. Investigation of the relationship between “Sella Turcica Bridge” and “Ponticulus Posticus”: A lateral cephalometric study. Int. J. Morphol. 2017, 35, 337–344. [Google Scholar] [CrossRef]
- Allen, W. The varieties of the atlas in the human subject, and the homologies of its transverse processes. J. Anat. Physiol. 1879, 14, 18–27. [Google Scholar]
- Simsek, S.; Yigitkanli, K.; Comert, A.; Acar, H.I.; Seckin, H.; Er, U.; Belen, D.; Tekdemir, I.; Elhan, A. Posterior osseous bridging of C1. J. Clin. Neurosci. 2008, 15, 686–688. [Google Scholar] [CrossRef]
- Schilling, J.; Schilling, A.; Galdames, I.S. Ponticulus posticus on the posterior arch of atlas, prevalence analysis in asymptomatic patients. Int. J. Morphol. 2010, 28, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Ratnaparkhi, M.M.; Pokharkar, P.M.; Mhapuskar, A.; Hiremutt, D.R.; Jain, R.; Telrandhe, N.V. Co-relation between presence of ponticulus posticus on the lateral cephalogram with cervical pain and vertigo. Eur. J. Mol. Clin. Med. 2021, 7, 4047–4053. [Google Scholar]
- Cohnen, M.; Kemper, J.; Mobes, O.; Pawelzik, J.; Modder, U. Radiation dose in dental radiology. Eur. Radiol. 2002, 12, 634–637. [Google Scholar] [CrossRef] [PubMed]
- Geist, J.R.; Geist, S.M.; Lin, L.M. A cone beam CT investigation of ponticulus posticus and lateralis in children and adolescents. Dentomaxillofac. Radiol. 2014, 43, 2013045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buyuk, S.K.; Sekerci, A.E.; Benkli, Y.A.; Ekizer, A. A survey of ponticulus posticus: Radiological analysis of atlas in an orthodontic population based on cone-beam computed tomography. Niger. J. Clin. Pract. 2017, 20, 106–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayrakdar, I.S.; Miloglu, O.; Altun, O.; Gumussoy, I.; Durna, D.; Yilmaz, A.B. Cone beam computed tomography imaging of ponticulus posticus: Prevalence, characteristics, and a review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, e210–e219. [Google Scholar] [CrossRef] [Green Version]
- Silberstein, S.D. Migraine pathophysiology and its clinical implications. Cephalalgia 2004, 24 (Suppl. 2), 2–7. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013, 33, 629–808. [Google Scholar] [CrossRef] [Green Version]
- Festa, F.; Rotelli, C.; Scarano, A.; Navarra, R.; Caulo, M.; Macrì, M. Functional magnetic resonance connectivity in patients with temporomadibular joint disorders. Front. Neurol. 2021, 12, 629211. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-W.; Lai, P.-Y.; Chen, Y.-L.; Wang, Y.-F.; Lirng, J.-F.; Chen, S.-T.; Lai, K.-L.; Chen, W.-T.; Wu, Y.-T.; Wang, S.-J. The Use of Neuroimaging for Predicting Sumatriptan Treatment Response in Patients With Migraine. Front. Neurol. 2022, 13, 798695. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.J.; Fuh, J.L.; Young, Y.H.; Lu, S.R.; Shia, B.C. Prevalence of migraine in Taipei, Taiwan: A population-based survey. Cephalalgia 2000, 20, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Feragalli, B.; Rampado, O.; Abate, C.; Festa, F.; Stromei, F.; Caputi, S.; Guglielmi, G.; Macrì, M. Cone beam computed tomography for dental and maxillofacial imaging: Technique improvement and low-dose protocols. Radiol. Med. 2017, 122, 581–588. [Google Scholar] [CrossRef]
- Macrì, M.; Medori, S.; Varvara, G.; Festa, F. A Digital 3D Retrospective Study Evaluating the Efficacy of Root Control during Orthodontic Treatment with Clear Aligners. Appl. Sci. 2023, 13, 1540. [Google Scholar] [CrossRef]
- Macrì, M.; Festa, F. Three-dimensional evaluation using CBCT of the mandibular asymmetry and the compensation mechanism in a growing patient: A case report. Front. Public Health 2022, 10, 921413. [Google Scholar] [CrossRef]
- Natsis, K.; Piperaki, E.T.; Fratzoglou, M.; Lazaridis, N.; Tsitsopoulos, P.P.; Samolis, A.; Kostares, M.; Piagkou, M. Atlas posterior arch and vertebral artery’s groove variants: A classification, morphometric study, clinical and surgical implications. Surg. Radiol. Anat. 2019, 41, 985–1001. [Google Scholar] [CrossRef]
- Levy, D. Migraine pain, meningeal inflammation, and mast cells. Curr. Pain Headache Rep. 2009, 13, 237–240. [Google Scholar] [CrossRef]
- Hawkins, J.L.; Cornelison, L.E.; Blankenship, B.A.; Durham, P.L. Vagus nerve stimulation inhibits trigeminal nociception in a rodent model of episodic migraine. Pain Rep. 2017, 2, e628. [Google Scholar] [CrossRef]
- Padmalatha, K.; Prathap Kumar, J.; Prakash, B.S.; Udupa, K. An osteological study of arcuate foramen in atlas and its clinical significance. Int. J. Anat. Res. 2018, 6, 5835–5839. [Google Scholar] [CrossRef]
- Lambarty, B.G.H.; Zivanovic, S. The retroarticular vertebral artery ring of the atlas and its significance. Acta Anat. 1973, 85, 113–122. [Google Scholar] [CrossRef]
- Wight, S.; Osborne, N.; Breen, A.C. Incidence of ponticulus posterior of the atlas in migraine and cervicogenic headache. J. Manip. Physiol. Ther. 1999, 22, 15–20. [Google Scholar] [CrossRef]
- Sabir, H.; Kumbhare, S.; Rout, P. Evaluation of ponticulus posticus on digital lateral cephalograms and cone beam computed tomography in patients with migraine and healthy individuals: A comparative study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, N.; Ashtari, F.; Razavi, M.; Ghaffari, R. Prevalence and characteristics of ponticulus posticus and its association with cervicogenic headache and migraine: A lateral cephalometric study. J. Res. Med. Sci. 2022, 27, 61. [Google Scholar] [CrossRef] [PubMed]
- Cakmak, O.; Gurdal, E.; Ekinci, G.; Yildiz, E.; Cavdar, S. Arcuate foramen and its clinical significance. Saudi Med. J. 2005, 26, 1409–1413. [Google Scholar]
- Kim, K.H.; Park, K.W.; Manh, T.H.; Yeom, J.S.; Chang, B.S.; Lee, C.K. Prevalence and Morphologic Features of Ponticulus Posticus in Koreans: Analysis of 312 Radiographs and 225 Three-dimensional CT Scans. Asian Spine J. 2007, 1, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Macrì, M.; Perrella, G.; Varvara, G.; Murmura, G.; Traini, T.; Rendina, F.; Festa, F. Assessments of Prevalence of Ponticulus Posticus, Atlas Posterior Arch Deficiency, Sella Turcica Bridging, Maxillary Canine Impaction, and Associations Among Them in 500 CBCTs of Italian Orthodontic Patients. Front. Dent. Med. 2021, 2, 708169. [Google Scholar] [CrossRef]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine: Epidemiology, Burden, and Comorbidity. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Loder, S.; Sheikh, H.U.; Loder, E. The prevalence, burden, and treatment of severe, frequent, and migraine headaches in US minority populations: Statistics from National Survey studies. Headache 2015, 55, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Liu, R.; Zhao, G.; Yang, X.; Qiao, X.; Feng, J.; Steiner, T. The prevalence and burden of primary headaches in China: A population-based door-to-door survey. Headache J. Head Face Pain 2012, 52, 582–591. [Google Scholar] [CrossRef]
- Guo, Y.; Xu, S.; Nie, S.; Han, M.; Zhang, Y.; Chen, J.; Hou, X.; Hong, Y.; Liu, X. Female versus male migraine: An event-related potential study of visual neurocognitive processing. J. Headache Pain 2019, 20, 38. [Google Scholar] [CrossRef]
- Lipton, R.B.; Stewart, W.F.; Diamond, S.; Diamond, M.L.; Reed, M. Prevalence and burden of migraine in the United States: Data from the American Migraine Study II. Headache 2001, 41, 646–657. [Google Scholar] [CrossRef]
- Gibelli, D.; Cappella, A.; Cerutti, E.; Spagnoli, L.; Dolci, C.; Sforza, C. Prevalence of Ponticulus Posticus in a Northern Italian Orthodontic Population: A Lateral Cephalometric Study. Surg. Radiol. Anat. 2016, 38, 309–312. [Google Scholar] [CrossRef]
- Paraskevas, G.; Papaziogas, B.; Tsonidis, C.; Kapetanos, G. Gross morphology of the bridges over the vertebral artery groove on the atlas. Surg. Radiol. Anat. 2005, 27, 129–136. [Google Scholar] [CrossRef]
- Wang, S.-K.; Komatsu, Y.; Mishina, Y. Potential contribution of neural crest cells to dental enamel formation. Biochem. Biophys. Res. Commun. 2011, 415, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bavbek, N.C.; Akay, G.; Kar, I.; Tuncer, C.; Güngör, K.; Tuncer, B.B. Relationship between palatally impacted canines and dimensions and morphology of sella turcica: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2022, 162, 626–635. [Google Scholar] [CrossRef]
- Guarnieri, R.; Germanò, F.; Altieri, F.; Cassetta, M.; Grenga, C.; Padalino, G.; Di Giorgio, R.; Barbato, E. Predictive Analysis of Maxillary Canine Impaction through Sella Turcica Bridging, Ponticulus Posticus Calcification, and Lateral Incisor Anomalies: A Retrospective Observational Study. Methods Protoc. 2022, 5, 91. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; Murmura, G.; Varvara, G.; Traini, T.; Festa, F. Clinical performances and biological features of clear aligners materials in orthodontics. Front. Mater. 2022, 9, 2. [Google Scholar] [CrossRef]
- Macrì, M.; Murmura, G.; Scarano, A.; Festa, F. Prevalence of temporomandibular disorders and its association with malocclusion in children: A transversal study. Front. Public Heal. 2022, 10, 860833. [Google Scholar] [CrossRef] [PubMed]
- Macrì, M.; Flores, N.V.G.; Stefanelli, R.; Pegreffi, F.; Festa, F. Interpreting the prevalence of musculoskeletal pain impacting Italian and Peruvian dentists likewise: A cross-sectional study. Front. Public Heal. 2023, 11, 1090683. [Google Scholar] [CrossRef]
- Kayhan, B.; Çoruk, P.; Ertürk, M.; Sengul, G. Occipitocervical synostosis: Case report. Anatomy 2015, 9, 104–107. [Google Scholar] [CrossRef] [Green Version]
- Sharma, D.K.; Sharma, D.; Sharma, V. Atlantooccipital Fusion: Prevalence and its Developmental and Clinical Correlation. J. Clin. Diagn. Res. JCDR 2017, 11, AC01–AC03. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.K.; Kim, M.S.; Lee, G.J. The incidence and clinical implications of congenital defects of atlantal arch. J. Korean Neurosurg. Soc. 2009, 46, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.; Smith, Z.A.; Dlouhy, B.J.; Dahdaleh, N.S. Complete absence of the posterior arch of C1, Case report. J. Craniovertebral Junction Spine 2014, 5, 176–178. [Google Scholar] [CrossRef]
- Naqshi, B.F.; Shah, A.B.; Gupta, S. Ponticuli In Atlas Vertebrae And Its Clinical Aspect. Int. J. Anat. Res. 2018, 6, 4880–4883. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| % of Population | % of Group with PP | |
|---|---|---|
| Migraine without aura | 5.000% (N 11) | 32.608% (N 15) |
| Migraine with aura | 7.272% (N 16) | 19.565% (N 9) |
| Migraine absent | 87.272% (N 193) | 47.822% (N 22) |
| Marginal column totals | (N 220) | (N 46) |
| Migraine with Aura | Migraine without Aura | Migraine Absent | Marginal Row Totals | |
|---|---|---|---|---|
| Bilateral complete PP | 10.869% (N 5) | 8.695% (N 4) | 8.695% (N 4) | 28.260% (N 13) |
| Complete PP on the left | 2.173% (N 1) | 0.000% (N 0) | 4.347% (N 2) | 6.521% (N 3) |
| Complete PP on the right | 0.000% (N 0) | 0.000% (N 0) | 4.347% (N 2) | 4.347% (N 2) |
| Complete PP on the right and partial on the left | 2.173% (N 1) | 2.173% (N 1) | 2.173% (N 1) | 2.173% (N 3) |
| Complete PP on the left and partial on the right | 0.000% (N 0) | 0.000% (N 0) | 4.347% (N 2) | 4.347% (N 2) |
| Partial bilateral PP | 10.869% (N 5) | 6.521% (N 3) | 15.211% (N 7) | 32.595% (N 15) |
| Partial left PP | 4.347% (N 2) | 2.173% (N 1) | 4.347% (N 2) | 10.869% (N 5) |
| Partial right PP | 2.173% (N 1) | 0.000% (N 0) | 4.347% (N 2) | 6.521% (N 3) |
| Marginal column totals | 32.595% (N 15) | 19.557% (N 9) | 47.806% (N 22) | (N 46) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macrì, M.; Rendina, F.; Feragalli, B.; Pegreffi, F.; Festa, F. Prevalence of Ponticulus Posticus and Migraine in 220 Orthodontic Patients: A Cross-Sectional Study. Biology 2023, 12, 471. https://doi.org/10.3390/biology12030471
Macrì M, Rendina F, Feragalli B, Pegreffi F, Festa F. Prevalence of Ponticulus Posticus and Migraine in 220 Orthodontic Patients: A Cross-Sectional Study. Biology. 2023; 12(3):471. https://doi.org/10.3390/biology12030471
Chicago/Turabian StyleMacrì, Monica, Fabiola Rendina, Beatrice Feragalli, Francesco Pegreffi, and Felice Festa. 2023. "Prevalence of Ponticulus Posticus and Migraine in 220 Orthodontic Patients: A Cross-Sectional Study" Biology 12, no. 3: 471. https://doi.org/10.3390/biology12030471