
Advancement of Marginal Bone and Soft Tissue Aesthetics for Slope-Configured Implants
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Treatment
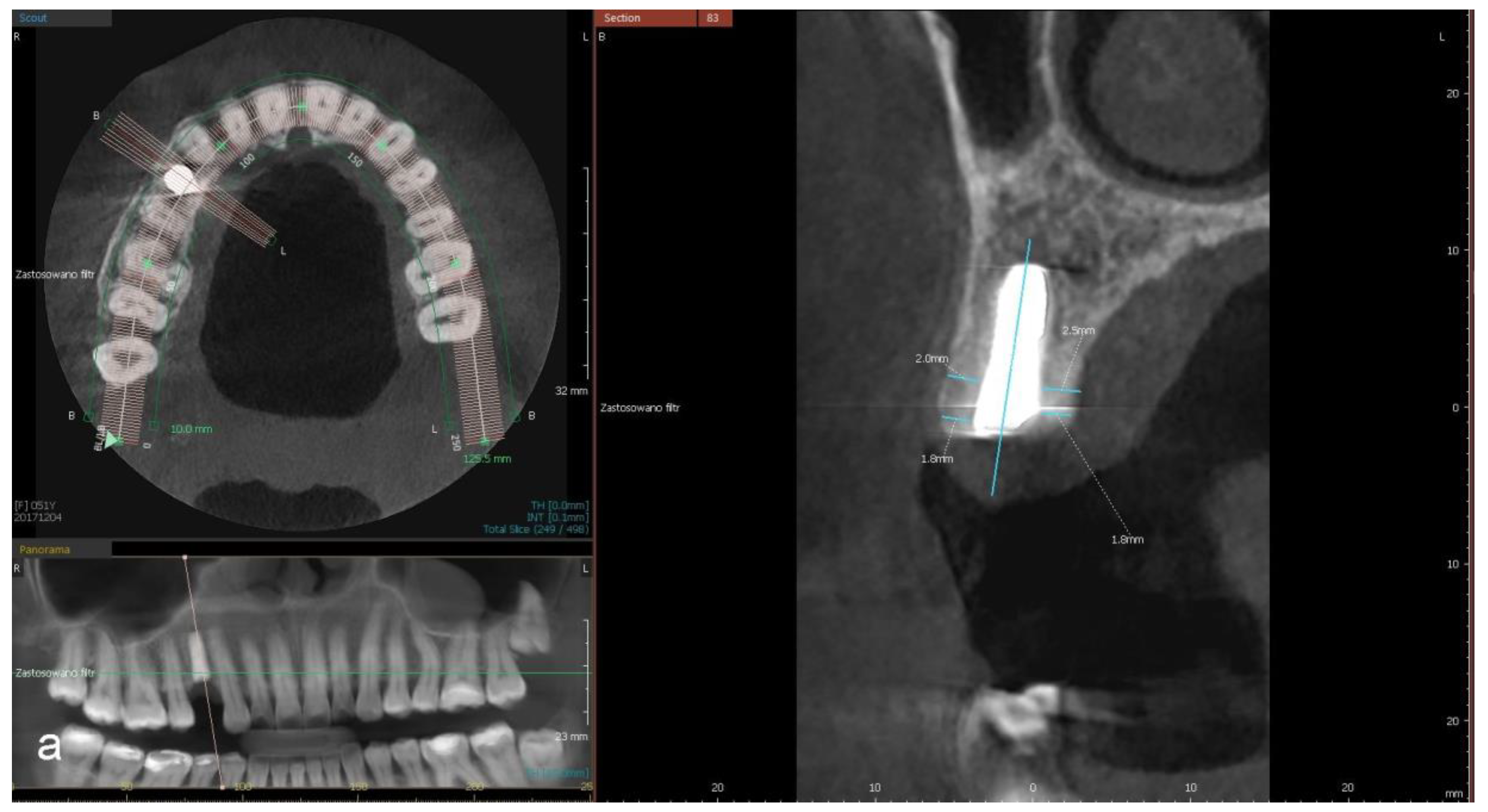
2.3. Radiographic Examination
- a distance between the implant’s platform and buccal and palatal/lingual bone margin (dehiscence)
- thickness of buccal and palatal/lingual plates, 1 mm and 3 mm apically from the implant’s platform (perpendicular to the long axis of the implant).
2.4. Aesthetic Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CBCT | cone-beam computed tomography |
| IMP | immediately after the implantation |
| PES | Pink Aesthetic Score |
| PI | Papilla Index |
| PId | Papilla Index for distal papilla |
| PIm | Papilla Index for mesial papilla |
| TCD | after the temporary crown delivery |
| 1YIMP | one year after implantation |
| DCD | after the definitive crown delivery |
References
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Jung, R.E.; Heitz-Mayfield, L.; Schwarz, F. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 3-Aesthetics of peri-implant soft tissues. Clin. Oral. Implant Res. 2018, 29, 14–17. [Google Scholar] [CrossRef]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single tooth extraction: A clinical and radiographic 12 month prospective study. Int. J. Periodontics Rest. Dent. 2003, 23, 313–323. [Google Scholar]
- Araújo, M.G.; Silva, C.O.; Misawa, M.; Sukekava, F. Alveolar socket healing: What can we learn? Periodontology 2000 2015, 68, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Troeltzsch, M.; Troeltzsch, M.; Kauffmann, P.; Gruber, R.; Brockmeyer, P.; Moser, N.; Rau, A.; Schliephake, H. Clinical efficacy of grafting materials in alveolar ridge augmentation: A systematic review. J. Craniomaxillofac. Surg. 2016, 44, 1618–1629. [Google Scholar] [CrossRef]
- Elnayef, B.; Monje, A.; Gargallo-Albiol, J.; Galindo-Moreno, P.; Wang, H.-L.; Hernández-Alfaro, F. Vertical ridge augmentation in the atrophic mandible: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Implant 2017, 32, 291–312. [Google Scholar] [CrossRef]
- Cucchi, A.; Vignudelli, E.; Napolitano, A.; Marchetti, C.; Corinaldesi, G. Evaluation of complication rates and vertical bone gain after guided bone regeneration with non-resorbable membranes versus titanium meshes and resorbable membranes. A randomized clinical trial. Clin. Implant Dent. Relat.Res. 2017, 19, 821–832. [Google Scholar] [CrossRef]
- Felice, P.; Barausse, C.; Pistilli, R.; Ippolito, D.R.; Esposito, M. Five-year results from a randomised controlled trial comparing prostheses supported by 5-mm long implants or by longer implants in augmented bone in posterior atrophic edentulous jaws. Int. J. Oral. Implant 2019, 12, 25–37. [Google Scholar]
- Abrahamsson, I.; Welander, M.; Linder, E.; Berglundh, T. Healing at implants placed in an alveolar ridge with a sloped configuration: An experimental study in dogs. Clin. Implant Dent. Relat. Res. 2014, 16, 62–69. [Google Scholar] [CrossRef]
- Schiegnitz, E.; Noelken, R.; Moergel, M.; Berres, M.; Wagner, W. Survival and tissue maintenance of an implant with a sloped configurated shoulder in the posterior mandible—A prospective multicenter study. Clin. Oral. Implants Res. 2017, 28, 721–726. [Google Scholar] [CrossRef]
- Tu, C.-C.; Wang, S.-H.; Hu, C.-Y.; Chang, P.-C. Comparison of regular- and slope-configurated dental implants placed in the edentulous ridge with height discrepancy: A pilot randomized controlled trial. ScienceDirect 2020, 120, 1386–1393. [Google Scholar] [CrossRef]
- Noelken, R.; Donati, M.; Fiorellini, J.; Gellrich, N.-C.; Parker, W.; Wada, K.; Berglundh, T. Soft and hard tissue alterations around implant placed in an alveolar ridge with a sloped configuration. Clin. Oral. Implants Res. 2014, 25, 3–9. [Google Scholar] [CrossRef]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score in the anterior mandible. Clin. Oral. Implants Res. 2005, 16, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Jemt, T. Regeneration of gingival papillae after single-implant treatment. Int. J. Periodontics Res. Dent. 1997, 17, 326–333. [Google Scholar]
- Veltri, M.; Ekestubbe, A.; Abrahamsson, I.; Wennström, J.L. Three-Dimensional buccal bone anatomy and aesthetic outcome of single dental implants replacing maxillary incisors. Clin. Oral. Implants Res. 2016, 27, 956–963. [Google Scholar] [CrossRef]
- Meijer, H.J.A.; Slagter, K.W.; Vissink, A.; Raghoebar, G.M. Buccal bone thickness at dental implants in the maxillary anterior region with large bony defects at time of immediate implant placement: A 1-year cohort study. Clin. Implant Dent. Relat. Res. 2019, 21, 73–79. [Google Scholar] [CrossRef]
- Temmerman, A.; Keestra, J.A.J.; Coucke, W.; Teughels, W.; Quirynen, M. The outcome of oral implants placed in bone with limited bucco-oral dimensions: A 3-year follow-up study. J. Clin. Periodontol. 2015, 42, 311–318. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Horner, K.; Jacobs, R. Use of cone beam computed tomography in implant dentistry: Current concepts, indications and limitations for clinical practice and research. Periodontol. 2000 2017, 73, 51–72. [Google Scholar] [CrossRef]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are Hounsfield units applicable? Dentomaxillofacial 2015, 44, 20140238. [Google Scholar] [CrossRef]
- Hatcher, D.C.; Aboudara, C.L. Diagnosis goes digital. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 512–515. [Google Scholar] [CrossRef]
- Ballrick, J.W.; Martin Palomo, J.; Ruch, E.; Amberman, B.D.; Hans, M.G. Image distortion and spatial resolution of a commercially available cone-beam computed tomography machine. Am. J. Orthod Dentofac. Orthop. 2008, 134, 573–582. [Google Scholar] [CrossRef]
- Stratemann, S.A.; Huang, J.C.; Maki, K.; Miller, A.J.; Hatcher, D.C. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac. Radiol. 2008, 37, 80–93. [Google Scholar] [CrossRef]
- Razavi, T.; Palmer, R.M.; Davies, J.; Wilson, R.; Palme, P.J. Accuracy of measuring the cortical bone thickness adjacent to dental implants using cone beam computed tomography. Clin. Oral. Implants Res. 2010, 21, 718–725. [Google Scholar] [CrossRef]
- Naitoh, M.; Hayashi, H.; Tsukamoto, N.; Ariji, N. Labial bone assessment surrounding dental implant using cone-beam computed tomography: An in vitro study. Clin. Oral. Implants Res. 2012, 23, 970–974. [Google Scholar] [CrossRef]
- Tettamanti, S.; Millen, C.; Gavric, J.; Buser, D.; Belser, U.C.; Brägger, U.; Wittneben, J.-G. Esthetic evaluation of implant crowns and peri-implant soft tissue in the anterior maxilla: Comparison and reproducibility of three different indices. Clin. Implant Dent. Relat Res. 2016, 18, 517–526. [Google Scholar] [CrossRef]
- Hof, M.; Umar, N.; Budas, N.; Seemann, R.; Pommer, B.; Zechner, W. Evaluation of implant esthetics using eight objective indices-Comparative analysis of reliability and validity. Clin. Oral. Implants Res. 2018, 29, 697–706. [Google Scholar] [CrossRef]
- Hof, M.; Pommer, B.; Strbac, G.D.; Sütö, D.; Watzek, G.; Zechner, W. Esthetic evaluation of single-tooth implants in the anterior maxilla following autologous bone augmentation. Clin. Oral. Implants Res. 2011, 24, 88–93. [Google Scholar] [CrossRef]
- Hof, M.; Tepper, G.; Koller, B.; Krainhöfner, M.; Watzek, G.; Pommer, B. Esthetic evaluation of single-tooth implants in the anterior mandible. Clin. Oral. Implants 2014, 25, 1022–1026. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; De Bruyn, H.; Dierens, M.; De Rouck, T. Single implant treatment in healing versus healed sites of the anterior maxilla: An aesthetic evaluation. Clin. Implant Dent. Relat Res. 2012, 14, 517–526. [Google Scholar] [CrossRef]
- Lai, H.-C.; Zhang, Z.-Y.; Wang, F.; Zhuang, L.-F.; Liu, X.; Pu, Y.P. Evaluation of soft-tissue alteration around implant- supported single-tooth restoration in anterior maxilla: The pink esthetic score. Clin. Oral. Implants Res. 2008, 19, 560–564. [Google Scholar] [CrossRef]
- Meijndert, L.; Meijer, H.J.A.; Stellingsma, K.; Stegenga, B.; Raghoebar, G.M. Evaluation of aesthetics of implant-supported single-tooth replacements using different bone augmentation procedures: A prospective randomized clinical study. Clin. Oral. Implants Res. 2007, 18, 715–719. [Google Scholar] [CrossRef]
- Agabiti, I.; Alí Apaza Alccayhuaman, K.; Nakajima, Y.; Botticelli, D. An enigmatic soft tissue creeping phenomenon: The spontaneous peri-implant mucosa margin and papilla growth. A retrospective clinical study. Clin. Exp. Dent. Res. 2021, 7, 474–483. [Google Scholar] [CrossRef]
- Cardaropoli, G.; Lekholm, U.; Wennström, J.L. Tissue alterations at implant-supported single-tooth replacements: A 1-year prospective clinical study. Clin. Implant Dent. Relat Res. 2006, 17, 165–171. [Google Scholar] [CrossRef]
- Cosyn, J.; Raes, M.; Packet, M.; Cleymaet, R.; De Bruyn, H. Disparity in embrasure fill and papilla height between tooth- and implant-borne fixed restorations in the anterior maxilla: A cross-sectional study. J. Clin. Periodontol. 2013, 40, 728–733. [Google Scholar] [CrossRef]
- Priest, G. Predictability of soft tissue form around single-tooth implant restorations. Int. J. Periodontics Res. Dent. 2003, 23, 19–27. [Google Scholar]
- Barwacz, C.A.; Stanford, C.M.; Diehl, U.A.; Cooper, L.F.; Feine, J.; McGuire, M.; Scheyer, T. Pink Esthetic Score outcomes around three implant-abutment configurations: 3-year results. Int. J. Oral. Maxillofac. Implants 2018, 33, 1126–1135. [Google Scholar] [CrossRef]
- Schropp, L.; Isidor, F.; Kostopoulos, L.; Wenzel, A. Interproximal papilla levels following early versus delayed placement of single-tooth implants: A controlled clinical trial. Int. Oral. Maxillofac. Impl. 2005, 20, 753–761. [Google Scholar] [CrossRef]
- Schropp, L.; Isidor, F. Papilla dimension and soft tissue level after early vs. delayed placement of single-tooth implants: 10-year results from a randomized controlled clinical trial. Clin. Oral. Implants Res. 2015, 26, 278–286. [Google Scholar] [CrossRef]
- Grunder, U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int. J. Periodontics Res. Dent. 2000, 20, 11–17. [Google Scholar]
- Choquet, V.; Hermans, M.; Adriaenssens, P.; Daelemans, P.; Tarnow, D.P.; Malevez, C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J. Periodontol. 2001, 72, 1364–1371. [Google Scholar] [CrossRef]
- Benic, G.I.; Wolleb, K.; Sancho-Puchades, M.; Hammerle, C.H. Systematic review of parameters and methods for the professional assessment of aesthetic in dental implant research. J. Clin. Periodontol. 2012, 39, 160–192. [Google Scholar] [CrossRef] [PubMed]
- Roccuzzo, M.; Roccuzzo, A.; Ramanuskaite, A. Papilla height in relation to the distance between bone crest and interproximal contact point at single-tooth implants: A systematic review. Clin. Oral. Implants Res. 2017, 29, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Lops, D.; Chiapasco, M.; Rossi, A.; Bressan, E.; Romeo, E. Incidence of inter-proximal papilla between a tooth and an adjacent immediate implant placed into a fresh extraction socket: 1-year prospective study. Clin. Oral. Implants Res. 2008, 19, 1135–1140. [Google Scholar] [CrossRef]
- Romeo, E.; Lops, D.; Rossi, A.; Storelli, S.; Rozza, R.; Chiapasco, M. Surgical and prosthetic management of interproximal region with single-implant restorations: 1-year prospective study. J. Periodontol. 2018, 79, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.; Felton, D.A.; Kugelberg, C.F.; Ellner, S.; Chaffee, N.; Molina, A.L.; Moriarty, J.D.; Paquette, D.; Palmqvist, U. A multicenter 12-month evaluation of single-tooth implants restored 3 weeks after 1-stage surgery. Int. J. Oral. Maxillofac. Implant 2001, 16, 182–192. [Google Scholar]
- Palmer, R.M.; Farkondeh, N.; Palmer, P.J.; Wilson, R.F. Astra Tech single-tooth implants: An audit of patient satisfaction and soft tissue form. J. Clin. Periodontol. 2007, 34, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; De Kok, I.J.; Zhong, S.; Vo, C.; Mendonça, G.; Nares, S.; Cooper, L. The role of implant-tooth distance on marginal bone levels and esthetics. Int. J. Oral. Maxillofac. Implants 2019, 34, 499–505. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Mean ± SD | Minimum | Maximum | Median | −95%Cl | 95%Cl | Difference ± SD | p (Post-Hock) | |
|---|---|---|---|---|---|---|---|---|---|
| 1 mm (n = 16) | BP0 | 1.85 ± 0.68 | 0.9 | 3.2 | 1.77 | 1.53 | 2.17 | ||
| PP0 | 1.87 ± 0.75 | 0.5 | 3.2 | 1.8 | 1.52 | 2.23 | |||
| BPtc | 1.83 ± 0.66 | 0.65 | 3.05 | 1.65 | 1.48 | 2.18 | −0.13 ± 0.44 | 0.27 | |
| PPtc | 1.9 ± 0.76 | 0.5 | 3.65 | 2.1 | 1.5 | 2.29 | −0.1 ± 0.68 | 0.50 | |
| BP1y | 1.53 ± 0.77 | 0.1 | 3.55 | 1.4 | 1.16 | 1.89 | −0.32 ± 0.53 | 0.04 | |
| PP1y | 1.67 ± 0.69 | 0.7 | 3.35 | 1.72 | 1.34 | 1.99 | −0.21 ± 0.71 | 0.22 | |
| 3 mm (n = 30) | BP0 | 1.99 ± 1.05 | 0.2 | 4.65 | 1.72 | 1.59 | 2.38 | ||
| PP0 | 2.55 ± 1.01 | 0.7 | 4.4 | 2.62 | 2.17 | 2.93 | |||
| BPtc | 1.67 ± 1.04 | 0.2 | 4.7 | 1.4 | 1.27 | 2.07 | −0.23 ± 0.42 | 0.03 | |
| PPtc | 2.6 ± 1.07 | 0.7 | 4.8 | 2.65 | 2.19 | 3.01 | 0.06 ± 0.43 | 0.43 | |
| BP1y | 1.84 ± 1.2 | 0.3 | 4.9 | 1.62 | 1.39 | 2.29 | −0.15 ± 0.39 | 0.39 | |
| PP1y | 2.6 ± 0.95 | 0.85 | 4.25 | 2.65 | 2.24 | 2/95 | 0.05 ± 0.33 | 0.39 |
| Parameter | Thickness Increase | Thickness Reduction | No Change | ||
|---|---|---|---|---|---|
| 1 mm (n = 16) | Buccal plate | IMP—tc | 6 | 10 | 0 |
| tc—1y | 4 | 10 | 2 | ||
| Palatal/lingual plate | IMP—tc | 7 | 9 | 0 | |
| tc—1y | 5 | 8 | 3 | ||
| 3 mm (n = 30) | Buccal plate | IMP—tc | 6 | 19 | 5 |
| tc—1y | 17 | 12 | 1 | ||
| Palatal/lingual plate | IMP—tc | 16 | 12 | 2 | |
| tc—1y | 15 | 12 | 3 |
| PES | Median | Minimum | Maximum | p (tc-dc) | p (tc-dc 1y) |
|---|---|---|---|---|---|
| MPtc | 1.0 | 0.0 | 1.0 | ||
| DPtc | 1.0 | 0.0 | 1.0 | ||
| Ctc | 1.0 | 0.5 | 2.0 | ||
| LMtc | 1.0 | 0.5 | 2.0 | ||
| CCtc | 1.0 | 1.0 | 2.0 | ||
| PEStc | 5.0 | 3.0 | 8.0 | ||
| MPdc | 1.0 | 1.0 | 2.0 | 0.006 | |
| DPdc | 1.0 | 0.0 | 2.0 | 0.031 | |
| Cdc | 1.0 | 1.0 | 2.0 | 0.03 | |
| LMdc | 1.5 | 0.5 | 2.0 | 0.51 | |
| CCdc | 1.0 | 1.0 | 2.0 | 0.0305 | |
| PESdc | 6.0 | 4.0 | 8.0 | 0.0007 | |
| MPdc 1y | 1.0 | 1 | 2 | 0.009 | |
| DPdc 1y | 1.0 | 0 | 2 | 0.13 | |
| Cdc 1y | 1.5 | 1 | 2 | 0.135 | |
| LMdc 1y | 2.0 | 1 | 2 | 0.27 | |
| CCdc 1y | 1.25 | 1 | 2 | 0.13 | |
| PESdc 1y | 7.75 | 5 | 10 | <0.0001 |
| PI | Median | Minimum | Maximum | p (tc-dc) | p (tc-dc 1y) |
|---|---|---|---|---|---|
| PIMtc | 1.00 | 0 | 2 | ||
| PIDtc | 1.00 | 0 | 2 | ||
| PIMdc | 1.25 | 1 | 3 | 0.0355 | |
| PIDdc | 1.00 | 0 | 3 | 0.1836 | |
| PIMdc 1y | 2 | 1 | 3 | <0.0001 | |
| PIDdc 1y | 2 | 0 | 3 | <0.0001 |
| Parameter | Kendall’s W | P |
|---|---|---|
| BP | 0.994 | 0.0012 |
| PP | 0.989 | 0.0013 |
| PES | 0.936 | 0.0030 |
| PIM | 0.947 | 0.0025 |
| PID | 0.938 | 0.0029 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pietruska, M.; Pietruski, J.K. Advancement of Marginal Bone and Soft Tissue Aesthetics for Slope-Configured Implants. Coatings 2022, 12, 1295. https://doi.org/10.3390/coatings12091295
Pietruska M, Pietruski JK. Advancement of Marginal Bone and Soft Tissue Aesthetics for Slope-Configured Implants. Coatings. 2022; 12(9):1295. https://doi.org/10.3390/coatings12091295
Chicago/Turabian StylePietruska, Małgorzata, and Jan Krzysztof Pietruski. 2022. "Advancement of Marginal Bone and Soft Tissue Aesthetics for Slope-Configured Implants" Coatings 12, no. 9: 1295. https://doi.org/10.3390/coatings12091295