
Novel Technology for Enamel Remineralization in Artificially Induced White Spot Lesions: In Vitro Study
 , and
, and
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
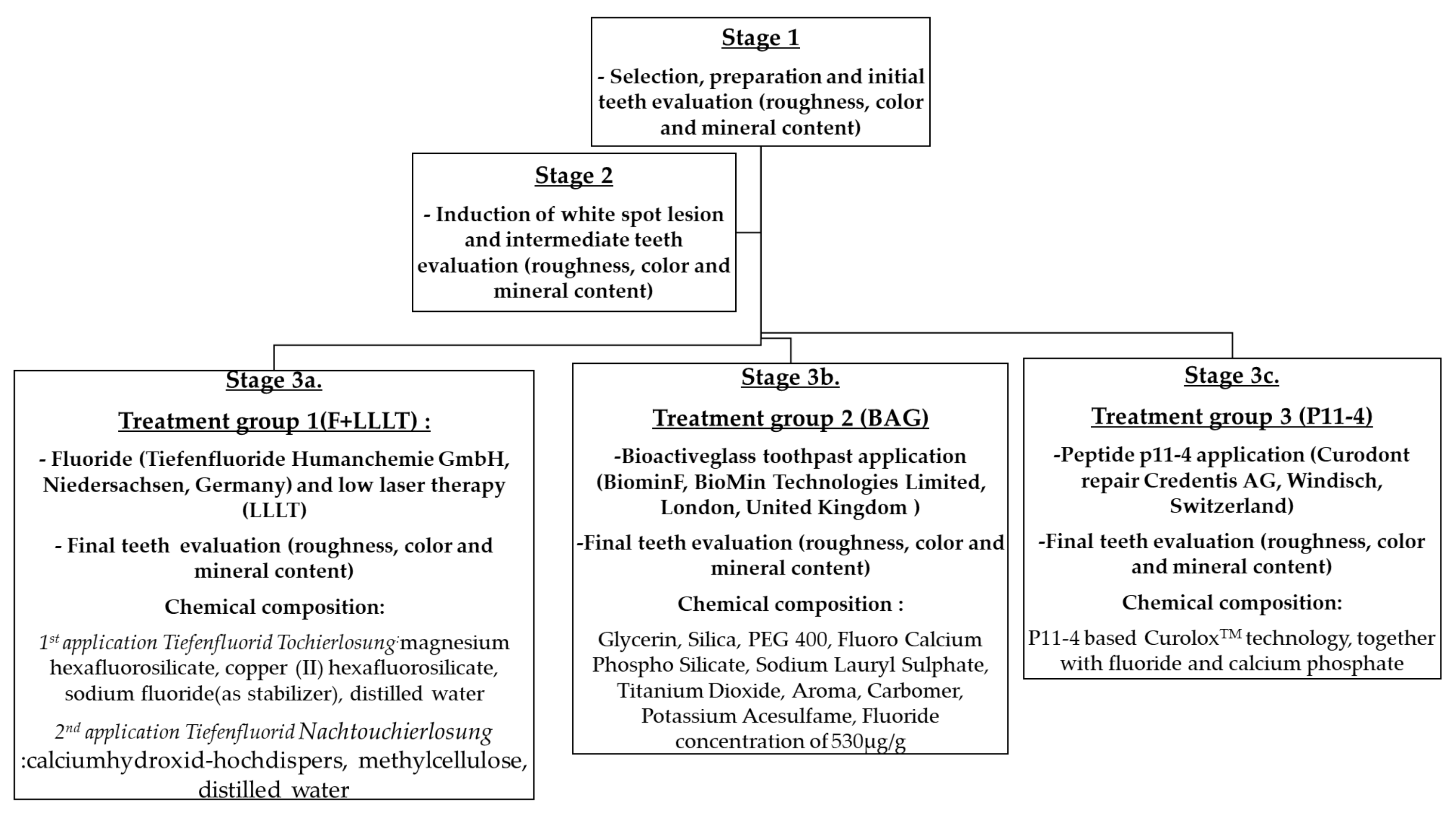
2. Materials and Methods
3. Results
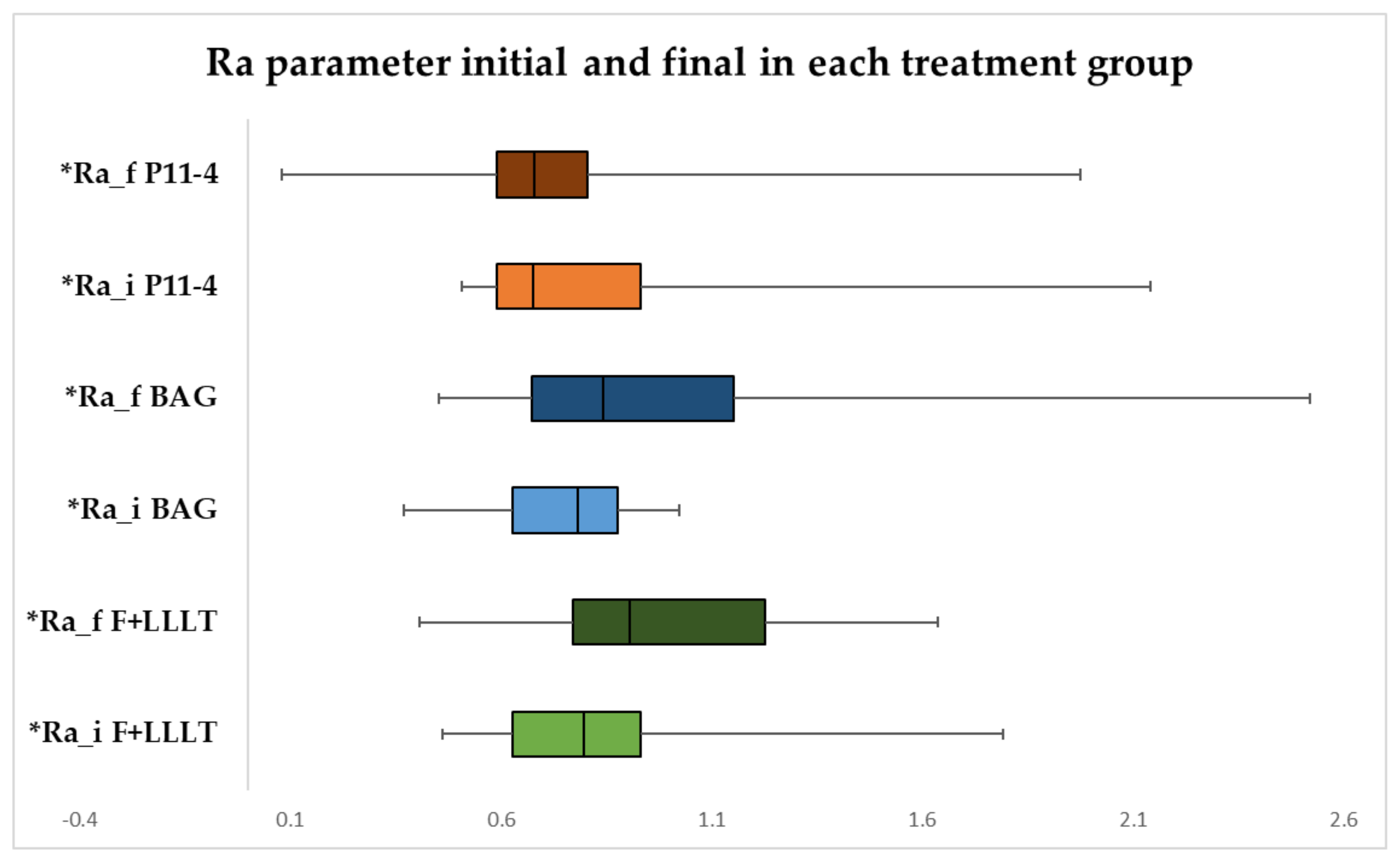
3.1. Surface Roughness Measurement Ra Parameter in Each Treatment Group
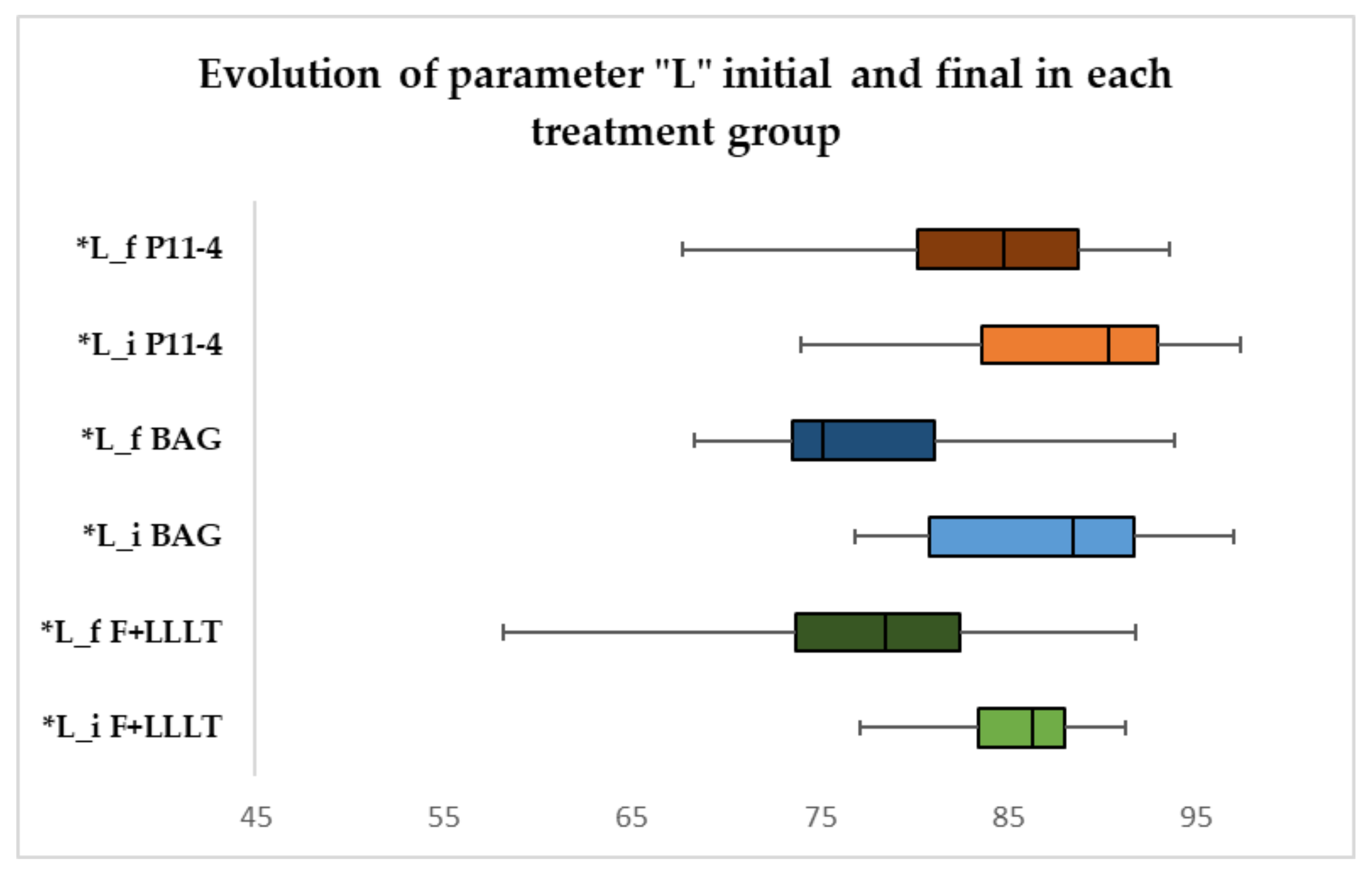
3.2. Color Measurement of “L” Parameter in Each Treatment Group
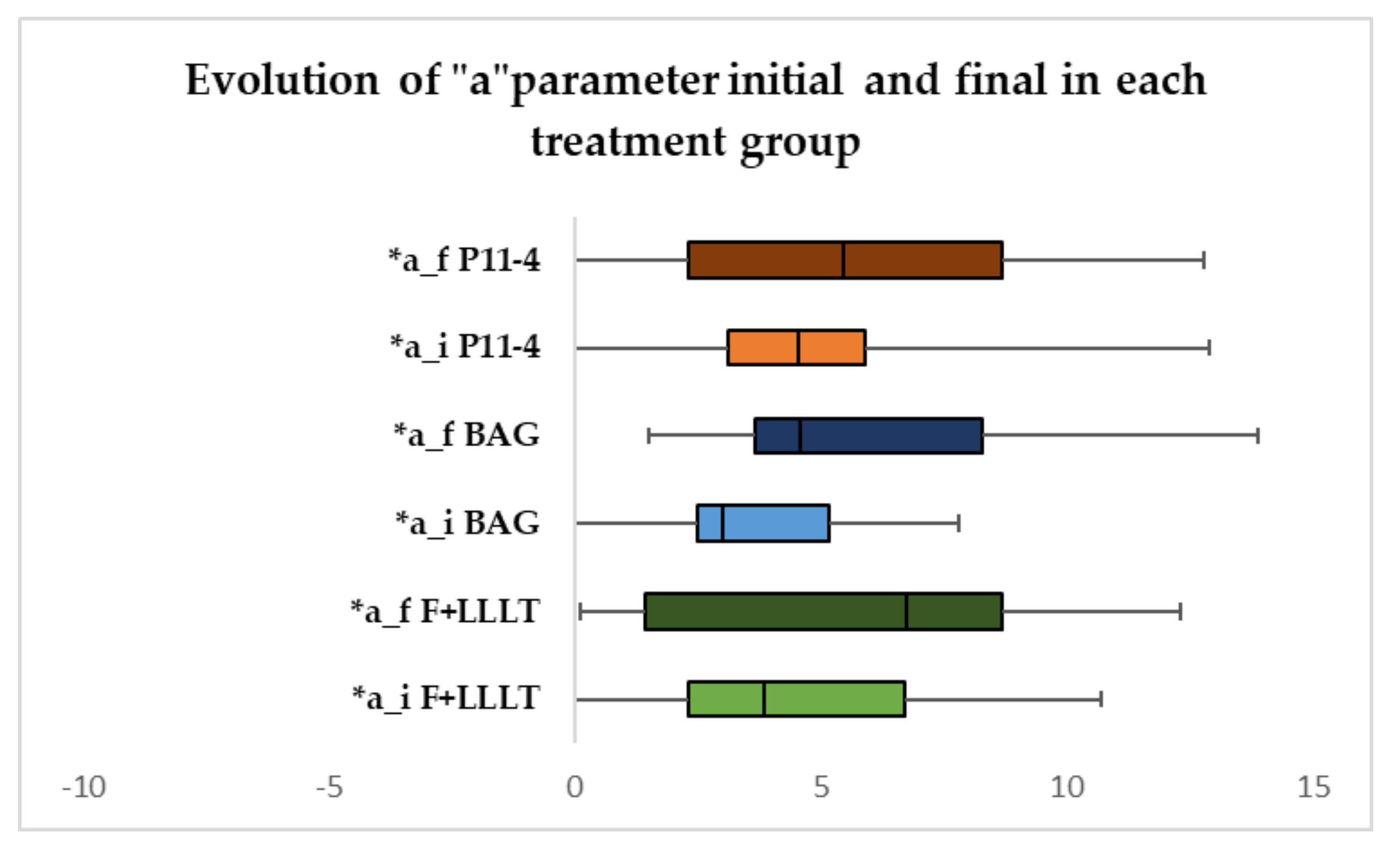
3.3. Colour Measurement of “a” Parameter in Each Treatment Group
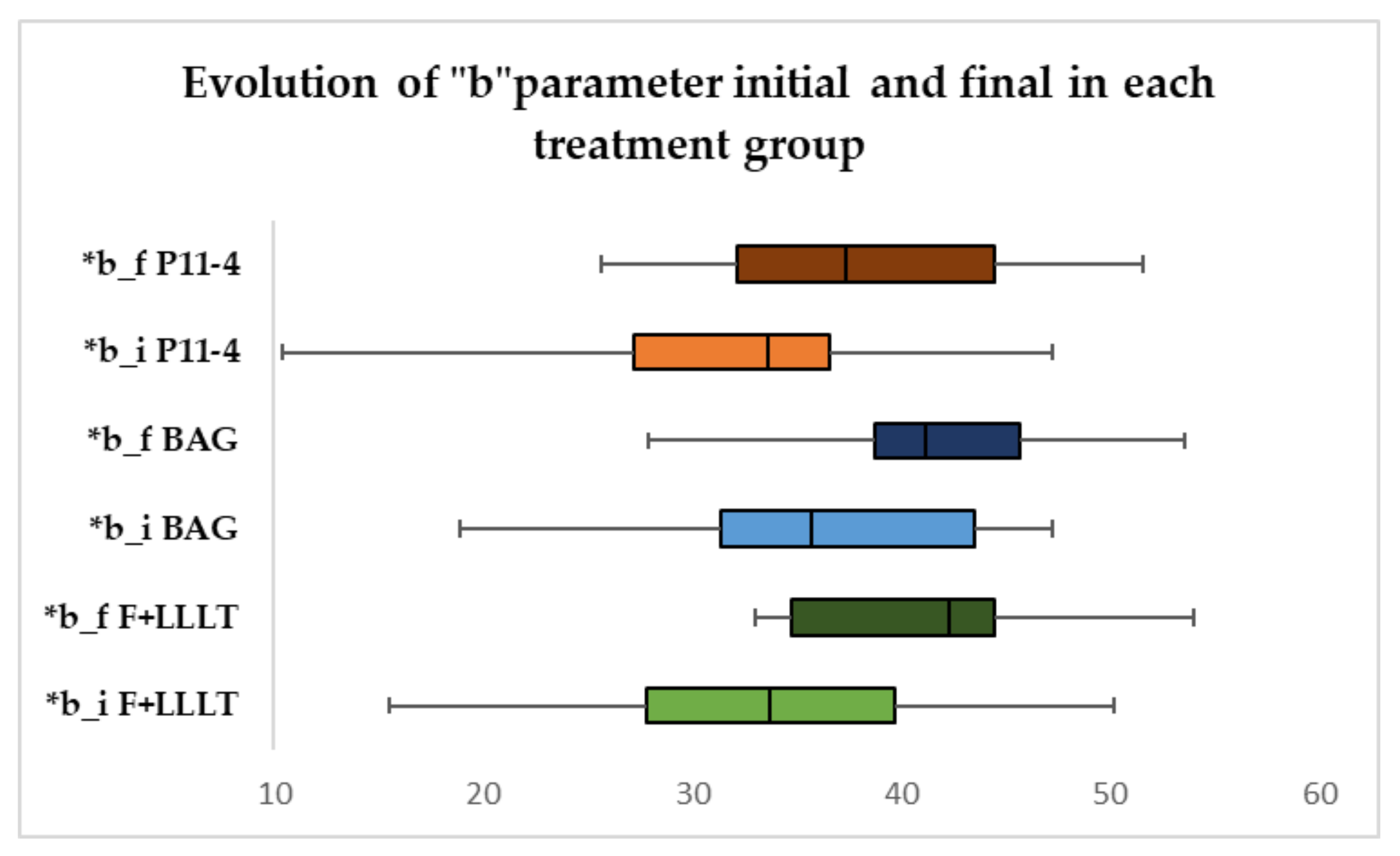
3.4. Colour Measurement of “b” Parameter in Each Treatment Group
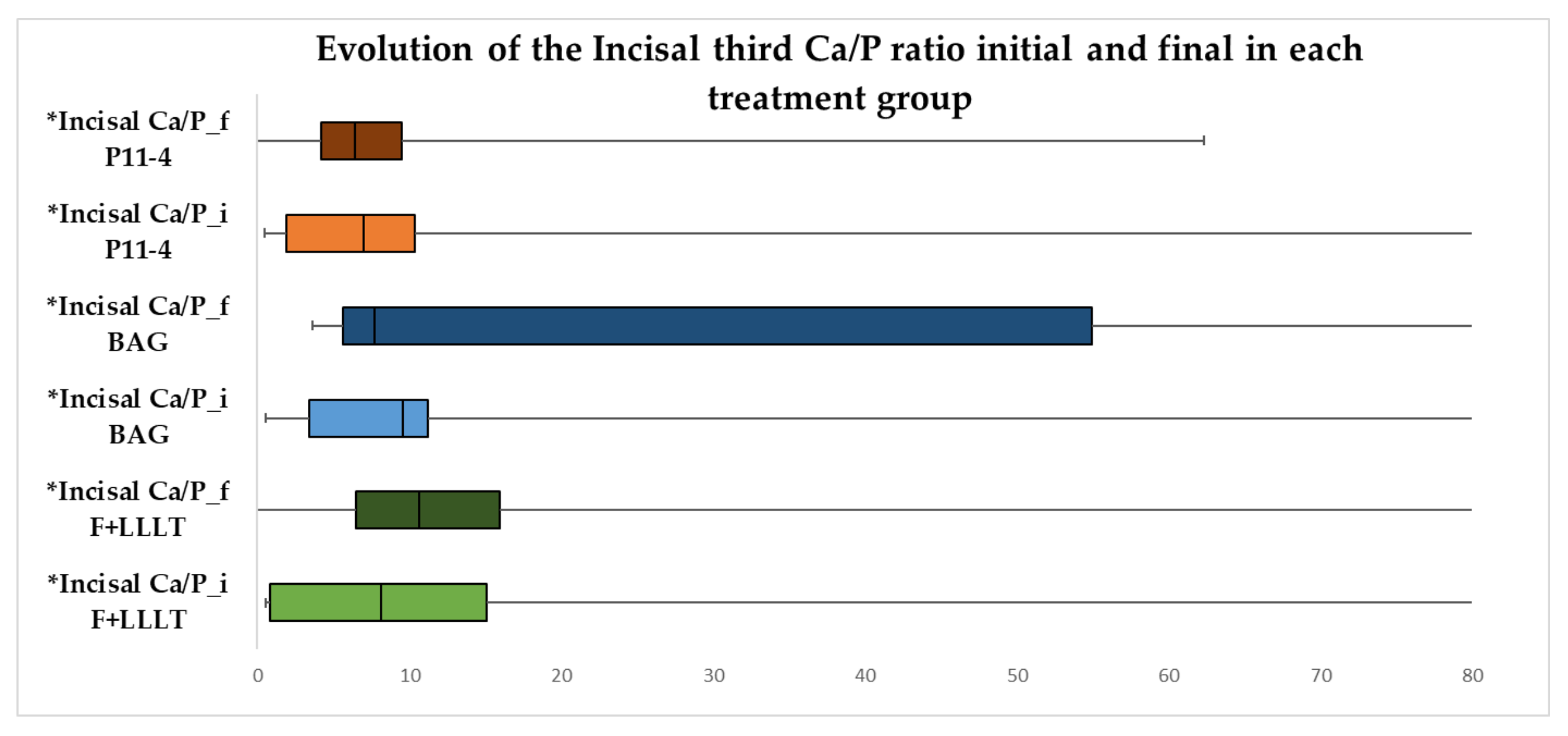
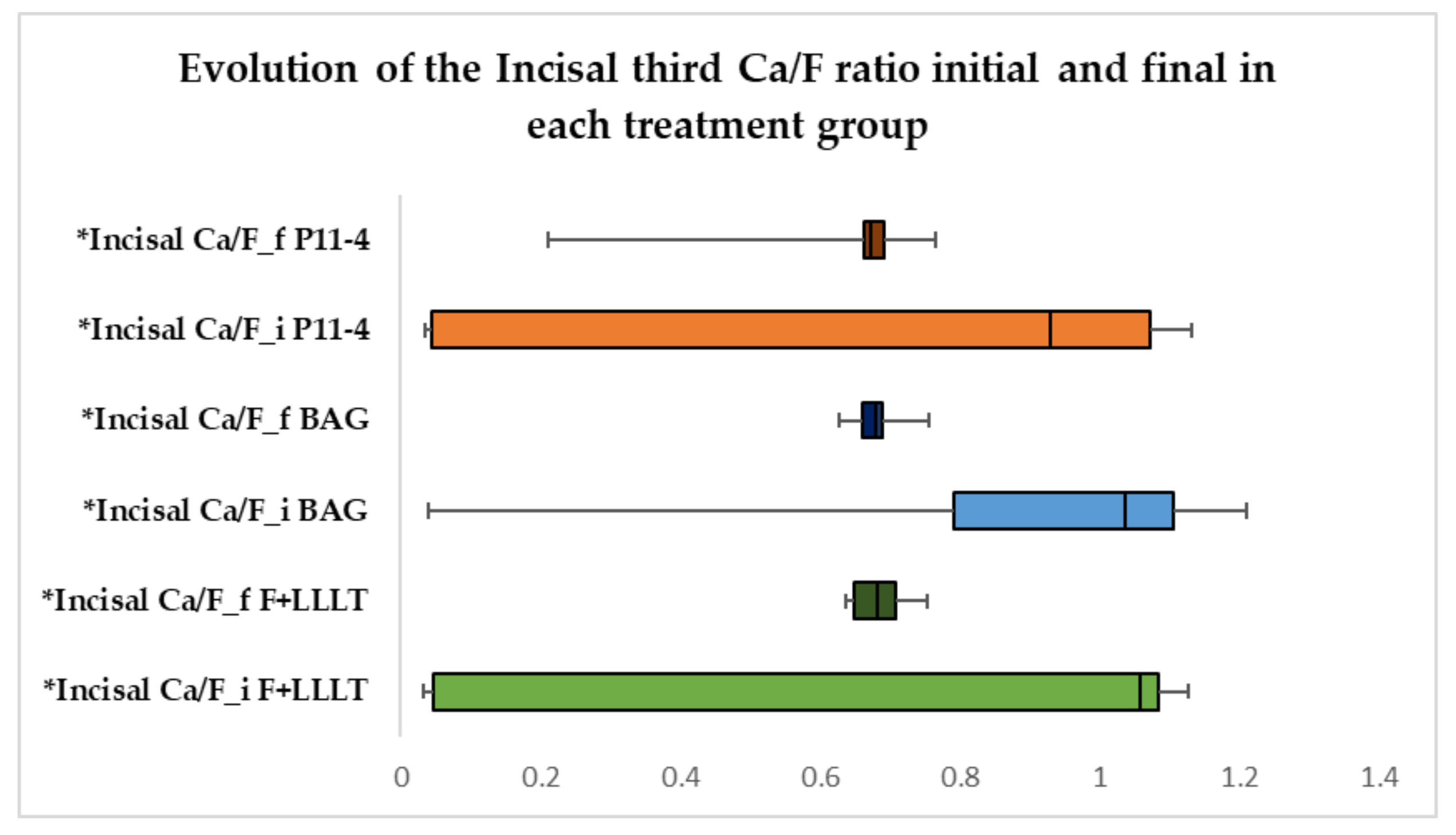
3.5. Evolution of the Incisal Third Ca/P and Ca/F Ratio in Each Treatment Group
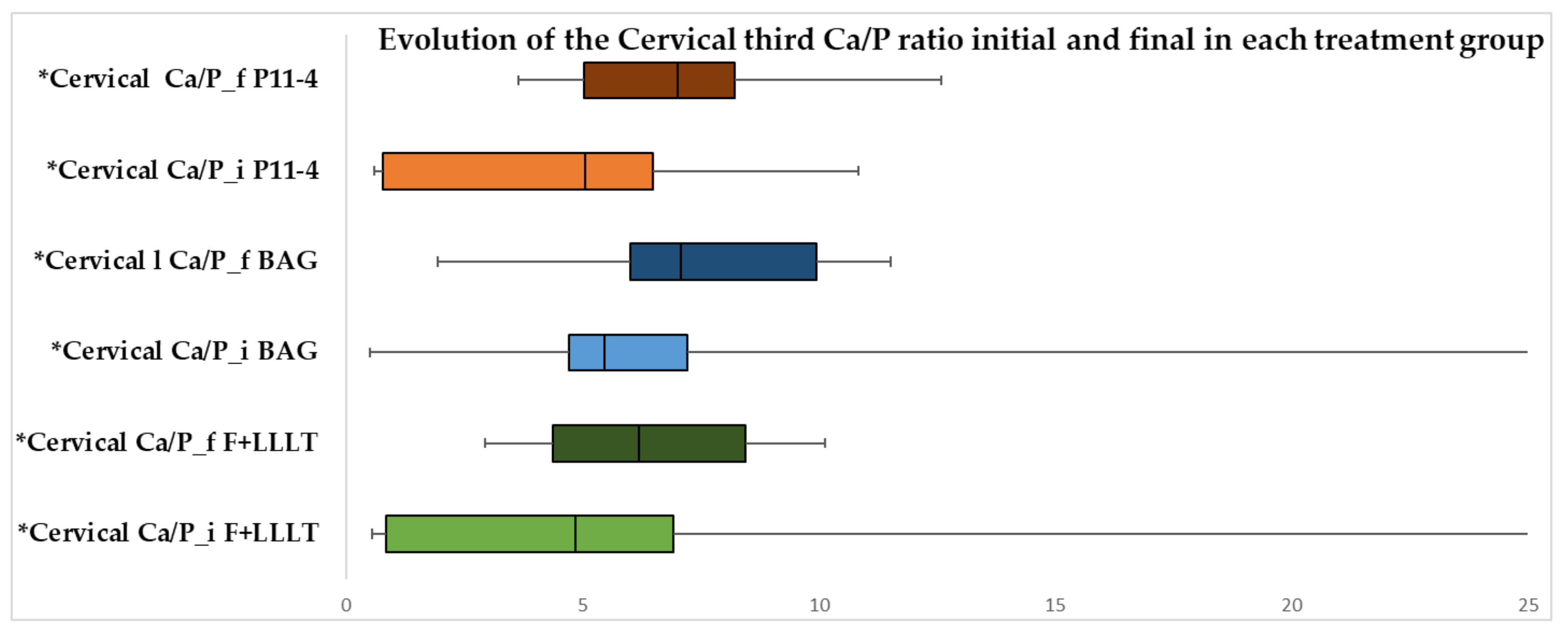
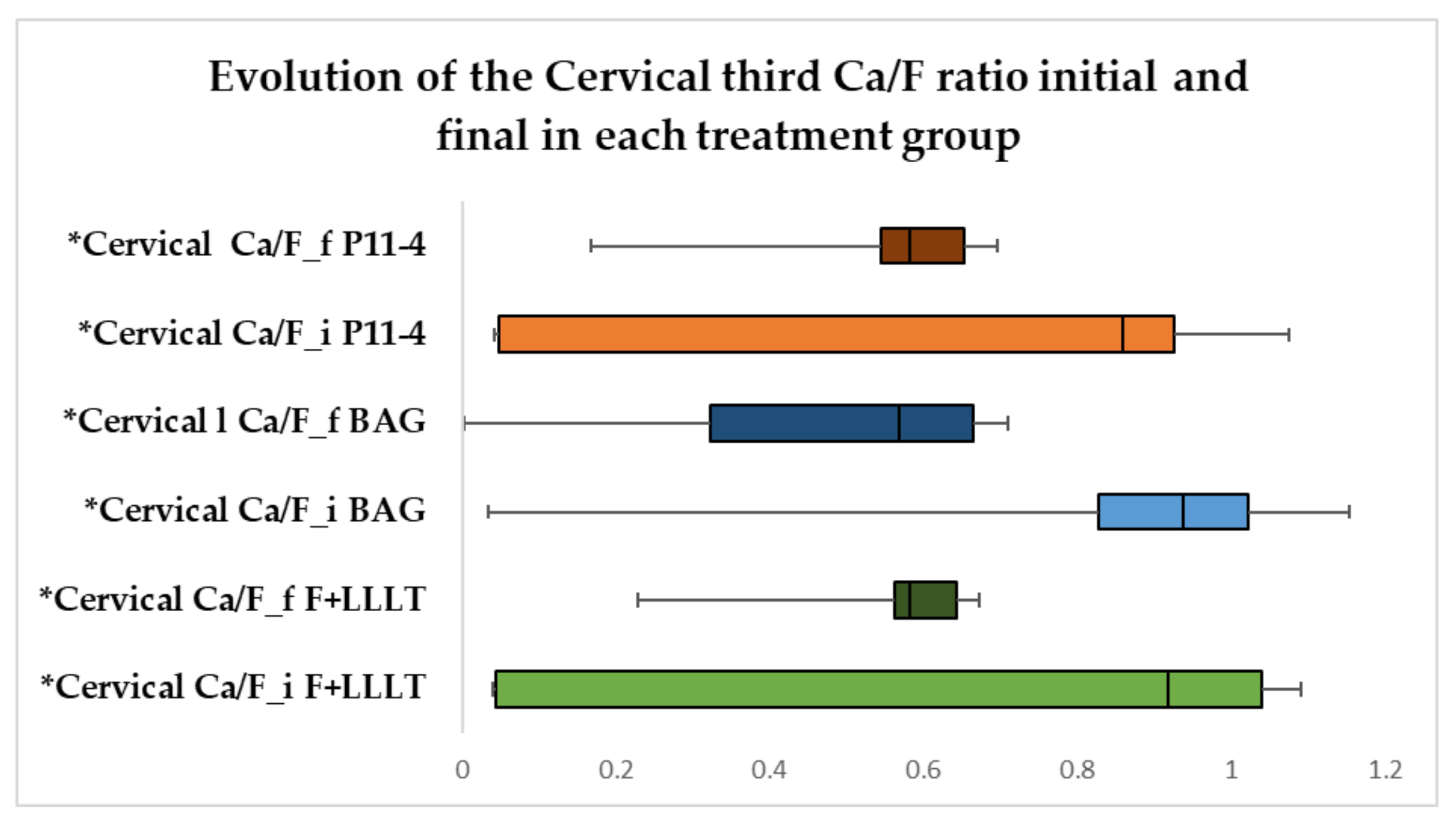
3.6. Evolution of Cervical Ca/P and Ca/F Ratio in Each Treatment Group
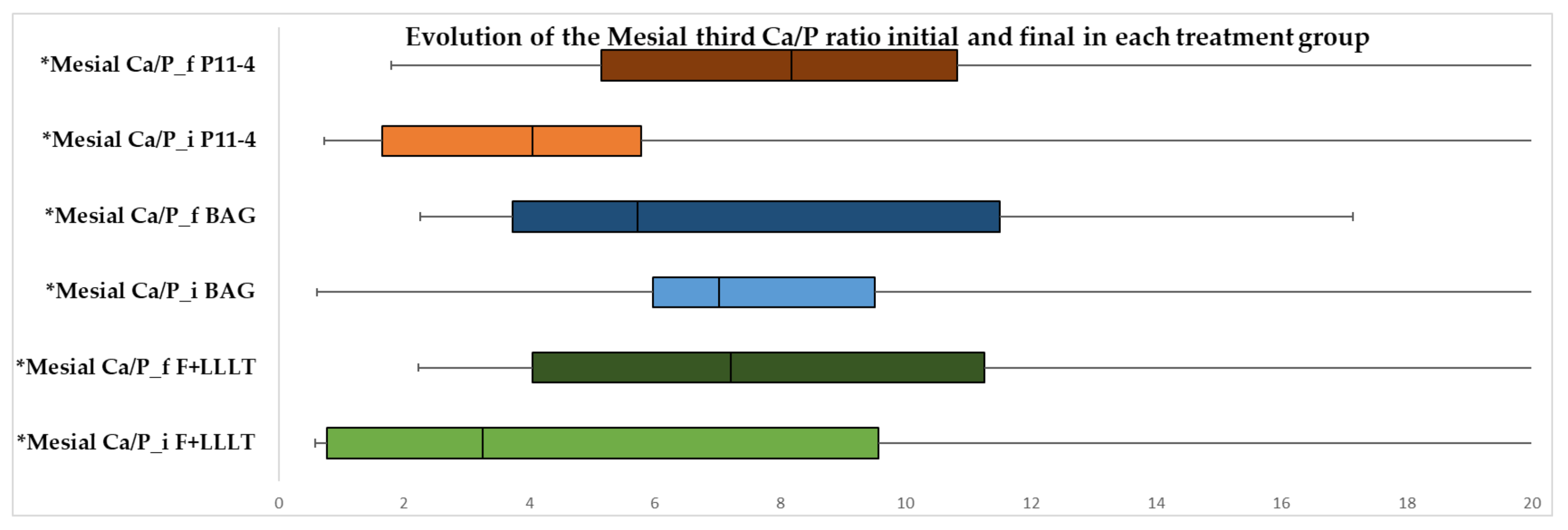
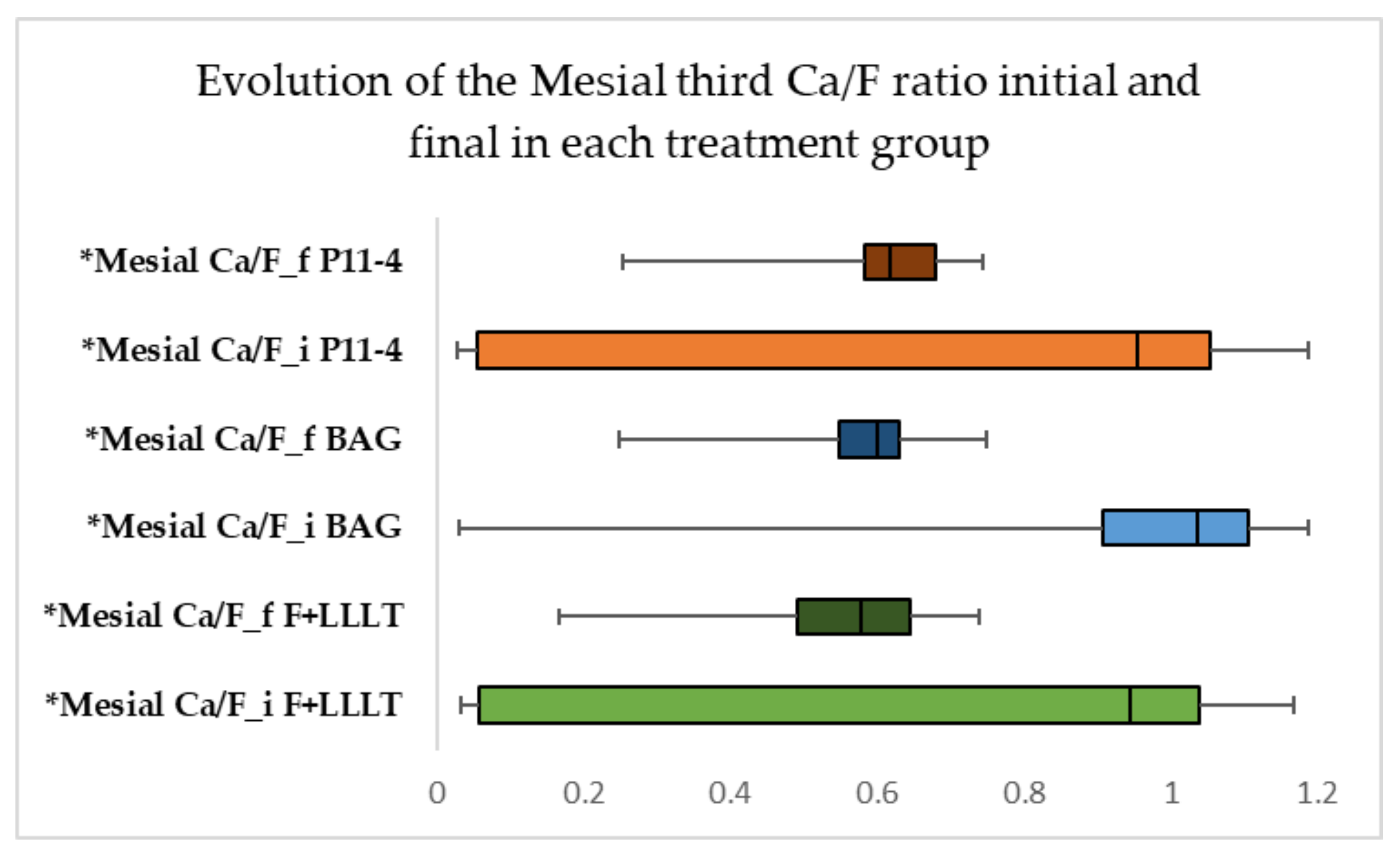
3.7. Evolution of Mesial Ca/P and Ca/F Ratio in Each Treatment Group
3.8. Evolution of Distal Ca/P and Ca/F Ratio in Each Treatment Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nanci, A. Ten Cate’s Oral Histology; Elsevier: Montreal, QC, Canada, 2017; pp. 289–307. [Google Scholar]
- Heidemann, D.; Hellwig, E.; Hickel, R.; Hugo, B.; Klaiber, B.; Klimek, J. Kariologie und Fullungstherapie; Urban und Schwarzenberg: Munchen, Germany, 1999; pp. 31–33. [Google Scholar]
- Chanachai, S.; Chaichana, W.; Insee, K.; Benjakul, S.; Aupaphong, V.; Panpisut, P. Physical/Mechanical and Antibacterial Properties of Orthodontic Adhesives Containing Calcium Phosphate and Nisin. J. Funct. Biomater. 2021, 12, 73. [Google Scholar] [CrossRef]
- Cosma, L.L.; Suhani, R.D.; Mesaros, A.; Badea, M.E. Current Treatment Modalities of Orthodontically Induced White Spot Lesions and Their Outcome. Med. Pharm. Rep. 2019, 92, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J. The Continuum of Dental Caries--Evidence for a Dynamic Disease Process. J. Dent. Res. 2004, 83, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.A.; Roberts, E.W.; Eckert, G.J.; Kula, K.S.; Gonzalez-Cabezas, C. Risk Factors for Incidence and Severity of White Spot Lesions during Treatment with Fixed Orthodontic Appliances. Am. J. Orthod. Dentofacial. Orthop. 2010, 138, 88–94. [Google Scholar] [CrossRef]
- Khoroushi, M.; Kachuie, M. Prevention and Treatment of White Spot Lesions in Orthodontic Patients. Contemp. Clin. Dent. 2017, 8, 11–19. [Google Scholar]
- Gorelick, L.; Geiger, A.; Gwinnett, A. Incidence of White Spot Formation after Bonding and Banding. Am. J. Orthod. 1982, 81, 93–98. [Google Scholar] [CrossRef]
- Ritter, A.; Eidson, R.; Donovan, T. Sturdevant’s Art and Science of Operative Dentistry; Elsevier: Saint Louis, MO, USA, 2018; pp. 40–94. [Google Scholar]
- Karabekiroglu, S.; Unlu, N.; Kucukyilmaze, E.; Sener, S.; Botsali, M.; Malkoc, S. Treatment of Post-Orthodontic White Spot Lesions with CPP-ACP Paste: A Three Year Follow up Study. Dent. Mater. J. 2017, 36, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Abbassy, M.; Bakry, A.; Almoabady, E.; Almusally, S.; Hassan, A. Characterization of a Novel Enamel Sealer for Bioactive Remineralization of White Spot Lesions. J. Dent. 2021, 109, 103663. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Davis, H.; Tufekci, E.; Crowe, J.; Covell, D.; Mitchell, J. Ion Release from a Novel Orthodontic Resin Bonding Agent for the Reduction and/or Prevention of White Spot Lesions. Angle Orthod. 2011, 81, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, V.; Bhatia, A.; Varma, H. Development, Characterization and Comparison of Two Strontium Doped Nano Hydroxyapatite Molecules for Enamel Repair/Regeneration. Dent. Mater. J. 2016, 32, 646–659. [Google Scholar] [CrossRef]
- Jablonski-Momeni, A.; Heinzel-Gutenbrunner, M. Efficacy of the Self-Assembling Peptide P11-4 in Constructing a Remineralization Scaffold on Artificially-Induced Enamel Lesions on Smooth Surfaces. J. Orofac. Orthop. 2014, 75, 175–190. [Google Scholar] [CrossRef] [PubMed]
- El-Wassefy, N. Remineralizing Effect of Cold Plasma and/or Bioglass on Demineralized Enamel. Dent. Mater. J. 2017, 36, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Coordes, S.; Brinkmann, P.; Prager, T.; Bartzela, T.; Visel, D.; Jacker, T.; Hartwich, R. A Comparison of Different Sealants Preventing Demineralization around Brackets. J. Orofac. Orthop. 2018, 79, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Meto, A.; Meto, A.; Tragaj, E.; Lipo, M.; Bauermann, C. The Use of Tiefenfluorid for Desensitization of Dentinal Hyperesthesia*. Balk. J. Dent. Med. 2014, 18, 85–88. [Google Scholar] [CrossRef]
- Ahrari, F.; Poosti, M.; Motahari, P. Enamel Resistance to Demineralization Following Er:YAG Laser Etching for Bonding Orthodontic Brackets. Dent. Res. J. 2012, 9, 472–477. [Google Scholar]
- Bishara, S.; Abadi, E. The Effect on the Bonding Strength of Orthodontic Brackets of Fluoride Application after Etching. Am. J. Orthod. Dentofacial. Orthop. 1989, 95, 259–260. [Google Scholar] [CrossRef]
- Ferraris, S.; Yamaguchi, S.; Barbani, N.; Cazzola, M.; Cristallini, C.; Miola, M.; Verne, E.; Spriano, S. Bioactive Materials: In Vitro Investigation of Different Mechanisms of Hydroxyapatite Precipitation. Acta Biomater. 2020, 102, 468–480. [Google Scholar] [CrossRef]
- Earl, J.; Leary, R.; Muller, K.; Langford, R.; Greenspan, D. Physical and Chemical Characterization of Dentin Surface Following Treatment with NovaMin Technology. J. Clin. Dent. 2011, 22, 62–67. [Google Scholar]
- Dai, L.; Mei, M.; Chu, C.; Lo, E. Mechanisms of Bioactive Glass on Caries Management: A Review. Materials 2019, 12, 4183. [Google Scholar] [CrossRef]
- Maude, S.; Tai, L.; Davies, R. Peptide Synthesis Andself-Assembly. Top. Curr. Chem. 2011, 310, 27–69. [Google Scholar]
- Benfenati, E.; Gini, G.; Luttik, R.; Hoffmann, S. Comparing In Vivo, In Vitro and In Silico Methods and Integrated Strategies for Chemical Assessment: Problems and Prospects. Altern. Lab. Anim. 2010, 38, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Jamari, I.; Ammarullah, M.; Santoso, G.; Sugiharto, S.; Supriyono, T.; van der Heide, E. In Silico Contact Pressure of Metal-on-Metal Total Hip Implant with Different Materials Subjected to Gait Loading. Metals 2022, 12, 1241. [Google Scholar] [CrossRef]
- Staley, R. Effect of Fluoride Varnish on Demineralization Around Orthodontic Brackets. Semin. Orthod. 2008, 14, 194–199. [Google Scholar] [CrossRef]
- Greene, L.; Bearn, D. Reducing White Spot Lesion Incidence during Fixed Appliance Therapy. Dent. Update 2013, 40, 487–490. [Google Scholar] [CrossRef]
- Iovan, G. Caria Dentară: Repere Etiologice Şi Patogenice; GR. T. Popa: Iasi, Romania, 2011; pp. 176–182. [Google Scholar]
- Featherstone, J. Dental Caries: A Dynamic Disease Process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef]
- Caixeta, R.; Berger, S.; Lopes, M.; Paloco, E.; Faria, E.; Contreras, E. Evaluation of Enamel Roughness after the Removal of Brackets Bonded with Different Materials: In Vivo Study. Braz. Dent. J. 2021, 32, 34–40. [Google Scholar] [CrossRef]
- Sindhura, V.; Uloopi, K.; Vinay, C.; Chandrasekhar, R. Evaluation of Enamel Remineralizing Potential of Self-Assembling Peptide P11-4 on Artificially Induced Enamel Lesions in Vitro. J. Indian Soc. Pedod. Prev. Dent. 2018, 36, 352–356. [Google Scholar] [CrossRef]
- Magalhaes, G.; Fraga, M.; Araujo, I.; Pachero, R.; Correr, A.; Puppin-Rontani, R. Effect of a Self-Assembly Peptide on Surface Roughness and Hardness of Bleached Enamel. J. Funct. Biomater. 2022, 13, 79. [Google Scholar] [CrossRef]
- Farooq, I.; Khan, A.; Moheet, I.; Alshwaimi, E. Preparation of a Toothpaste Containing Theobromine and Fluoridated Bioactive Glass and Its Effect on Surface Micro-Hardness and Roughness of Enamel. Dent. Mater. J. 2021, 40, 393–398. [Google Scholar] [CrossRef]
- Pribadi, N.; Citra, A.; Rukmo, M. The Difference in Enamel Surface Hardness after Immersion Process with Cocoa Rind Extract (Theobroma cacao) and Fluoride. J. Int. Oral Health 2019, 11, 100–103. [Google Scholar] [CrossRef]
- Taha, A.; Fleming, P.; Hill, R.; Patel, M. Enamel Remineralization with Novel Bioactive Glass Air Abrasion. J. Int. Oral Health 2018, 97, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Tranaeus, S.; Al-Khateeb, S.; Bjorkman, S.; Twetman, S.; Angmar-Mansson, B. Application of Quantitative Light-Induced Fluorescence to Monitor Incipient Lesions in Caries-Active Children. A Comparative Study of Remineralisation by Fluoride Varnish and Professional Cleaning. Eur. J. Oral Sci 2001, 109, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Joiner, A.; Hopkinson, I.; Deng, Y.; Westland, S. A Review of Tooth Colour and Whiteness. J. Dent. 2008, 36, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Son, H.; Yi, K.; Kim, H.; Ahn, J.; Chang, J. The Color Change in Artificial White Spot Lesions Measured Using a Spectroradiometer. Clin. Oral Investig. 2013, 17, 139–146. [Google Scholar] [CrossRef]
- Torres, C.; Borges, A.; Torres, L.; Gomes, I.; de Oliveira, R.S. Effect of Caries Infiltration Technique and Fluoride Therapy on the Colour Masking of White Spot Lesions. J. Dent. 2011, 39, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Yetkiner, E.; Wegehaupt, F.; Wiegand, A.; Attin, R.; Attin, T. Colour Improvement and Stability of White Spot Lesions Following Infiltration, Micro-Abrasion, or Fluoride Treatments in Vitro. Eur. J. Orthod. 2014, 36, 595–602. [Google Scholar] [CrossRef]
- Mohamed, A.; Wong, K.; Lee, W.; Marizan Nor, M.; Mohd Hussaini, H.; Rosli, T. In Vitro Study of White Spot Lesion: Maxilla and Mandibular Teeth. Saudi Dent. J. 2018, 30, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Iwami, Y.; Hayashi, N.; Takeshige, F.; Ebisu, S. Relationship between the Color of Carious Dentin with Varying Lesion Activity, and Bacterial Detection. J. Dent. 2008, 36, 143–151. [Google Scholar] [CrossRef]
- Chin, M.Y.; Sandham, A.; Rumachik, E.; Ruben, J.; Huysmans, M.C. Fluoride Release and Cariostatic Potential of Orthodontic Adhesives with and without Daily Fluoride Rinsing. Am. J. Orthod. Dentofacial. Orthop. 2009, 136, 547–553. [Google Scholar] [CrossRef]
- Paris, S.; Schwendicke, F.; Keltsch, J.; Dorfer, C.; Meyer-Lueckel, H. Masking of White Spot Lesions by Resin Infiltration In Vitro. J. Dent. 2013, 41, 28–34. [Google Scholar] [CrossRef]
- Gomez-Polo, C.; Montero, J.; Gomez-Polo, M.; de Parga, J.; Celemin-Vinuels, A. Natural Tooth Color Estimation Based on Age and Gender. J. Prosthodont. 2017, 26, 107–114. [Google Scholar] [CrossRef] [PubMed]
- West, N.; Joiner, A. Enamel Mineral Loss. J. Dent. 2014, 42, 2–11. [Google Scholar] [CrossRef]
- Robinson, C.; Shore, R.; Brookes, S.; Strafford, S.; Wood, S.; Kirkham, J. The Chemistry of Enamel Caries. Crit. Rev. Oral Biol. Med. 2000, 11, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J. Prevention and Reversal of Dental Caries: Role of Low Level Fluoride. Community Dent. Oral Epidemiol. 1999, 27, 31–40. [Google Scholar] [CrossRef]
- Robinson, C. Fluoride and the Caries Lesion: Interactions and Mechanism of Action. Eur. Arch. Paediatr. Dent. 2009, 10, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.; Goodman, P.; Mclean, J. Electron Microscope Study of Defect Zones in Dental Enamel. J. Ultrastruct. Res. 1979, 67, 117–123. [Google Scholar] [CrossRef]
- Beerens, M.; Van Der Veen, M.; Van Beek, H.; Ten Cate, J. Effects of Casein Phosphopeptide Amorphous Calcium Fluoride Phosphate Paste on White Spot Lesions and Dental Plaque after Orthodontic Treatment: A 3-Month Follow-Up. Eur. J. Oral Sci. 2010, 118, 610–617. [Google Scholar] [CrossRef]
- Marinho, V.; Higgins, J.; Logan, S.; Sheiham, A. Topical Fluoride (Toothpastes, Mouthrinses, Gels or Varnishes) for Preventing Dental Caries in Children and Adolescents. Cochrane Database Syst. Rev. 2003, 4, CD002782. [Google Scholar] [CrossRef]
- Derks, A.; Katsaros, C.; Frencken, J.; Van’t Hof, M.; Kuijpers-Jagtman, A. Caries-Inhibiting Effect of Preventive Measures during Orthodontic Treatment with Fixed Appliances: A Systematic Review. Caries Res. 2004, 38, 413–420. [Google Scholar] [CrossRef]
- Cochrane, N.; Cai, F.; Huq, N.; Burrow, M.; Reynolds, E. New Approaches to Enhanced Remineralization of Tooth Enamel. J. Dent. Res. 2010, 89, 1187–1197. [Google Scholar] [CrossRef]
- Arends, J.; Davidson, C. HPO2-4 Content in Enamel and Artificial Carious Lesions. Calcif Tissue Res. 1975, 18, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Ingram, G.; Nash, P. A Mechanism for the Anticaries Action of Fluoride. Caries Res. 1980, 14, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Tomazic, B.; Tomson, M.; Nancollas, G. Growth of Calcium Phosphates on Hydroxyapatite Crystals: The Effect of Magnesium. Arch. Oral Biol. 1975, 20, 803–808. [Google Scholar] [CrossRef]
- Akkus, A.; Akkus, O.; Roperto, R.; Lang, L. Investigation of Intra- and Inter-Individual Variations of Mineralisation in Healthy Permanent Human Enamel by Raman Spectroscopy. Oral Health Prev. Dent. 2016, 14, 321–327. [Google Scholar]
- Yeni, Y.; Yerramshetty, J.; Akkus, O.; Pechey, C.; Les, C. Effect of Fixation and Embedding on Raman Spectroscopic Analysis of Bone Tissue. Calcif Tissue Res. 2006, 78, 363–371. [Google Scholar] [CrossRef]













Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voina Cosma, L.L.; Moldovan, M.; Muntean, A.; Olteanu, C.D.; Chifor, R.; Badea, M.E. Novel Technology for Enamel Remineralization in Artificially Induced White Spot Lesions: In Vitro Study. Coatings 2022, 12, 1285. https://doi.org/10.3390/coatings12091285
Voina Cosma LL, Moldovan M, Muntean A, Olteanu CD, Chifor R, Badea ME. Novel Technology for Enamel Remineralization in Artificially Induced White Spot Lesions: In Vitro Study. Coatings. 2022; 12(9):1285. https://doi.org/10.3390/coatings12091285
Chicago/Turabian StyleVoina Cosma, Lavinia Luminita, Marioara Moldovan, Alexandrina Muntean, Cristian Doru Olteanu, Radu Chifor, and Mindra Eugenia Badea. 2022. "Novel Technology for Enamel Remineralization in Artificially Induced White Spot Lesions: In Vitro Study" Coatings 12, no. 9: 1285. https://doi.org/10.3390/coatings12091285