
Dental Ceramics: Fabrication Methods and Aesthetic Characterization

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
Source Selection
3. Results
4. Literature Review and Discussion
4.1. Ceramic Restorations
4.2. Ceramic Restorations Thickness
4.3. Monolithic Restorations
4.4. Aesthetic Characterization of the Ceramic Surface
4.5. Analysis of the Roughness and Hardness Properties of Ceramic Materials
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hara, M.; Takuma, Y.; Sato, T.; Koyama, T.; Yoshinari, M. Wear performance of bovine tooth enamel against translucent tetragonal zirconia polycrystals after different surface treatments. Dent. Mater. J. 2014, 33, 811–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potiket, N.; Chiche, G.; Finger, I.M. In vitro fracture strength of teeth was restored with different all-ceramic crown systems. J. Prosthet. Dent. 2004, 92, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Campos, T.M.; Ramos, N.C.; Machado, J.P.; Bottino, M.A.; Souza, R.O.; Melo, R.M. A new silica-infiltrated Y-TZP was obtained by the sol-gel method. J. Dent. 2016, 48, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matos, J.D.M.; Nakano, L.J.N.; Bottino, M.A.; Jesus, R.H.; Maciel, L.C. Current considerations for dental ceramics and their respective union systems. Rev. Bras. Odontol. 2020, 77, 1768. [Google Scholar] [CrossRef]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.; Bonfante, E.A. A new classification system for all-ceramic and ceramic-like restorative materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef] [Green Version]
- Amaral, M.; Villefort, R.F.; Melo, R.M.; Pereira, G.K.R.; Zhang, Y.; Valandro, L.F.; Bottino, M.A. Fatigue limit of monolithic Y-TZP three-unit-fixed dental prostheses: Effect of grinding at the gingival zone of the connector. J. Mech. Behav. Biomed. Mater. 2014, 72, 159–162. [Google Scholar] [CrossRef] [Green Version]
- Souza, R.; Barbosa, F.; Araújo, G.; Miyashita, E.; Bottino, M.A.; Melo, R.; Zhang, Y. Ultrathin Monolithic Zirconia Veneers: Reality or Future? Report of a Clinical Case and One-year Follow-up. Oper. Dent. 2018, 43, 3–11. [Google Scholar] [CrossRef]
- Zhang, Y.; Kelly, J.R. Dental Ceramics for Restoration and Metal Veneering. Dent. Clin. N. Am. 2017, 61, 797–819. [Google Scholar] [CrossRef]
- Bai, Y.; Zhao, J.; Si, W.; Wang, X. Two-body wear performance of dental colored zirconia after different surface treatments. J. Prosthet. Dent. 2016, 116, 584–590. [Google Scholar] [CrossRef]
- Barizon, K.T.; Bergeron, C.; Vargas, M.A.; Qian, F.; Cobb, D.S.; Gratton, D.G.; Geraldeli, S. Ceramic materials for porcelain veneers: Part II. Effect of material, shade, and thickness on translucency. J. Prosthet. Dent. 2014, 112, 864–870. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Dozic, A.; Liem, J.K. Influence of framework color and layering technique on the final color of zirconia veneered restorations. Quintessence Int. 2010, 41, 84–89. [Google Scholar]
- Catelan, A.; Guedes, A.P.; Suzuki, T.Y.; Takahashi, M.K.; Souza, E.M.; Briso, A.L.; Santos, P.H. Fluorescence intensity of composite layering combined with surface sealant submitted to staining solutions. J. Esthet. Restor. Dent. 2015, 27, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Anil, N.; Bolay, S. Effect of toothbrushing on the material loss, roughness, and color of intrinsically and extrinsically stained porcelain used in metal-ceramic restorations: An in vitro study. Int. J. Prosthodont. 2002, 15, 483–487. [Google Scholar] [PubMed]
- Koutayas, S.O.; Kakaboura, A.; Hussein, A.; Strub, J.R. Colorimetric evaluation of the influence of five different restorative materials on the color of veneered densely sintered alumina. J. Esthet. Restor. Dent. 2003, 15, 353–360. [Google Scholar] [CrossRef]
- O’Keefe, K.L.; Powers, J.M.; Noie, F. Effect of dissolution on color of extrinsic porcelain colorants. Int. J. Prosthodont. 1993, 6, 558–563. [Google Scholar]
- Aker, D.A.; Aker, J.R.; Sorensen, S.E. Toothbrush abrasion of color-corrective porcelain stains applied to porcelain-fused-to-metal restorations. J. Prosthet. Dent. 1980, 44, 161–163. [Google Scholar] [CrossRef]
- Bativala, F.; Weiner, S.; Berendsen, P.; Vincent, G.R.; Ianzano, J.; Harris, W.T., Jr. The microscopic appearance and effect of toothbrushing on extrinsically stained metal-ceramic restorations. J. Prosthet. Dent. 1987, 57, 47–52. [Google Scholar] [CrossRef]
- Garza, L.A.; Thompson, G.; Cho, S.H.; Berzins, D.W. Effect of toothbrushing on shade and surface roughness of extrinsically stained pressable ceramics. J. Prosthet. Dent. 2016, 115, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.C.; Barão, V.A.R.; Wee, A.G.; Alfaro, M.F.; Afshari, F.S.; Sukotjo, C. Effect of brushing and thermocycling on the shade and surface roughness of CAD-CAM ceramic restorations. J. Prosthet. Dent. 2018, 119, 1000–1006. [Google Scholar] [CrossRef]
- Kelly, J.R.; Benetti, P. Ceramic materials in dentistry: Historical evolution and current practice. Aust. Dent. J. 2011, 56 (Suppl. S1), 84–96. [Google Scholar] [CrossRef]
- Aurélio, I.L.; Dorneles, L.S.; May, L.G. Extended glaze firing on ceramics for hard machining: Crack healing, residual stresses, optical and microstructural aspects. Dent. Mater. 2017, 33, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Aurélio, I.L.; Fraga, S.; Dorneles, L.S.; Bottino, M.A.; May, L.G. Extended glaze firing improves flexural strength of a glass ceramic. Dent. Mater. 2015, 31, 316–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tribst, J.P.M.; Dal Piva, A.M.O.; Werner, A.; Anami, L.C.; Bottino, M.A.; Kleverlaan, J.C. Durability of staining and glazing on a hybrid ceramics after the three-body wear. J. Mech. Behav. Biomed. Mater. 2020, 103, 103856. [Google Scholar] [CrossRef]
- Dal Piva, A.M.O.; Tribst, J.P.M.; Werner, A.; Anami, L.C.; Bottino, M.A.; Kleverlaan, J.C. Three-body wear effect on different CAD/CAM ceramics staining durability. J. Mech. Behav. Biomed. Mater. 2019, 103, 103579. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K.J.; Shen, C.; Rawls, H.R. Phillips Materiais Dentários; Elsevier: Rio de Janeiro, Brazil, 2013. [Google Scholar]
- Gomes, E.A.; Assuncao, W.G.; Rocha, E.P.; Santos, P.H. Cerâmicas odontológicas: O estado atual. Rev. Cerâmica 2008, 54, 319–325. [Google Scholar] [CrossRef] [Green Version]
- Bottino, M.A.; Faria, R.; Valandro, L.F. Percepção: Estética em Próteses Livres de Metal em Dentes Naturais e Implantes; Artes Médicas: São Paulo, Brazi, 2009. [Google Scholar]
- Amoroso, A.P.; Ferreira, M.B.; Torcato, L.B.; Pellizzer, E.P.; Mazaro, J.V.Q.; Gennari, H.F. Cerâmicas odontológicas: Propriedades, indicações e considerações clínicas. Rev. Odontológica Araçatuba 2012, 33, 19–25. [Google Scholar]
- Della Bona, A.; Anusavice, K.J. Microstructure, composition, and etching topography of dental ceramics. Int. J. Prosthodont. 2002, 15, 159–167. [Google Scholar]
- Della Bona, A.; Corazza, P.H.; Zhang, Y. Characterization of a polymer-infiltrated ceramic-network material. Dent. Mater. 2014, 30, 564–569. [Google Scholar] [CrossRef] [Green Version]
- Vita Akzent® Plus. In Working Instructions for External Characterization Independent Stains for Finishing, Coloring and Glazing; Available as a Powder, Paste and Spray; Vita Zahnfabrik: Bad Säckingen, Germany, 2017.
- Figueiredo-Pina, C.G.; Patas, N.; Canhoto, J.; Cláudio, R.; Olhero, S.M.; Serro, A.P.; Ferro, A.C.; Guedes, M. Tribological behaviour of unveneered and veneered lithium disilicate dental material. J. Mech. Behav. Biomed. Mater. 2016, 53, 226–238. [Google Scholar] [CrossRef]
- Campos, T.M.B.; Ramos, N.C.; Matos, J.D.M.; Thim, G.P.; Souza, R.O.A.; Bottino, M.A.; Valandro, L.F.; Melo, R.M. Silica infiltration in partially stabilized zirconia: Effect of hydrothermal aging on mechanical properties. J. Mech. Behav. Biomed. Mater. 2020, 109, 103774. [Google Scholar] [CrossRef]
- Wang, R.J.; Liu, M.; Song, D.Y.; Yang, S.; Wang, Q.; Wang, L.; Feng, H.L. Analysis of edge morphology of partial veneers made by different processing techniques and materials. Beijing Da Xue Xue Bao Yi Xue Ban 2019, 51, 93–99. [Google Scholar]
- Lin, W.S.; Ercoli, C.; Feng, C.; Morton, D. The effect of core material, veneering porcelain, and fabrication technique on the biaxial flexural strength and weibull analysis of selected dental ceramics. J. Prosthodont. 2012, 21, 353–362. [Google Scholar] [CrossRef]
- Cho, S.H.; Nagy, W.W.; Goodman, J.T.; Solomon, E.; Koike, M. The effect of multiple firings on the marginal integrity of pressable ceramic single crowns. J. Prosthet. Dent. 2012, 107, 17–23. [Google Scholar] [CrossRef]
- Subaş, M.G.; Demir, N.; Kara, Ö.; Ozturk, A.N.; Özel, F. Mechanical properties of zirconia after different surface treatments and repeated firings. J. Adv. Prosthodont. 2014, 6, 462–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vita Enamic® Stains Kit Vita. In Working Instructions for External Characterization Independent Stains for Finishing, Coloring and Glazing; Available as a powder, liquid, paste and glaze; Vita Zahnfabrik: Bad Säckingen, Germany, 2018.
- Biscaro, L.; Bonfiglioli, R.; Soattin, M.; Vigolo, P. An in vivo evaluation of fit of zirconium-oxide based ceramic single crowns, generated with two CAD/CAM systems, in comparison to metal ceramic single crowns. J. Prosthodont. 2013, 22, 36–41. [Google Scholar] [CrossRef]
- Fischer, J.; Stawarczyk, B.; Hämmerle, C.H. Flexural strength of veneering ceramics for zirconia. J. Dent. 2008, 36, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Corazza, P.H.; Cavalcanti, S.C.; Queiroz, J.R.; Bottino, M.A.; Valandro, L.F. Effect of post-silanization heat treatments of silanized feldspathic ceramic on adhesion to resin cement. J. Adhes Dent. 2013, 15, 473–479. [Google Scholar]
- Pereira, G.K.R.; Guilardi, L.F.; Dapieve, K.S.; Kleverlaan, C.J.; Rippe, M.P.; Valandro, L.F. Mechanical reliability, fatigue strength and survival analysis of new polycrystalline translucent zirconia ceramics for monolithic restorations. J. Mech. Behav. Biomed. Mater. 2018, 85, 57–65. [Google Scholar] [CrossRef]
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25. [Google Scholar] [CrossRef]
- Chevalier, J.; Gremillard, L.; Virkar, A.V.; Clarke, D.R. The tetragonal-monoclinic transformation in zirconia: Lessons learned and future trends. J. Am. Ceram. Soc. 2009, 92, 1901–1920. [Google Scholar] [CrossRef]
- Merli, M.; Bianchini, E.; Mariotti, G.; Moscatelli, M.; Piemontese, M.; Rappelli, G.; Nieri, M. Ceramic vs composite veneering of full arch implant-supported zirconium frameworks: Assessing patient preference and satisfaction. A crossover double-blind randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 311–322. [Google Scholar] [PubMed]
- Condon, J.R.; Ferracane, J.L. In vitro wear of composite with varied cure, filler level, and filler treatment. J. Dent. Res. 1997, 76, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.; Llukacej, A.; Baldissara, P.; Arena, A.; Scotti, R. Zirconia-based versus metal-based single crowns veneered with overpressing ceramic for restoration of posterior endodontically treated teeth: 5-year results of a randomized controlled clinical study. J. Dent. 2017, 65, 56–63. [Google Scholar] [CrossRef]
- Kaán, B.; Eichner, K.; Kaán, M.; Fejérdy, P.; Róth, L. In vivo and in vitro study of the marginal sealing in ceramic-covered gold inlays. Fogorv. Szle. 1998, 91, 363–373. [Google Scholar]
- Chun, E.P.; Anami, L.C.; Bonfante, E.A.; Bottino, M.A. Microstructural analysis and reliability of monolithic zirconia after simulated adjustment protocols. Dent. Mater. 2017, 33, 934–943. [Google Scholar] [CrossRef] [Green Version]
- Zhao, K.; Wei, Y.R.; Pan, Y.; Zhang, X.P.; Swain, M.V.; Guess, P.C. Influence of veneer and cyclic loading on failure behavior of lithium disilicate glass-ceramic molar crowns. Dent. Mater. 2014, 30, 164–171. [Google Scholar] [CrossRef]
- Kimmich, M.; Stappert, C.F. Intraoral treatment of veneering porcelain chipping of fixed dental restorations: A review and clinical application. J. Am. Dent. Assoc. 2013, 144, 31–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rauch, A.; Reich, S.; Schierz, O. Chair-side generated posterior monolithic lithium disilicate crowns: Clinical survival after 6 years. Clin. Oral Investig. 2017, 21, 2083–2089. [Google Scholar] [CrossRef]
- Joda, T.; Ferrari, M.; Brägger, U. Monolithic implant-supported lithium disilicate (LS2) crowns in a complete digital workflow: A prospective clinical trial with a 2-year follow-up. Clin. Implant Dent. Relat. Res. 2017, 19, 505–511. [Google Scholar] [CrossRef]
- Turp, V.; Turkoglu, P.; Sen, D. Influence of monolithic lithium disilicate and zirconia thickness on polymerization efficiency of dual-cure resin cements. J. Esthet. Restor. Dent. 2018, 30, 360–368. [Google Scholar] [CrossRef]
- Martins, F.V.; Vasques, W.F.; Fonseca, E.M. How the Variations of the Thickness in Ceramic Restorations of Lithium Disilicate and the Use of Different Photopolymerizers Influence the Degree of Conversion of the Resin Cements: A Systematic Review and Meta-Analysis. J. Prosthodont. 2019, 28, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, J.B.; Riquieri, H.; Prochnow, C.; Guilardi, L.F.; Pereira, G.K.R.; Borges, A.L.S.; Melo, R.M.; Valandro, L.F. Fatigue failure load of two resin-bonded zirconia-reinforced lithium silicate glass-ceramics: Effect of ceramic thickness. Dent. Mater. 2018, 34, 891–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wendler, M.; Belli, R.; Lohbauer, U. Factors influencing development of residual stresses during crystallization firing in a novel lithium silicate glass-ceramic. Dent. Mater. 2019, 35, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Arif, R.; Yilmaz, B.; Johnston, W.M. In vitro color stainability and relative translucency of CAD-CAM restorative materials used for laminate veneers and complete crowns. J. Prosthet. Dent. 2019, 122, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Kashkari, A.; Yilmaz, B.; Brantley, W.A.; Schricker, S.R.; Johnston, W.M. Fracture analysis of monolithic CAD-CAM crowns. J. Esthet. Restor. Dent. 2019, 31, 346–352. [Google Scholar] [CrossRef]
- Tabatabaian, F. Color Aspect of Monolithic Zirconia Restorations: A Review of the Literature. J. Prosthodont. 2019, 28, 276–287. [Google Scholar] [CrossRef]
- Turgut, S.; Kılınç, H.; Bağış, B. Effect of UV aging on translucency of currently used esthetic CAD-CAM materials. J. Esthet. Restor. Dent. 2019, 31, 147–152. [Google Scholar] [CrossRef]
- Monteiro, J.B.; Oliani, M.G.; Guilardi, L.F.; Prochnow, C.; Rocha Pereira, G.K.; Bottino, M.A.; Melo, R.M.; Valandro, L.F. Fatigue failure load of zirconia-reinforced lithium silicate glass ceramic cemented to a dentin analogue: Effect of etching time and hydrofluoric acid concentration. J. Mech. Behav. Biomed. Mater. 2018, 77, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Riccitiello, F.; Amato, M.; Leone, R.; Spagnuolo, G.; Sorrentino, R. In vitro Evaluation of the Marginal Fit and Internal Adaptation of Zirconia and Lithium Disilicate Single Crowns: Micro-CT Comparison between Different Manufacturing Procedures. Open Dent. J. 2018, 22, 160–172. [Google Scholar] [CrossRef]
- Nishioka, G.; Prochnow, C.; Firmino, A.; Amaral, M.; Bottino, M.A.; Valandro, L.F.; Melo, R.M. Fatigue strength of several dental ceramics indicated for CAD-CAM monolithic restorations. Braz. Oral Res. 2018, 11, 53. [Google Scholar] [CrossRef]
- Lohbauer, U.; Scherrer, S.S.; Della Bona, A.; Tholey, M.; Van Noort, R.; Vichi, A.; Kelly, J.R.; Cesar, P.F. ADM guidance-Ceramics: All-ceramic multilayer interfaces in dentistry. Dent. Mater. 2017, 33, 585–598. [Google Scholar] [CrossRef]
- Rinke, S.; Rödiger, M.; Ziebolz, D.; Schmidt, A.K. Fabrication of Zirconia-Reinforced Lithium Silicate Ceramic Restorations Using a Complete Digital Workflow. Case Rep. Dent. 2015, 2015, 162178. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.; Koller, C.; Mehl, A.; Hickel, R. Indirect zirconia-reinforced lithium silicate ceramic CAD/CAM restorations: Preliminary clinical results after 12 months. Quintessence Int. 2017, 48, 19–25. [Google Scholar]
- Aboushelib, M.N. Fatigue and fracture resistance of zirconia crowns prepared with different finish line designs. J. Prosthodont. 2012, 21, 22–27. [Google Scholar] [CrossRef]
- Pradies, G.; Zarauz, C.; Valverde, A.; Ferreiroa, A.; Martinez-Rus, F. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions based on wavefront sampling technology. J. Dent. 2015, 43, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Baroudi, K.; Ibraheem, S.N. Assessment of chair-side computer-aided design and computer-aided manufacturing restorations: A review of the literature. J. Int. Oral Health 2015, 7, 96–104. [Google Scholar]
- Aboushelib, M.N.; Elmahy, W.A.; Ghazy, M.H. Internal adaptation, marginal accuracy, and microleakage of pressable versus machinable ceramic laminate veneers. J. Dent. 2012, 40, 670–677. [Google Scholar] [CrossRef]
- Berrendero, S.; Salido, M.P.; Valverde, A.; Ferreiroa, A.; Pradies, G. Influence of conventional and digital intraoral impressions on the fit of CAD/CAM-fabricated all-ceramic crowns. Clin. Oral Investig. 2016, 20, 2403–2410. [Google Scholar] [CrossRef]
- Zandinejad, A.; Lin, W.S.; Atarodi, M.; Abdel-Azim, T.; Metz, M.J.; Morton, D. Digital workflow for virtually designing and milling ceramic lithium disilicate veneers: A clinical report. Oper. Dent. 2015, 40, 241–246. [Google Scholar] [CrossRef]
- Zarauz, C.; Valverde, A.; Martinez-Rus, F.; Hassan, B.; Pradies, G. Clinical evaluation comparing the fit of all-ceramic crowns obtained from silicone and digital intraoral impressions. Clin. Oral Investig. 2016, 20, 799–806. [Google Scholar] [CrossRef]
- Habib, A.W.; Aboushelib, M.N.; Habib, N.A. Effect of chemical aging on color stability and surface properties of stained all-ceramic restorations. J. Esthet. Restor. Dent. 2021, 33, 636–647. [Google Scholar] [CrossRef]
- Lee, W.F.; Iwasaki, N.; Peng, P.W.; Takahashi, H. Effect of toothbrushing on the optical properties and surface roughness of extrinsically stained high-translucency zirconia. Clin. Oral Investig. 2022, 26, 3041–3048. [Google Scholar] [CrossRef]
- Sulaiman, T.A.; Camino, R.N.; Cook, R.; Delgado, A.J.; Roulet, J.F.; Clark, W.A. Time-lasting ceramic stains and glaze: A toothbrush simulation study. J. Esthet. Restor. Dent. 2020, 32, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Barcellos, A.S.P.; Miranda, J.S.; Amaral, M.; Alvarenga, J.A.; Nogueira, L.; Kimpara, E.J. Effect of staining on the mechanical, surface and biological properties of lithium disilicate. Saudi Dent. J. 2022, 34, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.C.; Lin, W.C.; Lin, Y.L.; Yan, M.; Tang, C.M. In Vitro Evaluation of the Shading Effect of Various Zirconia Surface Stains on Porcelain Crowns. Coatings 2022, 12, 734. [Google Scholar] [CrossRef]
- Chi, W.J.; Browning, W.; Looney, S.; Mackert, J.R.; Windhorn, R.J.; Rueggeberg, F. Resistance to abrasion of extrinsic porcelain esthetic characterization techniques. US Army Med. Dep. J. 2017, 17, 71–79. [Google Scholar]
- Elsaka, S.E.; Elnaghy, A.M. Mechanical properties of zirconia reinforced lithium silicate glass-ceramic. Dent. Mater. 2016, 32, 908–914. [Google Scholar] [CrossRef]
- Kaizer, M.R.; Moraes, R.R.; Cava, S.S.; Zhang, Y. The progressive wear and abrasiveness of novel graded glass/zirconia materials relative to their dental ceramic counterparts. Dent. Mater. 2019, 35, 763–771. [Google Scholar] [CrossRef]
- Sakaguchi, R.L.; Douglas, W.H.; DeLong, R.; Pintado, M.R. The wear of a posterior composite in an artificial mouth: A clinical correlation. Dent. Mater. 1986, 2, 235–240. [Google Scholar] [CrossRef]
- Contreras, L.; Dal Piva, A.; Ribeiro, F.C.; Anami, L.C.; Camargo, S.; Jorge, A.; Bottino, M.A. Effects of manufacturing and finishing techniques of feldspathic ceramics on surface topography, biofilm formation, and cell viability for human gingival fibroblasts. Oper. Dent. 2018, 43, 593–601. [Google Scholar] [CrossRef]
- Poticny, D. Simplified ceramic restorations using CAD/CAM technologies. Pract. Proced. Aesthetic Dent. 2004, 16, 353–358. [Google Scholar]
- Wennerberg, A.; Albrektsson, T. Suggested guidelines for the topographic evaluation of implant surfaces. Int. J. Oral Maxillofac. Implant. 2000, 15, 331–344. [Google Scholar]
- Gadelmawla, E.S.; Koura, M.M.; Maksoud, T.M.A.; Elewa, I.M.; Soliman, H.H. Roughness parameters. J. Mater. Proc. Technol. 2002, 123, 133–145. [Google Scholar] [CrossRef]
- Vichi, A.; Fonzar, R.F.; Goracci, C.; Carrabba, M.; Ferrari, M. Effect of Finishing and Polishing on Roughness and Gloss of Lithium Disilicate and Lithium Silicate Zirconia Reinforced Glass-Ceramic for CAD/CAM Systems. Oper. Dent. 2018, 43, 90–100. [Google Scholar] [CrossRef]
- Oh, W.S.; Delong, R.; Anusavice, K.J. Factors affecting enamel and ceramic wear: A literature review. J. Prosthet. Dent. 2002, 87, 451–459. [Google Scholar] [CrossRef]
- Carvalho, I.F.A.; Santos Marques, T.M.S.; Araújo, F.M.; Azevedo, L.F.; Donato, H.; Correia, A. Clinical Performance of CAD/CAM Tooth-Supported Ceramic Restorations: A Systematic Review. Int. J. Periodontics Restor. Dent. 2018, 38, e68–e78. [Google Scholar] [CrossRef]
- Saravi, B.; Vollmer, A.; Hartmann, M.; Lang, G.; Kohal, R.J.; Boeker, M.; Patzelt, S.B.M. Clinical Performance of CAD/CAM All-Ceramic Tooth-Supported Fixed Dental Prostheses: A Systematic Review and Meta-Analysis. Materials 2021, 14, 2672. [Google Scholar] [CrossRef]
- Riquieri, H.; Monteiro, J.B.; Viegas, D.C.; Campos, T.M.B.; de Melo, R.M.; Saavedra, G.S.F.A. Impact of crystallization firing process on the microstructure and flexural strength of zirconia-reinforced lithium silicate glass-ceramics. Dent. Mater. 2018, 34, 1483–1491. [Google Scholar] [CrossRef] [Green Version]
- Romão, R.M.; Lopes, G.R.S.; Matos, J.D.M.; Lopes, G.R.S.; Vasconcelos, J.E.L.; Fontes, N.M. Causes of failures in ceramic veneers restorations: A literature review. Int. J. Adv. Res. 2018, 6, 896–906. [Google Scholar] [CrossRef] [Green Version]
- Peixoto, N.M.; Matos, J.D.M.; Andrade, V.C.; Bottino, M.A.; Zogheib, L.V. Evaluación de la resistenciade unión de brackets ortodónticos fijados a cerámica de disilicato de litio. Int. J. Odontostomatol. 2019, 13, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Pereira, S.M.; Kantorski, K.Z.; Brentel, A.S.; Valandro, L.F.; Bottino, M.A. SEM analysis of the in situ early bacterial colonization on two novel feldspathic ceramics submitted to different types of glazing. J. Contemp. Dent. Pract. 2008, 9, 49–56. [Google Scholar] [PubMed] [Green Version]
- Jiang, Y.; Akkus, A.; Roberto, R.; Akkus, O.; Li, B.; Lang, L.; Teich, S. Measurement of J-integral in CAD/CAM dental ceramics and composite resin by digital image correlation. J. Mech. Behav. Biomed. Mater. 2016, 62, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Rizkalla, A.S.; Jones, D.W. Indentation fracture toughness and dynamic elastic moduli for commercial feldspathic dental porcelain materials. Dent. Mater. 2004, 20, 198–206. [Google Scholar] [CrossRef]
- Farzin, M.; Ansarifard, E.; Taghva, M.; Imanpour, R. Effect of external staining on the optical properties and surface roughness of monolithic zirconia of different thicknesses. J. Prosthet. Dent. 2021, 126, 687.e1–687.e8. [Google Scholar] [CrossRef]
- Ural, C.; Burgaz, Y.; Saraç, D. In vitro evaluation of marginal adaptation in five ceramic restoration fabricating techniques. Quintessence Int. 2010, 41, 585–590. [Google Scholar]
- Andrade, G.S.; Diniz, V.; Datte, C.E.; Pereira, G.K.R.; Venturini, A.B.; Campos, T.M.B.; Amaral, M.; Bottino, M.A.; Valandro, L.F.; Melo, R.M. Newer vs. older CAD/CAM burs: Influence of bur experience on the fatigue behavior of adhesively cemented simplified lithium-disilicate glass-ceramic restorations. J. Mech. Behav. Biomed. Mater. 2019, 95, 172–179. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
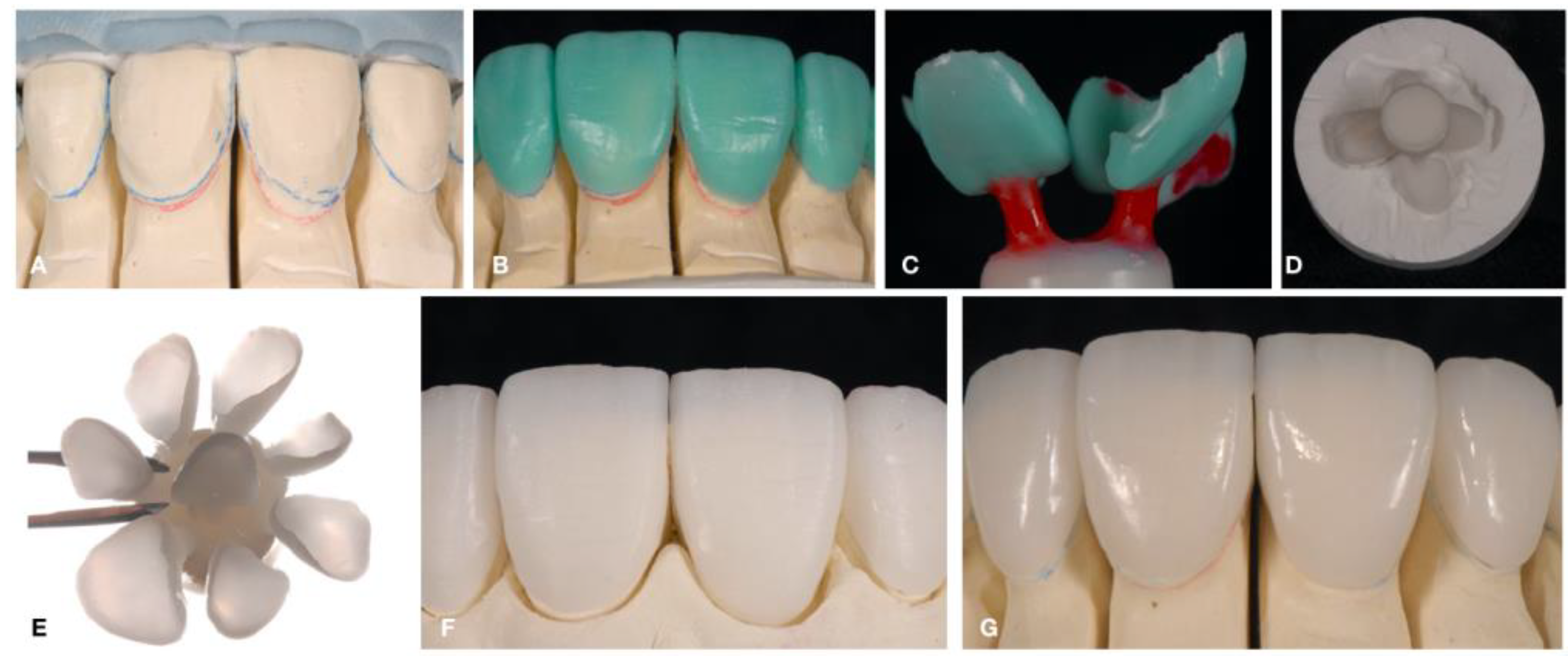
| Layering and/or Staining | (1st) Making a suspension (Paste): Union of porcelain powder + distilled water mixed with rheological modifiers and/or manufacturer’s specific diluent = Formation of viscous suspension, in which the indirect restoration of the ceramic can be built. (2nd) The restoration is made by mixing the porcelain powder with the styling liquid until a paste is formed and applied with a brush on the refractory die. This application is done in layers, to conform to the anatomical shape of the tooth. Another reason for applying several layers is the use of different porcelain colors, to allow greater reproduction of details of both dentin and enamel. The addition of metallic oxides (Al, Ca, Li, Mg, K, Na, Zr, Ti, among others) in dental ceramics will determine its final color, resulting from the firing of the material at high temperatures. For each layer applied, it is necessary to condense the paste by removing excess water. This can be done by vibrating with subsequent application of an absorbent paper or through specific dental vibrators for this processing. After completing the characterization steps, the restoration must be taken to a specific oven for dental ceramics, where the firing will be carried out. This process acts directly on the union of the dust particles, increasing the density of the mass by reducing porosities [23,24,25,31,38]. (3rd) Initially there is a preheating (drying) of the condensed porcelain mass at temperatures of approximately 400–500 °C for 5 min in the door of the preheated oven. This step ensures that the water slowly evaporates without causing damage to the mass. In the next step, once inside the oven, the restoration is heated to a maximum firing temperature of approximately 700–980 °C for 1 min at a speed of 40 to 90 °C/min. During this process, a vacuum pump is activated and guarantees a low-pressure vacuum (0.1 atm) inside the oven. When the maximum cycle temperature is reached, the pump is turned off and the external air (with a pressure of 1 atm) enters the oven again, increasing the pressure inside the muffle by 10 times. Thus, sintering/crystallization is a procedure for coalescing solid particles, not changing the chemical composition, only allowing the sculpting of the anatomy of a dental piece. It is worth mentioning that professionals should always follow the manufacturers’ recommendations. Ceramic restorations at elevated temperatures do not melt the particles, they just expand and modify. As a result, deformation can occur in the prosthetic structure. On the other hand, at low temperatures, the material cannot adhere to the restoration. |
| Pressed | (1st) Initially, the wax pattern is made and included in a coating ring. Then, this set must be heated in an oven. (2nd) The press phase of the pre-ceramic ingot is a crucial step for the press processing technique, where it is performed in a specific oven. The glass-matrix ceramic ingot is placed inside the ring’s feeding duct followed by an alumina plunger that will be responsible for injecting the vitro-ceramic when it is fluid. The ring-ingot-plunger assembly is taken into the injection furnace where it will undergo a thermal cycle lasting approximately 30 min. When reaching the maximum temperature, in which the ceramic is high fluidity, a plunger present inside the oven touches the alumina piston, pushing it into the ring. The result is the injection of the ingot, which takes the form of the restoration molded by the coating. (3rd) After the end of the cycle and the cooling of the ring, the coating is cut with a carbide disc and the part is removed from the inside, therefore, adjustments are necessary; especially in the case of glass-matrix ceramics, as the prosthetic structures receive a final characterization with a staining layer and glaze, since the restoration just out of the oven is monochromatic. |
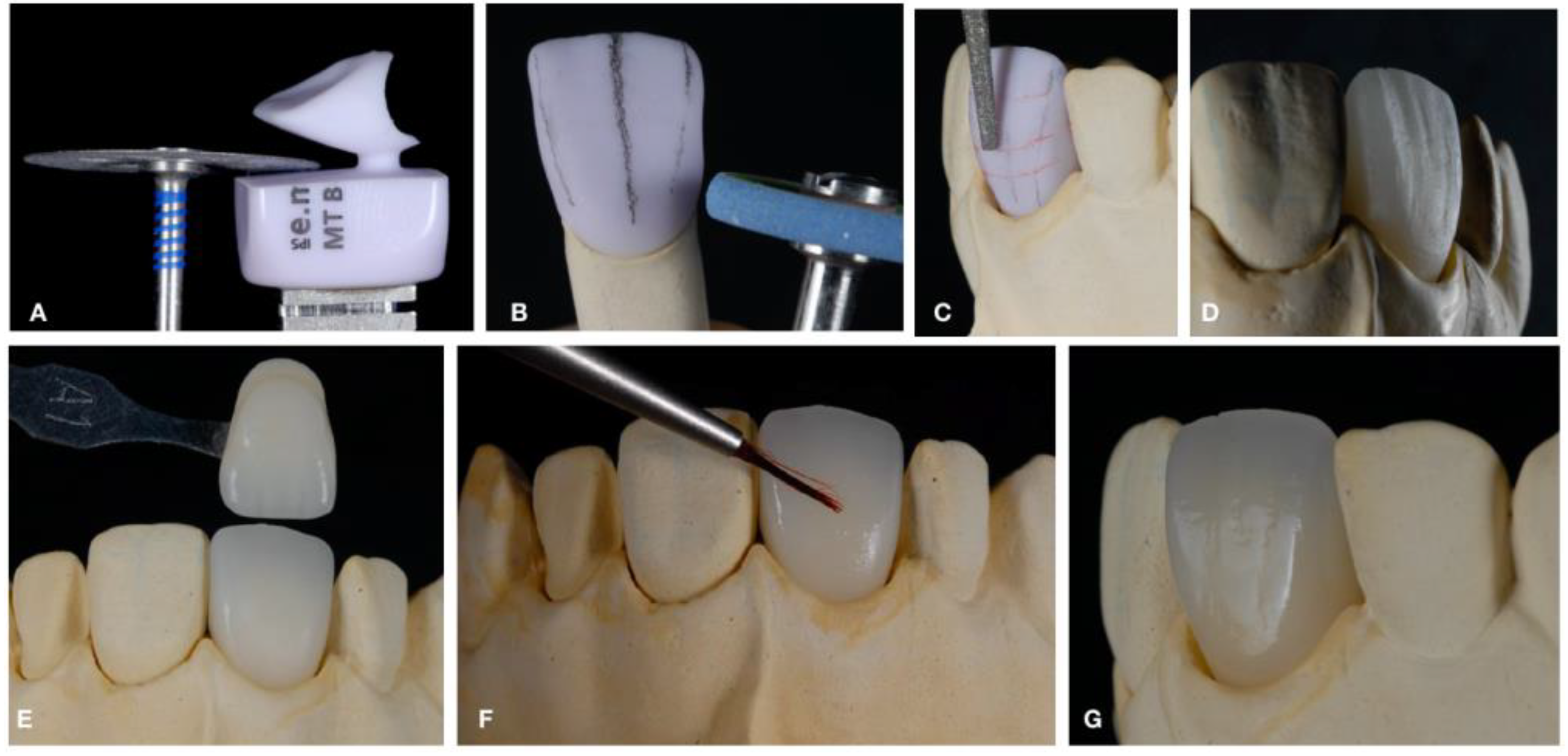
| Milling—Computer Aided Design and Computer Aided Manufacturing (CAD–CAM) | (1st) Initially, a digital image is acquired in a three-dimensional plane of the prepared tooth, and then it is constructed on a computer (.STL file). This image can be obtained directly from the prepared tooth with a digital intraoral scanner or scanning a plaster model with a desktop scanner. On the digital image of the prepared tooth, the digital image of the final restoration is constructed with the help of specific software. The dimension and shape information of the restoration is then sent to a milling unit in which the ceramic restoration is made [25,68,69,70,71,72,73,74,75,76,77,78,79]. (2nd) After obtaining all the digital information, the milling step of a previously sintered/crystallized block is started under ideal conditions by the manufacturer. This block is milled by two diamond tips coupled in fully articulated arms until acquiring the final shape of the restoration, proposed in the software. (3rd) After the milling step is finished and marginally adjusted, the subsequent finishing (glaze or polishing) is performed. In some cases, it is necessary to stain the prosthetic restoration associated with a characterization firing. It is interesting to clarify that in ceramics with polymers in their composition, after the pigmentation stage, the structure must be light-cured. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Matos, J.D.M.; Lopes, G.R.S.; Queiroz, D.A.; Nakano, L.J.N.; Ribeiro, N.C.R.; Barbosa, A.B.; Anami, L.C.; Bottino, M.A. Dental Ceramics: Fabrication Methods and Aesthetic Characterization. Coatings 2022, 12, 1228. https://doi.org/10.3390/coatings12081228
de Matos JDM, Lopes GRS, Queiroz DA, Nakano LJN, Ribeiro NCR, Barbosa AB, Anami LC, Bottino MA. Dental Ceramics: Fabrication Methods and Aesthetic Characterization. Coatings. 2022; 12(8):1228. https://doi.org/10.3390/coatings12081228
Chicago/Turabian Stylede Matos, Jefferson David Melo, Guilherme Rocha Scalzer Lopes, Daher Antonio Queiroz, Leonardo Jiro Nomura Nakano, Nathália Carvalho Ramos Ribeiro, Adriano Baldotto Barbosa, Lilian Costa Anami, and Marco Antonio Bottino. 2022. "Dental Ceramics: Fabrication Methods and Aesthetic Characterization" Coatings 12, no. 8: 1228. https://doi.org/10.3390/coatings12081228