
Bone Density around Titanium Dental Implants Coating Tested/Coated with Chitosan or Melatonin: An Evaluation via Microtomography in Jaws of Beagle Dogs

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Implant Surface Preparation
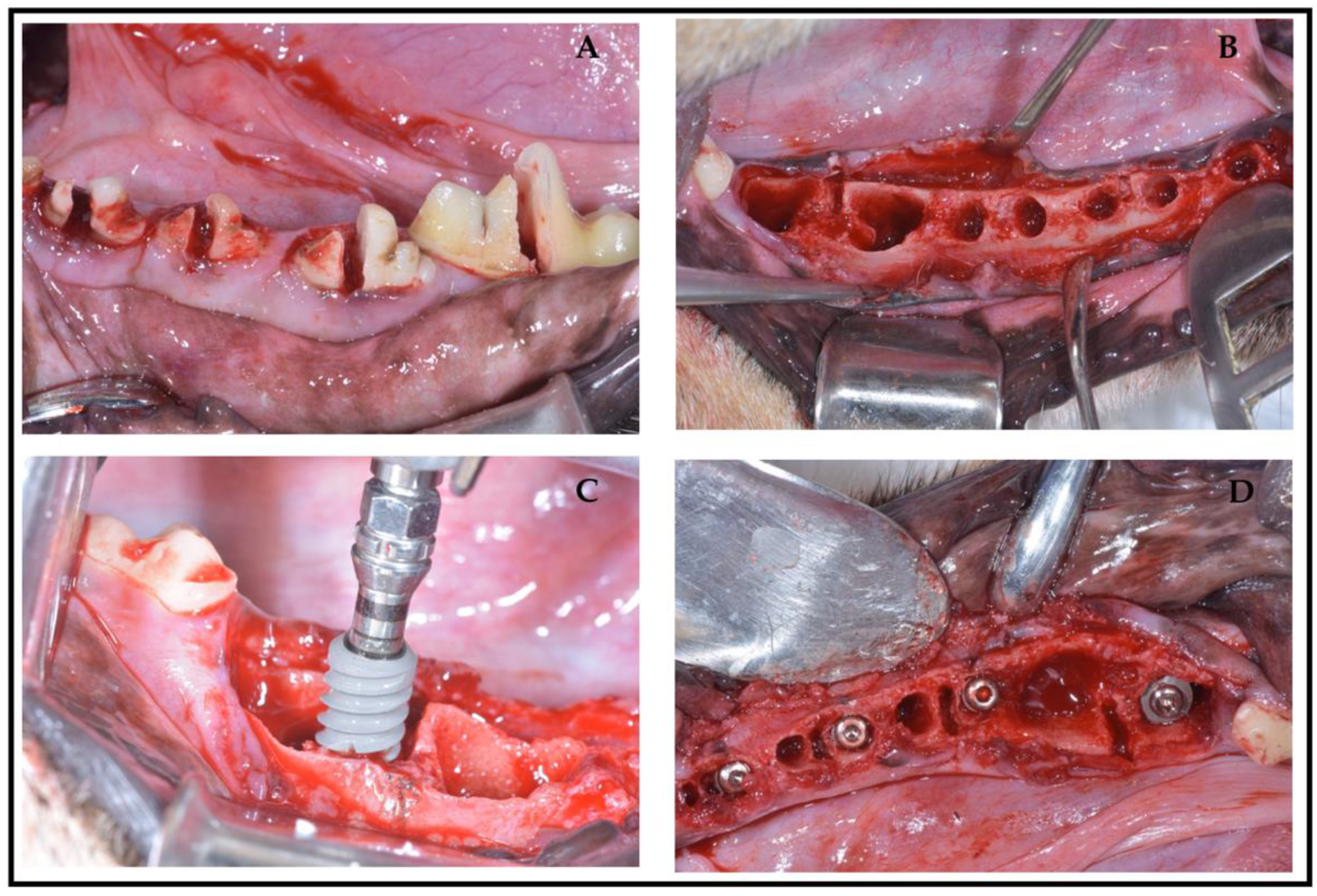
2.3. Surgical Protocol
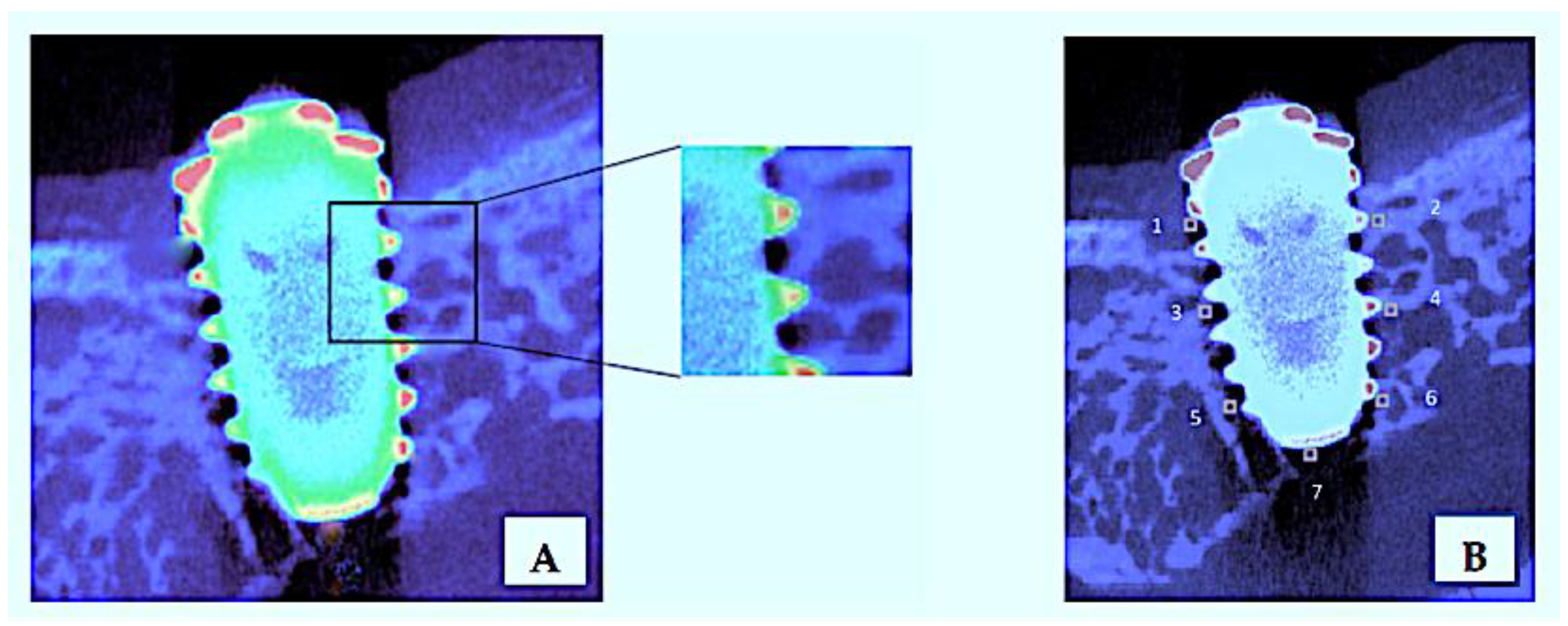
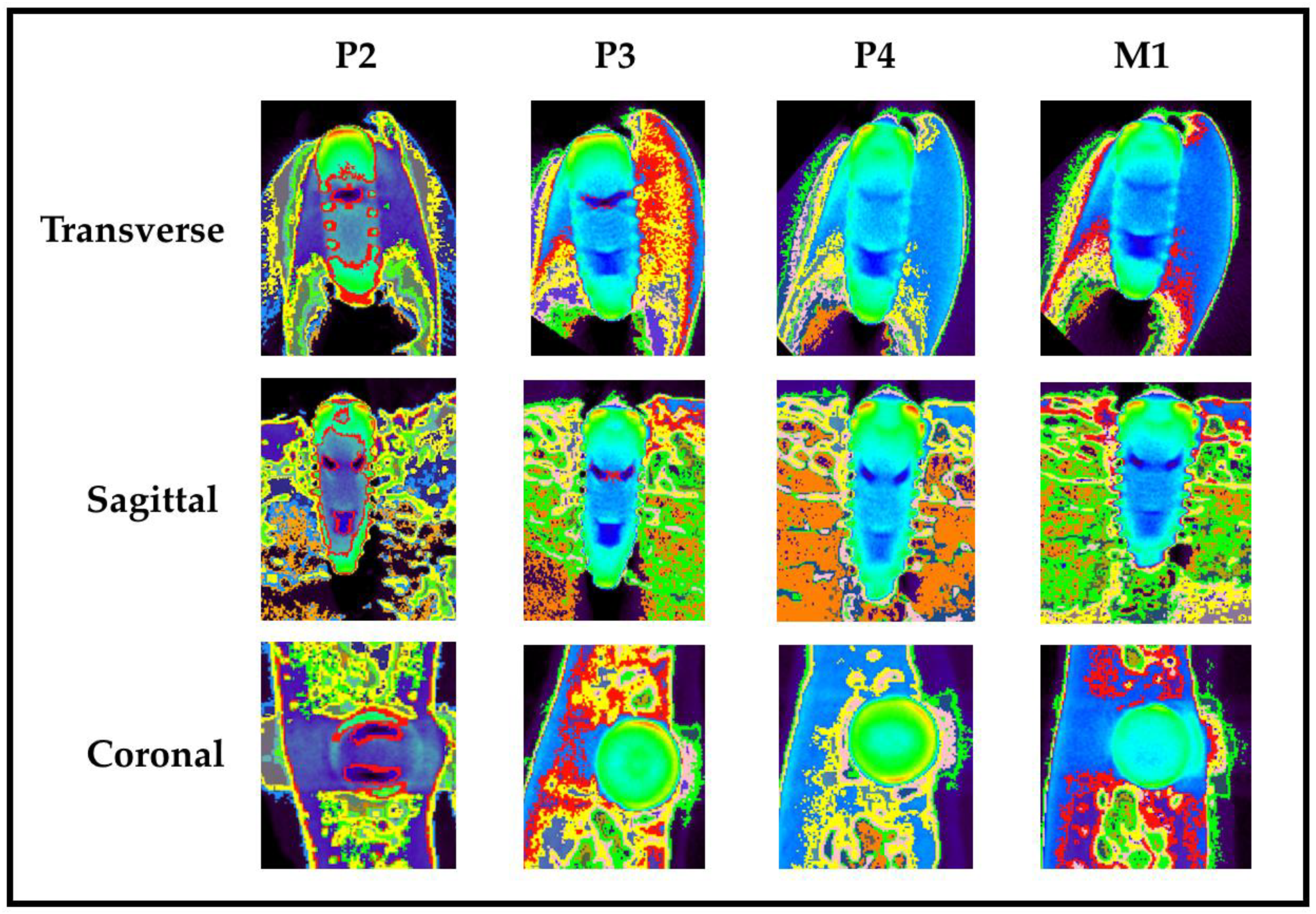
2.4. Micro-Computed Tomography Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BD | Bone Density |
| Ch | Chitosan |
| CT | Computed Tomography |
| FOV | Field of View |
| HU | Hounsfield Unity |
| Mt | Melatonin |
| ROI | Region of Interest |
| SLA | Sandblasted Large grit Acid etched |
| TiO2 | Titanium Oxide |
References
- Rautray, T.R.; Narayanan, R.; Kwon, T.-Y.; Kim, K.-H. Surface modification of titanium and titanium alloys by ion implantation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 581–591. [Google Scholar] [CrossRef]
- Shah, F.A.; Trobos, M.; Thomsen, P.; Palmquist, A. Commercially pure titanium (cp-Ti) versus titanium alloy (Ti6Al4V) materials as bone anchored implants—Is one truly better than the other? Mater. Sci. Eng. C 2016, 62, 960–966. [Google Scholar] [CrossRef]
- López-Valverde, N.; Flores-Fraile, J.; Ramírez, J.M.; De Sousa, B.M.; Herrero-Hernández, S.; López-Valverde, A. Bioactive Surfaces vs. Conventional Surfaces in Titanium Dental Implants: A Comparative Systematic Review. J. Clin. Med. 2020, 9, 2047. [Google Scholar] [CrossRef]
- Zhang, Y.; Zheng, Y.; Li, Y.; Wang, L.; Bai, Y.; Zhao, Q.; Xiong, X.; Cheng, Y.; Tang, Z.; Deng, Y.; et al. Tantalum Nitride-Decorated Titanium with Enhanced Resistance to Microbiologically Induced Corrosion and Mechanical Property for Dental Application. PLoS ONE 2015, 10, e0130774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elieh-Ali-Komi, D.; Hamblin, M.R. Chitin and Chitosan: Production and Application of Versatile Biomedical Nanomaterials. Int. J. Adv. Res. 2016, 4, 411–427. [Google Scholar]
- Qian, J.; Pan, C.; Liang, C. Antimicrobial activity of Fe-loaded chitosan nanoparticles. Eng. Life Sci. 2017, 17, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, B.; Ye, H.; Shang, S.; Xiong, Q.; Yu, K.; Li, Q.; Xiao, Y.; Dai, F.; Lan, G.; Dai, F. Novel wound dressing with chitosan gold nanoparticles capped with a small molecule for effective treatment of multiantibiotic-resistant bacterial infections. Nanotechnology 2018, 29, 425603. [Google Scholar] [CrossRef]
- Covarrubias, C.; Trepiana, D.; Corral, C. Synthesis of hybrid copper-chitosan nanoparticles with antibacterial activity against cariogenic Streptococcus mutans. Dent. Mater. J. 2018, 37, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, L.P.; Andrade, C.T.; Del Aguila, E.M.; Alexander, C.; Paschoalin, V.M. Assessing the antimicrobial activity of chitosan nanoparticles by fluorescence-labeling. Int. J. Biotechnol. Bioeng. 2018, 12, 111–117. [Google Scholar]
- Bojar, W.; Kucharska, M.; Ciach, T.; Koperski, Ł.; Jastrzebski, Z.; Szałwiński, M. Bone regeneration potential of the new chitosan-based alloplastic biomaterial. J. Biomater. Appl. 2014, 28, 1060–1068. [Google Scholar] [CrossRef]
- Aguilar, A.; Zein, N.; Harmouch, E.; Hafdi, B.; Bornert, F.; Offner, D.; Clauss, F.; Fioretti, F.; Huck, O.; Benkirane-Jessel, N.; et al. Application of Chitosan in Bone and Dental Engineering. Molecules 2019, 24, 3009. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-S.; Choi, S.-H.; Moon, I.-S.; Cho, K.S.; Chai, J.-K.; Kim, C.-K. Eight-week histological analysis on the effect of chitosan on surgically created one-wall intrabony defects in beagle dogs. J. Clin. Periodontol. 2003, 30, 443–453. [Google Scholar] [CrossRef]
- Abinaya, B.; Prasith, T.P.; Ashwin, B.; Chandran, S.V.; Selvamurugan, N. Chitosan in Surface Modification for Bone Tissue Engineering Applications. Biotechnol. J. 2019, 14, e1900171. [Google Scholar] [CrossRef] [PubMed]
- Soundarya, S.P.; Menon, A.H.; Chandran, S.V.; Selvamurugan, N. Bone tissue engineering: Scaffold preparation using chitosan and other biomaterials with different design and fabrication techniques. Int. J. Biol. Macromol. 2018, 119, 1228–1239. [Google Scholar] [CrossRef]
- He, L.-H.; Yao, L.; Xue, R.; Sun, J.; Song, R. In-situ mineralization of chitosan/calcium phosphate composite and the effect of solvent on the structure. Front. Mater. Sci. 2011, 5, 282–292. [Google Scholar] [CrossRef]
- Leonor, I.; Baran, E.; Kawashita, M.; Reis, R.L.; Kokubo, T.; Nakamura, T. Growth of a bonelike apatite on chitosan microparticles after a calcium silicate treatment. Acta Biomater. 2008, 4, 1349–1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.-T.; Lu, T.-W.; Chen, C.-H.; Lu, K.-Y.; Mi, F.-L. Development of nanocomposite scaffolds based on biomineralization of N,O-carboxymethyl chitosan/fucoidan conjugates for bone tissue engineering. Int. J. Biol. Macromol. 2018, 120, 2335–2345. [Google Scholar] [CrossRef]
- Xie, C.-M.; Lu, X.; Wang, K.-F.; Meng, F.-Z.; Jiang, O.; Zhang, H.-P.; Zhi, W.; Fang, L. Silver Nanoparticles and Growth Factors Incorporated Hydroxyapatite Coatings on Metallic Implant Surfaces for Enhancement of Osteoinductivity and Antibacterial Properties. ACS Appl. Mater. Interfaces 2014, 6, 8580–8589. [Google Scholar] [CrossRef]
- Ishihara, M.; Nakanishi, K.; Ono, K.; Sato, M.; Kikuchi, M.; Saito, Y.; Yura, H.; Matsui, T.; Hattori, H.; Uenoyama, M.; et al. Photocrosslinkable chitosan as a dressing for wound occlusion and accelerator in healing process. Biomaterials 2002, 23, 833–840. [Google Scholar] [CrossRef]
- Tan, D.X.; Xu, B.; Zhou, X.; Reiter, R.J. Pineal Calcification, Melatonin Production, Aging, Associated Health Consequences and Rejuvenation of the Pineal Gland. Molecules 2018, 23, 301. [Google Scholar] [CrossRef] [Green Version]
- Maria, S.; Samsonraj, R.; Munmun, F.; Glas, J.; Silvestros, M.; Kotlarczyk, M.; Rylands, R.; Dudakovic, A.; Van Wijnen, A.J.; Enderby, L.T.; et al. Biological effects of melatonin on osteoblast/osteoclast cocultures, bone, and quality of life: Implications of a role for MT2 melatonin receptors, MEK1/2, and MEK5 in melatonin-mediated osteoblastogenesis. J. Pineal Res. 2018, 64, e12465. [Google Scholar] [CrossRef]
- Manchester, L.C.; Coto-Montes, A.; Boga, J.A.; Andersen, L.P.H.; Zhou, Z.; Galano, A.; Vriend, J.; Tan, D.-X.; Reiter, R.J. Melatonin: An ancient molecule that makes oxygen metabolically tolerable. J. Pineal Res. 2015, 59, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Salvatierra, A.A.; Gargallo-Albiol, J.; Delgado-Ruiz, R.A.; Sanchez, J.E.M.; Satorres-Nieto, M. Zirconia with laser-modified microgrooved surface vs. titanium implants covered with melatonin stimulates bone formation. Experimental study in tibia rabbits. Clin. Oral Implant. Res. 2014, 26, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Guardia, J.; Gómez-Moreno, G.; Ferrera, M.J.; Cutando, A.; Dds, G.G. Evaluation of Effects of Topic Melatonin on Implant Surface at 5 and 8 Weeks in Beagle Dogs. Clin. Implant. Dent. Relat. Res. 2009, 13, 262–268. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Gómez-Moreno, G.; López-Marí, L.; Guardia, J.; Marínez-González, J.M.; Barone, A.; Tresguerres, I.F.; Paredes, S.D.; Fuentes-Breto, L. Retracted: Actions of melatonin mixed with collagenized porcine bone versus porcine bone only on osteointegration of dental implants. J. Pineal Res. 2010, 48, 194–203. [Google Scholar] [CrossRef]
- Hounsfield, G.N. Computerized transverse axial scanning (tomography): Description of system. Br. J. Radiol. 1973, 46, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Muller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef]
- Irie, M.S.; Rabelo, G.; Spin-Neto, R.; Dechichi, P.; Borges, J.S.; Soares, P.B.F. Use of Micro-Computed Tomography for Bone Evaluation in Dentistry. Braz. Dent. J. 2018, 29, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Peyrin, F. Evaluation of bone scaffolds by micro-CT. Osteoporos. Int. 2011, 22, 2043–2048. [Google Scholar] [CrossRef] [PubMed]
- Shi, G.; Subramanian, S.; Cao, Q.; Demehri, S.; Siewerdsen, J.H.; Zbijewski, W. Application of a novel ultra-high resolution multi-detector CT in quantitative imaging of trabecular microstructure. Proc. SPIE Int. Soc. Opt. Eng. 2020, 11317, 113171E. [Google Scholar]
- Young, S.; Kretlow, J.D.; Nguyen, C.; Bashoura, A.G.; Baggett, L.S.; Jansen, J.A.; Wong, M.; Mikos, A.G. Microcomputed tomography characterization of neovascularization in bone tissue engineering applications. Tissue Eng. Part B Rev. 2008, 14, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-S.; Yi, K.-Y.; Lee, I.-S.; Jung, Y.-C. Correlation between microtomography and histomorphometry for assessment of implant osseointegration. Clin. Oral Implant. Res. 2005, 16, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Swain, M.; Xue, J. State of the art of Micro-CT applications in dental research. Int. J. Oral Sci. 2009, 1, 177–188. [Google Scholar] [CrossRef]
- Salomó-Coll, O.; Maté-Sánchez de Val, J.E.; Ramírez-Fernández, M.P.; Satorres-Nieto, M.; Gargallo-Albiol, J.; Calvo-Guirado, J.L. Osseoinductive elements for promoting osseointegration around immediate implants: A pilot study in the foxhound dog. Clin. Oral Implant. Res. 2016, 27, e167–e175. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, Z.; Li, Y.; Yang, Y.; Ju, X.; He, R. The preparation and physiochemical characterization of rapeseed protein hydrolysate-chitosan composite films. Food Chem. 2019, 272, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Norton, M.R.; Gamble, C. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implant. Res. 2001, 12, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E. Density of bone: Effect on treatment planning, surgical approach, and healing. In Contemporary Implant Dentistry; Mosby: St. Louis, MO, USA, 1993; pp. 469–485. [Google Scholar]
- Bra-Nemark, P.-I.; Zarb, G.A.; Albrektsson, T.; Rosen, H.M. Tissue-Integrated Prostheses. Osseointegration in Clinical Dentistry. Plast. Reconstr. Surg. 1986, 77, 496–497. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: Hillsdale, MI, USA; Hove, UK, 1988. [Google Scholar]
- Sawilowsky, S. New effect size rules of thumb. J. Mod. App. Stat. Methods 2009, 8, 597–599. [Google Scholar] [CrossRef]
- Balbinot, G.S.; Leitune, V.C.B.; Ponzoni, D.; Collares, F.M. Bone healing with niobium-containing bioactive glass composition in rat femur model: A micro-CT study. Dent Mater. 2019, 35, 1490–1497. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhao, J.; Liao, E.Y.; Dai, R.C.; Wu, X.P.; Genant, H.K. Application of micro-CT assessment of 3-D bone micro- structure in preclinical and clinical studies. J. Bone Miner. Metab. 2005, 23, 122–131. [Google Scholar] [CrossRef]
- Sennerby, L.; Wennerberg, A.; Pasop, F. A new microtomo-graphic technique for non-invasive evaluation of the bone structure around implants. Clin. Oral Implant. Res. 2001, 12, 91–94. [Google Scholar] [CrossRef]
- Van Dessel, J.; Nicolielo, L.F.; Huang, Y.; Coudyzer, W.; Salmon, B.; Lambrichts, I.; Jacobs, R. Accuracy and reliability of different cone beam computed tomography (CBCT) devices for structural analysis of alveolar bone in comparison with multislice CT and micro-CT. Eur. J. Oral Implantol. 2017, 10, 95–105. [Google Scholar]
- Rebaudi, A.; Trisi, P.; Cella, R.; Cecchini, G. Preoperative evaluation of bone quality and bone density using a novel CT/microCT-based hard-normal-soft classification system. Int. J. Oral Maxillofac. Implant. 2010, 25, 75–85. [Google Scholar]
- Fanuscu, M.I.; Chang, T.-L. Three-dimensional morphometric analysis of human cadaver bone: Microstructural data from maxilla and mandible. Clin. Oral Implant. Res. 2004, 15, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Cano, J.; Campo, J.; Vaquero, J.J.; González, J.M.M.; Bascones, A. High resolution image in bone biology II. Review of the literature. Med. Oral Patol. Oral Cir. Bucal 2008, 13, E31–E35. [Google Scholar] [PubMed]
- Tjong, W.; Nirody, J.; Burghardt, A.J.; Carballido-Gamio, J.; Kazakia, G.J. Structural analysis of cortical porosity applied to HR-pQCT data. Med. Phys. 2014, 41, 013701. [Google Scholar] [CrossRef]
- Rabelo, G.D.; Coutinho-Camillo, C.; Kowalski, L.P.; Portero-Muzy, N.; Roux, J.-P.; Chavassieux, P.; Alves, F.A. Evaluation of cortical mandibular bone in patients with oral squamous cell carcinoma. Clin. Oral Investig. 2017, 22, 783–790. [Google Scholar] [CrossRef]
- Blok, Y.; Gravesteijn, F.; van Ruijven, L.; Koolstra, J. Micro-architecture and mineralization of the human alveolar bone obtained with microCT. Arch. Oral Biol. 2013, 58, 621–627. [Google Scholar] [CrossRef]
- Romão, M.; Marques, M.; Cortes, A.; Horliana, A.; Moreira, M.; Lascala, C. Micro-computed tomography and histomorphometric analysis of human alveolar bone repair induced by laser phototherapy: A pilot study. Int. J. Oral Maxillofac. Surg. 2015, 44, 1521–1528. [Google Scholar] [CrossRef]
- Chesnutt, B.M.; Yuan, Y.; Buddington, K.; Haggard, W.O.; Bumgardner, J.D. Composite Chitosan/Nano-Hydroxyapatite Scaffolds Induce Osteocalcin Production by Osteoblasts In Vitro and Support Bone Formation In Vivo. Tissue Eng. Part A 2009, 15, 2571–2579. [Google Scholar] [CrossRef]
- Cheung, R.C.F.; Ng, T.B.; Wong, J.H.; Chan, W.Y. Chitosan: An Update on Potential Biomedical and Pharmaceutical Applications. Mar. Drugs 2015, 13, 5156–5186. [Google Scholar] [CrossRef] [PubMed]
- Ezoddini-Ardakani, F.; Navabazam, A.; Fatehi, F.; Danesh-Ardekani, M.; Khadem, S.; Rouhi, G. Histologic evaluation of chitosan as an accelerator of bone regeneration in microdrilled rat tibias. Dent. Res. J. 2012, 9, 694–699. [Google Scholar]
- Khajuria, D.K.; Zahra, S.F.; Razdan, R. Effect of locally administered novel biodegradable chitosan based risedronate/zinc-hydroxyapatite intra-pocket dental film on alveolar bone density in rat model of periodontitis. J. Biomater. Sci. Polym. Ed. 2017, 29, 74–91. [Google Scholar] [CrossRef]
- López-Valverde, N.; López-Valverde, A.; Ramírez, J. Systematic Review of Effectiveness of Chitosan as a Biofunctionalizer of Titanium Implants. Biology 2021, 10, 102. [Google Scholar] [CrossRef]
- Koyama, H.; Nakade, O.; Takada, Y.; Kaku, T.; Lau, K.-H.W. Melatonin at Pharmacologic Doses Increases Bone Mass by Suppressing Resorption Through Down-Regulation of the RANKL-Mediated Osteoclast Formation and Activation. J. Bone Miner. Res. 2002, 17, 1219–1229. [Google Scholar] [CrossRef]
- Cutando, A.; Gómez-Moreno, G.; Arana, C.; Muñoz, F.; Lopez-Peña, M.; Stephenson, J.; Reiter, R.J. Melatoninstimulates osteointegration of dental implants. J. Pineal Res. 2008, 45, 174–179. [Google Scholar] [CrossRef]
- Tresguerres, I.F.; Clemente, C.; Blanco, L.; Khraisat, A.; Tamimi, F.; Tresguerres, J.A. Effects of Local Melatonin Application on Implant Osseointegration. Clin. Implant. Dent. Relat. Res. 2010, 14, 395–399. [Google Scholar] [CrossRef] [PubMed]
- López-Valverde, N.; Pardal-Peláez, B.; López-Valverde, A.; Ramírez, J. Role of Melatonin in Bone Remodeling around Titanium Dental Implants: Meta-Analysis. Coatings 2021, 11, 271. [Google Scholar] [CrossRef]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface characteristics of dental implants: A review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef]
- Sultankulov, B.; Berillo, D.; Sultankulova, K.; Tokay, T.; Saparov, A. Progress in the development of chitosan-based biomaterials for tissue engineering and regenerative medicine. Biomolecules 2019, 9, 470. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Yu, S.; Chen, G.; Zheng, W.; Peng, J.; Huang, X.; Chen, L. Insight into the roles of melatonin in bone tissue and bone-related diseases (Review). Int. J. Mol. Med. 2021, 47, 82. [Google Scholar] [CrossRef]
- Annunziata, M.; Guida, L. The Effect of Titanium Surface Modifications on Dental Implant Osseointegration. Craniofacial Sutures 2015, 17, 62–77. [Google Scholar] [CrossRef]
- Junker, R.; Dimakis, A.; Thoneick, M.; Jansen, J.A. Effects of implant surface coatings and composition on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20, 185–206. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, L.T.; Leeuwenburgh, S.; Wolke, J.G.C.; Jansen, J.A. Organic–Inorganic Surface Modifications for Titanium Implant Surfaces. Pharm. Res. 2008, 25, 2357–2369. [Google Scholar] [CrossRef] [Green Version]
- Shapurian, T.; Damoulis, P.D.; Reiser, G.M.; Griffin, T.J.; Rand, W.M. Quantitative evaluation of bone density using the Hounsfield index. Int. J. Oral Maxillofac. Implant. 2006, 21, 290–297. [Google Scholar]
- Di Stefano, D.A.; Arosio, P.; Pagnutti, S.; Vinci, R.; Gherlone, E. Distribution of Trabecular Bone Density in the Maxilla and Mandible. Implant Dent. 2019, 28, 340–348. [Google Scholar] [CrossRef]
- Molly, L. Bone density and primary stability in implant therapy. Clin. Oral Implant. Res. 2006, 17, 124–135. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; Tozum, T.; Tumer, C. Bone density assessments of oral implant sites using computerized tomography. J. Oral Rehabil. 2007, 34, 267–272. [Google Scholar] [CrossRef]
- De Smet, E.; Jaecques, S.; Wevers, M.; Jansen, J.A.; Jacobs, R.; Sloten, J.V.; Naert, I.E. Effect of controlled early implant loading on bone healing and bone mass in guinea pigs, as assessed by micro-CT and histology. Eur. J. Oral Sci. 2006, 114, 232–242. [Google Scholar] [CrossRef]
- Barrett, J.F.; Keat, N. Artifacts in CT: Recognition and Avoidance. Radiographics 2004, 24, 1679–1691. [Google Scholar] [CrossRef]
- Rebaudi, A.; Koller, B.; Laib, A.; Trisi, P. Microcomputed tomographic analysis of the peri-implant bone. Int. J. Periodontics Restor. Dent. 2004, 24, 316–325. [Google Scholar]
- Stoppie, N.; Van Der Waerden, J.-P.; Jansen, J.A.; Duyck, J.; Wevers, M.; Naert, I.E. Validation of Microfocus Computed Tomography in the Evaluation of Bone Implant Specimens. Clin. Implant. Dent. Relat. Res. 2005, 7, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Song, J.W.; Cha, J.Y.; Bechtold, T.E.; Park, Y.C. Influence of peri-implant artifacts on bone morphometric analysis with micro-computed tomography. Int. J. Oral Maxillofac. Implant. 2013, 28, 519–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, A.I.; Richards, R.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cells Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | ChG | MtG | CG | p-Global c | |||
|---|---|---|---|---|---|---|---|
| - | Mean ± SD | n | Mean ± SD | n | Mean ± SD | ||
| All | 112 | 0.35 ± 0.32 | 112 | 0.33 ± 0.32 | 112 | 0.37 ± 0.30 | 0.631 |
| ROI’s (in levels) | - | - | - | - | - | - | - |
| Crestal [C] | 32 | 0.58 ± 0.20 | 32 | 0.54 ± 0.13 | 32 | 0.59 ± 0.14 | 0.438 |
| Medial [M] | 64 | 0.38 ± 0.18 | 64 | 0.35 ± 0.22 | 64 | 0.38 ± 0.19 | 0.680 |
| Apical [A] | 16 | −0.20 ± 0.32 | 16 | −0.18 ± 0.38 | 16 | −0.11 ± 0.33 | 0.723 |
| p-global c | - | <0.001 | - | <0.001 | - | <0.001 | - |
| paired comparisons d | - | C ≠ M ≠ A | - | C ≠ M ≠ A | - | C ≠ M ≠ A | - |
| Tooth type (position) | - | - | - | - | - | - | - |
| P2 | 35 | 0.11 ± 0.34 | 21 | 0.12 ± 0.35 | 28 | 0.09 ± 0.31 | <0.001 |
| P3 | 28 | 0.11 ± 0.34 | 35 | 0.08 ± 0.28 | 21 | 0.12 ± 0.34 | 0.207 |
| P4 | 35 | 0.11 ± 0.33 | 35 | 0.12 ± 0.34 | 14 | 0.05 ± 0.22 | 0.963 |
| M1 | 14 | 0.05 ± 0.23 | 21 | 0.07 ± 0.27 | 49 | 0.08 ± 0.29 | 0.693 |
| p-global c | - | 0.003 | - | 0.004 | - | 0.582 | - |
| paired comparisons d | - | PM2 ≠ M1 | - | PM2 ≠ PM3, M1 | - | - | - |
| Variable | β ± se b | p-Value c |
|---|---|---|
| Group | - | 0.653 |
| ChG | 0.00 ± 0.04 | |
| MtG | −0.04 ± 0.04 | |
| CG | 0 | |
| ROIs (in levels) | - | <0.001 |
| Crestal | 0.73 ± 0.04 | |
| Medial | 0.54 ± 0.04 | |
| Apical (reference) | 0 | |
| Tooth type (position) | - | 0.032 |
| P2 | −0.10 ± 0.04 | |
| P3 | −0.04 ± 0.05 | |
| P4 | −0.04 ± 0.05 | |
| M1 (reference) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Valverde, N.; López-Valverde, A.; Aragoneses, J.M.; Martínez-Martínez, F.; González-Escudero, M.C.; Ramírez, J.M. Bone Density around Titanium Dental Implants Coating Tested/Coated with Chitosan or Melatonin: An Evaluation via Microtomography in Jaws of Beagle Dogs. Coatings 2021, 11, 777. https://doi.org/10.3390/coatings11070777
López-Valverde N, López-Valverde A, Aragoneses JM, Martínez-Martínez F, González-Escudero MC, Ramírez JM. Bone Density around Titanium Dental Implants Coating Tested/Coated with Chitosan or Melatonin: An Evaluation via Microtomography in Jaws of Beagle Dogs. Coatings. 2021; 11(7):777. https://doi.org/10.3390/coatings11070777
Chicago/Turabian StyleLópez-Valverde, Nansi, Antonio López-Valverde, Juan Manuel Aragoneses, Francisco Martínez-Martínez, María C. González-Escudero, and Juan Manuel Ramírez. 2021. "Bone Density around Titanium Dental Implants Coating Tested/Coated with Chitosan or Melatonin: An Evaluation via Microtomography in Jaws of Beagle Dogs" Coatings 11, no. 7: 777. https://doi.org/10.3390/coatings11070777