
Trends in Pseudomonas aeruginosa (P. aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review
 , ,
, ,
Abstract
:1. Introduction
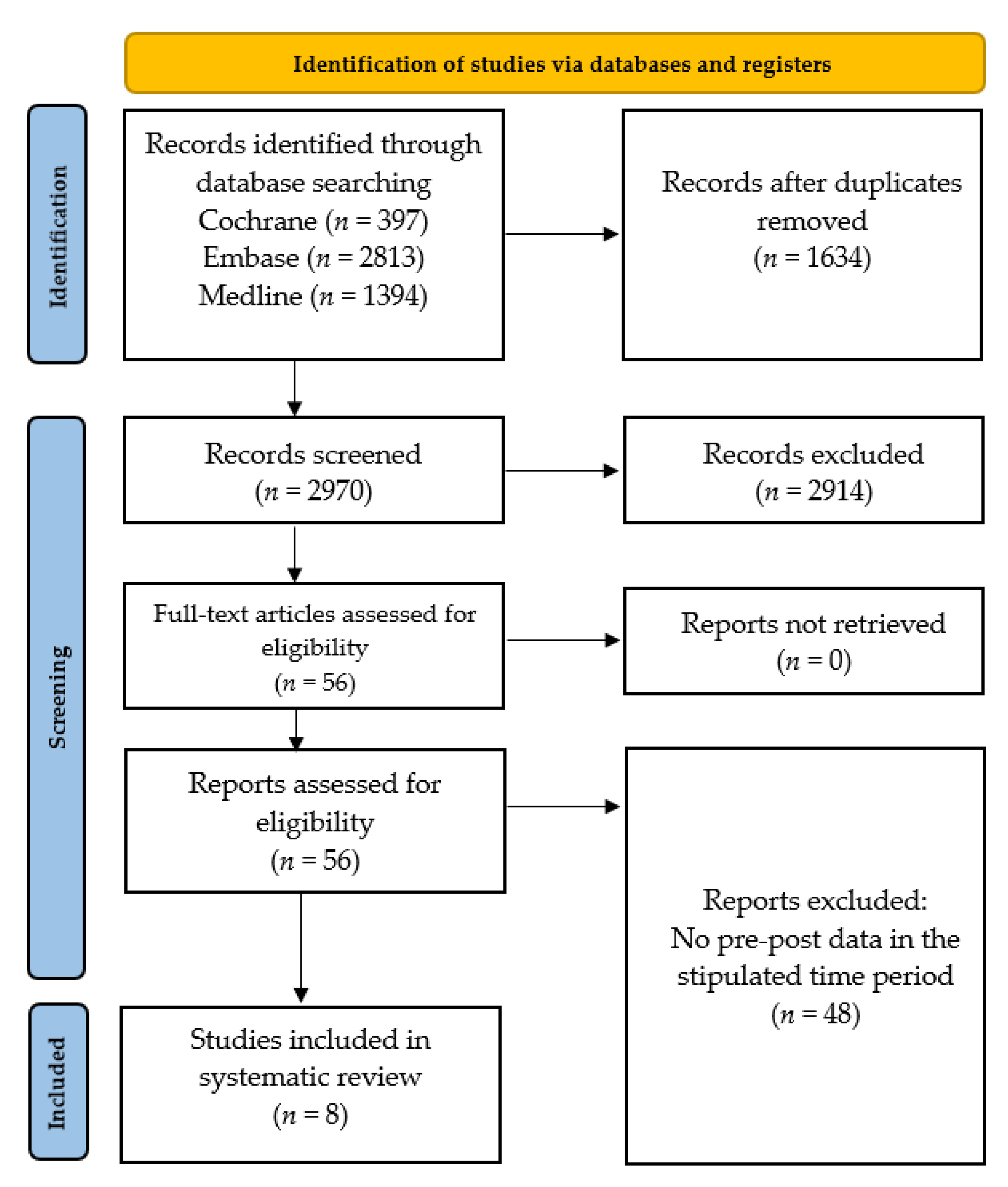
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kollef, M.H.; Torres, A.; Shorr, A.F.; Martin-Loeches, I.; Micek, S.T. Nosocomial Infection. Crit. Care Med. 2021, 49, 169–187. [Google Scholar] [CrossRef] [PubMed]
- Lucena, A.; Dalla Costa, L.M.; Nogueira, K.S.; Matos, A.P.; Gales, A.C.; Paganini, M.C.; Castro, M.E.; Raboni, S.M. Nosocomial infections with metallo-beta-lactamase-producing Pseudomonas aeruginosa: Molecular epidemiology, risk factors, clinical features and outcomes. J. Hosp. Infect. 2014, 87, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Cots, F.; Sala, M.; Comas, M.; Belvis, F.; Riu, M.; Salvadó, M.; Grau, S.; Horcajada, J.P.; Montero, M.M.; et al. Hospital costs of nosocomial multi-drug resistant Pseudomonas aeruginosa acquisition. BMC Health Serv. Res. 2012, 12, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaier, K.; Heister, T.; Götting, T.; Wolkewitz, M.; Mutters, N.T. Measuring the in-hospital costs of Pseudomonas aeruginosa pneumonia: Methodology and results from a German teaching hospital. BMC Infect. Dis. 2019, 19, 1028. [Google Scholar] [CrossRef] [Green Version]
- Vidal, F.; Mensa, J.; Almela, M.; Martínez, J.A.; Marco, F.; Casals, C.; Gatell, J.M.; Soriano, E.; Jimenez de Anta, M.T. Epidemiology and outcome of Pseudomonas aeruginosa bacteremia, with special emphasis on the influence of antibiotic treatment. Analysis of 189 episodes. Arch. Intern. Med. 1996, 156, 2121–2126. [Google Scholar] [CrossRef] [PubMed]
- Pfaller, M.A.; Jones, R.N.; Doern, G.V.; Kugler, K. Bacterial pathogens isolated from patients with bloodstream infection: Frequencies of occurrence and antimicrobial susceptibility patterns from the SENTRY antimicrobial surveillance program (United States and Canada, 1997). Antimicrob. Agents Chemother. 1998, 42, 1762–1770. [Google Scholar] [CrossRef] [Green Version]
- Richards, M.J.; Edwards, J.R.; Culver, D.H.; Gaynes, R.P. Nosocomial infections in medical intensive care units in the United States. National Nosocomial Infections Surveillance System. Crit. Care Med. 1999, 27, 887–892. [Google Scholar] [CrossRef]
- Bodey, G.P.; Jadeja, L.; Elting, L. Pseudomonas bacteremia. Retrospective analysis of 410 episodes. Arch. Intern. Med. 1985, 145, 1621–1629. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Emerging Infections Program Healthcare-Associated Infections and Antimicrobial Use Prevalence Survey Team. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [Green Version]
- Weiner, L.M.; Webb, A.K.; Limbago, B.; Dudeck, M.A.; Patel, J.; Kallen, A.J.; Edwards, J.R.; Sievert, D.M. Antimicrobial-Resistant Pathogens Associated With Healthcare-Associated Infections: Summary of Data Reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2011–2014. Infect. Control. Hosp. Epidemiol. 2016, 37, 1288–1301. [Google Scholar] [CrossRef] [Green Version]
- Gottesman, T.; Fedorowsky, R.; Yerushalmi, R.; Lellouche, J.; Nutman, A. An outbreak of carbapenem-resistant Acinetobacter baumannii in a COVID-19 dedicated hospital. Infect. Prev. Pract. 2021, 3, 100113. [Google Scholar] [CrossRef] [PubMed]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef] [PubMed]
- Campion, M.; Scully, G. Antibiotic Use in the Intensive Care Unit: Optimization and De-Escalation. J. Intensive Care Med. 2018, 33, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Gerver, S.M.; Nsonwu, O.; Thelwall, S.; Brown, C.S.; Hope, R. Trends in rates of incidence, fatality and antimicrobial resistance among isolates of Pseudomonas spp. causing bloodstream infections in England between 2009 and 2018: Results from a national voluntary surveillance scheme. J. Hosp. Infect. 2022, 120, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Werth, B.J.; Carreno, J.J.; Reveles, K.R. Shifting trends in the incidence of Pseudomonas aeruginosa septicemia in hospitalized adults in the United States from 1996–2010. Am. J. Infect. Control. 2015, 43, 465–468. [Google Scholar] [CrossRef]
- Iversen, B.G. Contaminated mouth swabs caused a multi-hospital outbreak of Pseudomonas aeruginosa infection. J. Oral Microbiol. 2010, 2, 5123. [Google Scholar] [CrossRef]
- Zhu, N.J.; Rawson, T.M.; Mookerjee, S.; Price, J.R.; Davies, F.; Otter, J.; Aylin, P.; Hope, R.; Gilchrist, M.; Shersing, Y.; et al. Changing patterns of bloodstream infections in the community and acute care across 2 coronavirus disease 2019 epidemic waves: A retrospective analysis using data linkage. Clin. Infect. Dis. 2022, 75, e1082–e1091. [Google Scholar] [CrossRef]
- Sturm, L.K.; Saake, K.; Roberts, P.B.; Masoudi, F.A.; Fakih, M.G. Impact of COVID-19 pandemic on hospital onset bloodstream infections (HOBSI) at a large health system. Am. J. Infect. Control 2022, 50, 245–249. [Google Scholar] [CrossRef]
- Amarsy, R.; Trystram, D.; Cambau, E.; Monteil, C.; Fournier, S.; Oliary, J.; Junot, H.; Sabatier, P.; Porcher, R.; Robert, J.; et al. “la Collégiale de Bactériologie–Virologie–Hygiène de l’Assistance Publique—Hôpitaux de Paris”. Surging bloodstream infections and antimicrobial resistance during the first wave of COVID-19: A study in a large multihospital institution in the Paris region. Int. J. Infect. Dis. 2022, 114, 90–96. [Google Scholar] [CrossRef]
- Hirabayashi, A.; Kajihara, T.; Yahara, K.; Shibayama, K.; Sugai, M. Impact of the COVID-19 pandemic on the surveillance of antimicrobial resistance. J. Hosp. Infect. 2021, 117, 147–156. [Google Scholar] [CrossRef]
- İpek, S.; Şahin, A.; Gungor, S.; Yurttutan, S.; Güllü, U.U.; Inal, S.; Demiray, Ş. Nosocomial Infections in Non-COVID-19 Pediatric Patients Prior to and During the Pandemic in a Pediatric Intensive Care Unit. Cureus 2022, 14, e21451. [Google Scholar] [CrossRef]
- Winders, H.R.; Bailey, P.; Kohn, J.; Faulkner-Fennell, C.M.; Utley, S.; Lantz, E.; Sarbacker, L.; Justo, J.A.; Bookstaver, P.B.; Weissman, S.; et al. Change in Antimicrobial Use During COVID-19 Pandemic in South Carolina Hospitals: A Multicenter Observational Cohort Study. Int. J. Antimicrob. Agents. 2021, 58, 106453. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, E.; Van Herendael, B.; Verbrugghe, W.; Ieven, M.; Goovaerts, E.; Bergs, K.; Wouters, K.; Jorens, P.G.; Goossens, H. Emergence of antimicrobial resistance to Pseudomonas aeruginosa in the intensive care unit: Association with the duration of antibiotic exposure and mode of administration. Ann. Intensive Care. 2017, 7, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Despotovic, A.; Milosevic, B.; Cirkovic, A.; Vujovic, A.; Cucanic, K.; Cucanic, T.; Stevanovic, G. The Impact of COVID-19 on the Profile of Hospital-Acquired Infections in Adult Intensive Care Units. Antibiotics 2021, 10, 1146. [Google Scholar] [CrossRef] [PubMed]
- Meschiari, M.; Onorato, L.; Bacca, E.; Orlando, G.; Menozzi, M.; Franceschini, E.; Bedini, A.; Cervo, A.; Santoro, A.; Sarti, M.; et al. Long-Term Impact of the COVID-19 Pandemic on In-Hospital Antibiotic Consumption and Antibiotic Resistance: A Time Series Analysis (2015–2021). Antibiotics 2022, 11, 826. [Google Scholar] [CrossRef]
- Shbaklo, N.; Corcione, S.; Vicentini, C.; Giordano, S.; Fiorentino, D.; Bianco, G.; Cattel, F.; Cavallo, R.; Zotti, C.M.; De Rosa, F.G. An Observational Study of MDR Hospital-Acquired Infections and Antibiotic Use during COVID-19 Pandemic: A Call for Antimicrobial Stewardship Programs. Antibiotics 2022, 11, 695. [Google Scholar] [CrossRef]
- Sloot, R.; Nsonwu, O.; Chudasama, D.; Rooney, G.; Pearson, C.; Choi, H.; Mason, E.; Springer, A.; Gerver, S.; Brown, C.; et al. Rising rates of hospital-onset Klebsiella spp. and Pseudomonas aeruginosa bacteraemia in NHS acute trusts in England: A review of national surveillance data, August 2020-February 2021. J. Hosp. Infect. 2022, 119, 175–181. [Google Scholar] [CrossRef]
- Yardimci, A.C.; Arman, D. Prevalence and Antimicrobial Resistance of Bloodstream Infections Caused by ESKAPEEc Pathogens: A Five-Year Analysis. Jundishapur J. Microbiol. 2022, 31, 15. [Google Scholar] [CrossRef]
- Morrissey, I.; Hackel, M.; Badal, R.; Bouchillon, S.; Hawser, S.; Biedenbach, D. A Review of Ten Years of the Study for Monitoring Antimicrobial Resistance Trends (SMART) from 2002 to 2011. Pharmaceuticals 2013, 6, 1335–1346. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, P.W.; Sax, H.; Wolfensberger, A.; Clack, L.; Kuster, S.P.; Swissnoso. The preventable proportion of healthcare-associated infections 2005–2016: Systematic review and meta-analysis. Infect. Control Hosp. Epidemiol. 2018, 39, 1277–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Q.X.; Yau, C.E.; Yaow, C.Y.L.; Lim, Y.L.; Xin, X.; Thumboo, J.; Fong, K.Y. Impact of COVID-19 on environmental services workers in healthcare settings: A scoping review. J. Hosp. Infect. 2022, 130, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Wee, L.E.I.; Conceicao, E.P.; Tan, J.Y.; Magesparan, K.D.; Amin, I.B.M.; Ismail, B.B.S.; Toh, H.X.; Jin, P.; Zhang, J.; Wee, E.G.L.; et al. Unintended consequences of infection prevention and control measures during COVID-19 pandemic. Am. J. Infect. Control 2021, 49, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Meda, M.; Gentry, V.; Reidy, P.; Garner, D. Unintended consequences of long-sleeved gowns in a critical care setting during the COVID-19 pandemic. J. Hosp. Infect. 2020, 106, 605–609. [Google Scholar] [CrossRef] [PubMed]
- Fakih, M.G.; Bufalino, A.; Sturm, L.; Huang, R.H.; Ottenbacher, A.; Saake, K.; Winegar, A.; Fogel, R.; Cacchione, J. Coronavirus disease 2019 (COVID-19) pandemic, central-line-associated bloodstream infection (CLABSI), and catheter-associated urinary tract infection (CAUTI): The urgent need to refocus on hardwiring prevention efforts. Infect. Control Hosp. Epidemiol. 2022, 43, 26–31. [Google Scholar] [CrossRef]
- Stangerup, M.; Hansen, M.B.; Hansen, R.; Sode, L.P.; Hesselbo, B.; Kostadinov, K.; Olesen, B.S.; Calum, H. Hand hygiene compliance of healthcare workers before and during the COVID-19 pandemic: A long-term follow-up study. Am. J. Infect. Control 2021, 49, 1118–1122. [Google Scholar] [CrossRef]
- Sandbøl, S.G.; Glassou, E.N.; Ellermann-Eriksen, S.; Haagerup, A. Hand hygiene compliance among healthcare workers before and during the COVID-19 pandemic. Am. J. Infect. Control 2022, 50, 719–723. [Google Scholar] [CrossRef]
- Lytras, T.; Tsiodras, S. Total patient load, regional disparities and in-hospital mortality of intubated COVID-19 patients in Greece, from September 2020 to May 2021. Scand J. Public Health 2022, 50, 671–675. [Google Scholar] [CrossRef]
- Hill, B. Changes to nurse-to-patient ratios in intensive care during the pandemic. Br. J. Nurs. 2020, 29, 1238–1240. [Google Scholar] [CrossRef]
- DeVoe, C.; Segal, M.R.; Wang, L.; Stanley, K.; Madera, S.; Fan, J.; Schouest, J.; Graham-Ojo, R.; Nichols, A.; Prasad, P.A.; et al. Increased rates of secondary bacterial infections, including Enterococcus bacteremia, in patients hospitalized with coronavirus disease 2019 (COVID-19). Infect. Control Hosp. Epidemiol. 2022, 43, 1416–1423. [Google Scholar] [CrossRef]
- Gottlieb, L.; Fridkin, S.K. It’s Hard to Measure Success While Caring for Surges in Coronavirus Disease 2019 (COVID-19) Hospitalizations. Clin. Infect. Dis. 2022, 74, 1755–1756. [Google Scholar] [CrossRef] [PubMed]
- Chughtai, A.A.; Chen, X.; Macintyre, C.R. Risk of self-contamination during doffing of personal protective equipment. Am. J. Infect. Control 2018, 46, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.C.H.; Farhanah, S.; Linn, K.Z.; Tang, Y.W.; Poon, C.Y.; Lim, A.Y.; Tan, H.R.; Binte Hamed, N.H.; Huan, X.; Puah, S.H.; et al. Nosocomial infections among COVID-19 patients: An analysis of intensive care unit surveillance data. Antimicrob Resist. Infect. Control 2021, 10, 119. [Google Scholar] [CrossRef] [PubMed]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; Group, C.W.; Jombart, T.; Procter, S.R.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Makris, D.; Artigas, A.; Bouchereau, M.; Lambiotte, F.; Metzelard, M.; Cuchet, P.; Boulle Geronimi, C.; et al. Relationship between SARS-CoV-2 infection and the incidence of ventilator-associated lower respiratory tract infections: A European multicenter cohort study. Intensive Care Med. 2021, 47, 188–198. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of Antimicrobial Consumption During the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef]
- Khan, S.; Hasan, S.S.; Bond, S.E.; Conway, B.R.; Aldeyab, M.A. Antimicrobial consumption in patients with COVID-19: A systematic review and meta-analysis. Expert. Rev. Anti. Infect. Ther. 2022, 20, 749–772. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influ. Other Respir Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Wang, Q.; Mei, H.; Zheng, H.; Liang, G.; She, X.; Liu, W. Fungal co-infection in COVID-19 patients: Evidence from a systematic review and meta-analysis. Aging 2021, 13, 7745–7757. [Google Scholar] [CrossRef] [PubMed]
- Bara, W.; Brun-Buisson, C.; Coignard, B.; Watier, L. Outpatient Antibiotic Prescriptions in France: Patients and Providers Characteristics and Impact of the COVID-19 Pandemic. Antibiotics 2022, 11, 643. [Google Scholar] [CrossRef] [PubMed]
- Hek, K.; Ramerman, L.; Weesie, Y.M.; Lambooij, A.C.; Lambert, M.; Heins, M.J.; Hendriksen, J.M.T.; Verheij, R.A.; Cals, J.W.L.; van Dijk, L. Antibiotic Prescribing in Dutch Daytime and Out-of-Hours General Practice during the COVID-19 Pandemic: A Retrospective Database Study. Antibiotics 2022, 11, 309. [Google Scholar] [CrossRef]
- Livermore, D.M. Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: Our worst nightmare? Clin. Infect. Dis. 2002, 34, 634–640. [Google Scholar] [CrossRef] [Green Version]
- Ul Mustafa, Z.; Salman, M.; Aldeyab, M.; Kow, C.S.; Hasan, S.S. Antimicrobial consumption among hospitalized patients with COVID-19 in Pakistan. SN Compr. Clin. Med. 2021, 3, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic, Z.M.; Folic, M.M.; Jankovic, S.M. Correlation between cefepime utilisation and Pseudomonas aeruginosa resistance rates to β-lactams and carbapenems in patients with healthcare-associated infections. J. Glob. Antimicrob. Resist. 2018, 13, 60–64. [Google Scholar] [CrossRef]
- Delgado-Rodríguez, M.; Bueno-Cavanillas, A.; López-Gigosos, R.; de Dios Luna-Castillo, J.; Guillén-Solvas, J.; Moreno-Abril, O.; Rodríguez-Tuñas, B.; Cueto-Espinar, A.; Rodríguez-Contreras, R.; Gálvez-Vargas, R.; et al. Hospital stay length as an effect modifier of other risk factors for nosocomial infection. Eur. J. Epidemiol. 1990, 6, 34–39. [Google Scholar] [CrossRef]
- Ramos, G.P.; Rocha, J.L.; Tuon, F.F. Seasonal humidity may influence Pseudomonas aeruginosa hospital-acquired infection rates. Int. J. Infect. Dis. 2013, 17, e757–e761. [Google Scholar] [CrossRef] [Green Version]
- Al-Hasan, M.N.; Wilson, J.W.; Lahr, B.D.; Eckel-Passow, J.E.; Baddour, L.M. Incidence of Pseudomonas aeruginosa bacteremia: A population-based study. Am. J. Med. 2008, 121, 702–708. [Google Scholar] [CrossRef] [Green Version]
- Vendrik, K.E.W.; Baktash, A.; Goeman, J.J.; Harmanus, C.; Notermans, D.W.; de Greeff, S.C.; Kuijper, E.J.; Cdifficile surveillance study group. Comparison of trends in Clostridioides difficile infections in hospitalised patients during the first and second waves of the COVID-19 pandemic: A retrospective sentinel surveillance study. Lancet Reg. Health Eur. 2022, 19, 100424. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.I.; Kim, S.H.; Kim, H.B.; Park, S.W.; Choe, Y.J.; Oh, M.D.; Kim, E.C.; Choe, K.W. Pseudomonas aeruginosa bacteremia: Risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin. Infect. Dis. 2003, 37, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Medline | |
| 1 | (Incidence or surveillance).ti,ab. or exp “incidence”/ |
| 2 | (pseudomonas aeruginosa or PAE).ti,ab. or exp “pseudomonas aeruginosa”/ |
| 3 | 1 and 2 |
| 4 | limit 3 to (english language and year = “2019 to 2023”) |
| EMBASE | |
| 1 | Incidence:ti,ab OR surveillance:ti,ab OR ‘incidence’/exp |
| 2 | ‘pseudomonas aeruginosis’:ti,ab OR ‘pseudomonas aeruginosa’/exp OR ‘pae’:ti,ab |
| 3 | #1 AND #2 |
| 4 | #1 AND #2 AND [English]/lim AND [2019 to 2023]/py |
| Cochrane Database | |
| #1 | (incidence or surveillance):ti,ab,kw AND (“pseudomonas aeruginosa” or PAE):ti,ab,kw |
| #2 | Incidence or surveillance |
| #3 | (incidence or surveillance):ti,ab,kw |
| #4 | MeSH descriptor: [Incidence] explode all trees |
| #5 | MeSH descriptor: [Pseudomonas aeruginosa] explode all trees |
| #6 | (pseudomonas aeruginosa OR PAE):ti,ab,kw |
| #7 | #5 OR #6 |
| #8 | #5 AND #6 |
| #9 | #3 OR #4 |
| #10 | #7 AND #9 |
| Study (Year) | Country | Setting | Time Periods Compared | Key Findings |
|---|---|---|---|---|
| Amarsy, 2022 [19] | France | Multihospital institution | Jan–Apr 2019 and Jan–Apr 2020 |
|
| Despotovic, 2022 [25] | Serbia | Adult ICU, single-center | Apr 2019–Apr 2021 |
|
| Hirabayashi, 2022 [20] | Japan | 1300 hospitals with ≥200 beds | Jan–Sep 2019 and Jan–Sep 2020 |
|
| İpek, 2022 [21] | Turkey | Paediatric ICU, single-center | Apr–Sep 2019 and Apr–Sep 2020 |
|
| Meschiari, 2022 [26] | Italy | University hospital, single-center | Jan 2015–Feb 2020 and Mar 2020–Nov 2021 |
|
| Shbaklo, 2022 [27] | Italy | Tertiary hospital, single-center | Aug 2019–Feb 2020 and Feb 2020–Mar 2021 |
|
| Sloot, 2022 [28] | England | NHS acute trusts | Aug 2020 and Feb 2021 |
|
| Yardimci, 2022 [29] | Turkey | Tertiary hospital, single-center | Jan 2016–Dec 2020 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, Q.X.; Ong, N.Y.; Lee, D.Y.X.; Yau, C.E.; Lim, Y.L.; Kwa, A.L.H.; Tan, B.H. Trends in Pseudomonas aeruginosa (P. aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review. Antibiotics 2023, 12, 409. https://doi.org/10.3390/antibiotics12020409
Ng QX, Ong NY, Lee DYX, Yau CE, Lim YL, Kwa ALH, Tan BH. Trends in Pseudomonas aeruginosa (P. aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review. Antibiotics. 2023; 12(2):409. https://doi.org/10.3390/antibiotics12020409
Chicago/Turabian StyleNg, Qin Xiang, Natasha Yixuan Ong, Dawn Yi Xin Lee, Chun En Yau, Yu Liang Lim, Andrea Lay Hoon Kwa, and Ban Hock Tan. 2023. "Trends in Pseudomonas aeruginosa (P. aeruginosa) Bacteremia during the COVID-19 Pandemic: A Systematic Review" Antibiotics 12, no. 2: 409. https://doi.org/10.3390/antibiotics12020409