
Evidence-Based Treatment of Pseudomonas aeruginosa Infections: A Critical Reappraisal

 , and
, and
Abstract
:1. Introduction
2. Search Strategy and Design of the Review
3. Pseudomonas aeruginosa Information Path: Walking in the Right Direction
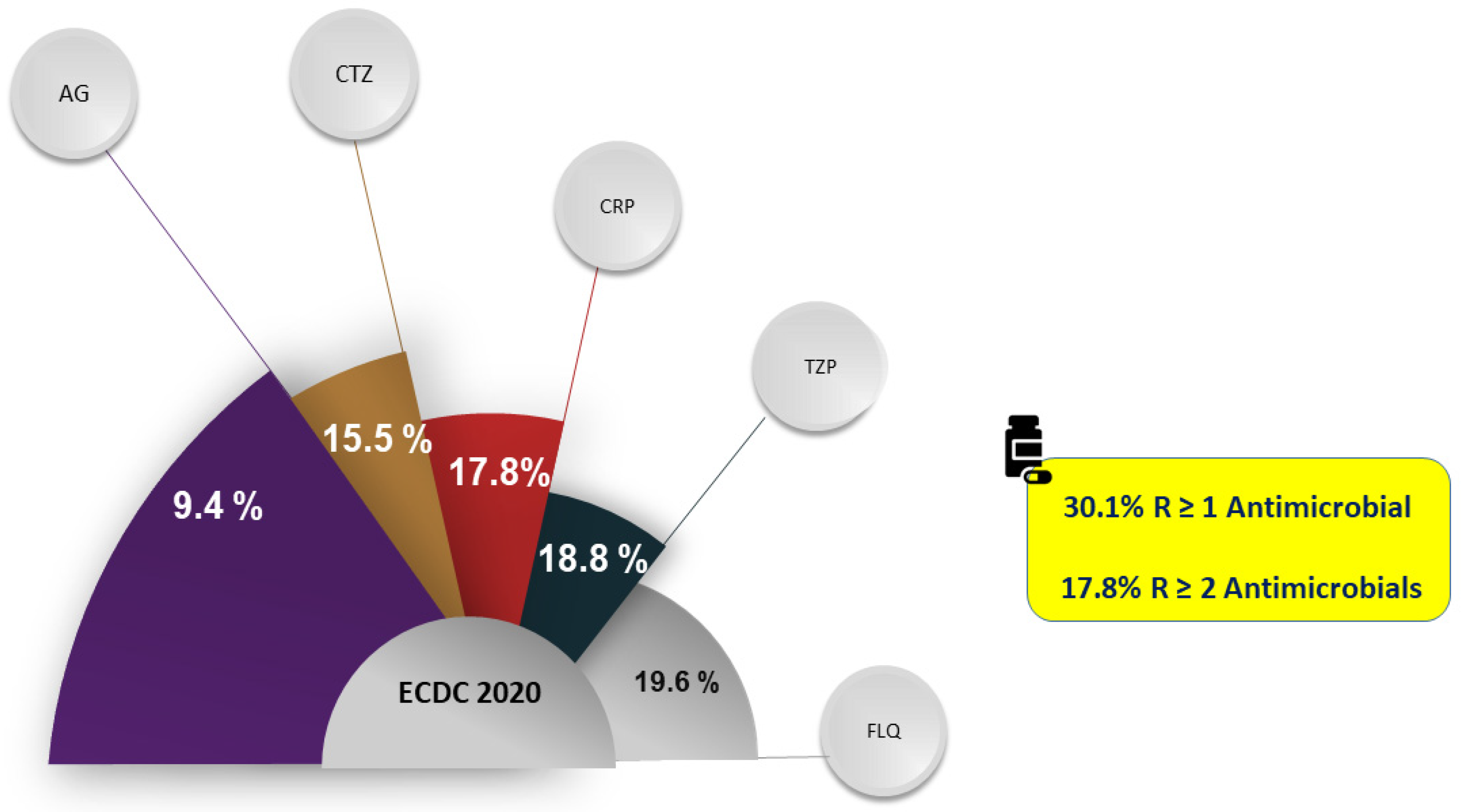
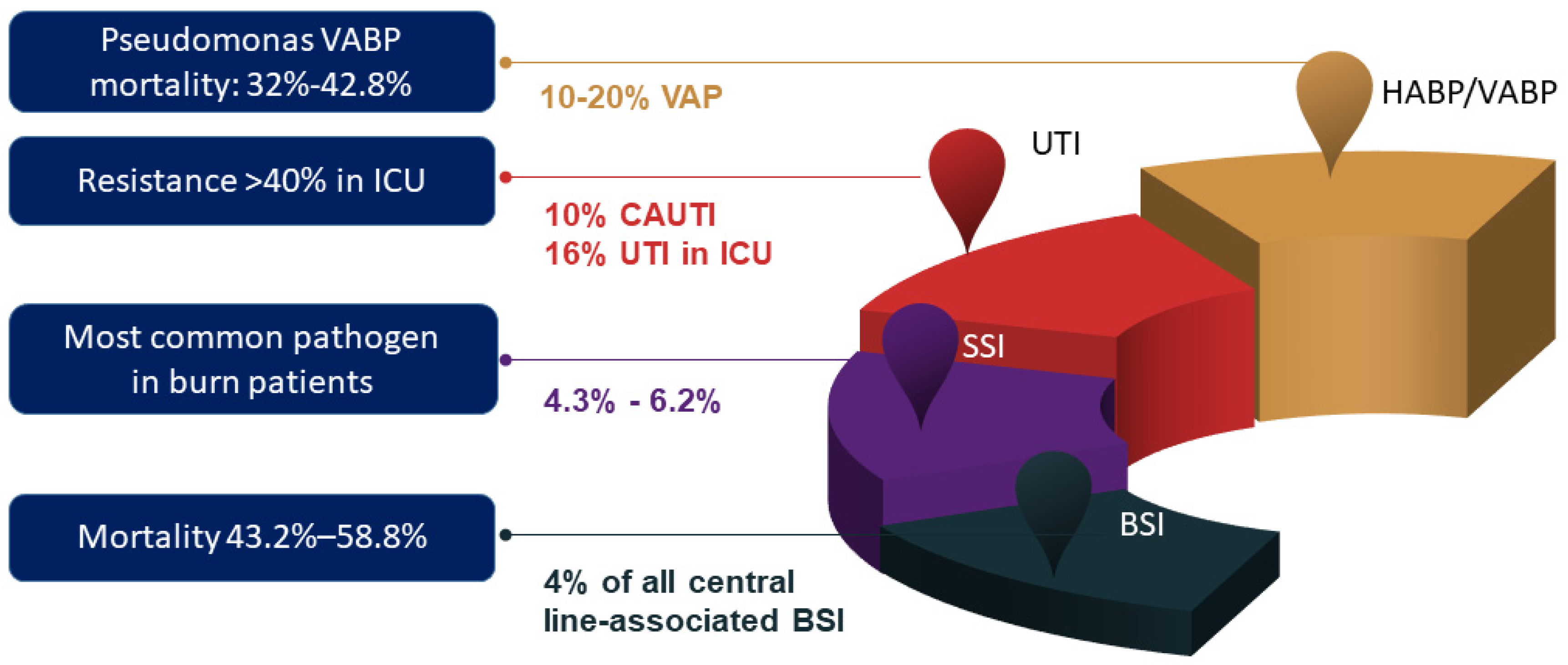
3.1. Resistance Patterns and Infection Syndromes
3.2. P. aeruginosa Diagnosis
3.2.1. Planktonic form: Bacterial Identification and Antibiotic Susceptibility Testing
3.2.2. Sessile form: Biofilm Detection
3.3. Risk Factors for P. aeruginosa/Resistant P. aeruginosa Infection
3.4. Major Resistance Mechanisms
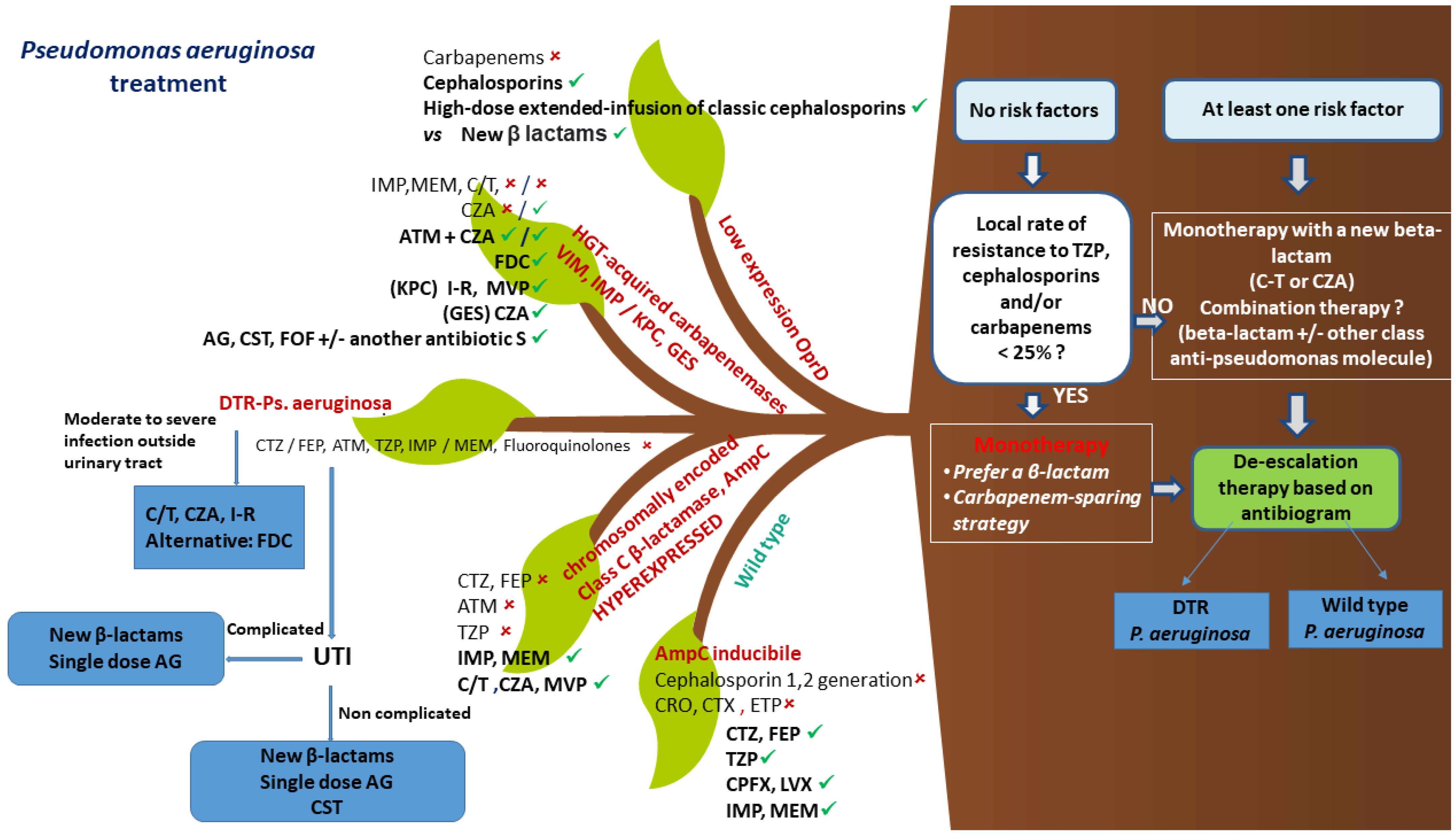
3.5. Treatment
3.5.1. Empirical Treatment
3.5.2. Combination Therapy or Monotherapy
3.5.3. Definitive Treatment after AST Results
Wild-Type Pseudomonas aeruginosa
Specific Antibiotic Class, Possible Applications, and Resistance Scenarios
High MIC of Conventional Antipseudomonal Beta Lactams
Resistance to Carbapenems with Maintained Susceptibility to Cephalosporins
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics. 2017. Available online: http://www.who.int/medicines/publications/WHO-PPL-Short_Summary_25Feb-ET_NM_WHO.pdf (accessed on 1 January 2023).
- Rice, L.B. Federal Funding for the Study of Antimicrobial Resistance in Nosocomial Pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Eurosurveillance 2018, 23, 1800516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vincent, J.-L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; Machado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.D.S.; Crozatti, M.T.L.; da Silva, A.A.; Macedo, R.S.; Machado, A.M.D.O.; Silva, A.T.D.A. Pseudomonas aeruginosa in the ICU: Prevalence, resistance profile, and antimicrobial consumption. Rev. Soc. Bras. Med. Trop. 2020, 53, e20180498. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States. 2019. Available online: https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pd (accessed on 1 January 2023).
- Nathwani, D.; Raman, G.; Sulham, K.; Gavaghan, M.; Menon, V. Clinical and economic consequences of hospital-acquired resistant and multidrug-resistant Pseudomonas aeruginosa infections: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2014, 3, 32. [Google Scholar] [CrossRef] [Green Version]
- Hirsch, E.B.; Tam, V.H. Impact of multidrug-resistant Pseudomonas aeruginosa infection on patient outcomes. Expert Rev. Pharm. Outcomes Res. 2010, 10, 441–451. [Google Scholar] [CrossRef] [Green Version]
- Matos, E.C.O.D.; Andriolo, R.B.; Rodrigues, Y.C.; Lima, P.D.L.D.; Carneiro, I.C.D.R.S.; Lima, K.V.B. Mortality in patients with multidrug-resistant Pseudomonas aeruginosa infections: A meta-analysis. Rev. Soc. Bras. Med. Trop. 2018, 51, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [Green Version]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [Green Version]
- ECDC. Antimicrobial Resistance Surveillance in EUROPE 2020 Data. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Joint-WHO-ECDC-AMR-report-2022.pdf (accessed on 7 January 2023).
- Reynolds, D.; Kollef, M. The Epidemiology and Pathogenesis and Treatment of Pseudomonas aeruginosa Infections: An Update. Drugs 2021, 81, 2117–2131. [Google Scholar] [CrossRef]
- Morin, C.D.; Déziel, E.; Gauthier, J.; Levesque, R.C.; Lau, G.W. An Organ System-Based Synopsis of Pseudomonas aeruginosa Virulence. Virulence 2021, 12, 1469–1507. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Andini, R.; Agrusta, F.; Iossa, D.; Mattucci, I.; Bernardo, M.; Utili, R. Infective endocarditis due to multidrug resistant gram-negative bacilli: Single centre experience over 5years. Eur. J. Intern. Med. 2014, 25, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Tiseo, G.; Durante-Mangoni, E.; Ravasio, V.; Barbaro, F.; Ursi, M.P.; Pasticci, M.B.; Bassetti, M.; Grossi, P.; Venditti, M.; et al. Risk Factors and Outcomes of Endocarditis Due to Non-HACEK Gram-Negative Bacilli: Data from the Prospective Multicenter Italian Endocarditis Study Cohort. Antimicrob. Agents Chemother. 2018, 62, e02208-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hombach, M.; Zbinden, R.; Böttger, E.C. Standardisation of disk diffusion results for antibiotic susceptibility testing using the sirscan automated zone reader. BMC Microbiol. 2013, 13, 225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute. Performance and Standards for Antimicrobial Susceptibility Testing. Available online: https://www.nih.org.pk/wp-content/uploads/2021/02/CLSI-2020.pdf (accessed on 10 January 2023).
- Lavano, M.A.; Foglia, F.; Della Rocca, M.T.; Folliero, V.; Zannella, C.; Crudele, V.; Boccia, G.; Franci, G.; Finamore, E.; Galdiero, M. Epidemiology of Multi and Extensively Drug Resistance Pseudomonas Aeruginosa Infections from University Hospital “Luigi Vanvitelli”. J. Community Med. Public Health 2020, 4, 199. [Google Scholar]
- European Committee on Antimicrobial Susceptibility Testing. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_13.0_Breakpoint_Tables.pdf (accessed on 7 January 2023).
- Daragon, B.; Fournier, D.; Plésiat, P.; Jeannot, K. Performance of disc diffusion, MIC gradient tests and Vitek 2 for ceftolozane/tazobactam and ceftazidime/avibactam susceptibility testing of Pseudomonas aeruginosa. J. Antimicrob. Chemother. 2021, 76, 2586–2592. [Google Scholar] [CrossRef]
- Dwivedi, H.P.; Franklin, S.; Chandrasekaran, S.; Garner, O.; Traczewski, M.M.; Beasley, D.; Procop, G.W.; Tuohy, M.; Wilson, D.; Bala, Y.; et al. Multicenter Clinical Evaluation of Vitek 2 Meropenem-Vaborbactam for Susceptibility Testing of Enterobacterales and Pseudomonas aeruginosa. J. Clin. Microbiol. 2022, 60, e0161021. [Google Scholar] [CrossRef]
- Jean, S.; Garrett, S.; Anglade, C.; Bridon, L.; Davies, L.; Garner, O.B.; Richards, J.; Wallace, M.; Wootton, M.; Burnham, C.-A.D. Multicenter Clinical Evaluation of Etest Meropenem-Vaborbactam (bioMérieux) for Susceptibility Testing of Enterobacterales (Enterobacteriaceae) and Pseudomonas aeruginosa. J. Clin. Microbiol. 2019, 58, e01205-19. [Google Scholar] [CrossRef]
- Devoos, L.; Biguenet, A.; Rousselot, J.; Bour, M.; Plésiat, P.; Fournier, D.; Jeannot, K. Performance of discs, sensititre EUMDROXF microplates and MTS gradient strips for the determination of the susceptibility of multidrug-resistant Pseudomonas aeruginosa to cefiderocol. Clin. Microbiol. Infect. 2022. [Google Scholar] [CrossRef]
- Tan, T.Y.; Ng, S.Y. Comparison of Etest, Vitek and agar dilution for susceptibility testing of colistin. Clin. Microbiol. Infect. 2007, 13, 541–544. [Google Scholar] [CrossRef] [Green Version]
- Matuschek, E.; Åhman, J.; Webster, C.; Kahlmeter, G. Antimicrobial susceptibility testing of colistin—Evaluation of seven commercial MIC products against standard broth microdilution for Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter spp. Clin. Microbiol. Infect. 2018, 24, 865–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing. On Recent Changes in Clinical Microbiology Susceptibility Reports—New Interpretation of Susceptibility Categories S, I and R. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Guidance_documents/To_clinical_colleagues_on_recent_changes_in_clinical_microbiology_susceptibility_reports_9_July2021.pdf (accessed on 5 February 2023).
- The European Committee on Antimicrobial Susceptibility Testing. Clinical Breakpoints—Bacteria (v 9.0). 2019. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf (accessed on 5 February 2023).
- Davey, M.E.; O’Toole, G.A. Microbial Biofilms: From Ecology to Molecular Genetics. Microbiol. Mol. Biol. Rev. 2000, 64, 847–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasamiravaka, T.; Labtani, Q.; Duez, P.; El Jaziri, M. The Formation of Biofilms by Pseudomonas aeruginosa: A Review of the Natural and Synthetic Compounds Interfering with Control Mechanisms. Biomed Res. Int. 2015, 2015, 759348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghafoor, A.; Hay, I.D.; Rehm, B.H.A. Role of Exopolysaccharides in Pseudomonas aeruginosa Biofilm Formation and Architecture. Appl. Environ. Microbiol. 2011, 77, 5238–5246. [Google Scholar] [CrossRef] [Green Version]
- Leid, J.G. Bacterial biofilms resist key host defenses. Microbe 2009, 4, 66–70. [Google Scholar]
- Page, M.G.; Heim, J. Prospects for the next anti-Pseudomonas drug. Curr. Opin. Pharmacol. 2009, 9, 558–565. [Google Scholar] [CrossRef]
- Watnick, P.; Kolter, R. Biofilm, city of microbes. J. Bacteriol. 2000, 182, 2675–2679. [Google Scholar] [CrossRef] [Green Version]
- Flemming, H.-C.; Neu, T.R.; Wozniak, D.J. The EPS matrix: The “house of biofilm cells”. J. Bacteriol. 2007, 189, 7945–7947. [Google Scholar] [CrossRef] [Green Version]
- Donlan, R.M.; Costerton, J.W. Biofilms: Survival Mechanisms of Clinically Relevant Microorganisms. Clin. Microbiol. Rev. 2002, 15, 167–193. [Google Scholar] [CrossRef] [Green Version]
- Ghannoum, M.; O’Toole, G.A. Microbial Biofilms; ASM Press: Washington, DC, USA, 2004. [Google Scholar]
- Haussler, S.; Fuqua, C. Biofilms 2012: New Discoveries and Significant Wrinkles in a Dynamic Field. J. Bacteriol. 2013, 195, 2947–2958. [Google Scholar] [CrossRef] [Green Version]
- Castro, J.; França, A.; Bradwell, K.R.; Serrano, M.G.; Jefferson, K.K.; Cerca, N. Comparative transcriptomic analysis of Gardnerella vaginalis biofilms vs. planktonic cultures using RNA-seq. NPJ Biofilms Microbiomes 2017, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, S.M.; Penstoft, L.N.; Nørskov-Lauritsen, N. Motility, Biofilm Formation and Antimicrobial Efflux of Sessile and Planktonic Cells of Achromobacter xylosoxidans. Pathogens 2019, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoyle, B.D.; Costerton, J.W. Bacterial resistance to antibiotics: The role of biofilms. Prog. Drug Res. 1991, 37, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Folliero, V.; Franci, G.; Dell’Annunziata, F.; Giugliano, R.; Foglia, F.; Sperlongano, R.; De Filippis, A.; Finamore, E.; Galdiero, M. Evaluation of Antibiotic Resistance and Biofilm Production among Clinical Strain Isolated from Medical Devices. Int. J. Microbiol. 2021, 2021, 9033278. [Google Scholar] [CrossRef] [PubMed]
- Neopane, P.; Nepal, H.P.; Shrestha, R.; Uehara, O.; Abiko, Y. In vitro biofilm formation by Staphylococcus aureus isolated from wounds of hospital-admitted patients and their association with antimicrobial resistance. Int. J. Gen. Med. 2018, 11, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Vuotto, C.; Longo, F.; Pascolini, C.; Donelli, G.; Balice, M.; Libori, M.; Tiracchia, V.; Salvia, A.; Varaldo, P. Biofilm formation and antibiotic resistance in Klebsiella pneumoniaeurinary strains. J. Appl. Microbiol. 2017, 123, 1003–1018. [Google Scholar] [CrossRef]
- Hassan, A.; Usman, J.; Kaleem, F.; Omair, M.; Khalid, A.; Iqbal, M. Evaluation of different detection methods of biofilm formation in the clinical isolates. Braz. J. Infect. Dis. 2011, 15, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Lima, J.L.D.C.; Alves, L.R.; Da Paz, J.N.P.; Rabelo, M.A.; Maciel, M.A.V.; De Morais, M.M.C. Analysis of biofilm production by clinical isolates of Pseudomonas aeruginosa from patients with ventilator-associated pneumonia. Rev. Bras. Ter. Intensiv. 2017, 29, 310–316. [Google Scholar] [CrossRef]
- Silva, N.; Marques, L.; Röder, D. Diagnosis of biofilm infections: Current methods used, challenges and perspectives for the future. J. Appl. Microbiol. 2021, 131, 2148–2160. [Google Scholar] [CrossRef]
- Thi, M.; Wibowo, D.; Rehm, B. Pseudomonas aeruginosa Biofilms. Int. J. Mol. Sci. 2020, 21, 8671. [Google Scholar] [CrossRef]
- Gellatly, S.L.; Hancock, R.E. Pseudomonas aeruginosa: New insights into pathogenesis and host defenses. Pathog. Dis. 2013, 67, 159–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restrepo, M.I.; Babu, B.L.; Reyes, L.F.; Chalmers, J.D.; Soni, N.J.; Sibila, O.; Faverio, P.; Cilloniz, C.; Rodriguez-Cintron, W.; Aliberti, S. Burden and risk factors for Pseudomonas aeruginosa community-acquired pneumonia: A multinational point prevalence study of hospitalised patients. Eur. Respir. J. 2018, 52, 1701190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rello, J.; Allegri, C.; Rodriguez, A.; Vidaur, L.; Sirgo, G.; Gomez, F.; Agbaht, K.; Pobo, A.; Diaz, E. Risk Factors for Ventilator-associated Pneumonia by Pseudomonas aeruginosa in Presence of Recent Antibiotic Exposure. Anesthesiology 2006, 105, 709–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, C.M.; Kutsogiannis, J.; Muscedere, J.; Cook, D.; Dodek, P.; Day, A.G.; Heyland, D.K. Ventilator-associated pneumonia caused by multidrug-resistant organisms or Pseudomonas aeruginosa: Prevalence, incidence, risk factors, and outcomes. J. Crit. Care 2008, 23, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Avendano, E.E.; Chan, J.; Merchant, S.; Puzniak, L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2018, 7, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merchant, S.; Proudfoot, E.M.; Quadri, H.N.; McElroy, H.J.; Wright, W.R.; Gupta, A.; Sarpong, E.M. Risk factors for Pseudomonas aeruginosa infections in Asia-Pacific and consequences of inappropriate initial antimicrobial therapy: A systematic literature review and meta-analysis. J. Glob. Antimicrob. Resist. 2018, 14, 33–44. [Google Scholar] [CrossRef]
- Aloush, V.; Navon-Venezia, S.; Seigman-Igra, Y.; Cabili, S.; Carmeli, Y. Multidrug-Resistant Pseudomonas aeruginosa: Risk Factors and Clinical Impact. Antimicrob. Agents Chemother. 2006, 50, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Paramythiotou, E.; Lucet, J.-C.; Timsit, J.-F.; Vanjak, D.; Paugam-Burtz, C.; Trouillet, J.-L.; Belloc, S.; Kassis, N.; Karabinis, A.; Andremont, A. Acquisition of multidrug-resistant Pseudomonas aeruginosa in patients in intensive care units: Role of antibiotics with antipseudomonal activity. Clin. Infect. Dis. 2004, 38, 670–677. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, D.; Lieberman, D. Pseudomonal infections in patients with COPD: Epidemiology and management. Am. J. Respir. Med. 2003, 2, 459–468. [Google Scholar] [CrossRef]
- Harris, A.D.; Smith, D.; Johnson, J.A.; Bradham, D.D.; Roghmann, M.-C. Risk Factors for Imipenem-Resistant Pseudomonas aeruginosa among Hospitalized Patients. Clin. Infect. Dis. 2002, 34, 340–345. [Google Scholar] [CrossRef] [Green Version]
- Montero, M.M.; Sala, M.; Riú, M.; Belvis, F.; Salvado, M.; Grau, S.; Horcajada, J.P.; Alvarez-Lerma, F.; Terradas, R.; Orozco-Levi, M.; et al. Risk factors for multidrug-resistant Pseudomonas aeruginosa acquisition. Impact of antibiotic use in a double case–control study. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 29, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Baena, Z.R.; Giannella, M.; Manissero, D.; Rodríguez-Baño, J.; Viale, P.; Lopes, S.; Wilson, K.; McCool, R.; Longshaw, C. Risk factors for carbapenem-resistant Gram-negative bacterial infections: A systematic review. Clin. Microbiol. Infect. 2020, 27, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Patolia, S.; Abate, G.; Patel, N.; Patolia, S.; Frey, S. Risk factors and outcomes for multidrug-resistant Gram-negative bacilli bacteremia. Ther. Adv. Infect. Dis. 2017, 5, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Hamdan, A.S.; Alghamdi, A.A.; Alyousif, G.F.; Hamza, F.A.; Shafey, M.M.; AlAmri, A.M.; Sunki, A.A. Evaluating the Prevalence and the Risk Factors of Gram-Negative Multi-Drug Resistant Bacteria in Eastern Saudi Arabia. Infect. Drug Resist. 2022, 15, 475–490. [Google Scholar] [CrossRef]
- Karruli, A.; Boccia, F.; Gagliardi, M.; Patauner, F.; Ursi, M.P.; Sommese, P.; De Rosa, R.; Murino, P.; Ruocco, G.; Corcione, A.; et al. Multidrug-Resistant Infections and Outcome of Critically Ill Patients with Coronavirus Disease 2019: A Single Center Experience. Microb. Drug Resist. 2021, 27, 1167–1175. [Google Scholar] [CrossRef]
- Karruli, A.; de Cristofaro, J.; Andini, R.; Iossa, D.; Bernardo, M.; Amarelli, C.; Mattucci, I.; Zampino, R.; Zarrilli, R.; Durante-Mangoni, E. Risk Factors and Outcome of Multidrug-Resistant Infections after Heart Transplant: A Contemporary Single Center Experience. Microorganisms 2021, 9, 1210. [Google Scholar] [CrossRef]
- Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Pseudomonas aeruginosa in the healthcare facility setting. Rev. Med. Microbiol. 2021, 32, 169–175. [Google Scholar] [CrossRef]
- Morita, Y.; Tomida, J.; Kawamura, Y. Responses of Pseudomonas aeruginosa to antimicrobials. Front. Microbiol. 2014, 4, 422. [Google Scholar] [CrossRef] [Green Version]
- Livermore, D.M. Multiple Mechanisms of Antimicrobial Resistance in Pseudomonas aeruginosa: Our Worst Nightmare? Clin. Infect. Dis. 2002, 34, 634–640. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Rao, S.; Bansal, A.; Dang, S.; Gupta, S.; Gabrani, R. Pseudomonas aeruginosa biofilm: Potential therapeutic targets. Biologicals 2014, 42, 1–7. [Google Scholar] [CrossRef]
- Pachori, P.; Gothalwal, R.; Gandhi, P. Emergence of antibiotic resistance Pseudomonas aeruginosa in intensive care unit; a critical review. Genes Dis. 2019, 6, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Henrichfreise, B.; Wiegand, I.; Pfister, W.; Wiedemann, B. Resistance Mechanisms of Multiresistant Pseudomonas aeruginosa Strains from Germany and Correlation with Hypermutation. Antimicrob. Agents Chemother. 2007, 51, 4062–4070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, Z.; Raudonis, R.; Glick, B.R.; Lin, T.J.; Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol. Adv. 2019, 37, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Bert, F.; Branger, C.; Lambert-Zechovsky, N. Identification of PSE and OXA beta-lactamase genes in Pseudomonas aeruginosa using PCR-restriction fragment length polymorphism. J. Antimicrob. Chemother. 2002, 50, 11–18. [Google Scholar] [CrossRef]
- Ramirez, M.S.; Tolmasky, M.E. Aminoglycoside modifying enzymes. Drug Resist. Updat. 2010, 13, 151–171. [Google Scholar] [CrossRef] [Green Version]
- Memar, M.Y.; Pormehrali, R.; Alizadeh, N.; Ghotaslou, R.; Baghi, H.B. Colistin, an option for treatment of multiple drug resistant Pseudomonas aeruginosa. Physiol. Pharmacol. 2016, 20, 130–136. [Google Scholar]
- Iregui, M.; Ward, S.; Sherman, G.; Fraser, V.J.; Kollef, M.H. Clinical Importance of Delays in the Initiation of Appropriate Antibiotic Treatment for Ventilator-Associated Pneumonia. Chest 2002, 122, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Mesaros, N.; Nordmann, P.; Plésiat, P.; Roussel-Delvallez, M.; Van Eldere, J.; Glupczynski, Y.; Van Laethem, Y.; Jacobs, F.; Lebecque, P.; Malfroot, A.; et al. Pseudomonas aeruginosa: Resistance and therapeutic options at the turn of the new millennium. Clin. Microbiol. Infect. 2007, 13, 560–578. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, M.; Vena, A.; Croxatto, A.; Righi, E.; Guery, B. How to manage Pseudomonas aeruginosa infections. Drugs Context 2018, 7, 212527. [Google Scholar] [CrossRef]
- Paul, M.; Leibovici, L. Editorial commentary: Combination therapy for Pseudomonas aeruginosa bacteremia: Where do we stand? Clin. Infect. Dis. 2013, 57, 217–220. [Google Scholar] [CrossRef] [Green Version]
- Thu, P.N.T.; Huong, M.N.T.; Thi, N.T.; Thanh, H.N.; Minh, K.P. Combination antibiotic therapy versus monotherapy in the treatment of acute exacerbations of chronic obstructive pulmonary disease: An open-label randomized trial. BMC Infect. Dis. 2021, 21, 1019. [Google Scholar] [CrossRef]
- Babich, T.; Naucler, P.; Valik, J.K.; Giske, C.G.; Benito, N.; Cardona, R.; Rivera, A.; Pulcini, C.; Fattah, M.A.; Haquin, J.; et al. Combination versus monotherapy as definitive treatment for Pseudomonas aeruginosa bacteraemia: A multicentre retrospective observational cohort study. J. Antimicrob. Chemother. 2021, 76, 2172–2181. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-Y.; Park, H.J.; Moon, S.M.; Park, K.-H.; Chong, Y.P.; Kim, M.-N.; Kim, S.-H.; Lee, S.-O.; Kim, Y.S.; Woo, J.H.; et al. Impact of adequate empirical combination therapy on mortality from bacteremic Pseudomonas aeruginosa pneumonia. BMC Infect. Dis. 2012, 12, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, D.; Jabbour, J.-F.; Kanj, S.S. Current choices of antibiotic treatment for Pseudomonas aeruginosa infections. Curr. Opin. Infect. Dis. 2020, 33, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2020, 72, e169–e183. [Google Scholar] [CrossRef]
- Farhan, S.M.; Raafat, M.; Abourehab, M.A.S.; El-Baky, R.M.A.; Abdalla, S.; El-Gendy, A.O.; Azmy, A.F. Effect of Imipenem and Amikacin Combination against Multi-Drug Resistant Pseudomonas aeruginosa. Antibiotics 2021, 10, 1429. [Google Scholar] [CrossRef] [PubMed]
- Yadav, R.; Bulitta, J.B.; Nation, R.L.; Landersdorfer, C.B. Optimization of Synergistic Combination Regimens against Carbapenem- and Aminoglycoside-Resistant Clinical Pseudomonas aeruginosa Isolates via Mechanism-Based Pharmacokinetic/Pharmacodynamic Modeling. Antimicrob. Agents Chemother. 2017, 61, e01011-16. [Google Scholar] [CrossRef] [Green Version]
- Deelen, J.T.; Rottier, W.; Buiting, A.; Dorigo-Zetsma, J.; Kluytmans, J.; van der Linden, P.; Thijsen, S.; Vlaminckx, B.; Weersink, A.; Ammerlaan, H.; et al. Short-course aminoglycosides as adjunctive empirical therapy in patients with Gram-negative bloodstream infection, a cohort study. Clin. Microbiol. Infect. 2021, 27, 269–275. [Google Scholar] [CrossRef]
- Papst, L.; Beović, B.; Pulcini, C.; Durante-Mangoni, E.; Rodríguez-Baño, J.; Kaye, K.S.; Daikos, G.L.; Raka, L.; Paul, M.; on behalf ofESGAP, ESGBIS, ESGIE and the CRGNB Treatment Survey Study Group. Antibiotic treatment of infections caused by carbapenem-resistant Gram-negative bacilli: An international ESCMID cross-sectional survey among infectious diseases specialists practicing in large hospitals. Clin. Microbiol. Infect. 2018, 24, 1070–1076. [Google Scholar] [CrossRef] [Green Version]
- Coppola, N.; Maraolo, A.E.; Onorato, L.; Scotto, R.; Calò, F.; Atripaldi, L.; Borrelli, A.; Corcione, A.; De Cristofaro, M.G.; Durante-Mangoni, E.; et al. Epidemiology, Mechanisms of Resistance and Treatment Algorithm for Infections Due to Carbapenem-Resistant Gram-Negative Bacteria: An Expert Panel Opinion. Antibiotics 2022, 11, 1263. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2022 Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin. Infect. Dis. 2022, 75, 187–212. [Google Scholar] [CrossRef] [PubMed]
- Young, O.; Psirides, A. Wellington ICU Drug Manual. 2020. Available online: https://drug.wellingtonicu.com/PDF/WellingtonICUDrugManual.pdf (accessed on 10 January 2023).
- Köhler, T.; Michea-Hamzehpour, M.; Plesiat, P.; Kahr, A.L.; Pechere, J.C. Differential selection of multi drug efflux systems by quinolones in Pseudomonas aeruginosa. Antimicrob. Agents Chemother. 1997, 41, 2540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante-Mangoni, E.; Grammatikos, A.; Utili, R.; Falagas, M.E. Do we still need the aminoglycosides? Int. J. Antimicrob. Agents 2009, 33, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, T.; Hempstead, S.E.; Brady, C.; Cannon, C.L.; Clark, K.; Condren, M.E.; Guill, M.F.; Guillerman, R.P.; Leone, C.G.; Maguiness, K.; et al. Clinical Practice Guidelines From the Cystic Fibrosis Foundation for Preschoolers with Cystic Fibrosis. Pediatrics 2016, 137, e20151784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaeer, K.M.; Zmarlicka, M.T.; Chahine, E.B.; Piccicacco, N.; Cho, J.C. Plazomicin: A next-generation aminoglycoside. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2019, 39, 77–93. [Google Scholar] [CrossRef] [Green Version]
- Durante-Mangoni, E.; Andini, R.; Signoriello, S.; Cavezza, G.; Murino, P.; Buono, S.; De Cristofaro, M.; Taglialatela, C.; Bassetti, M.; Malacarne, P.; et al. Acute kidney injury during colistin therapy: A prospective study in patients with extensively-drug resistant Acinetobacter baumannii infections. Clin. Microbiol. Infect. 2016, 22, 984–989. [Google Scholar] [CrossRef]
- Florescu, D.F.; Qiu, F.; McCartan, M.A.; Mindru, C.; Fey, P.D.; Kalil, A.C. What Is the Efficacy and Safety of Colistin for the Treatment of Ventilator-Associated Pneumonia? A Systematic Review and Meta-Regression. Clin. Infect. Dis. 2012, 54, 670–680. [Google Scholar] [CrossRef]
- Boisson, M.; Jacobs, M.; Grégoire, N.; Gobin, P.; Marchand, S.; Couet, W.; Mimoz, O. Comparison of intrapulmonary and systemic pharmacokinetics of colistin methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically ill patients. Antimicrob. Agents Chemother. 2014, 58, 7331–7339. [Google Scholar] [CrossRef] [Green Version]
- Zak-Doron, Y.; Benattar, Y.D.; Pfeffer, I.; Daikos, G.L.; Skiada, A.; Antoniadou, A.; Durante-Mangoni, E.; Andini, R.; Cavezza, G.; Leibovici, L.; et al. The Association Between Empirical Antibiotic Treatment and Mortality in Severe Infections Caused by Carbapenem-resistant Gram-negative Bacteria: A Prospective Study. Clin. Infect. Dis. 2018, 67, 1815–1823. [Google Scholar] [CrossRef]
- Nutman, A.; Lellouche, J.; Temkin, E.; Daikos, G.; Skiada, A.; Durante-Mangoni, E.; Dishon-Benattar, Y.; Bitterman, R.; Yahav, D.; Daitch, V.; et al. Colistin plus meropenem for carbapenem-resistant Gram-negative infections: In vitro synergism is not associated with better clinical outcomes. Clin. Microbiol. Infect. 2020, 26, 1185–1191. [Google Scholar] [CrossRef]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: An open-label, randomised controlled trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, Y.; Leibovici, L.; Yahav, D.; Eliakim-Raz, N.; Daikos, G.L.; Skiada, A.; Antoniadou, A.; Carmeli, Y.; Nutman, A.; Levi, I.; et al. Multicentre open-label randomised controlled trial to compare colistin alone with colistin plus meropenem for the treatment of severe infections caused by carbapenem-resistant Gram-negative infections (AIDA): A study protocol. BMJ Open 2016, 6, e009956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannouli, M.; Di Popolo, A.; Durante-Mangoni, E.; Bernardo, M.; Cuccurullo, S.; Amato, G.; Tripodi, M.-F.; Triassi, M.; Utili, R.; Zarrilli, R. Molecular epidemiology and mechanisms of rifampicin resistance in Acinetobacter baumannii isolates from Italy. Int. J. Antimicrob. Agents 2012, 39, 58–63. [Google Scholar] [CrossRef] [PubMed]
- MONUROL. Prescribing Information; Forest Pharmaceuticals, Inc.: St. Louis, MO, USA, 2007. Available online: www.accessdata.fda.gov/drugsatfda_docs/label/2008/050717s005lbl.pdf (accessed on 13 January 2023).
- Reffert, J.L.; Smith, W.J. Fosfomycin for the Treatment of Resistant Gram-Negative Bacterial Infections. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2014, 34, 845–857. [Google Scholar] [CrossRef]
- Mirakhur, A.; Gallagher, M.; Ledson, M.; Hart, C.; Walshaw, M. Fosfomycin therapy for multiresistant Pseudomonas aeruginosa in cystic fibrosis. J. Cyst. Fibros. 2003, 2, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Asuphon, O.; Montakantikul, P.; Houngsaitong, J.; Kiratisin, P.; Sonthisombat, P. Optimizing intravenous fosfomycin dosing in combination with carbapenems for treatment of Pseudomonas aeruginosa infections in critically ill patients based on pharmacokinetic/pharmacodynamic (PK/PD) simulation. Int. J. Infect. Dis. 2016, 50, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Kaye, K.S.; Rice, L.B.; Dane, A.L.; Stus, V.; Sagan, O.; Fedosiuk, E.; Das, A.F.; Skarinsky, D.; Eckburg, P.B.; Ellis-Grosse, E.J. Fosfomycin for Injection (ZTI-01) Versus Piperacillin-tazobactam for the Treatment of Complicated Urinary Tract Infection Including Acute Pyelonephritis: ZEUS, A Phase 2/3 Randomized Trial. Clin. Infect. Dis. 2019, 69, 2045–2056. [Google Scholar] [CrossRef] [Green Version]
- Coyne, A.J.K.; El Ghali, A.; Holger, D.; Rebold, N.; Rybak, M.J. Therapeutic Strategies for Emerging Multidrug-Resistant Pseudomonas aeruginosa. Infect. Dis. Ther. 2022, 11, 661–682. [Google Scholar] [CrossRef]
- Bauer, K.A.; West, J.E.; O’Brien, J.M.; Goff, D.A. Extended-Infusion Cefepime Reduces Mortality in Patients with Pseudomonas aeruginosa Infections. Antimicrob. Agents Chemother. 2013, 57, 2907–2912. [Google Scholar] [CrossRef] [Green Version]
- Lodise, T.P., Jr.; Lomaestro, B.; Drusano, G.L. Piperacillin-Tazobactam for Pseudomonas aeruginosa Infection: Clinical Implications of an Extended-Infusion Dosing Strategy. Clin. Infect. Dis. 2007, 44, 357–363. [Google Scholar] [CrossRef]
- Hong, D.J.; Bae, I.K.; Jang, I.-H.; Jeong, S.H.; Kang, H.-K.; Lee, K. Epidemiology and Characteristics of Metallo-β-Lactamase-Producing Pseudomonas aeruginosa. Infect. Chemother. 2015, 47, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Glen, K.A.; Lamont, I.L. β-lactam Resistance in Pseudomonas aeruginosa: Current Status, Future Prospects. Pathogens 2021, 10, 1638. [Google Scholar] [CrossRef]
- Karruli, A.; Massa, A.; Andini, R.; Marrazzo, T.; Ruocco, G.; Zampino, R.; Durante-Mangoni, E. Clinical efficacy and safety of cefiderocol for resistant Gram-negative infections: A real-life, single-centre experience. Int. J. Antimicrob. Agents 2023, 61, 106723. [Google Scholar] [CrossRef]
- Mauri, C.; Maraolo, A.E.; Di Bella, S.; Luzzaro, F.; Principe, L. The Revival of Aztreonam in Combination with Avibactam against Metallo-β-Lactamase-Producing Gram-Negatives: A Systematic Review of In Vitro Studies and Clinical Cases. Antibiotics 2021, 10, 1012. [Google Scholar] [CrossRef]
- Solomkin, J.; Hershberger, E.; Miller, B.; Popejoy, M.; Friedland, I.; Steenbergen, J.; Yoon, M.; Collins, S.; Yuan, G.; Barie, P.S.; et al. Ceftolozane/tazobactam plus metronidazole for complicated intra-abdominal infections in an era of multidrug resistance: Results from a randomized, double-blind, phase 3 trial (ASPECT-cIAI). Clin. Infect. Dis. 2015, 60, 1462–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagenlehner, F.M.; Umeh, O.; Steenbergen, J.; Yuan, G.; Darouiche, R.O.; Wagenlehner, F.M.; Umeh, O.; Steenbergen, J.; Yuan, G.; Darouiche, R.O. Ceftolozane-tazobactam compared with levofloxacin in the treatment of complicated urinary-tract infections, including pyelonephritis: A randomised, double-blind, phase 3 trial (ASPECT-cUTI). Lancet 2015, 385, 1949–1956. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Nováček, M.; Kivistik, U.; Réa-Neto, A.; Shime, N.; Martin-Loeches, I.; Timsit, J.-F.; Wunderink, R.G.; Bruno, C.J.; Huntington, J.A.; et al. Ceftolozane–tazobactam versus meropenem for treatment of nosocomial pneumonia (ASPECT-NP): A randomised, controlled, double-blind, phase 3, non-inferiority trial. Lancet Infect. Dis. 2019, 19, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.C.; Satlin, M.J.; Elabor, A.; Saraiya, N.; McCreary, E.K.; Molnar, E.; El-Beyrouty, C.; Jones, B.M.; Dixit, D.; Heil, E.L.; et al. Ceftolozane-Tazobactam for the Treatment of Multidrug-Resistant Pseudomonas aeruginosa Infections: A Multicenter Study. Open Forum Infect. Dis. 2018, 5, ofy280. [Google Scholar] [CrossRef]
- Parisio, E.M. Camarlinghi G Le Nuove Molecole Antibiotiche per il Trattamento Delle Infezioni da Batteri Gram-Negativi. Available online: https://www.infezioniobiettivozero.info/9-infection-control/125-le-nuove-molecole-antibiotiche-per-il-trattamento-delle-infezioni-da-batteri-gram-negativi (accessed on 11 January 2023).
- Fraile-Ribot, P.A.; Cabot, G.; Mulet, X.; Periañez, L.; Martín-Pena, M.L.; Juan, C.; Pérez, J.L.; Oliver, A. Mechanisms leading to in vivo ceftolozane/tazobactam resistance development during the treatment of infections caused by MDR Pseudomonas aeruginosa. J. Antimicrob. Chemother. 2017, 73, 658–663. [Google Scholar] [CrossRef] [Green Version]
- Gill, C.M.; Aktaþ, E.; Alfouzan, W.; Bourassa, L.; Brink, A.; Burnham, C.-A.D.; Canton, R.; Carmeli, Y.; Falcone, M.; Kiffer, C.; et al. The ERACE-PA Global Surveillance Program: Ceftolozane/tazobactam and Ceftazidime/avibactam in vitro Activity against a Global Collection of Carbapenem-resistant Pseudomonas aeruginosa. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 2533–2541. [Google Scholar] [CrossRef]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): A randomised, open-label, multicentre, pathogen-focused, descriptive, phase 3 trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Karruli, A.; Massa, A.; Bertolino, L.; Andini, R.; Sansone, P.; Dongiovanni, S.; Pace, M.C.; Pota, V.; Durante-Mangoni, E. Clinical Characteristics and Outcome of MDR/XDR Bacterial Infections in a Neuromuscular Semi-Intensive/Sub-Intensive Care Unit. Antibiotics 2022, 11, 1411. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Individual Antimicrobials Tested against P. aeruginosa | |||
|---|---|---|---|
| Phenotype | Resistant to at least 1 of the below compounds | ||
| Carbapenem-resistant | Imipenem-cilastatin | Meropenem | Doripenem |
| Cephalosporin-resistant | Ceftazidime | Cefepime | |
| Fluoroquinolone-resistant | Ciprofloxacin | Levofloxacin | |
| Aminoglycoside-resistant | Amikacin | Gentamycin | Tobramycin |
| Ureido penicillin-resistant | Piperacillin | Piperacillin-Tazobactam | |
| Traditional Antibiotics | EUCAST 2019 * | EUCAST 2023 ** | New Antibiotics | EUCAST 2019 * | EUCAST 2023 ** | ||||
|---|---|---|---|---|---|---|---|---|---|
| MIC Breakpoints | MIC Breakpoints | ||||||||
| S≤ | R> | S≤ | R> | S≤ | R> | S≤ | R> | ||
| Beta Lactams | |||||||||
| Cephalosporin | |||||||||
| Ceftazidime | 8 | 8 | 0.001 | 8 | Ceftazidime-Avibactam | 8 | 8 | 8 | 8 |
| Cefepime | 8 | 8 | 0.001 | 8 | Ceftolozane-Tazobactam | 4 | 4 | 4 | 4 |
| Cefiderocol | 2 | 2 | |||||||
| Ureidopenicillin | |||||||||
| Piperacillin/tazobactam | 16 | 16 | 0.001 | 16 | |||||
| Carbapenem | |||||||||
| Imipenem-cilastatin | 4 | 4 | 0.001 | 4 | Imipenem-Cilastatin-Relebactam | ||||
| Meropenem | 2 | 8 | 2 | 2/8 | Meropenem-Vaborbactam | 8 | 8 | 8 | 8 |
| Doripenem | 0.001 | 2 | |||||||
| Monobactam | |||||||||
| Aztreonam | 16 | 16 | 0.001 | 16 | Aztreonam-Avibactam | ||||
| Other antibiotics | |||||||||
| Polymixin | |||||||||
| Colistin | 2 | 2 | 4 | 4 | |||||
| Fluoroquinolones | |||||||||
| Ciprofloxacin | 0.5 | 0.5 | 0.001 | 0.5 | |||||
| Levofloxacin | 1 | 1 | 0.001 | 2 | |||||
| Aminoglycosides | |||||||||
| Gentamycin | 4 | 4 | IE | IE | Plazomicin | ||||
| Amikacin | 8 | 16 | 16 | 16 | |||||
| Tobramycin | 4 | 4 | 2 | 2 | |||||
| Fosfomycin | |||||||||
| Resistance Mechanisms | ||||
|---|---|---|---|---|
| Antibiotic class | Mechanism 1 | Mechanism 2 | Mechanism 3 | Mechanism 4 |
| Beta-lactams | chromosomal AmpC hyper-expression | OprM porin mutation or loss | OXA-1 & -2 enzyme production | MexXY efflux pump overexpression |
| Aminoglycosides | altered permeability | cytoplasm expression of aminoglycoside-modifying enzymes, such as aminoglycoside-2″-O-nucleotidyltransferase ANT (ANT 2″Ia) and aminoglycoside 4′-O-adenylyltransferase (ANT 4′-IIb | overexpression of MexXY efflux pumps | |
| Fluoroquinolones | gyrase (gyr A)—topoisomerase expression; (par C) mutations | altered permeability | efflux systems | |
| Carbapenems | OprD porin loss | MexXY efflux pump expression | beta-lactamase production | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karruli, A.; Catalini, C.; D’Amore, C.; Foglia, F.; Mari, F.; Harxhi, A.; Galdiero, M.; Durante-Mangoni, E. Evidence-Based Treatment of Pseudomonas aeruginosa Infections: A Critical Reappraisal. Antibiotics 2023, 12, 399. https://doi.org/10.3390/antibiotics12020399
Karruli A, Catalini C, D’Amore C, Foglia F, Mari F, Harxhi A, Galdiero M, Durante-Mangoni E. Evidence-Based Treatment of Pseudomonas aeruginosa Infections: A Critical Reappraisal. Antibiotics. 2023; 12(2):399. https://doi.org/10.3390/antibiotics12020399
Chicago/Turabian StyleKarruli, Arta, Christian Catalini, Chiara D’Amore, Francesco Foglia, Fabio Mari, Arjan Harxhi, Massimiliano Galdiero, and Emanuele Durante-Mangoni. 2023. "Evidence-Based Treatment of Pseudomonas aeruginosa Infections: A Critical Reappraisal" Antibiotics 12, no. 2: 399. https://doi.org/10.3390/antibiotics12020399