
Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern



Abstract
:1. Introduction
2. Methods
3. Results and Discussion
3.1. Evolution of Antibiotic Resistance in H. pylori over the Years
3.1.1. Amoxicillin
3.1.2. Metronidazole
3.1.3. Clarithromycin
3.1.4. Tetracycline
3.1.5. Levofloxacin
3.1.6. Double and Multidrug Resistance
3.2. Factors for Resistance Evolution
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kotilea, K.; Bontems, P.; Touati, E. Epidemiology, diagnosis and risk factors of Helicobacter pylori infection. Adv. Exp. Med. Biol. 2019, 1149, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.H.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M.H. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef]
- Violeta Filip, P.; Cuciureanu, D.; Sorina Diaconu, L.; Maria Vladareanu, A.; Silvia Pop, C. MALT lymphoma: Epidemiology, clinical diagnosis and treatment. J. Med. Life 2018, 11, 187–193. [Google Scholar] [CrossRef]
- Ailloud, F.; Estibariz, I.; Suerbaum, S. Evolved to vary: Genome and epigenome variation in the human pathogen Helicobacter pylori. FEMS Microbiol. Rev. 2021, 45, fuaa042. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhu, Y.; Lu, N.H. Recent progress in Helicobacter pylori treatment. Chin. Med. J. 2020, 133, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, R.; Zagari, R.M.; Zhang, S.; Saracco, G.M.; Moss, S.F. Pharmacological considerations and step-by-step proposal for the treatment of Helicobacter pylori infection in the year 2018. Minerva Gastroenterol. Dietol. 2018, 64, 310–321. [Google Scholar] [CrossRef]
- Graham, D.Y.; Dore, M.P.; Lu, H. Understanding treatment guidelines with bismuth and non-bismuth quadruple Helicobacter pylori eradication therapies. Expert. Rev. Anti Infect. Ther. 2018, 16, 679–687. [Google Scholar] [CrossRef]
- Zanotti, G.; Cendron, L. Structural aspects of Helicobacter pylori antibiotic resistance. Adv. Exp. Med. Biol. 2019, 1149, 227–241. [Google Scholar] [CrossRef]
- Fauzia, K.A.; Miftahussurur, M.; Syam, A.F.; Waskito, L.A.; Doohan, D.; Rezkitha, Y.A.A.; Matsumoto, T.; Tuan, V.P.; Akada, J.; Yonezawa, H.; et al. Biofilm formation and antibiotic resistance phenotype of Helicobacter pylori clinical isolates. Toxins 2020, 12, 473. [Google Scholar] [CrossRef]
- Tshibangu-Kabamba, E.; Yamaoka, Y. Helicobacter pylori infection and antibiotic resistance—From biology to clinical implications. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 613–629. [Google Scholar] [CrossRef]
- Boyanova, L.; Kandilarov, N.; Hadzhiyski, P.; Gergova, R.; Gergova, G.; Markovska, R. Increase in amoxicillin resistance in Helicobacter pylori from Bulgarian patients over 15 years. Diagn. Microbiol. Infect. Dis. 2022, 104, 115746. [Google Scholar] [CrossRef]
- Boyanova, L.; Gergova, G.; Evstatiev, I.; Spassova, Z.; Kandilarov, N.; Yaneva, P.; Markovska, R.; Mitov, I. Helicobacter pylori resistance to six antibiotics by two breakpoint systems and resistance evolution in Bulgaria. Infect. Dis. 2016, 48, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Matta, A.J.; Zambrano, D.C.; Martínez, Y.C.; Fernández, F.F. Point mutations in the glycosyltransferase domain of the pbp1a gene in amoxicillin-resistant Helicobacter pylori isolates. Rev. Gastroenterol. Mex. 2022. [Google Scholar] [CrossRef]
- Hsu, P.I.; Lin, P.C.; Graham, D.Y. Helicobacter pylori infection: A systemic review and meta-analysis. World J. Gastroenterol. 2015, 21, 12954–12962. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. Correction: ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2018, 113, 1102. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S.; Kusano, C.; Horii, T.; Ichijima, R.; Ikehara, H. The ideal Helicobacter pylori treatment for the present and the future. Digestion 2022, 103, 62–68. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of antibiotic resistance in Helicobacter pylori: A systematic review and meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed]
- Miendje Deyi, V.Y.; Lare, M.S.; Burette, A.; Ntounda, R.; Elkilic, O.; Cadranel, S.; Bontems, P.; Hallin, M. Update of primary Helicobacter pylori resistance to antimicrobials in Brussels, Belgium. Diagn. Microbiol. Infect. Dis. 2019, 95, 114875. [Google Scholar] [CrossRef] [PubMed]
- Miendje Deyi, V.Y.; Bontems, P.; Vanderpas, J.; De Koster, E.; Ntounda, R.; Van den Borre, C.; Cadranel, S.; Burette, A. Multicenter survey of routine determinations of resistance of Helicobacter pylori to antimicrobials over the last 20 years (1990 to 2009) in Belgium. J. Clin. Microbiol. 2011, 49, 2200–2209. [Google Scholar] [CrossRef] [PubMed]
- Mégraud, F.; Alix, C.; Charron, P.; Bénéjat, L.; Ducournau, A.; Bessède, E.; Lehours, P. Survey of the antimicrobial resistance of Helicobacter pylori in France in 2018 and evolution during the previous 5 years. Helicobacter 2021, 26, e12767. [Google Scholar] [CrossRef]
- Megraud, F.; Bruyndonckx, R.; Coenen, S.; Wittkop, L.; Huang, T.D.; Hoebeke, M.; Bénéjat, L.; Lehours, P.; Goossens, H.; et al.; European Helicobacter pylori Antimicrobial Susceptibility Testing Working Group Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut 2021, 70, 1815–1822. [Google Scholar] [CrossRef] [PubMed]
- Bujanda, L.; Nyssen, O.P.; Vaira, D.; Saracino, I.M.; Fiorini, G.; Lerang, F.; Georgopoulos, S.; Tepes, B.; Heluwaert, F.; Gasbarrini, A.; et al. Antibiotic resistance prevalence and trends in patients infected with Helicobacter pylori in the period 2013–2020: Results of the European Registry on H. pylori Management (Hp-EuReg). Antibiotics 2021, 10, 1058. [Google Scholar] [CrossRef] [PubMed]
- Botija, G.; García Rodríguez, C.; Recio Linares, A.; Campelo Gutiérrez, C.; Pérez-Fernández, E.; Barrio Merino, A. Antibiotic resistances and eradication rates in Helicobacter pylori infection. An. Pediatr. 2021, 95, 431–437. [Google Scholar] [CrossRef]
- Dekhnich, N.; Ivanchik, N.; Kozlov, R.; Alimov, A.; Steshits, A.; Kirsov, P.; Pandav, K. Dynamics of antimicrobial resistance of Helicobacter pylori isolates in the Smolensk region of Russian Federation. Helicobacter 2018, 23, e12545. [Google Scholar] [CrossRef]
- Schubert, J.P.; Warner, M.S.; Rayner, C.K.; Roberts-Thomson, I.C.; Mangoni, A.A.; Costello, S.; Bryant, R.V. Increasing Helicobacter pylori clarithromycin resistance in Australia over 20 years. Intern. Med. J. 2022, 52, 1554–1560. [Google Scholar] [CrossRef]
- Mosites, E.; Bruden, D.; Morris, J.; Reasonover, A.; Rudolph, K.; Hurlburt, D.; Hennessy, T.; McMahon, B.; Bruce, M. Antimicrobial resistance among Helicobacter pylori isolates in Alaska, 2000–2016. J. Glob. Antimicrob. Resist. 2018, 15, 148–153. [Google Scholar] [CrossRef]
- Bedoya-Gómez, I.J.; Alvarez-Aldana, A.; Moncayo-Ortiz, J.I.; Guaca-González, Y.M.; Santacruz-Ibarra, J.J.; Arturo-Arias, B.L.; Castañeda-Chávez, L.J.; Leon Rodriguez, D.A.; Beltrán-Angarita, L. Surveillance of the antimicrobial resistance rates of Helicobacter pylori ten years later in the Western central region, Colombia. Dig Dis. 2020, 38, 196–203. [Google Scholar] [CrossRef]
- Alvarez, A.; Moncayo, J.I.; Santacruz, J.J.; Santacoloma, M.; Corredor, L.F.; Reinosa, E. Antimicrobial susceptibility and mutations involved in clarithromycin resistance in Helicobacter pylori isolates from patients in the western central region of Colombia. Antimicrob. Agents Chemother. 2009, 53, 4022–4024. [Google Scholar] [CrossRef] [Green Version]
- Parra-Sepúlveda, C.; Merino, J.S.; Sáez-Carrillo, K.; González, C.; García-Cancino, A. Antibiotic resistance surveillance of Helicobacter pylori at the Biobío region (Chile) in a decade. Arq. Gastroenterol. 2019, 56, 361–366. [Google Scholar] [CrossRef]
- Liang, C.M.; Tai, W.C.; Hsu, P.I.; Wu, D.C.; Kuo, C.H.; Tsay, F.W.; Lee, C.L.; Chen, K.Y.; Chuah, S.K. Trend of changes in antibiotic resistance in Helicobacter pylori from 2013 to 2019: A multicentre report from Taiwan. Therap. Adv. Gastroenterol. 2020, 13, 1756284820976990. [Google Scholar] [CrossRef]
- Wang, D.; Guo, Q.; Yuan, Y.; Gong, Y. The antibiotic resistance of Helicobacter pylori to five antibiotics and influencing factors in an area of China with a high risk of gastric cancer. BMC Microbiol. 2019, 19, 152. [Google Scholar] [CrossRef]
- Sholeh, M.; Maleki, F.; Krutova, M.; Bavari, S.; Golmoradi, R.; Sadeghifard, N.; Amiriani, T.; Kouhsari, E. The increasing antimicrobial resistance of Helicobacter pylori in Iran: A systematic review and meta-analysis. Helicobacter 2020, 25, e12730. [Google Scholar] [CrossRef]
- Tran, T.T.; Nguyen, A.T.; Quach, D.T.; Pham, D.T.; Cao, N.M.; Nguyen, U.T.; Dang, A.N.; Tran, M.A.; Quach, L.H.; Tran, K.T.; et al. Emergence of amoxicillin resistance and identification of novel mutations of the pbp1A gene in Helicobacter pylori in Vietnam. BMC Microbiol. 2022, 22, 41. [Google Scholar] [CrossRef]
- ESAC-Net—European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2021; ECDC: Stockholm, Sweden, 2022.
- Chen, M.J.; Wu, M.S.; Chen, C.C.; Chen, C.C.; Fang, Y.J.; Bair, M.J.; Chang, C.Y.; Lee, J.Y.; Hsu, W.F.; Luo, J.C.; et al. Impact of amoxicillin resistance on the efficacy of amoxicillin-containing regimens for Helicobacter pylori eradication: Analysis of five randomized trials. J. Antimicrob. Chemother. 2017, 72, 3481–3489. [Google Scholar] [CrossRef] [PubMed]
- Dingsdag, S.A.; Hunter, N. Metronidazole: An update on metabolism, structure-cytotoxicity and resistance mechanisms. J. Antimicrob. Chemother. 2018, 73, 265–279. [Google Scholar] [CrossRef]
- Thomas, C.; Gwenin, C.D. The Role of nitroreductases in resistance to nitroimidazoles. Biology 2021, 10, 388. [Google Scholar] [CrossRef]
- Hashemi, S.J.; Sheikh, A.F.; Goodarzi, H.; Yadyad, M.J.; Seyedian, S.S.; Aslani, S.; Assarzadegan, M.A. Genetic basis for metronidazole and clarithromycin resistance in Helicobacter pylori strains isolated from patients with gastroduodenal disorders. Infect. Drug Resist. 2019, 12, 535–543. [Google Scholar] [CrossRef]
- Fiorini, G.; Zullo, A.; Saracino, I.M.; Pavoni, M.; Vaira, D. Antibiotic resistance pattern of Helicobacter pylori strains isolated in Italy during 2010–2016. Scand. J. Gastroenterol. 2018, 53, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Morilla, A.M.; Álvarez-Argüelles, M.E.; Duque, J.M.; Armesto, E.; Villar, H.; Melón, S. Primary antimicrobial resistance rates and prevalence of Helicobacter pylori infection in the north of Spain. A 13-year retrospective study. Gastroenterol. Hepatol. 2019, 42, 476–485. [Google Scholar] [CrossRef]
- Saracino, I.M.; Fiorini, G.; Zullo, A.; Pavoni, M.; Saccomanno, L.; Vaira, D. Trends in primary antibiotic resistance in H. pylori strains isolated in Italy between 2009 and 2019. Antibiotics 2020, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Jahanshahlou, F.; Hosseini, M.S. Antibiotic resistance: A disregarded concern for misuse of azithromycin in COVID-19 treatment. J. Res. Med. Sci. 2021, 26, 101. [Google Scholar] [CrossRef]
- McNicholl, A.G.; Bordin, D.S.; Lucendo, A.; Fadeenko, G.; Fernandez, M.C.; Voynovan, I.; Zakharova, N.V.; Sarsenbaeva, A.S.; Bujanda, L.; Perez-Aisa, Á.; et al. Combination of bismuth and standard triple therapy eradicates Helicobacter pylori infection in more than 90% of patients. Clin. Gastroenterol. Hepatol. 2020, 18, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Zhu, M.; Yue, L.; Hu, W. Multiple bismuth quadruple therapy containing tetracyclines combined with other antibiotics and Helicobacter pylori eradication therapy. J. Clin. Med. 2022, 11, 7040. [Google Scholar] [CrossRef] [PubMed]
- Seriki, A.T.; Smith, S.I.; Adeleye, A.I.; Fowora, M.A. Molecular analysis of low-level tetracycline resistance in clinical isolates of Helicobacter pylori among dyspeptic patients in South West Nigeria. J. Glob. Antimicrob. Resist. 2018, 13, 143–145. [Google Scholar] [CrossRef]
- Su, J.; Zhou, X.; Chen, H.; Hao, B.; Zhang, W.; Zhang, G. Efficacy of 1st-line bismuth-containing quadruple therapies with levofloxacin or clarithromycin for the eradication of Helicobacter pylori infection: A 1-week, open-label, randomized trial. Medicine 2017, 96, e5859. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Hadzhiyski, P.; Kandilarov, N.; Markovska, R.; Mitov, I. Multidrug resistance in Helicobacter pylori: Current state and future directions. Expert Rev. Clin. Pharmacol. 2019, 12, 909–915. [Google Scholar] [CrossRef]
- Boyanova, L.; Hadzhiyski, P.; Markovska, R.; Gergova, R. Investigation of multidrug-resistant Helicobacter pylori in pediatric patients: A Bulgarian study and literature. Acta Microbiol. Immunol. Hung. 2022, 69, 41–45. [Google Scholar] [CrossRef]
- Boyanova, L.; Hadzhiyski, P.; Markovska, R. Review—Epidemiology of Helicobacter pylori infection. Microb. Health Dis. 2021, 3, e543. [Google Scholar] [CrossRef]
- Lahaie, R.G.; Gaudreau, C. Helicobacter pylori antibiotic resistance: Trends over time. Can. J. Gastroenterol. 2000, 10, 895–899. [Google Scholar] [CrossRef]
- Nista, E.C.; Pellegrino, A.; Giuli, L.; Candelli, M.; Schepis, T.; De Lucia, S.S.; Ojetti, V.; Franceschi, F.; Gasbarrini, A. Clinical Implications of Helicobacter pylori antibiotic resistance in Italy: A Review of the literature. Antibiotics 2022, 11, 1452. [Google Scholar] [CrossRef]
- Karbalaei, M.; Talebi Bezmin Abadi, A.; Keikha, M. Clinical relevance of the cagA and vacA s1m1 status and antibiotic resistance in Helicobacter pylori: A systematic review and meta-analysis. BMC Infect. Dis. 2022, 22, 573. [Google Scholar] [CrossRef]
- Hou, C.; Yin, F.; Wang, S.; Zhao, A.; Li, Y.; Liu, Y. Helicobacter pylori biofilm-related drug resistance and new developments in its anti-biofilm agents. Infect. Drug Resist. 2022, 15, 1561–1571. [Google Scholar] [CrossRef]
- Rizvanov, A.A.; Haertlé, T.; Bogomolnaya, L.; Talebi Bezmin Abadi, A. Helicobacter pylori and its antibiotic heteroresistance: A neglected issue in published guidelines. Front. Microbiol. 2019, 10, 1796. [Google Scholar] [CrossRef]
- Machowska, A.; Stålsby Lundborg, C. Drivers of irrational use of antibiotics in Europe. Int. J. Environ. Res. Public Health 2018, 16, 27. [Google Scholar] [CrossRef]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu-Aguye, S.N.; Adeloye, D.; Strickland-Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta-analysis. J. Infect. 2019, 78, 8–18. [Google Scholar] [CrossRef]
- Suzuki, S.; Esaki, M.; Kusano, C.; Ikehara, H.; Gotoda, T. Development of Helicobacter pylori treatment: How do we manage antimicrobial resistance? World J. Gastroenterol. 2019, 25, 1907–1912. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Markovska, R.; Medeiros, J.; Gergova, G.; Mitov, I. Delafloxacin against Helicobacter pylori, a potential option for improving eradication success? Diagn. Microbiol. Infect. Dis. 2020, 96, 114980. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Jin, S.Y. Current guidelines for Helicobacter pylori treatment in East Asia 2022: Differences among China, Japan, and South Korea. World J Clin Cases 2022, 10, 6349–6359. [Google Scholar] [CrossRef]
- Saracino, I.M.; Pavoni, M.; Zullo, A.; Fiorini, G.; Lazzarotto, T.; Borghi, C.; Vaira, D. Next Generation Sequencing for the prediction of the antibiotic resistance in Helicobacter pylori: A Literature Review. Antibiotics 2021, 10, 437. [Google Scholar] [CrossRef] [PubMed]
- Cardos, I.A.; Zaha, D.C.; Sindhu, R.K.; Cavalu, S. Revisiting therapeutic strategies for H. pylori treatment in the context of antibiotic resistance: Focus on alternative and complementary therapies. Molecules 2021, 26, 6078. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Continent/ Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in Years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|
| Asia | |||||||
| China | Consecutive adults | E test, PCR | Specified | 23 in 1998–1999, 50 in 2002–2004, 27 in 2016–2017 | 4.3 in 1998–1999, 2.0 in 2002–2004, 25.9 in 2016–2017 | Increase | [33] |
| Iran | Children and adults | DDM, ADM | NA (review) | 3619 in 1999–2019 | 9.0 in 1999–2000, 14.0 in 2011–2016, 36.0 in 2017–2019 | Increase | [34] |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | ≤0.6 in 2013–2014, ≤1.0 in 2015–2019 | No | [32] |
| Taiwan | Adults, treated (2nd-line treatment) | E test | Specified | 196 in 2013–2019 | 0.0 in 2013–2019 | No | [32] |
| Taiwan | Adults, treated (3rd-line treatment) | E test | Specified | 184 in 2013–2019 | 0.0 in 2013–2014, 2.4 in 2015, 5.9 in 2016, 0.0 in 2017–2018, 5.6 in 2019 | No | [32] |
| Vietnam | Untreated adults and other data | E test, pbp1A sequencing | NA | 308 in 2019/2021 and previous data | ≤1.1 in 2013–2015, 10.4 in 2016, 15.0 in 2019, 25.7% in 2020 | Increase | [35] |
| Australia/ Oceania | |||||||
| Australia | Consecutive adults (mainly untreated) | E test | EUCAST | 907 in 1998–2007, 566 in 2008–2017 | 0.2 in 1998–2007, 0.0 in 2008–2017 | No | [27] |
| Europe | |||||||
| Belgium | Untreated patients, children and adults | DDM, E test | EUCAST | 1001 in 2008–2009, 438 in 2016 | 0.0 in 2008–2009, 0.0 in 2016 | No | [20,21] |
| Bulgaria | Consecutive, children and adults | E test | EUCAST | 237 in 2007–2014, 237 in 2015–2021 | 4.2 in 2007–2014, 8.9 in 2015–2021 | Increase | [11] |
| France | Untreated adults | E test, DDM | EUCAST | 266 in 2014, 231 in 2016, 244 in 2018 | 0.7 in 2014, 0.9 in 2016, 0.0 in 2018 | No | [22] |
| France | Treated adults | E test, DDM | EUCAST | 115 in 2014, 125 in 2016, 110 in 2018 | 0.0 in 2014, 0.8 in 2016, 0.0 in 2018 | No | [22] |
| Russia | Consecutive adult patients | ADM | EUCAST | 133 in 2009–2010, 143 in 2015–2017 | 4.5 in 2009–2010, 1.4 in 2015–2017 | No | [26] |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 2000 in 2013–2016, 1250 in 2017–2020 | 0.3 in 2013–2016, 0.4 in 2017–2020 | No | [24] |
| South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 299 in 2005–2007, 72 in 2015–2017 | 2.0 in 2005–2007, 4.2 in 2015–2017 | No | [31] |
| Colombia | Consecutive adults | E test | CLSI, EUCAST | 106 in 2009, 61 in 2015 | 1.9 in 2009, 0.0 in 2015 | No | [29,30] |
| Continent/Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in Years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|
| Asia | |||||||
| China | Consecutive adults | E test, PCR | Specified | 23 in 1998–1999, 50 in 2002–2004, 27 in 2016–2017 | 87.0 in 1998–1999, 66.0 in 2002–2004, 92.6 in 2016–2017 | No | [33] |
| Iran | Children and adults | DDM, ADM | NA (review) | 4330 in 1999–2019 | 67.0 in 1999–2000, 52.0 in 2011–2016, 66.0 in 2017–2019 | No | [34] |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | 25.6 in 2013, >29.0 in 2015–2018, 42.3 in 2019 | Increase | [32] |
| Taiwan | Adults, treated (2nd-line treatment) | E test | Specified | 196 in 2013–2019 | ≤50.0 in 2013–2016, >70.0 in 2017–2019 | Increase | [32] |
| Taiwan | Adults, treated (3rd-line treatment) | E test | Specified | 184 in 2013–2019 | 44.4 in 2013, <53.0 in 2014–2015 to 83.3 in 2019 | Increase | [32] |
| Australia/Oceania | |||||||
| Australia | Consecutive adults (mainly untreated) | E test | EUCAST | 907 in 1998–2007, 566 in 2008–2017 | 32.3 (1998–2007), 39.9 (2008–2017) | No | [27] |
| Europe | |||||||
| Belgium | Untreated children and adults | DDM, E test | EUCAST | 1001 in 2008–2009, 438 in 2016 | 28.0 in 2008–2009, 40.0 in 2016 | Increase | [20,21] |
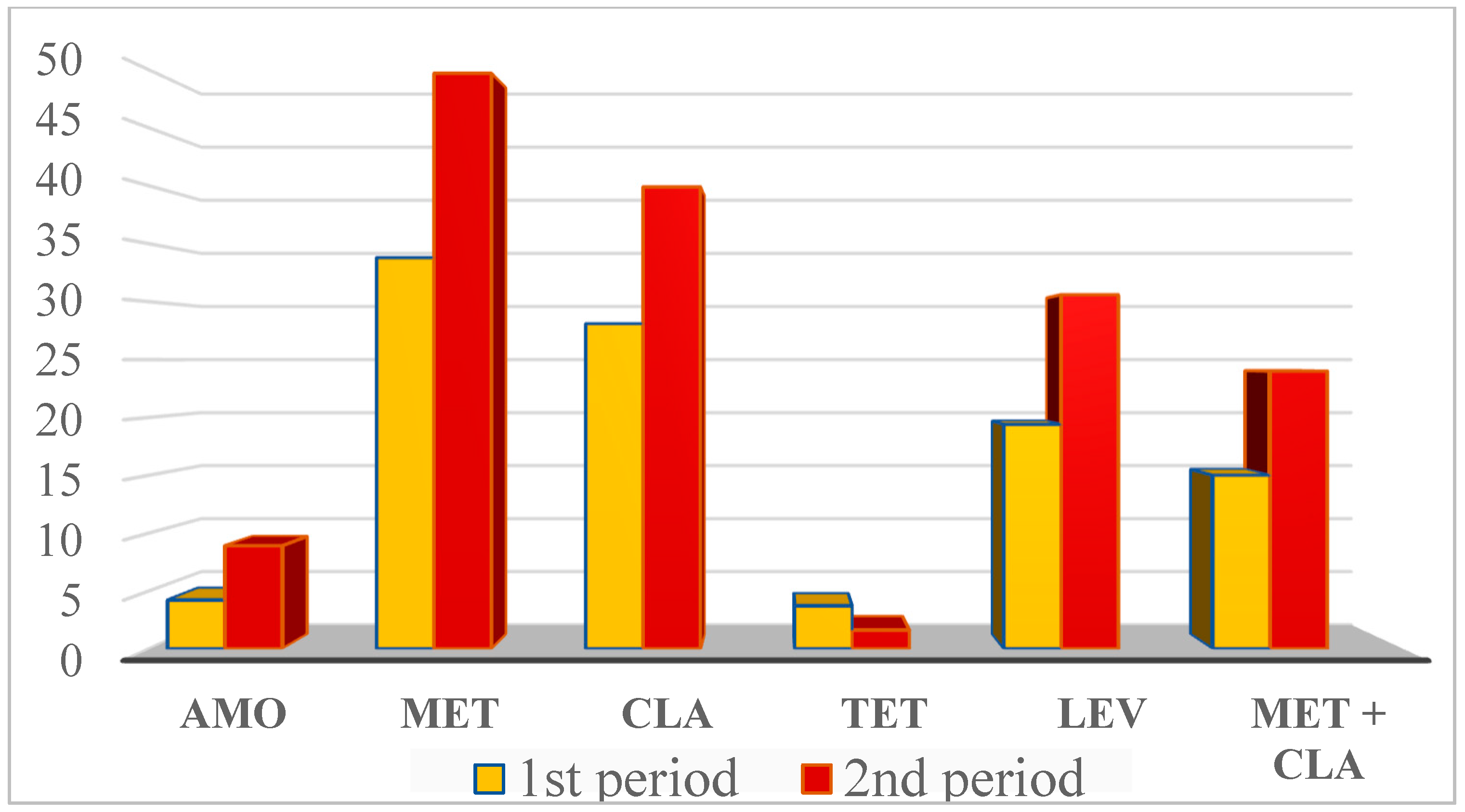
| Bulgaria | Consecutive adults and children | E test, DDM | EUCAST | 299 in 2010–2015, 183 in 2016–2022 | 33.8 in 2010–2015, 49.7 in 2016–2022 | Increase | [12], Boyanova, this study |
| France | Untreated adults | E test, DDM | EUCAST | 266 in 2014, 231 in 2016, 244 in 2018 | 45.9 in 2014, 52.4 in 2016, 58.6 in 2018 | Increase | [22] |
| France | Treated adults | E test, DDM | EUCAST | 115 in 2014, 125 in 2016, 110 in 2018 | 78.3 in 2014, 80.6 in 2016, 87.3 in 2018 | Slight increase | [22] |
| Italy | Consecutive untreated adults | E test | EUCAST | 907 in 2009–2014, 739 in 2015–2019 | 33.3 in 2009–2014, 33.6 in 2015–2019 | No | [43] |
| Italy | Consecutive patients | E test | EUCAST | 1424 in 2010–2016 | 33.6 in 2010, 45.3 in 2013, 40.2 in 2016 | Increase in 2010/2013, plateau in 2014–2016 | [41] |
| Russia | Consecutive adult patients | ADM | EUCAST | 133 in 2009–2010, 143 in 2015–2017 | 3.8 in 2009–2010, 23.8 in 2015–2017 | Increase | [26] |
| Spain | Children untreated and treated | E test | EUCAST | 27 in in 2014–2015, 24 in in 2016–2017, 29 in 2018–2019 | Around 30 in 2014–2015 and 2018–2019 | No | [25] |
| Spain | Untreated patients, mostly adults | E test | EUCAST | 254 in 2004–2005, 233 in 2015–2016 | 45.0 in 2004, 41.0 in 2005, 30.0 in 2015, 34.0 in 2016 | Decrease | [42] |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 1733 in 2013–2016, 1139 in 2017–2020 | 33.0 in 2013–2016, 24.5 in 2017–2020 | Decrease | [24] |
| South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 364 in 2005–2007, 72 in 2015–2017 | 55.5 in 2005–2007, 37.5 in 2015–2017 | Decrease | [31] |
| Colombia | Consecutive adults | E test | CLSI, EUCAST | 106 in 2009, 61 in 2015 | 82.0 in 2009, 78.7 in 2015 | No | [29,30] |
| Continent/ Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|
| Asia | |||||||
| China | Consecutive adults | E test, PCR | Specified | 23 in 1998–1999, 50 in 2002–2004, 27 in 2016–2017 | 39.1 in 1998–1999, 14.0 in 2002–2004, 55.6 in 2016–2017 | No | [33] |
| Iran | Children and adults | DDM, ADM | NA (review) | 5145 in 1999–2019 | 9.0 in 1999–2000, 21.0 in 2011–2016, 36.0 in 2017–2019 | Increase | [34] |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | <14.0 in 2013–2014, 20.4 in 2019 | Increase | [32] |
| Taiwan | Treated adults (2nd-line treatment) | E test | Specified | 196 in 2013–2019 | 70.3 in 2013, <70.0 in 2014 and 2017–2018, 80.6 in 2019 | No | [32] |
| Taiwan | Treated adults (3rd-line treatment) | E test | Specified | 184 in 2013–2019 | <77.0 in 2013–2014, 80.5–92.3 in 2015–2017, 64.0 in 2018, 83.3 in 2019 | No | [32] |
| South-East Asia | Overall patients | NA (review) | NA (review) | 1830 in 2006–2016 | 13 in 2006–2008, 21 in 2012–2016 | Increase | [19] |
| Australia/Oceania | |||||||
| Australia | Consecutive adults (mainly untreated) | E test | EUCAST | 907 in 1998–2007, 566 in 2008–2017 | 16.0 (1998–2007), 21.2 (2008–2017) | Increase | [27] |
| Europe | |||||||
| Belgium | Untreated children and adults | DDM, E test | EUCAST | 1001 in 2008–2009, 438 in 2016 | 10.5 in 2008–2009, 18.0 in 2016 | Increase | [20,21] |
| Bulgaria | Consecutive adults and children | E test, DDM | EUCAST | 299 in 2010–2015, 183 in 2016–2022 | 28.1 in 2010–2015, 39.9 in 2016–2022 | Increase | [12], Boyanova, this study |
| France | Untreated adults | E test, DDM, PCR | EUCAST | 266 in 2014, 231 in 2016, 244 in 2018 | 22.2 in 2014, 20.3 in 2016, 20.9 in 2018 | No | [22] |
| France | Treated adults | E test, DDM, PCR | EUCAST | 115 in 2014, 125 2016, 110 in 2018 | 73.9 in 2014, 59.7 in 2016, 56.4 in 2018 | Decrease | [22] |
| Italy | Consecutive untreated adults | E test | EUCAST | 907 in 2009–2014, 739 in 2015–2019 | 30.2 in 2009–2014, 37.8 in 2015–2019 | Increase | [43] |
| Italy | Consecutive patients | E test | EUCAST | 1424 in 2010–2016 | 19.0 in 2010, 35.6 in 2013, 35.9 in 2016 | Increase (2010/13), plateau in 2014/16 | [41] |
| Russia | Consecutive adult patients | ADM | EUCAST | 133 in 2009–2010, 143 in 2015–2017 | 5.3 in 2009–2010, 6.3 in 2015–2017 | No | [26] |
| Spain | Children untreated and treated | E test | EUCAST | 80 in 2014–2019 | Around 50.0 in 2014–2015 and 2018–2019 | No | [25] |
| Spain | Consecutive patients, mostly adults | E test | EUCAST | 253 in in 2004–2005, 233 in in 2015–2016 | 21.0 in 2004, 20.0 in 2005, 23.0 in 2015, 22.0 in 2016 | No | [42] |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 1724 in 2013–2016, 1150 in 2017–2020 | 25.0 in 2013–2016, 20.0 in 2017–2020 | No | [24] |
| South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 333 in 2005–2007, 72 in 2015–2017 | 22.5 in 2005–2007, 29.2 in 2015–2017 | No | [31] |
| Colombia | Consecutive adults | E test, sequencing | CLSI, EUCAST | 106 in 2009, 61 in 2015 | 3.8 in 2009, 8.2 in 2015 | No | [29,30] |
| Continent/Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in Years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|
| Asia | |||||||
| China | Consecutive adults | E test, PCR | Specified | 23 in 1998–1999, 50 in 2002–2004, 27 in 2016–2017 | 13.0 in 1998–1999, 14.0 in 2002–2004, 18.5 in 2016–2017 | No | [33] |
| Iran | Children and adults | DDM, ADM | NA (review) | 3061 in 1999–2019 | 3.0 in 1999–2000, 12.0 in 2011–2016, 18.0 in 2017–2019 | Increase | [34] |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | 0.0 in 2013–2014, 0.8 in 2015, 0.0 in 2016–2019 | No | [32] |
| Taiwan | Treated adults (2nd-line treatment) | E test | Specified | 196 in 2013–2019 | 0.0 except for 1.7 in 2014 and 7.1 in 2016 | No | [32] |
| Taiwan | Treated adults (3rd-line treatment) | E test | Specified | 184 in 2013–2019 | 11.1 in 2013, 0.0–7.7 in 2014–2017, 0.0 in 2018–2019 | No | [32] |
| Australia/Oceania | |||||||
| Australia | Consecutive adults (mainly untreated) | E test | EUCAST | 907 in 1998–2007, 566 in 2008–2017 | 0.2 (1998–2007), 0.5 (2008–2017) | No | [27] |
| Europe | |||||||
| Belgium | Untreated patients, children and adults | DDM, E test | EUCAST | 1001 in 2008–2009, 438 in 2016 | 0.0 in 2008–2009, 0.0 in 2016 | No | [20,21] |
| Bulgaria | Consecutive adults and children | E test, DDM | EUCAST | 134 in 2010–2015, 183 in 2016–2022 | 3.7 in 2010–2015, 1.6 in 2016–2022 | No | [12], Boyanova, this study |
| France | Untreated adults | E test, DDM | EUCAST | 266 in 2014, 231 in 2016, 244 in 2018 | 0.0 in 2014, 0.0 in 2016, 0.0 in 2018 | No | [22] |
| France | Treated adults | E test, DDM | EUCAST | 115 in 2014, 125 in 2016, 110 in 2018 | 0.0 in 2014, 0.0 in 2016, 0.0 in 2018 | No | [22] |
| Russia | Consecutive adult patients | ADM | EUCAST | 133 in 2009–2010, 143 in 2015–2017 | 0.0 in 2009–2010, 0.7 in 2015–2017 | No | [26] |
| Spain | Children untreated and treated | E test | EUCAST | 80 in 2014–2019 | 0 in 2014–2015 and 2018–2019 | No | [25] |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 2000 in 2013–2016, 1250 in 2017–2020 | 0.2 in 2013–2016, 0.08 in 2017–2020 | No | [24] |
| South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 311 in 2005–2007, 72 in 2015–2017 | 1.0 in 2005–2007, 1.4 in 2015–2017 | No | [31] |
| Colombia | Consecutive adults | E test | CLSI, EUCAST | 106 in 2009, 61 in 2015 | 0.0 in 2009, 0.0 in 2015 | No | [29,30] |
| Continent/ Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in Years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|
| Asia | |||||||
| China | Consecutive adults | E test, PCR | Specified | 23 in 1998–1999, 50 in 2002–2004, 27 in 2016–2017 | 47.8 in 1998–1999, 46.0 in 2002–2004, 81.5 in 2016–2017 | Increase | [33] |
| Iran (ciprofloxacin) | Children and adults | DDM, ADM | NA (review) | 2046 in 1999–2019 | 15.0 in 1999–2000, 18.0 in 2011–2016, 36.0 in 2017–2019 | Increase | [34] |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | <24.0 in 2013–2015, 29.1–32.4 in 2016–2018, 38.8 in 2019 | Increase | [32] |
| Taiwan | Treated adults (2nd-line treatment) | E test | Specified | 196 in 2013–2019 | <38.0 in 2013–2015, 51.6–64.7 in 2016–2019 | Increase | [32] |
| Taiwan | Treated adults (3rd-line treatment) | E test | Specified | 184 in 2013–2019 | 72.2 in 2013, >94.0 in 2016 and 2017, 76.0 in 2018, 83.3 in 2019 | No | [32] |
| Western Pacific region | Overall patients | NA (review) | NA (review) | 28946 in 2006–2016 | 12.0 in 2006–2008, 31.0 in 2012–2016 | Increase | [19] |
| Europe | |||||||
| Belgium | Untreated patients, children and adults | DDM, E test | EUCAST | 1001 in 2008–2009, 438 in 2016 | 12.4 in 2008–2009, 22.8 in 2016 | Increase | [20,21] |
| Bulgaria | Consecutive adults and children | E test, DDM | EUCAST | 299 in 2010–2015, 183 in 2016–2022 | 19.4 in 2010–2015, 30.6 in 2016–2022 | Increase | [12], Boyanova, this study |
| France | Untreated adults | E test, DDM | EUCAST | 266 in 2014, 231 in 2016, 244 in 2018 | 15.4 in 2014, 14.7 in 2016, 17.6 in 2018 | No | [22] |
| France | Treated adults | E test, DDM | EUCAST | 115 in 2014, 125 in 2016, 110 in 2018 | 14.8 in 2014, 23.4 in 2016, 22.7 in 2018 | Slight increase | [22] |
| Italy | Consecutive untreated adults | E test | EUCAST | 907 in 2009–2014, 739 in 2015–2019 | 25.6 in 2009–2014, 33.8 in 2015–2019 | Increase | [43] |
| Italy | Consecutive patients | E test | EUCAST | 1424 in 2010–2016 | 19.0 in 2010, 29.7 in 2013, 29.3 in 2016 | Increase (2010/13), plateau in 2013/16 | [41] |
| Russia | Consecutive adult patients | ADM | EUCAST | 133 in 2009–2010, 143 2015–2017 | 8.3 in 2009–2010, 24.5 in 2015–2017 | Increase | [26] |
| Spain | Children untreated and treated | E test | EUCAST | 80 in 2014–2019 | Around 10.0 in 2014–2015 and 2018–2019 | No | [25] |
| Spain | Consecutive patients, mostly adults | E test | EUCAST | 212 in 2011–2012, 233 in 2015–2016 | 15.0 in 2011, 17.0 in 2012, 22.0 in 2015, 17.0 in 2016 | No | [42] |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 1717 in 2013–2016, 1155 in 2017–2020 | 20.5 in 2013–2016, 18.0 in 2017–2020 | No | [24] |
| North America | |||||||
| USA | Consecutive patients | E test | Specified | 800 in 2000 to 2016 | <10.0 in 2000–2001, around 30.0 in 2012-2013, <20.0 in 2016 | Overall increase, decrease since 2012/13 | [28] |
| South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 321 in 2005–2007, 72 in 2015–2017 | 15.3 in 2005–2007, 20.8 in 2015–2017 | No | [31] |
| Resistance to | Continent/ Country | Patients | Method | Breakpoints | No. of Patients | Resistance (% in Years) | Resistance Evolution | Reference |
|---|---|---|---|---|---|---|---|---|
| MET + CLA | Asia | |||||||
| Iran | Children and adults | DDM, ADM | NA (review) | 1562 in 1999–2019 | 15.0 in 1999–2000, 17.0 in 2011–2016, 17.0 in 2017–2019 | No | [34] | |
| Taiwan | Untreated adults | E test | Specified | 1369 in 2013–2019 | 2.4 in 2013, 5.1–8.4 in 2014–2018, 10.4 in 2019 | Increase | [32] | |
| Europe | ||||||||
| Bulgaria | Consecutive adults and children | E test, DDM | EUCAST | 299 in 2010–2015, 183 in 2016–2022 | 15.0 in 2010–2015, 24.0 in 2016–2022 | Increase | [12], Boyanova, this study | |
| Italy | Consecutive untreated adults | E test | EUCAST | 907 in 2009–2014, 739 in 2015–2019 | 18.9 in 2009–2014, 20.7 in 2015–2019 | No | [43] | |
| Italy | Consecutive patients | E test | EUCAST | 1424 in 2010–2016 | 11.4 in 2010, 28.2 in 2013, 21.9 in 2016 | Increase (2010–2013), plateau in 2014–2016 | [41] | |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 1728 in 2013–2016, 1145 in 2017–2020 | 14.0 in 2013–2016, 11.0 in 2017–2020 | No | [24] | |
| South America | ||||||||
| Chile | Untreated children and adults | DDM | Specified | 271 in 2005–2007, 72 in 2015–2017 | 12.2 in 2005–2007, 18.0 in 2015–2017 | No | [31] | |
| Colombia | Consecutive adults | E test | CLSI, EUCAST | 106 in 2009, 61 in 2015 | 3.8 in 2009, 8.2 in 2015 | No | [29,30] | |
| MDR triple | Europe | |||||||
| Italy | Consecutive untreated adults | E test | EUCAST | 907 in 2009–2014, 739 in 2015–2019 | 10.4 in 2009–2014, 12.6 in 2015–2019 | No | [43] | |
| Nine European countries * | Untreated patients | NA (review) | NA (review) | 1722 in 2013–2016, 1133 in 2017–2020 | 7.2 in 2013–2016, 4.5 in 2017–2020 | No | [24] | |
| South America | ||||||||
| Chile | Untreated children and adults | DDM | Specified | 271 in 2005–2007, 72 in 2015–2017 | 3.7 in 2005–2007, 18.0 in 2015–2017 | Increase | [31] | |
| MDR quadruple | South America | |||||||
| Chile | Untreated children and adults | DDM | Specified | 271 in 2005–2007, 72 in 2015–2017 | 0.4 in 2005–2007, 2.8 in 2015–2017 | No | [31] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyanova, L.; Hadzhiyski, P.; Gergova, R.; Markovska, R. Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern. Antibiotics 2023, 12, 332. https://doi.org/10.3390/antibiotics12020332
Boyanova L, Hadzhiyski P, Gergova R, Markovska R. Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern. Antibiotics. 2023; 12(2):332. https://doi.org/10.3390/antibiotics12020332
Chicago/Turabian StyleBoyanova, Lyudmila, Petyo Hadzhiyski, Raina Gergova, and Rumyana Markovska. 2023. "Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern" Antibiotics 12, no. 2: 332. https://doi.org/10.3390/antibiotics12020332