
Comparison between EUCAST Broth Microdilution and MIC Strip Test in Defining Isavuconazole In Vitro Susceptibility against Candida and Rare Yeast Clinical Isolates

 ,
,
Abstract
:1. Introduction
2. Results
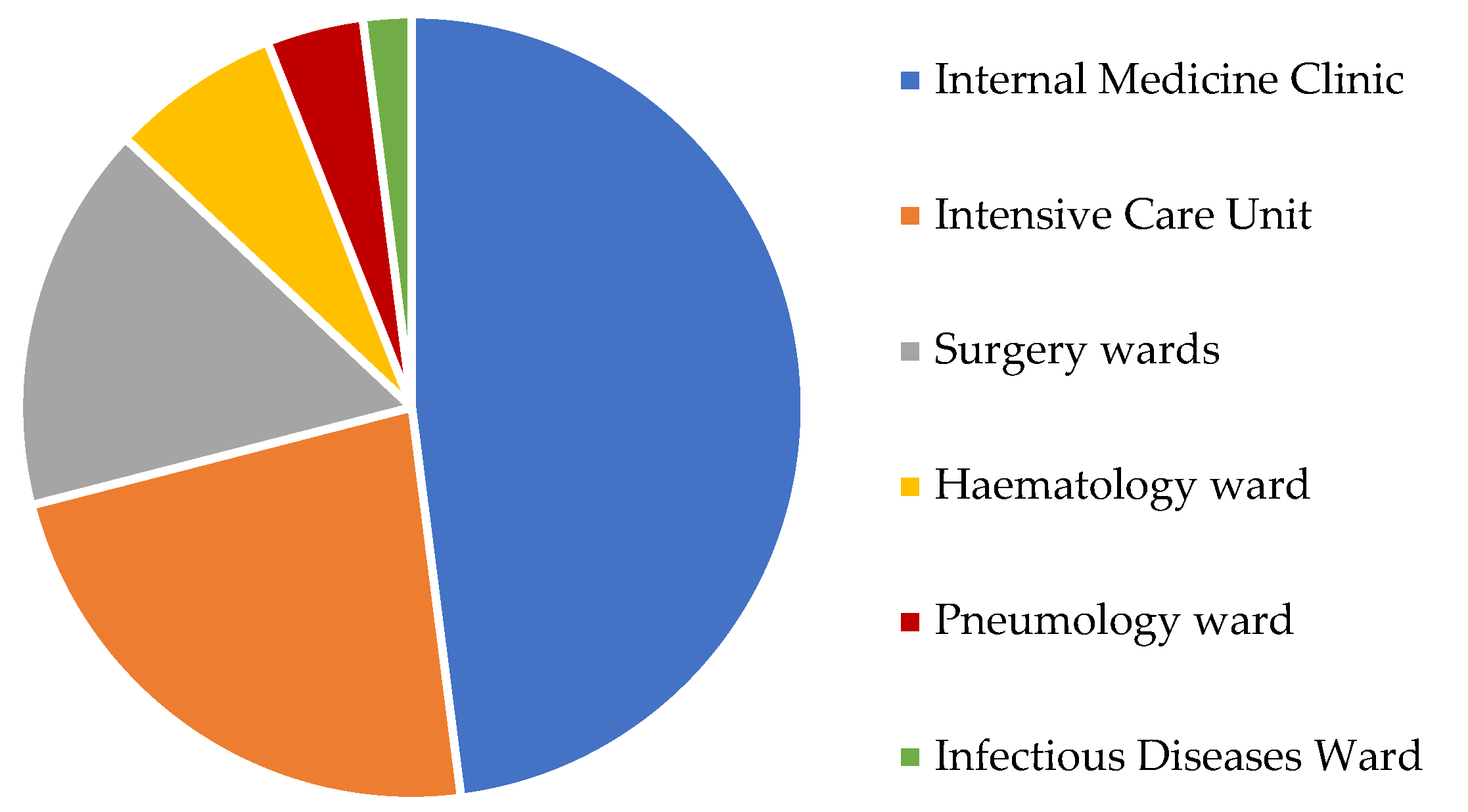
2.1. Isolates Distribution
2.2. EUCAST Broth Microdilution
2.3. MIC Strip Test
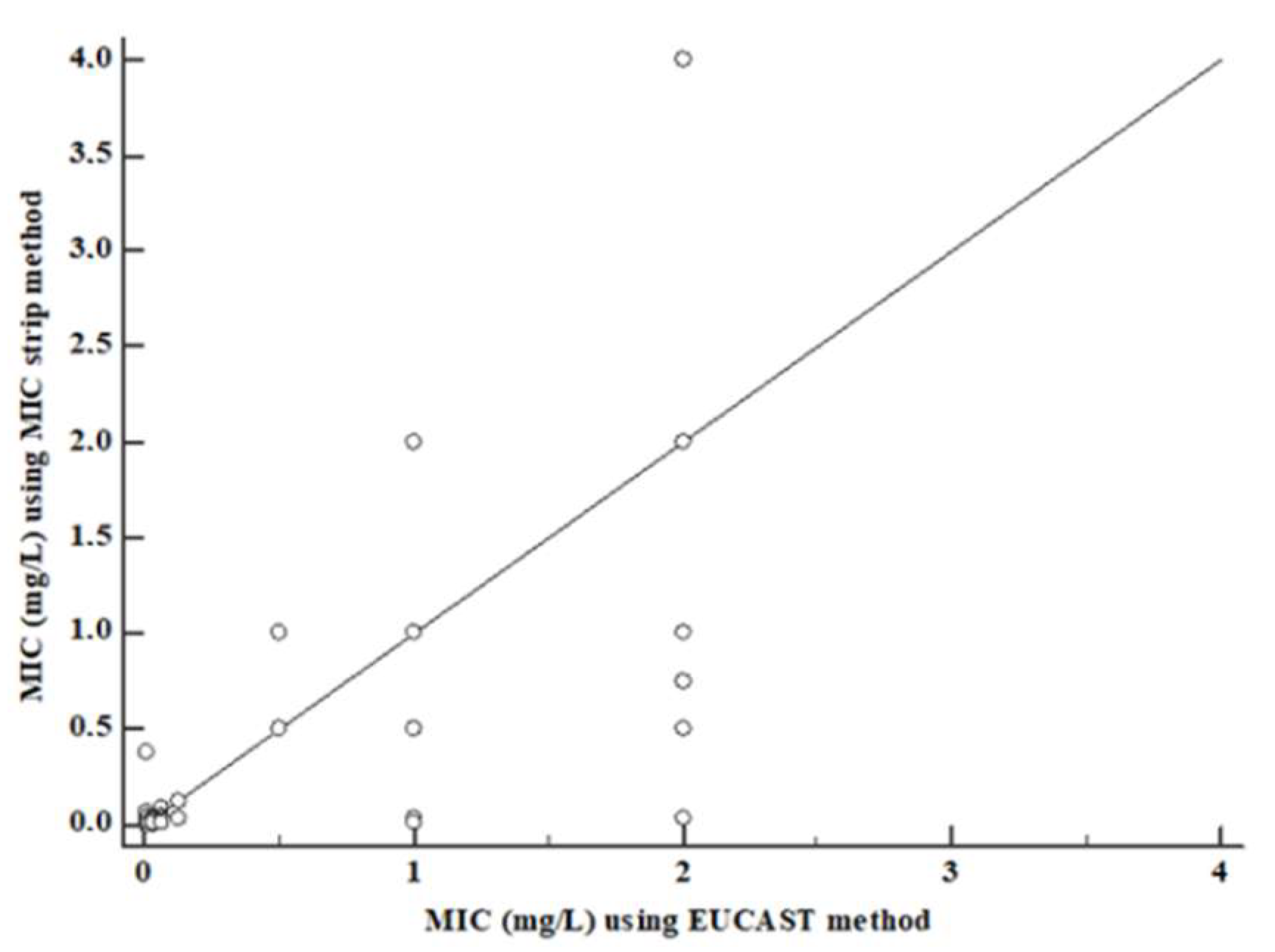
2.4. Statistical Analysis
2.5. P-ECOFF Calculation
3. Discussion
4. Materials and Methods
4.1. Sample Size
4.2. EUCAST Broth Microdilution
4.3. MIC Strip Method
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- European Medicines Agency (EMA). Cresemba: EPAR e Product Information; EMA: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Denis, J.; Ledoux, M.P.; Nivoix, Y.; Herbrecht, R. Isavuconazole: A new broad-spectrum azole. Part 1: In vitro activity. J. Mycol. Med. 2018, 3, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Guinea, J.; Bouza, E. Isavuconazole: A new and promising antifungal triazole for the treatment of invasive fungal infections. Future Microbiol. 2008, 3, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Girmenia, C. New generation azole antifungals in clinical investigation. Expert Opin. Investig. Drugs 2009, 3, 1279–1295. [Google Scholar] [CrossRef] [PubMed]
- Livermore, J.; Hope, W. Evaluation of the pharmacokinetics and clinical utility of isavuconazole for treatment of invasive fungal infections. Expert Opin. Drug Metab. Toxicol. 2012, 3, 759–765. [Google Scholar] [CrossRef]
- Isavuconazole for invasive fungal infections. Aust. Prescr. 2020, 3, 100–101.
- Gonzalez, G.M. In vitro activities of isavuconazole against opportunistic filamentous and dimorphic fungi. Med. Mycol. 2009, 47, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falci, D.R.; Pasqualotto, A.C. Profile of isavuconazole and its potential in the treatment of severe invasive fungal infections. Infect. Drug Resist. 2013, 6, 163–174. [Google Scholar]
- Ledoux, M.P.; Denis, J.; Nivoix, Y.; Herbrecht, R. Isavuconazole: A new broad-spectrum azole. Part 2: Pharmacokinetics and clinical activity. J. Mycol. Med. 2018, 3, 15–22. [Google Scholar] [CrossRef]
- Arendrup, M.C.; Jensen, R.H.; Meletiadis, J. In Vitro Activity of Isavuconazole and Comparators against Clinical Isolates of the Mucorales Order. Antimicrob. Agents Chemother. 2015, 3, 7735–7742. [Google Scholar] [CrossRef] [Green Version]
- Ellsworth, M.; Ostrosky-Zeichner, L. Isavuconazole: Mechanism of Action, Clinical Efficacy, and Resistance. J. Fungi 2020, 3, 324. [Google Scholar] [CrossRef]
- Clinical Laboratory Standards Institute. M60 Performance Standards For Antifungal Susceptibility Testing of Yeasts, 2nd ed.; Clinical Laboratory Standards Institute: Malvern, PA, USA, June 2020. [Google Scholar]
- Arendrup, M.C.; Cuenca-Estrella, M.; Lass-Flörl, C.; Hope, W.; EUCAST-AFST. EUCAST definitive document E. DEF 7.3: Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for yeasts. Eur. Comm. Antimicrob. Susceptibility Test-EUCAST 2020, 18, E246–E247. [Google Scholar]
- Liofilchem®—MIC Test Strip Technical Sheet Isavuconazole—MTS40—Rev.0/30.10.2015. Available online: http://www.liofilchem.net/login.area.mic/technical_sheets/MTS40.pdf (accessed on 20 November 2022).
- Trovato, L.; Scalia, G.; Palermo, C.I.; Costanzo, C.M.; Oliveri, S. Evaluation of isavuconazole MIC strips for susceptibility testing of Aspergillus and Scedosporium species. Med. Mycol. 2019, 3, 429–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing, Overview of Antifungal ECOFFs and Clinical Breakpoints for Yeasts, Moulds and Dermatophytes Using the EUCAST E.Def 7.3, E.Def 9.3 and E.Def 11.0 Procedures, September 2020. Available online: https://www.eucast.org/astoffungi/methodsinantifungalsusceptibilitytesting/susceptibility_testing_of_yeasts (accessed on 20 November 2022).
- Guinea, J.; Recio, S.; Escribano, P.; Pelaez, T.; Gama, B.; Bouza, E. In vitro antifungal activities of isavuconazole and comparators against rare yeast pathogens. Antimicrob. Agents Chemother. 2010, 54, 4012–4015. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, K.M.; Astvad, K.M.T.; Hare, R.K.; Arendrup, M.C. EUCAST Susceptibility Testing of Isavuconazole: MIC Data for Contemporary Clinical Mold and Yeast Isolates. Antimicrob. Agents Chemother. 2019, 3, e00073-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heep, M.; Grover, P.; Brown, N.P.; Pillar, C.M.; Jones, M.E.; Sahm, D.F. Evaluation of isavuconazole e-test compared to broth microdilution antifungal susceptibility testing against quality control strains and clinical Candida isolates. In Proceedings of the Programs and Abstracts of the 17th European Congress of Clinical Microbiology and Infectious Diseases (ECCMID), Munich, Germany, 31 March–3 April 2007. [Google Scholar]
- Pappas, P.; Kauffman, C.; Andes, D.; Clancy, C.; Marr, K.; Ostrosky-Zeichner, L.; Reboli, A.; Schuster, M.; Vazquez, J.; Walsh, T.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, e1–e50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Posteraro, B.; Torelli, R.; Vella, A.; Leone, P.; De Angelis, G.; De Carolis, E.; Ventura, G.; Sanguinetti, M.; Fantoni, M. Pan-Echinocandin-Resistant Candida glabrata Bloodstream Infection Complicating COVID-19: A Fatal Case Report. J. Fungi 2020, 3, 163. [Google Scholar] [CrossRef]
- Trovato, L.; Bongiorno, D.; Calvo, M.; Migliorisi, G.; Borraccino, A.; Musso, N.; Oliveri, S.; Stefani, S.; Scalia, G. Resistance to Echinocandins Complicates a Case of Candida albicans Bloodstream Infection: A Case Report. J. Fungi 2021, 7, 405. [Google Scholar] [CrossRef] [PubMed]
- El Zein, S.; Hindy, J.R.; Kanj, S.S. Invasive Saprochaete Infections: An Emerging Threat to Immunocompromised Patients. Pathogens 2020, 3, 922. [Google Scholar] [CrossRef]
- Maligie, M.A.; Selitrennikoff, C.P. Cryptococcus neoformans resistance to echinocandins: (1,3)beta-glucan synthase activity is sensitive to echinocandins. Antimicrob. Agents Chemother. 2005, 3, 2851–2856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayadi, R.; Sitterlé, E.; d’Enfert, C.; Dannaoui, E.; Bougnoux, M.E. Candida albicans and Candida dubliniensis Show Different Trailing Effect Patterns When Exposed to Echinocandins and Azoles. Front. Microbiol. 2020, 11, 1286. [Google Scholar] [CrossRef] [PubMed]
- Arendrup, M.C.; Friberg, N.; Mares, M.; Kahlmeter, G.; Meletiadis, J.; Guinea, J. Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). How to interpret MICs of antifungal compounds according to the revised clinical breakpoints v. 10.0 European committee on antimicrobial susceptibility testing (EUCAST). Clin. Microbiol. Infect. 2020, 3, 1464–1472. [Google Scholar]
- Pfaller, M.A.; Messer, S.A.; Rhomberg, P.R.; Jones, R.N.; Castanheira, M. In vitro activities of isavuconazole and comparator antifungal agents tested against a global collection of opportunistic yeasts and molds. J. Clin. Microbiol. 2013, 51, 2608–2616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, G.R., 3rd; Wiederhold, N.P.; Sutton, D.A.; Fothergill, A.; Patterson, T.F. In vitro activity of isavuconazole against Trichosporon, Rhodotorula, Geotrichum, Saccharomyces and Pichia species. J. Antimicrob. Chemother. 2009, 3, 79–83. [Google Scholar] [CrossRef] [Green Version]
- Illnait-Zaragozi, M.T.; Martinez, G.F.; Curfs-Breuker, I.; Fernandez, C.M.; Boekhout, T.; Meis, J.F. In Vitro activity of the new azole isavuconazole (BAL4815) compared with six other antifungal agents against 162 Cryptococcus neoformans isolates from Cuba. Antimicrob. Agents Chemother. 2008, 52, 1580–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desnos-Ollivier, M.; Bretagne, S.; Boullié, A.; Gautier, C.; Dromer, F.; Lortholary, O.; French Mycoses Study Group. Isavuconazole MIC distribution of 29 yeast species responsible for invasive infections (2015–2017). Clin. Microbiol. Infect. 2019, 3, e1–e634. [Google Scholar] [CrossRef] [PubMed]
- Kullberg, B.J.; Viscoli, C.; Pappas, P.G.; Vazquez, J.; Ostrosky-Zeichner, L.; Rotstein, C.; Sobel, J.D.; Herbrecht, R.; Rahav, G.; Jaruratanasirikul, S.; et al. Isavuconazole Versus Caspofungin in the Treatment of Candidemia and Other Invasive Candida Infections: The ACTIVE Trial. Clin. Infect. Dis. 2019, 68, 1981–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, P.; Brethon, B.; Roupret-Serzec, J.; Caseris, M.; Goldwirt, L.; Baruchel, A.; de Tersant, M. Isavuconazole Treatment for Invasive Fungal Infections in Pediatric Patients. Pharmaceuticals 2022, 3, 375. [Google Scholar] [CrossRef] [PubMed]
- Astvad, K.M.T.; Hare, R.K.; Arendrup, M.C. Evaluation of the in vitro activity of isavuconazole and comparator voriconazole against 2635 contemporary clinical Candida and Aspergillus isolates. Clin. Microbiol. Infect. 2017, 3, 882–887. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N (%) | EUCAST (E. Def. 9.3) | MIC Strip Test | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC Range (mg/L) | MIC50 | MIC90 | ECOFF (mg/L) | % >ECOFF | MIC Range (mg/L) | MIC50 | MIC90 | ECOFF (mg/L) | % >ECOFF | ||
| C. albicans | 283 (44.9%) | 0.008–1 | 0.008 | 0.016 | 0.125 | 0.70 | 0.004–0.125 | 0.004 | 0.032 | 0.125 | 0 |
| C. glabrata | 53 (8.4%) | 1–2 | 2 | 2 | - | - | 0.5–4 | 2 | 2 | - | - |
| C. parapsilosis complex | 151 (24.0%) | 0.008–0.125 | 0.016 | 0.016 | 16 | 0 | 0.004–0.032 | 0.016 | 0.032 | 16 | 0 |
| C. krusei | 24 (3.8%) | 0.5–2 | 0.5 | 0.5 | 16 | 0 | 0.5–1 | 0.5 | 0.5 | 16 | 0 |
| C. tropicalis | 68 (10.8%) | 0.008–2 | 0.008 | 0.008 | 16 | 0 | 0.004–0.38 | 0.004 | 0.004 | 16 | 0 |
| C. guilliermondii | 12 (1.9%) | 0.016–0.032 | 0.016 | 0.016 | 16 | 0 | 0.016–0.032 | 0.008 | 0.008 | 16 | 0 |
| C. famata | 6 (0.9%) | 0.008 | 0.008 | 0.008 | - | - | 0.008 | 0.008 | 0.008 | - | - |
| S. capitata | 12 (1.9%) | 2 | 2 | 2 | 16 | 0 | 1 | 1 | 1 | 16 | 0 |
| S. cerevisiae | 12 (1.9%) | 0.03 | 0.03 | 0.03 | 16 | 0 | 0.004 | 0.004 | 0.004 | 16 | 0 |
| C. neoformans | 5 (0.8%) | 0.016 | 0.016 | 0.016 | 16 | 0 | 0.008 | 0.008 | 0.008 | 16 | 0 |
| Rhodotorula species | 4 (0.6%) | 0.016 | 0.016 | 0.016 | - | - | 0.008 | 0.008 | 0.008 | - | - |
| C. krusei ATCC 6258 | - | 0.016–0.06 | 0.03 | - | - | - | 0.016–0.06 | 0.03 | - | - | - |
| C. parapsilosis ATCC 22019 | - | 0.008–0.03 | 0.016 | - | - | - | 0.008–0.03 | 0.016 | - | - | - |
| N | % Essential Agreement (±2-Fold Dilution) | |
|---|---|---|
| C. albicans | 283 | 99.2% |
| C. glabrata | 53 | 98.1% |
| C. parapsilosis complex | 151 | 100% |
| C. krusei | 23 | 100% |
| C. tropicalis | 68 | 95.6% |
| C. guilliermondii | 12 | 100% |
| C. famata | 6 | 100% |
| S. capitata | 12 | 100% |
| S. cerevisiae | 12 | 100% |
| C. neoformans | 5 | 100% |
| Rhodotorula species | 4 | 100% |
| Total | 629 | 99.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo, M.; Scalia, G.; Palermo, C.I.; Oliveri, S.; Trovato, L. Comparison between EUCAST Broth Microdilution and MIC Strip Test in Defining Isavuconazole In Vitro Susceptibility against Candida and Rare Yeast Clinical Isolates. Antibiotics 2023, 12, 251. https://doi.org/10.3390/antibiotics12020251
Calvo M, Scalia G, Palermo CI, Oliveri S, Trovato L. Comparison between EUCAST Broth Microdilution and MIC Strip Test in Defining Isavuconazole In Vitro Susceptibility against Candida and Rare Yeast Clinical Isolates. Antibiotics. 2023; 12(2):251. https://doi.org/10.3390/antibiotics12020251
Chicago/Turabian StyleCalvo, Maddalena, Guido Scalia, Concetta Ilenia Palermo, Salvatore Oliveri, and Laura Trovato. 2023. "Comparison between EUCAST Broth Microdilution and MIC Strip Test in Defining Isavuconazole In Vitro Susceptibility against Candida and Rare Yeast Clinical Isolates" Antibiotics 12, no. 2: 251. https://doi.org/10.3390/antibiotics12020251