
Assessment of the Plans to Optimize Antimicrobial Use in the Pediatric Population in Catalan Hospitals: The VINCat Pediatric PROA SHARP Survey
 ,
,
Abstract
:1. Introduction
2. Results
2.1. Structure Indicators
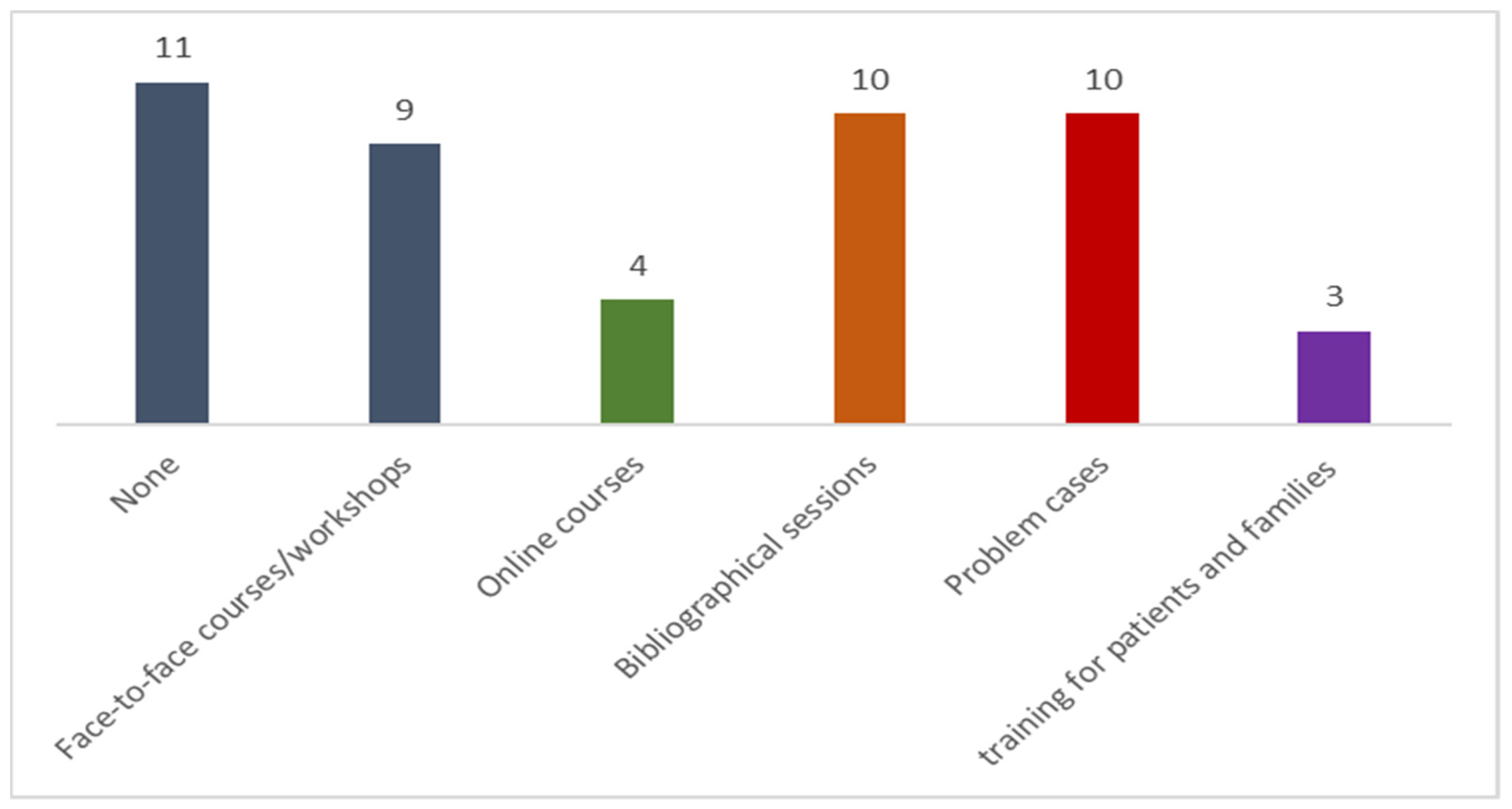
2.2. Process Indicators and Antimicrobial Stewardship Activities
3. Discussion
4. Material and Methods
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 11 December 2021).
- Aguilera-Alonso, D. It is time for pediatric antimicrobial stewardship programs. Enferm. Infecc. Microbiol. Clin. (Engl. Ed.) 2021, 39, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.H.; Moore, L.S.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef] [PubMed]
- CDC. Core Elements of Hospital Antibiotic Stewardship Programs. Atlanta, G.A. US Department of Health and Human Services, CDC. 2019. Available online: https://www.cdc.gov/antibiotic-use/core-elements/hospital.html (accessed on 2 August 2021).
- Dellit, T.H.; Owens, R.C.; McGowan, J.E.; Gerding, D.N.; Weinstein, R.A.; Burke, J.P.; Huskins, W.C.; Paterson, D.L.; Fishman, N.O.; Carpenter, C.F.; et al. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin. Infect. Dis. 2007, 44, 159–177. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Paño-Pardo, J.R.; Alvarez-Rocha, L.; Asensio, A.; Calbo, E.; Cercenado, E.; Sierra, R. Programs for optimizing the use of antibiotics (PROA) in Spanish hospitals: GEIH-SEIMC, SEFH and SEMPSPH consensus document. Enferm. Infecc. Microbiol. Clin. 2012, 30, 22.e1–22.e23. [Google Scholar] [CrossRef]
- Goycochea-Valdivia, W.A.; Melendo Pérez, S.; Aguilera-Alonso, D.; Escosa-Garcia, L.; Martínez Campos, L.; Baquero-Artigao, F.; Grupo de Trabajo PROA de la Sociedad Española de Infectología Pediátrica (SEIP). Position statement of the Spanish Society of Paediatric Infectious Diseases on the introduction, implementation and assessment of antimicrobial stewardship programmes in paediatric hospitals. An. De Pediatr. (Engl. Ed.) 2022, 97, 351.e1–351.e12. [Google Scholar] [CrossRef] [PubMed]
- Principi, N.; Esposito, S. Antimicrobial stewardship in paediatrics. BMC Infect. Dis. 2016, 16, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronman, M.P.; Banerjee, R.; Duchon, J.; Gerber, J.S.; Green, M.D.; Hersh, A.L.; Hyun, D.; Maples, H.; Nash, C.B.; Parker, S.; et al. Expanding Existing Antimicrobial Stewardship Programs in Pediatrics: What Comes Next. J. Pediatr. Infect. Dis. Soc. 2018, 7, 241–248. [Google Scholar] [CrossRef]
- Melendo, S.; Fernández-Polo, A.; Asens, I.C.; Mendoza-Palomar, N.; Barnés-Mayolas, M.; Soler-Palacín, P. Prescription quality of prolonged antibiotherapy in pediatrics. Impact of ASP program interventions. Enferm. Infecc. Microbiol. Clin. 2021, 39, 134–138. [Google Scholar] [CrossRef]
- Klatte, J.M. Pediatric Antimicrobial Stewardship Programs: Current Perspectives. Pediatr. Health Med. Ther. 2020, 11, 245–255. [Google Scholar] [CrossRef]
- Magsarili, H.K.; Girotto, J.E.; Bennett, N.J.; Nicolau, D.P. Making a case for pediatric antimicrobial stewardship programs. Pharmacotherapy 2015, 35, 1026–1036. [Google Scholar] [CrossRef]
- Goldman, J.L.; Newland, J.G. New horizons for pediatric antibiotic stewardship. Infect. Dis. Clin. N. Am. 2015, 29, 503–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simó, S.; Velasco-Arnaiz, E.; Ríos-Barnés, M.; López-Ramos, M.G.; Monsonís, M.; Urrea-Ayala, M.; Fortuny, C. Effects of a Paediatric Antimicrobial Stewardship Program on Antimicrobial Use and Quality of Prescriptions in Patients with Appendix-Related Intraabdominal Infections. Antibiotics 2020, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Arnaiz, E.; Simó-Nebot, S.; Ríos-Barnés, M.; Ramos, M.G.L.; Monsonís, M.; Urrea-Ayala, M.; Jordan, I.; Mas-Comas, A.; Casadevall-Llandrich, R.; Ormazábal-Kirchner, D.; et al. Benefits of a Pediatric Antimicrobial Stewardship Program in Antimicrobial Use and Quality of Prescriptions in a Referral Children’s Hospital. J. Pediatr. 2020, 225, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Programa de Vigilància de les Infeccions Nosocomials als Hospitals de Catalunya (VINCat). Available online: https://catsalut.gencat.cat/web/.content/minisite/vincat/documents/objectiu_6/PROA/Metodologia-VINCat-PROA.pdf (accessed on 11 December 2021).
- Gudiol, F.; Limón, E.; Fondevilla, E.; Argimon, J.M.; Almirante, B.; Pujol, M. The development and successful implementation of the VINCat Program. Enferm. Infecc. Microbiol. Clin. 2012, 30 (Suppl. 3), 3–6. [Google Scholar] [CrossRef]
- Grau, S.; Hernández, S.; Limón, E.; Calbo, E.; Horcajada, J.P.; Catalan Infection Control and Antimicrobial Stewardship National Program (VINCat-PROA). Impact of changes in the WHO’s 2019 update of DDDs on the measurement of adult hospital antibacterial consumption in Catalonia (Spain), 2008–2018. JAC Antimicrob. Resist. 2020, 2, dlaa079. [Google Scholar] [CrossRef]
- Donà, D.; Barbieri, E.; Daverio, M.; Lundin, R.; Giaquinto, C.; Zaoutis, T.; Sharland, M. Implementation and impact of pediatric antimicrobial stewardship programs: A systematic scoping review. Antimicrob. Resist. Infect. Control 2020, 9, 3. [Google Scholar] [CrossRef]
- McPherson, C.; Lee, B.R.; Terrill, C.; Hersh, A.L.; Gerber, J.S.; Kronman, M.P.; Newland, J.G. Characteristics of Pediatric Antimicrobial Stewardship Programs: Current Status of the Sharing Antimicrobial Reports for Pediatric Stewardship (SHARPS) Collaborative. Antibiotics 2018, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Newland, J.G.; Gerber, J.S.; Kronman, M.P.; Meredith, G.; Lee, B.R.; Thurm, C.; Hersh, A.L. SHARPS Collaborative. Sharing Antimicrobial Reports for Pediatric Stewardship (SHARPS): A Quality Improvement Collaborative. J. Pediatr. Infect. Dis. Soc. 2018, 7, 124–128. [Google Scholar] [CrossRef] [Green Version]
- Vergnano, S.; Bamford, A.; Bandi, S.; Chappel, F.; Demirjian, A.; Doerholt, K.; Emonts, M.; Ferreras-Antolin, L.; Goenka, A.; Jones, L.; et al. Paediatric antimicrobial stewardship programmes in the UK’s regional children’s hospitals. J. Hosp. Infect. 2020, 105, 736–740. [Google Scholar] [CrossRef]
- Registre del Conjunt Mínim Bàsic de Dades (CMBD) dels Hospital D’aguts. Servei Català de la Salut. Available online: http://catsalut.gencat.cat/ca/proveidors-professionals/registres-catalegs/registres/cmbd/informes-anuals (accessed on 11 December 2021).
- Cisneros, J.M.; Mensa, J.; Rodriguez Baño, J.; Trilla, A.; Cainzos, M. En Grupo de Infección Hospitalaria (GEIH-SEIMC). Profilaxis con antimicrobianos en Cirugía. Enferm. Infecc. Microbiol. Clin. 2002, 20, 335–340. [Google Scholar] [CrossRef]
- McQuillen, D.P.; Petrak, R.M.; Wasserman, R.B.; Nahass, R.G.; Scull, J.A.; Martinelli, L.P. The value of Infectious Diseases Specialists: Non-patient care activities. Clin. Infect. Dis. 2008, 47, 1051–1063. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Hospitals Affiliated to the VINCAT-Pediatric PROA (n = 26) | |
|---|---|
| Pediatric service (n; %) | |
| Presence of a pediatrician in the pediatric PROA | 21/26 (81%) |
| Number of pediatricians with full time dedication to the pediatric PROA ▪ one ▪ two or more | 2/26 (8%) 1/26 (4%) |
| Number of pediatricians specializing in infectious diseases in the pediatric PROA ▪ one ▪ two or more | 15/26 (58%) 2/26 (8%) |
| Pharmacy service (n; %) | |
| Presence of a pharmacist devoted to the pediatric PROA | 15/26 (58%) |
| Number of pharmacists with full time dedication to the pediatric PROA ▪ one | 0/26 (0%) |
| Microbiology service (n; %) | |
| Presence of a microbiologist devoted to the pediatric PROA | 14/26 (54%) |
| Number of microbiologists with full time dedication to the pediatric PROA ▪ one | 0/26 (0%) |
| Presence of a microbiology laboratory at the center | 24/26 (92%) |
| Performance of viral PCR at the laboratory at the center | 21/26 (81%) |
| Performance of microbiological diagnostic tests at the laboratory at the center | 22/26 (85%) |
| Electronic reports | 26/26 (100%) |
| Radiology service (n; %) | |
| Presence of pediatric radiologists | 16/26 (62%) |
| 24-h access to CT 7 days a week at the same center | 24/26 (92%) |
| 24-h access to MRI 7 days a week at the same center | 12/26 (46%) |
| Electronic reports | 25/26 (96%) |
| Hospitals Affiliated to the VINCat-Pediatric PROA (n = 26) | |
|---|---|
| Pharmacy service (n; %) | |
| No process indicators | 5/26 (19%) |
| Monitoring of antimicrobial use | |
| Clinical audit | 6/26 (23%) |
| Creation of protocols | 6/26 (23%) |
| Microbiology service (n;%) | |
| No process indicators | 7/26 (27%) |
| Monitoring of antimicrobial susceptibility | 16/26 (62%) |
| Clinical audit | 4/26 (15%) |
| Creation of protocols | 5/26 (19%) |
| YES | NO | |
|---|---|---|
| Possible audits are carried out with feedback for professionals | 62% | 38% |
| Restrictive measures are applied in prescriptions | 42% | 58% |
| Protocols are reviewed and updated | 96% | 4% |
| Presence of a protocol for surgical prophylaxis | 54% | 46% |
| Presence of an anti-infection guide for community infections in pediatrics | 73% | 27% |
| The prescription of certain antimicrobials must be justified in the computer program | 54% | 46% |
| Results of patient’s point of care tests are obtained | 58% | 42% |
| Antimicrobials are prescribed with a specific end date | 62% | 38% |
| The activities of the pediatric PROA are presented in an annual report or similar document | 23% | 77% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarch-Ibáñez, B.; Fernández-Polo, A.; Hernández, S.; Velasco-Arnaiz, E.; Giménez, M.; Sala-Castellvi, P.; Pineda, V.; Melendo, S.; VINCat Pediatric PROA Group. Assessment of the Plans to Optimize Antimicrobial Use in the Pediatric Population in Catalan Hospitals: The VINCat Pediatric PROA SHARP Survey. Antibiotics 2023, 12, 250. https://doi.org/10.3390/antibiotics12020250
Guarch-Ibáñez B, Fernández-Polo A, Hernández S, Velasco-Arnaiz E, Giménez M, Sala-Castellvi P, Pineda V, Melendo S, VINCat Pediatric PROA Group. Assessment of the Plans to Optimize Antimicrobial Use in the Pediatric Population in Catalan Hospitals: The VINCat Pediatric PROA SHARP Survey. Antibiotics. 2023; 12(2):250. https://doi.org/10.3390/antibiotics12020250
Chicago/Turabian StyleGuarch-Ibáñez, Borja, Aurora Fernández-Polo, Sergi Hernández, Eneritz Velasco-Arnaiz, Montse Giménez, Pere Sala-Castellvi, Valentí Pineda, Susana Melendo, and VINCat Pediatric PROA Group. 2023. "Assessment of the Plans to Optimize Antimicrobial Use in the Pediatric Population in Catalan Hospitals: The VINCat Pediatric PROA SHARP Survey" Antibiotics 12, no. 2: 250. https://doi.org/10.3390/antibiotics12020250