
The Impact of Care Bundles on Ventilator-Associated Pneumonia (VAP) Prevention in Adult ICUs: A Systematic Review
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Strategies
2.2. Selection and Eligibility Criteria
2.3. Data Extraction and Risk of Bias Assessment
3. Results
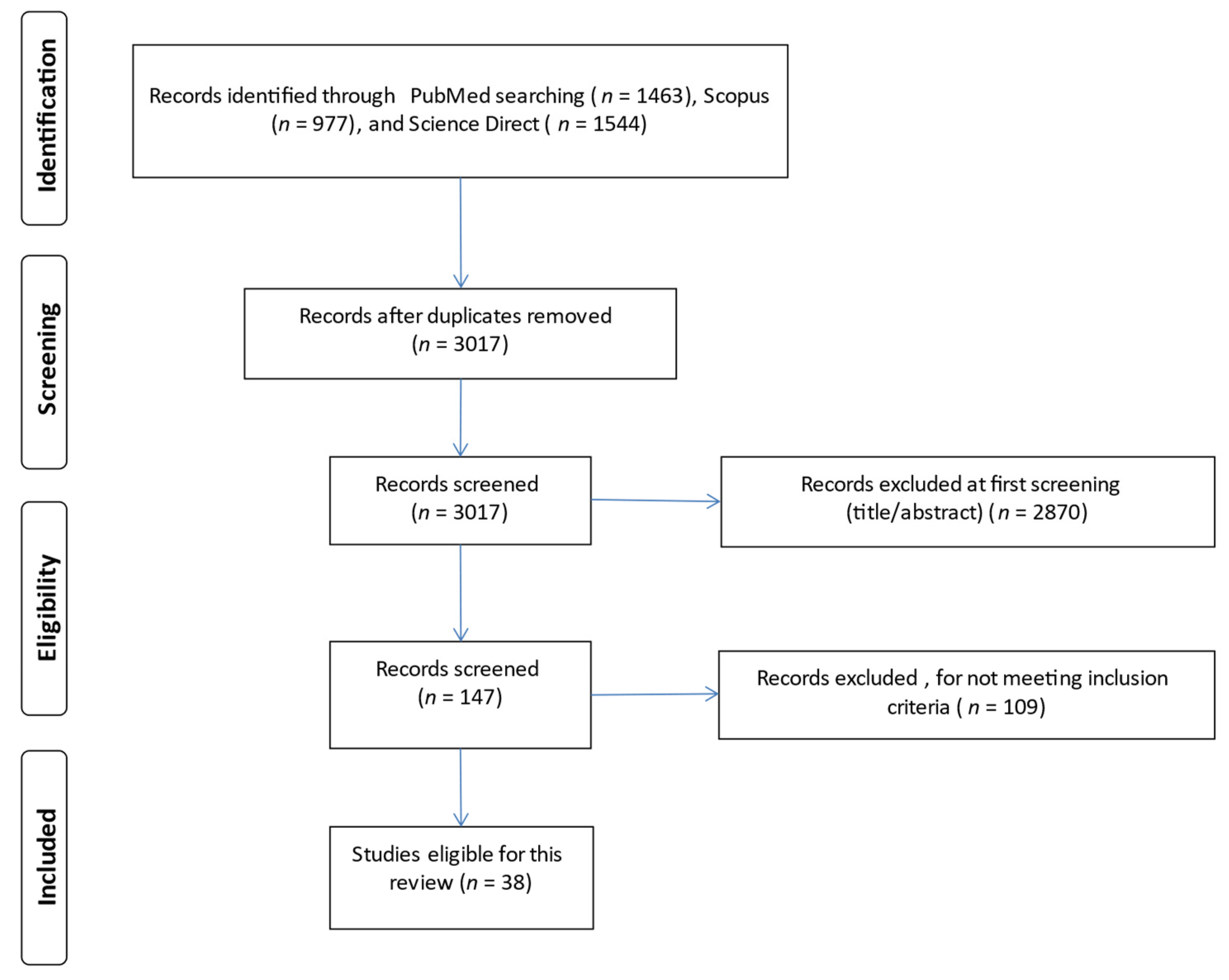
3.1. Identification and Selection of Studies
3.2. Characteristics of the Studies Included in This Review
3.3. Risk of Bias Assessment
3.4. Ventilator-Associated Care Bundles—Patients’ Outcomes
3.5. Educational Program
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klompas, M.; Branson, R.; Eichenwald, E.C.; Greene, L.R.; Howell, M.D.; Lee, G.; Magill, S.; Maragakis, L.L.; Priebe, G.P.; Speck, K.; et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 Update. Infect. Control. Hosp. Epidemiol. 2014, 35, 133–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, A.S.; Ferriso, C.; Paira, J.A. Application of a ventilator associated pneumonia prevention guideline and outcomes: A quasi-experimental study. Intensive Crit. Care Nurs. 2019, 51, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Parisi, M.; Gerovasili, V.; Dimopoulos, D.; Kampisiouli, E.; Goga, C.; Perivolioti, E.; Argyropoulou, A.; Routsi, C.; Tsiodras, S.; Nanas, S. Use of Ventilator Bundle and Staff Education to Decrease Ventilator Associated Pneumonia in Intensive Care Patients. Crit. Care Nurse 2016, 36, e1–e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pileggi, C.; Mascaro, V.; Bianco, A.; Nobile, C.G.; Pavia, M. Ventilator Bundle and Its Effects on Mortality Among ICU Patients: A Meta-Analysis. Crit. Care Med. 2018, 46, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Al-Dorzi, H.M.; Al-Attas, K.; Ahmed, F.W.; Marini, A.M.; Mundekkadan, S.; Balkhy, H.H.; Tarnous, J.; Arabi, Y.M. The impact of implementing multifaceted interventions on the prevention of ventilator-associated pneumonia. Am. J. Infect. Control. 2016, 44, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.P.; Kuo, S.W.; Ko, W.J.; Sheng, W.H.; Chang, Y.Y.; Hong, M.C.; Sun, C.C.; Chen, Y.C.; Chang, S.C. Efficacy of ventilator-associated pneumonia care bundle for prevention of ventilator-associated pneumonia in the surgical intensive care units of a medical center. J. Microbiol. Immunol. Infect. 2015, 48, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Moore, K.R. Critical Care Nursing Interventions and Incidence of Ventilator Associated Pneumonia in the Trauma Population 2012, Nursing Theses and Capstone Projects.135. Available online: https://digitalcommons.gardner-webb.edu/cgi/viewcontent.cgi?article=1134&context=nursing_etd (accessed on 1 September 2022).
- Resar, R.; Pronovost, P.; Haraden, C.; Simmond, T.; Rainey, T.; Nolan, T. Using a Bundle Approach to Improve Ventilator Care Processes and Reduce Ventilator Associated Pneumonia. J. Qual. Patient Saf. 2005, 31, 243–248. [Google Scholar] [CrossRef]
- Munro, N.; Ruggiero, M. Ventilator-Associated Pneumonia Bundle. Reconstruction for Best Care. AACN Adv. Crit. Care 2014, 25, 163–175. [Google Scholar] [CrossRef]
- Kandeel, N.; Tantawy, N. Current Nursing Practice for Prevention of Ventilator Associated Pneumonia in ICUs. Life Sci. J. 2012, 9, 966–975. [Google Scholar]
- Chahoud, J.; Semaan, A.; Almoosa, K. Ventilator-associated events prevention, learning lessons from the past: A systematic review. Heart Lung 2015, 44, 251–259. [Google Scholar] [CrossRef]
- Alecrim, R.X.; Taminato, M.; Belasco, A.; Longo, M.C.; Lusahara, D.M.; Fram, D. Strategies for preventing ventilator-associated pneumonia: An integrative review. Rev. Bras. Enferm. 2019, 72, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Kallet, R.H. Ventilator Bundles in Transition: From Prevention of Ventilator Associated Pneumonia to Prevention of Ventilator-Associated Events. Respir. Care 2019, 8, 994–1006. [Google Scholar] [CrossRef] [PubMed]
- Thapa, D.; Liu, T.; Chair, S.Y. Multifaceted interventions are likely to be more effective to increase adherence to the ventilator care bundle: A systematic review of strategies to improve care bundle compliance. Intensive Crit. Care Nurs. 2022, 74, 103310. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Berenholtz, S.M.; Pham, J.C.; Thompson, D.A.; Needham, D.M.; Lubomski, L.H.; Hyzy, R.C.; Welsh, R.; Cosgrove, S.E.; Sexton, J.B.; Colantuoni, E.; et al. Collaborative Cohort Study of an Intervention to Reduce Ventilator-Associated Pneumonia in the Intensive Care Unit. Infect. Control. Hosp. Epidemiol. 2011, 32, 305–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaban, A.M.; El-Mokadem, N.M.; Abdallah, S.E. Effectiveness of Implementing Ventilator Associated Pneumonia Prevention Bundle among Mechanically Ventilated Patients. Int. J. Nov. Res. Healthc. Nurs. 2021, 8, 329–342. [Google Scholar]
- Marini, A.L.; Khan, R.; Mundekkadan, S. Multifaceted bundle interventions shown effective in reducing VAP rates in our multidisciplinary ICUs. BMJ Qual. Improv. Rep. 2016, 5, u205566-w2278. [Google Scholar] [CrossRef] [Green Version]
- Ismail, R.; Zahran, E. The effect of nurses training on ventilator-associated pneumonia (VAP) prevention bundle on VAP incidence rate at a critical care unit. J. Nurs. Educ. Pract. 2015, 5, 42–48. [Google Scholar] [CrossRef] [Green Version]
- AÁlvarez-Lerma, F.; Palomar-Martínez, M.; Sánchez-García, M.; Martínez-Alonso, M.; Álvarez-Rodríguez, J.; Lorente, L.; Arias-Rivera, S.; García, R.; Gordo, F.; Añón, J.M.; et al. Prevention of Ventilator-Associated Pneumonia: The Multimodal Approach of the Spanish ICU “Pneumonia Zero” Program. Crit. Care Med. 2018, 46, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Cengiz, H.O.; Kanan, N. The effectiveness of training given to nurses for reducing ventilator-associated pneumonia in intensive care patients. Dev. Health Sci. 2019, 2, 36–45. [Google Scholar]
- Chen, J.K.; Chen, T.H.; Liu, H.E.; Kao, C.C.; Chen, C.F.; Ou, T.Y.; Tseng, P.C.; Kuo, K.N.; Lee, W.S. Bundle Care for Preventing Ventilator-associated Pneumonia at a Medical Center: A Preliminary Report. J. Exp. Clin. Med. 2014, 6, 157–160. [Google Scholar] [CrossRef]
- Eom, J.S.; Lee, M.S.; Chun, H.K.; Choi, H.J.; Jung, S.Y.; Kim, Y.S.; Yoon, S.J.; Kwak, Y.G.; Oh, G.B.; Jeon, M.H.; et al. The impact of a ventilator bundle on preventing ventilator-associated pneumonia: A multicenter study. Am. J. Infect. Control. 2014, 42, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Landelle, C.; NocquetBooyer, V.; Abbas, M.; Genevois, E.; Abidi, N.; Naimo, S.; Raulais, R.; Bouchoud, L.; Boroli, F.; Terrisse, H.; et al. Impact of a multifaceted prevention program on ventilator-associated pneumonia including selective oropharyngeal decontamination. Intensive Care Med. 2018, 44, 1777–1786. [Google Scholar] [CrossRef] [PubMed]
- Mogyorodi, B.; Dunai, E.; Gal, J.; Ivanyi, Z. Ventilator—Associated pneumonia and the importance of education of ICU nurses on prevention—Preliminary results. Interv. Med. Appl. Sci. 2016, 8, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Fortaleza, C.M.C.B.; Filho, S.P.F.; Silva, M.O.; Queiroz, S.M.; Cavalcante, R.S. Sustained reduction of healthcare-associated infections after the introduction of a bundle for prevention of ventilator-associated pneumonia in medical-surgical intensive care units. Braz. J. Infect. Dis. 2020, 24, 373–379. [Google Scholar] [CrossRef]
- Zeng, W.P.; Su, H.; Chen, C.W.; Cheng, S.M.; Chang, L.F.; Tzeng, W.C.; Tzeng, B.H. Care Bundle for Ventilator-Associated Pneumonia in a Medical Intensive Care Unit in Northern Taiwan. J. Med. Sci. 2015, 35, 68–73. [Google Scholar]
- Al-Tawfiq, J.A.; Abed, M.S. Decreasing ventilator-associated pneumonia in adult intensive care units using the Institute for Healthcare Improvement bundle. Am. J. Infect. Control. 2010, 38, 552–556. [Google Scholar] [CrossRef]
- Bird, D.; Zambuto, A.; O’Donnell, C.; Silva, J.; Korn, C.; Burke, R.; Burke, P.; Agarwal, S. Adherence to Ventilator-Associated Pneumonia Bundle and Incidence of Ventilator-Associated Pneumonia in the Surgical Intensive Care Unit. Achieves Surg. 2010, 145, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Branco, A.; Louvencone, E.M.; Monteiro, A.B.; Fonseca, J.P.; Blatt, C.R.; Caregnato, R.C. Education to prevent ventilator-associated pneumonia in intensive care unit. Rev. Bras. De Enferm. 2020, 73, e20190477. [Google Scholar] [CrossRef]
- Ban, K.O. The effectiveness of an evidence-based nursing program to reduce ventilator-associated pneumonia in a Korean ICU. Intensive Crit. Care Nurs. 2011, 27, 226–232. [Google Scholar] [CrossRef]
- Viana, W.N.; Bragazzi, C.; Couto de Castro, J.E.; Alves, M.B.; Rocco, J.R. Ventilator-associated pneumonia prevention by education and two combined bedside strategies. Int. J. Qual. Health Care 2013, 25, 308–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcan, A.O.; Korkmaz, F.D.; Uyar, M. Prevention of ventilator—Associated pneumonia: Use of the care bundle approach. Am. J. Infect. Control. 2016, 44, e173–e176. [Google Scholar] [CrossRef] [PubMed]
- Dosher, W.B.; Loomis, E.C.; Richardson, S.L.; Crowell, J.A.; Waltman, R.D.; Miller, L.D.; Nazim, M.; Khasawneh, F.A. The effect of a Nurse—Led Multidisciplinary Team on Ventilator—Associated Pneumonia Rates. Crit. Care Res. Pract. 2014, 2014, 682621. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, J.A. Implementation of VentilatorAssociated Pneumonia Clinical Guideline (Bundle). J. Nurse Pract. 2012, 8, 377–382. [Google Scholar] [CrossRef]
- Righi, E.; Aggazzotti, G.; Ferrari, E.; Giovanardi, C.; Busani, S.; Rinaldi, L.; Girardis, M. Trends in ventilator-associated pneumonia: Impact of a ventilator care bundle in an Italian tertiary care hospital intensive care unit. Am. J. Infect. Control. 2014, 42, 1312–1316. [Google Scholar] [CrossRef]
- Gatell, M.R.; Roig, M.S.; Vian, O.H.; Santin, E.C.; Duaso, C.T.; Moreno, I.F.; Daunis, J.V. Assessment of a training programme for the prevention of ventilator-associated pneumonia. Br. Assoc. Crit. Care Nurses 2012, 17, 285–292. [Google Scholar] [CrossRef] [Green Version]
- Kao, C.C.; Chiang, H.T.; Chen, C.Y.; Hung, C.T.; Chen, Y.C.; Su, L.H.; Shi, Z.Y.; Liu, J.W.; Liu, C.P.; Chuang, Y.C.; et al. National bundle care program implementation to reduce ventilator-associated pneumonia in intensive care units in Taiwan. J. Microbiol. Immunol. Infect. 2019, 52, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, Y.; Zhang, K.; Hai, Y.; Li, H.; Xing, H.; Xu, B.; Bai, H.; Zhao, H.; Bao, H.; et al. Evaluation of the effects of applying the ventricular care bundle (VCB) method for reducing ventilator-associated pneumonia (VAP) in the intensive care unit of a general Chinese tertiary hospital. Ann. Palliat. Med. 2020, 9, 2853–2861. [Google Scholar] [CrossRef]
- Guanche-Garcell, H.; Morales-Perez, C.; Rosenthal, V.D. Effectiveness of a multidimensional approach for the prevention of ventilator-associated pneumonia in an adult intensive care unit in Cuba: Findings of the International Nosocomial Infection Control Consortium (INICC). J. Infect. Public Health 2013, 6, 98–107. [Google Scholar] [CrossRef] [Green Version]
- Micik, S.; Besic, N.; Johnson, N.; Han, M.; Harnlyn, S.; Ball, H. Reducing risk for ventilator associated pneumonia through nursing sensitive interventions. Intensive Crit. Care Nurs. 2013, 29, 261–265. [Google Scholar] [CrossRef]
- Burja, S.; Belec, T.; Bizjak, N.; Mori, J.; Markota, A.; Sinkovic, A. Efficacy of a bundle approach in preventing the incidence of ventilator associated pneumonia (VAP). Bosn. J. Basic Med. Sci. 2018, 18, 105–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouadma, L.; Mourvillier, B.; Deiler, V.; Le Corre, B.; Lolom, I.; Regnier, B.; Wolff, M.; Lucet, J.C. A multifaceted program to prevent ventilator—Associated pneumonia: Impact on compliance with preventive measures. Crit. Care Med. 2010, 38, 789–796. [Google Scholar] [CrossRef]
- Michelangelo, H.; Angriman, F.; Pizarro, R.; Bauque, S.; Kecskes, C.; Staneloni, I.; Garcia, D.; Espinola, F.; Mazer, G.; Ferrari, C. Implementation of an experiential learning strategy to reduce the risk of ventilator-associated pneumonia in critically ill adult patients. J. Intensive Care Soc. 2020, 21, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Morris, A.C.; Hay, A.W.; Swann, D.G.; Everingham, K.; McCulloch, C.; McNulty, J.; Brooks, O.; Laurenson, I.F.; Cook, B.; Walsh, T.S. Reducing ventilator-associated pneumonia in intensive care: Impact of implementing a care bundle. Crit. Care Med. 2011, 39, 2218–2224. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Hein, E.; Choi, S.J.; Gomez-Santillan, J.A.; Oyervides-Alvarado, J.A.; Galindo-Fraga, A.; Rivero-Sigarroa, E.; Hernandez-Gilsoul, T.; Dominguez-Cherit, J.G. Near-zero ventilator-associated pneumonia rates after implementation of a multimodal preventive strategy in a Mexican hospital. Am. J. Infect. Control 2020, 48, 446–447. [Google Scholar] [CrossRef]
- Colombo, S.M.; Palomeque, A.C.; Bassi, G. The zero-VAP sophistry and controversies surrounding prevention of ventilator-associated pneumonia. Intensive Care Med. 2020, 46, 368–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leblebicioglu, H.; Yalcin, A.N.; Rosenthal, V.D.; Koksal, I.; Sirmatel, F.; Unal, S.; Turgut, H.; Ozdemir, D.; Ersoz, G.; Uzun, C. Effectiveness of a multidimensional approach for prevention of ventilator-associated pneumonia in 11 adult intensive care units from 10 cities of Turkey: Findings of the International Nosocomial Infection Control Consortium (INICC). Infection 2013, 41, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Mehta, Y.; Jaggi, N.; Rosenthal, V.D.; Rodrigues, C.; Todi, S.K.; Saini, N.; Udwadia, F.E.; Karlekar, A.; Kothari, V.; Myatra, S.N.; et al. Effectiveness of a multidimensional approach for prevention of ventilator-associated pneumonia in 21 adult intensive-care units from 10 cities in India: Findings of the International Nosocomial Infection Control Consortium (INICC). Epidemiol. Infect. 2013, 141, 2483–2491. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ID | Reference | Country | Data Collection Period | Study Setting | Sample Size | Mean Age of Patients (Standard Deviation) | Educational Program (Yes/No/NA) |
|---|---|---|---|---|---|---|---|
| 1. | Al-Tawfiq et al. (2010) | Saudi Arabia | 1 January 2006–31 December 2008 | One 18-bed ICU | NA | NA | yes |
| 2. | Bouadma et al. (2010) | France | 2-year period (Months and year NA) | One 20-bed MICU | 1649 ventilator days | NA | yes |
| 3. | Bird et al. (2010) | USA | 1 March 2006–31 May 2009 | Two SICUs | NA | NA | NA |
| 4. | Ban et al. (2011) | Korea | 31 October 2005–28 February 2006 | One ICU | 155 patients | NA | yes |
| 5. | Berenholtz et al. (2011) | USA | 1 October 2003–30 September 2005 | 81 ICUs | 550,800 ventilator days | NA | yes |
| 6. | Morris et al. (2011) | Scotland | NA | One 18-bed ICU | pre: 1460 patients post: 501 patients | pre: 60 (47–72) * post: 59 (48–70) * | yes |
| 7. | Gallagher et al. (2012) | USA | 31 August 2010–30 September 2011 | One ICU | 83 patients | 63 (NA) | yes |
| 8. | Moore et al. (2012) | USA | 1 January 2011–30 June 2012 | One 16-bed combined Neurosurgical & Trauma ICU | 1987 patients | NA | NA |
| 9. | Gatell et al. (2012) | Spain | 1 January 2008–31 May 2009 | One 16-bed GICU | NA | NA | yes |
| 10. | Guanche-Garcell et al. (2013) | Cuba | 31 January 2007–30 November 2010 | One ICU | pre: 67 patients post: 1008 patients | pre: 60 (17.6) post: 61.4 (17.6) | yes |
| 11. | Leblebicioglu et al. (2013) | Turkey | 31 August 2003–31 January 2009 | 11 ICUs | pre: 448 patients post: 3864 patients | pre: 52.4 (22.5) post: 49 (21.6) | yes |
| 12. | Mehta et al. (2013) | India | 31 July 2004–31 October 2011 | 21 ICUs | pre: 3979 patients post: 42,966 patients | pre: 54.8 (17.8) post: 54.5 (18.3) | yes |
| 13. | Micik et al. (2013) | Australia | 1 April 2011–31 August 2012 | One 8-bed cardiothoracic ICU | NA | NA | yes |
| 14. | Viana et al. (2013) | Brazil | 1 January 2014–30 June 2008 | One 14-bed ICU | pre: 294 patients post: 224 patients | pre: 77 (65–85) * post: 76 (61–83) * | NA |
| 15. | Chen et al. (2014) | Taiwan | 1 January 2010–31 December 2012 | One MICU & one SICU | NA | NA | yes |
| 16. | Docher et al. (2014) | USA | 1 April 2009–30 September 2012 | One 18-bed MICU | 713 patients | 58.8 (17.5) | yes |
| 17. | Eom et al. (2014) | Korea | 31 July 2010–30 June 2011 | 6 ICUs | NA | NA | yes |
| 18. | Righi et al. (2014) | Italy | 31 January 2004–31 December 2010 | One 10-bed ICU | 1372 patients | 61.1 (17.1) | NA |
| 19. | Ismail et al. (2015) | Lebanon | NA | One CCU | pre: 15 patients post: 28 patients | pre: 67.1 (16.5) post: 56.2 (25.7) | yes |
| 20. | Lim et al. (2015) | Taiwan | 1 January 2006–31 March 2013 | 5 SICUs | 27,125 patients pre: 12,913 patients post: 14,212 patients | pre: 63.2 (NA) post: 62.8 (NA) | yes |
| 21. | Zeng et al. (2015) | China | 1 December 2011–31 May 2014 | One MICU | 375 patients | NA | NA |
| 22. | Alcan et al. (2016) | Turkey | 7 April 2014–31 October 2014 | One GICU | 128 patients | NA | yes |
| 23. | Khan et al. (2016) | Saudi Arabia | 2008–2013 | One GICU | 3665 patients | 53.2 (21) | yes |
| 24. | Mogyorodi et al. (2016) | Hungary | 1 January 2015–31 December 2015 | One 12-bed ICU | 535 patients pre: 275 patients post: 260 patients | pre: 69.8 (14.3) post: 68.7 (14.0) | yes |
| 25. | Marini et al. (2016) | Saudi Arabia | 31 October 2012–30 June 2014 | One GICU | NA | NA | yes |
| 26. | Parisi et al. (2016) | Greece | 2–year study period | One 30-bed ICU | pre: 226 patients post: 136 patients | pre: 59 (41–73) * post: 58 (42–72) * | yes |
| 27. | Alvarez–Lerma et al. (2018) | Spain | 1 April 2011–31 December 2012 | One hundred eighty-one ICUs | 171,237 patients | NA | yes |
| 28. | Burja et al. (2018) | Slovenia | 1 September 2014–30 April 2015 | One 12-bed MICU | pre: 55 patients post: 74 patients | pre: 67.8 (14.5) post: 64.8 (13.7) | yes |
| 29. | Landelle et al. (2018) | Switzerland | 31 August 2014–31 July 2016 | One 34-bed ICU | pre: 291 patients post: 356 patients | pre: 61.9 (48.6–73.4) * post: 60.5 (49.4–71.2) * | yes |
| 30. | Cengiz et al. (2019) | Turkey | 1 January 2015–30 January 2016 | 9 ICUs | NA | NA | yes |
| 31. | Kao et al. (2019) | Taiwan | 1 January 2012–31 October 2014 | 7 SICUs, one CV/SICU, two MICUs | NA | NA | yes |
| 32. | Sousa et al. (2019) | Portugal | 31 October 2015–31 March 2017 | 3 ICUs | 828 patients | NA | yes |
| 33. | Branco et al. (2020) | Brazil | 30 June 2017–30 June 2018 | One GICU | 302 patients | 62.4 (17.1) | yes |
| 34. | Fortaleza et al. (2020) | Brazil | 1 January 2007–30 June 2019 | Two ICUs | NA | NA | yes |
| 35. | Liu et al. (2020) | China | 1 June 2017–31 May 2019 | 6 ICUs | 4716 patients | NA | NA |
| 36. | Michelangelo et al. (2020) | Argentina | 31 January 2016–31 December 2018 | 3 ICUs | NA | NA | yes |
| 37. | Ochoa-Hein et al. (2020) | Mexico | 2015–2018 | One 14-bed ICU | NA | NA | yes |
| 38. | Shaban et al. (2021) | Egypt | 31 March 2020–28 February 2021 | Two ICUs | pre: 52 patients post: 52 patients | pre: 58.4 (4.4) post: 57.8 (2.9) | NA |
| ID | Reference | Physicians’ Interventions | Nurses’ Interventions | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IHI Ventilator | Bundle | |||||||||||||||||||||
| Avoid Nasogastric Tube | Avoid Nasotracheal Intubation | PUD Prophylaxis | DVT Prophylaxis | Daily Sedation Vacation | Daily Assessment of Readiness for Extubating | HOB Elevation 30°–45° | Oral Care/Chlorhexidine 0.12% | Adequate ETT Cuff Pressure (20–30 cm H2O) | Subglottic Suctioning | Hand Hygiene | Aseptic Suctioning Technique | Avoid Accidental Extubation | Avoid Gastric Overdistension | Adherence to Recommended Frequency of Equipment Change ** | Suction When Necessary | Suitable Use & Replacement of HME Filters | Closed Suction System | Change Soiled/Damaged VC | Condensate Removal | Other | ||
| 1. | Al-Tawfiq et al. (2010) | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| 2. | Bird et al. (2010) | √ | √ | √ | √ | √ | ||||||||||||||||
| 3. | Bouadma et al. (2010) | √ | √ | √ | √ | √ | √ | √ | gloves gowns | |||||||||||||
| 4. | Ban et al. (2011) | √ | √ | √ | √ | √ | √ | gloves | ||||||||||||||
| 5. | Berenholtz et al. (2011) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||
| 6. | Gallagher et al. (2012) | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 7. | Morris et al. (2011) | √ | √ | √ | √ | |||||||||||||||||
| 8. | Moore et al. (2012) | √ | √ | √ | √ | √ | ||||||||||||||||
| 9. | Gatell et al. (2012) | √ | √ | √ | √ | √ | √ | √ | √ | (b) | ||||||||||||
| 10. | Guanche-Garcell et al. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | (c) | ||||||||
| 11. | Leblebicioglu et al. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | (c) (j) | ||||||||||
| 12. | Mehta et al. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | (c) (j) | ||||||||||
| 13. | Micik et al. (2013) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||
| 14. | Viana et al. (2013) | √ | √ | √ | √ | √ | √ **** | |||||||||||||||
| 15. | Chen et al. (2014) | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| 16. | Docher et al. (2014) | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| 17. | Eom et al. (2014) | √ | √ | √ | √ | |||||||||||||||||
| 18. | Righi et al. (2014) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | SDD | ||||||||||
| 19. | Ismail et al. (2015) | √ | √ | √ | √ | √ | √ | √ | √ | gloves | ||||||||||||
| 20. | Lim et al. (2015) | √ | √ | √ | √ | √ | √ | √ | √ | (a) | ||||||||||||
| 21. | Zeng et al. (2015) | √ | √ | √ | √ | √ | √ | √ | √ | (l) | ||||||||||||
| 22. | Alcan et al. (2016) | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 23. | Khan et al. (2016) | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 24. | Mogyorodi et al. (2016) | √ | √ | √ | √ | √ | √ | √ | √ | √ | ||||||||||||
| 25. | Marini et al. (2016) | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 26. | Parisi et al. (2016) | √ | √ | √ | √ | √ | √ *** | |||||||||||||||
| 27. | Alvarez-Lerma et al. (2018) | √ | √ | √ | √ | √ | √ | √ | (e) | |||||||||||||
| 28. | Burja et al. (2018) | √ | √ | √ | √ | √ | √ | √ | ||||||||||||||
| 29. | Landelle et al. (2018) | √ | √ | √ | √ | √ | √ | √ | (i) SOD | |||||||||||||
| 30. | Cengiz et al. (2019) | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | (f) | ||||||||||
| 31. | Kao et al. (2019) | √ | √ | √ | √ | √ | √ | (h) | ||||||||||||||
| 32. | Sousa et al. (2019) | √ | √ | √ | √ | √ | √ | √ | (c) (i) | |||||||||||||
| 33. | Branco et al. (2020) | √ | √ | √ | √ | √ | √ | |||||||||||||||
| 34. | Fortaleza et al. (2020) | √ | √ | √ | √ | (h) | ||||||||||||||||
| 35. | Liu et al. (2020) | √ | √ | √ | √ | √ | √ | √ | √ | |||||||||||||
| 36. | Michelangelo et al. (2020) | √ | √ | √ | √ | |||||||||||||||||
| 37. | Ochoa-Hein et al. (2020) | √ * | √ * | √ | √ | √ | √ | √ | √ | (k) | ||||||||||||
| 38. | Shaban et al. (2021) | √ | √ | √ | √ | √ | ||||||||||||||||
| ID | Reference | Pre-Intervention VAP | Post-Intervention VAP | p-Value | Comments |
|---|---|---|---|---|---|
| 1. | Al-Tawfiq et al. (2010) | 9.3 | 1-year after: 2.3 2-years after: 2.2 | p < 0.001 | |
| 2. | Bouadma et al. (2010) | 23.5 (26.7%) | 1-year after: 14.9 (15.3%) 2-years after: 11.5(11.1%) | p < 0.0001 | |
| 3. | Bird et al. (2010) | 10.2 | 3.4 | NA | |
| 4. | Ban et al. (2011) | 17.4 | 11.04 | p = 0.074 | |
| 5. | Berenholz et al. (2011) | 6.9 | 16-months after: 3.4 28–30 months after: 2.4 | NA | |
| 6. | Morris et al. (2011) | 32.0 | 12.0 | p < 0.001 | |
| 7. | Gallagher et al. (2012) | 25.5 | 0.0 | p = 0.003 | |
| 8. | Moore et al. (2012) | 4.5 | Ranged per quarter | NA | The VAP rate per quarter (total 6 quarters) ranged from 1.94 to 6.55 (M = 4.33, SD: 1.65) |
| 9. | Gatell et al. (2012) | 9.9 | 9.3 | p = 0.36 | VAP incidence (>4 days after intubation): 4.6 vs. 3.1 |
| 10. | Guanche-Garcell et al. (2013) | 52.6 | 15.3 | p = 0.003 | 70% reduction |
| 11. | Leblebicioglu et al. (2013) | 31.1 | 16.8 | p = 0.0001 | |
| 12. | Mehta et al. (2013) | 17.4 | 10.8 | p = 0.0001 | 38% reduction |
| 13. | Micik et al. (2013) | 13.4 | 7.7 | NA | |
| 14. | Viana et al. (2013) | 18.6 | 11.8 | p = 0.002 | |
| 15. | Chen et al. (2014) | 1.5 | 0.0 | NA | |
| 16. | Docher et al. (2014) | 9.3 | Ranged per month | p < 0.001 | ●Mean after IVR: 3.2 (SD: 5.71). ●Average VAP reduction/month: 0.27 |
| 17. | Eom et al. (2014) | 4.08 | 1.16 | NA | |
| 18. | Righi et al. (2014) | 15.9% | 6.7% | p < 0.001 | * VAP bundle period: 2004–2007 * VAP bundle & SOD period: 2008–2010 ●EVAP (6.6% to 1.9%) ●LVAP (9.3% to 4.7%) |
| 19. | Ismail et al. (2015) | 66.7% | 21.4% | p = 0.003 | |
| 20. | Lim et al. (2015) | 13.63 | 3.9 | p < 0.001 | ●Ventilator utilization ratio decreased by 9.9% & VAP density reduced by 1.9 cases/1000 ventilator days (up to a 57.6% reduction) |
| 21. | Zeng et al. (2015) | 0.495 | 0.281 | p = 0.001 | |
| 22. | Alcan et al. (2016) | 15.91 | 8.50 | p = 0.0001 | |
| 23. | Khan et al. (2016) | 8.6 | 2.0 | p < 0.001 | |
| 24. | Mogyorodi et al. (2016) | 21.5 (95% CI: 14.17–31.10) | 12.0 (95% CI: 7.2–19.49) | NA | Relative risk reduction: 44% (95% CI: −0.5 to 0.98) |
| 25. | Marini et al. (2016) | 4.0 | 0.8 | NA | |
| 26. | Parisi et al. (2016) | 21.6 | 11.6 | p = 0.01 | |
| 27. | Alvarez-Lerma et al. (2018) | 9.83 (95% CI: 8.42–11.48) | 4.34 (95% CI: 3.22–5.84) | NA | |
| 28. | Burja et al. (2018) | Total: 41.8% EVAP: 10.9% LVAP: 30.9% | Total: 25.7% EVAP: 12.2% LVAP: 13.5% | Total: p = 0.061 EVAP: p > 0.99 LVAP: 0.027 | |
| 29. | Landelle et al. (2018) | 24.0 | 3.9 | p < 0.001 | ●IVR without SOD: reduction 42% ●IVR with SOD: reduction 70% |
| 30. | Cengiz et al. (2019) | 12.856 | 6.866 | p = 0.036 | |
| 31. | Kao et al. (2019) | Total: 1.9 CV/SICU: 4.5 SICUs: 2.1 MICUs: 0.5 | Total: 1.5 CV/SICU: 4.5 SICUs: 1.4 MICUs: 1.0 | Total: p = 0.005 CV/SICU: p = 0.5391 SICUs: p < 0.001 MICUs: p = 0.0489 | |
| 32. | Sousa et al. (2019) | Total: 7.89 ICU A: 4.0% ICU B: 2.4% ICU C: 7.1% | Total: 6.81 ICU A: 4.7% ICU B: 2.1% ICU C: 3.5% | Total: p = 0.552 ICU A: p = 0.539 ICU B: p = 0.001 ICU C: p = 0.02 | |
| 33. | Branco et al. (2020) | 7.99 | 4.28 | p < 0.001 | |
| 34. | Fortaleza et al. (2020) | 36.58 | 12.04 | p < 0.001 | |
| 35. | Liu et al. (2020) | 18.85 | 13.70 | p = 0.019 | |
| 36. | Michelangelo et al. (2020) | 6.11 | 3.55 | p < 0.01 | |
| 37. | Ochoa et al. (2020) | 8.2 | 3.1 | p = 0.019 | |
| 38. | Shaban et al. (2021) | 62.20% | 26.90% | p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastrogianni, M.; Katsoulas, T.; Galanis, P.; Korompeli, A.; Myrianthefs, P. The Impact of Care Bundles on Ventilator-Associated Pneumonia (VAP) Prevention in Adult ICUs: A Systematic Review. Antibiotics 2023, 12, 227. https://doi.org/10.3390/antibiotics12020227
Mastrogianni M, Katsoulas T, Galanis P, Korompeli A, Myrianthefs P. The Impact of Care Bundles on Ventilator-Associated Pneumonia (VAP) Prevention in Adult ICUs: A Systematic Review. Antibiotics. 2023; 12(2):227. https://doi.org/10.3390/antibiotics12020227
Chicago/Turabian StyleMastrogianni, Maria, Theodoros Katsoulas, Petros Galanis, Anna Korompeli, and Pavlos Myrianthefs. 2023. "The Impact of Care Bundles on Ventilator-Associated Pneumonia (VAP) Prevention in Adult ICUs: A Systematic Review" Antibiotics 12, no. 2: 227. https://doi.org/10.3390/antibiotics12020227