

Tissue Penetration of Antimicrobials in Intensive Care Unit Patients: A Systematic Review—Part I
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Beta-Lactams
2.1.1. Penicillins

{kind=link}
| Drugs | Piperacillin (Pip/Tazo) | Ceftazidime | Ceftriaxone | Cefepime | Meropenem (Mer/Vab) | Imipenem [Imip/Rel] |
|---|---|---|---|---|---|---|
| Daily doses | −4.5 g q6h −22 g CI | −6 g CI −20 mg/kg q8h −2 g q8h | −1–2 g | −2 g q12h −4 g CI | −1 g q8h −2 g q8h EI or CI −[2 + 2 g q8h, 3 h-inf] | −1 g q6h −[0.5/0.25 g q6h] |
| CNS | 0.24X (2 h) | <0.1X (2 h) | 0.21X (2.5 h) | |||
| CSF | <0.1X | 0.3–2.14X A 0.03–1.14X B | 0.08X | <0.1X (1–4 h) | ||
| Lung tissue | 0.28 (0.5 h)–0.92X (1.5 h) | 0.45X (1 h) | >0.8X (0.5 h) | |||
| ELF | [0.4–0.5X/0.65–0.85X] | 0.21–0.44X 0.21X | 1X | 0.25–0.3X [0.52–1.85X/0.44–0.74X] | 0.2X (2 h) [0.3–0.6X/0.3–0.5X] | |
| Bronchial secretion | 0.02–0.25X | 0.76X | 0.02X | |||
| Bronchial mucosa | 0.6X | |||||
| Abdomen | 0.43–0.53X C | 0.35–0.56X D | 0.09X E | 0.51X | 0.74X D | |
| Bone | 0.1–0.4X 1X [0.5/0.4X] F | 0.1–0.3X (0.5 h) | 0.48X (1.5 h) 0.1–0.4X (2–2.5 h) | 0.87–1.06X | 0.4–1X | 0.4X >0.5X |
| Skin | 0.6–0.95X | 0.53X (4 h) | >1X (2 h) | >0.8X | ||
| ISF | 1X | 1X | 0.60–0.74X | |||
| Muscle | 0.18–0.3X | 0.1X | ||||
| Subcutis | 0.1–0.2X | 0.44–0.57X | 0.14X | |||
| Fat | 0.1X | 0.8X | ||||
| References | [16,17,18,19,20,21,22] | [20,23,24] | [25,26,27] | [20,28,29,30,31] | [14,20,24,32,33,34,35,36] | [14,20] |
2.1.2. Cephalosporins
2.1.3. Carbapenems
2.2. Glycopeptides
2.3. Other Antibacterial Drugs
2.3.1. Daptomycin
2.3.2. Fosfomycin
2.3.3. Colistin
3. Discussion
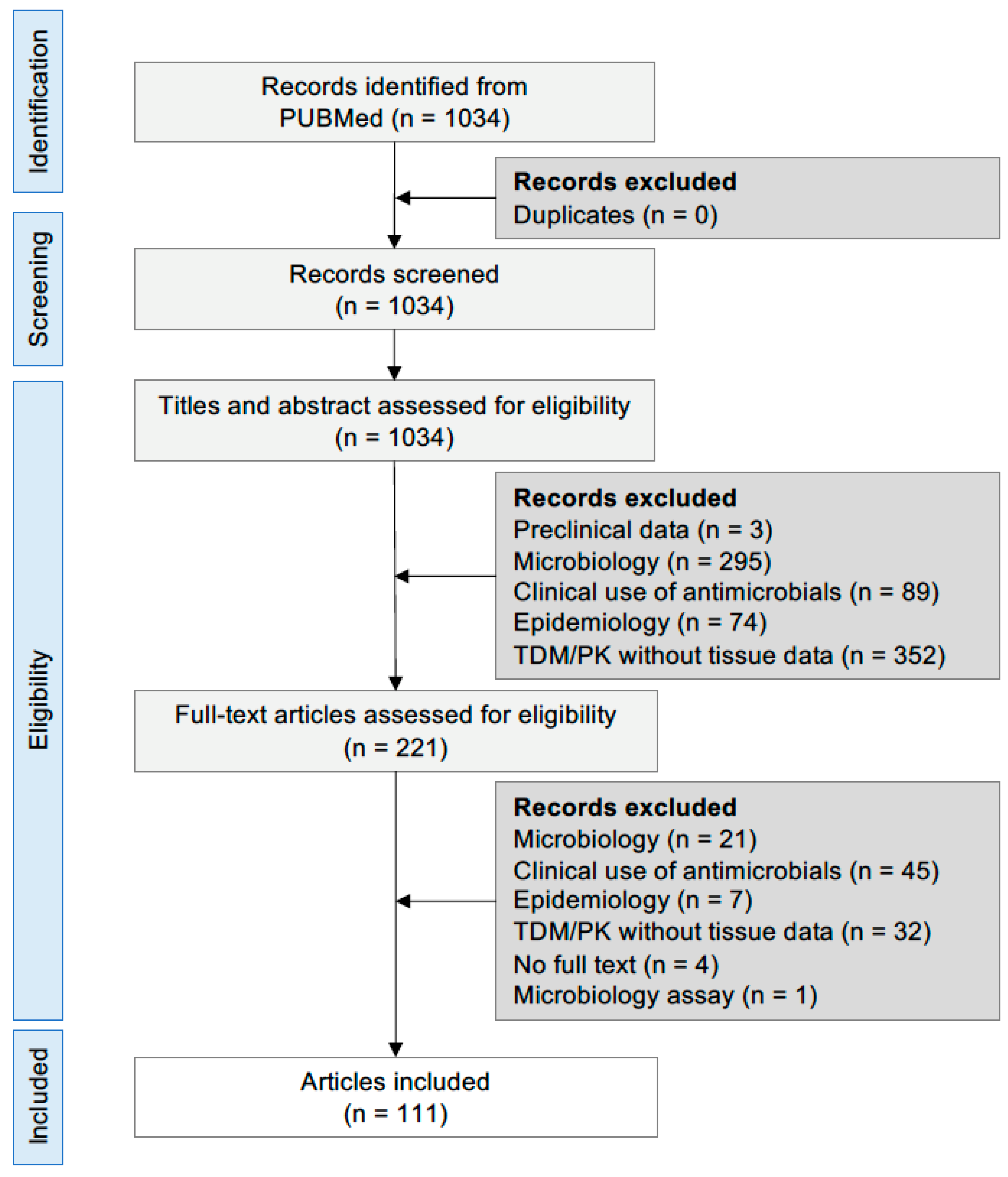
4. Materials and Methods
PRISMA Selection of Literature
- Domain 1: patients and ward: critically ill patient(s) OR intensive care unit OR ICU;
- Domain 2: study type: (study OR trial) AND (clinical OR human OR case series OR case report);
- Domain 3: drug list: antimicrobial(s) AND (amoxicillin OR ampicillin OR ampicillin/sulbactam OR aztreonam OR benzylpenicillin OR cefazolin OR cefepime OR cefixime OR cefotaxime OR ceftaroline fosamil OR ceftazidime/avibactam OR ceftazidime OR ceftobiprole OR ceftolozane/tazobactam OR ceftriaxone OR cefuroxime OR daptomycin OR ertapenem OR fosfomycin OR imipenem/cilastatin OR imipenem/cilastatin relebactam OR meropenem OR meropenem/vaborbactam OR oxacillin OR piperacillin OR piperacillin/tazobactam OR teicoplanin OR vancomycin);
- Domain 4: tissue distribution: tissue AND (distribution OR penetration OR diffusion OR pharmacokinetic(s)) AND (brain OR cerebrospinal fluid OR (epithelial lining fluid OR ELF) OR lung OR bronchial secretion OR skin OR interstitial fluid OR abdomen OR (peritoneal OR peritoneum) OR urine OR kidney OR liver OR bile OR bone OR synovial OR spleen OR muscle OR (subcutaneous OR subcutis) OR fat OR adipose).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Markwart, R.; Saito, H.; Harder, T.; Tomczyk, S.; Cassini, A.; Fleischmann-Struzek, C.; Reichert, F.; Eckmanns, T.; Allegranzi, B. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: A systematic review and meta-analysis. Intensive Care Med. 2020, 46, 1536–1551. [Google Scholar] [CrossRef] [PubMed]
- Bardi, T.; Pintado, V.; Gomez-Rojo, M.; Escudero-Sanchez, R.; Azzam Lopez, A.; Diez-Remesal, Y.; Martinez Castro, N.; Ruiz-Garbajosa, P.; Pestaña, D. Nosocomial infections associated to COVID-19 in the intensive care unit: Clinical characteristics and outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Mazzeffi, M.; Galvagno, S.; Rock, C. Prevention of healthcare-associated infections in intensive care unit patients. Anesthesiology 2021, 135, 1122–1131. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; Vena, A.; Graziano, E.; Russo, A.; Peghin, M. Risk stratification and treatment of ICU-acquired pneumonia caused by multidrug-resistant/extensively drug-resistant/pandrug-resistant bacteria. Curr. Opin. Crit. Care 2018, 24, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shorr, A.F.; Bassetti, M.; Timsit, J.-F.; Micek, S.T.; Michelson, A.P.; Garnacho-Montero, J. Timing of antibiotic therapy in the ICU. Crit. Care 2021, 25, 360. [Google Scholar] [CrossRef] [PubMed]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically Ill patients-guidelines from the french society of pharmacology and therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French society of anaesthesia and intensive care medicine (Société Française d’Anesthésie et Réanimation—SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef]
- Muller, A.E.; Huttner, B.; Huttner, A. Therapeutic drug monitoring of beta-lactams and other antibiotics in the intensive care unit: Which agents, which patients and which infections? Drugs 2018, 78, 439–451. [Google Scholar] [CrossRef]
- Cattaneo, D.; Corona, A.; De Rosa, F.G.; Gervasoni, C.; Kocic, D.; Marriott, D.J. The management of anti-infective agents in intensive care units: The potential role of a “fast” pharmacology. Expert Rev. Clin. Pharmacol. 2020, 13, 355–366. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically Ill adult patients: A position paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Pharmacokinetic issues for antibiotics in the critically Ill patient. Crit. Care Med. 2009, 37, 840–851. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically Ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef]
- Abdulla, A.; Dijkstra, A.; Hunfeld, N.G.M.; Endeman, H.; Bahmany, S.; Ewoldt, T.M.J.; Muller, A.E.; van Gelder, T.; Gommers, D.; Koch, B.C.P. Failure of target attainment of beta-lactam antibiotics in critically Ill patients and associated risk factors: A two-center prospective study (EXPAT). Crit. Care 2020, 24, 558. [Google Scholar] [CrossRef]
- Di Paolo, A.; Gori, G.; Tascini, C.; Danesi, R.; Del Tacca, M. Clinical pharmacokinetics of antibacterials in cerebrospinal fluid. Clin. Pharmacokinet. 2013, 52, 511–542. [Google Scholar] [CrossRef]
- Andes, D.; Craig, W.A. Animal model pharmacokinetics and pharmacodynamics: A critical review. Int. J. Antimicrob. Agents 2002, 19, 261–268. [Google Scholar] [CrossRef]
- Boselli, E.; Breilh, D.; Debon, R.; Duflo, F.; Bel, J.C.; Saux, M.C.; Chassard, D.; Allaouchiche, B. Penetration of Piperacillin/tazobactam (4 g/500 Mg) into synovial tissue. J. Chemother. 2002, 14, 54–58. [Google Scholar] [CrossRef]
- Boselli, E.; Breilh, D.; Rimmelé, T.; Guillaume, C.; Xuereb, F.; Saux, M.-C.; Bouvet, L.; Chassard, D.; Allaouchiche, B. Alveolar concentrations of piperacillin/tazobactam administered in continuous infusion to patients with ventilator-associated pneumonia. Crit. Care Med. 2008, 36, 1500–1506. [Google Scholar] [CrossRef]
- Roberts, J.A.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Piperacillin penetration into tissue of critically Ill patients with sepsis—Bolus versus continuous administration? Crit. Care Med. 2009, 37, 926–933. [Google Scholar] [CrossRef]
- Varghese, J.M.; Jarrett, P.; Boots, R.J.; Kirkpatrick, C.M.J.; Lipman, J.; Roberts, J.A. Pharmacokinetics of piperacillin and tazobactam in plasma and subcutaneous interstitial fluid in critically Ill patients receiving continuous venovenous haemodiafiltration. Int. J. Antimicrob. Agents 2014, 43, 343–348. [Google Scholar] [CrossRef]
- Heffernan, A.J.; Sime, F.B.; Lipman, J.; Dhanani, J.; Andrews, K.; Ellwood, D.; Grimwood, K.; Roberts, J.A. Intrapulmonary pharmacokinetics of antibiotics used to treat nosocomial pneumonia caused by gram-negative Bacilli: A systematic review. Int. J. Antimicrob. Agents 2019, 53, 234–245. [Google Scholar] [CrossRef] [Green Version]
- Felton, T.W.; Ogungbenro, K.; Boselli, E.; Hope, W.W.; Rodvold, K.A. Comparison of piperacillin exposure in the lungs of critically Ill patients and healthy volunteers. J. Antimicrob. Chemother. 2018, 73, 1340–1347. [Google Scholar] [CrossRef]
- Bergogne-Bérézin, E.; Berthelot, G.; Kafe, H. Diffusion of piperacillin into bronchial secretions. Pathol. Biol. 1986, 34, 653–656. [Google Scholar]
- Boselli, E.; Breilh, D.; Rimmelé, T.; Poupelin, J.-C.; Saux, M.-C.; Chassard, D.; Allaouchiche, B. Plasma and lung concentrations of ceftazidime administered in continuous infusion to critically Ill patients with severe nosocomial pneumonia. Intensive Care Med. 2004, 30, 989–991. [Google Scholar] [CrossRef]
- Lozano-Alonso, S.; Linares-Palomino, J.P.; Vera-Arroyo, B.; Bravo-Molina, A.; Hernández-Quero, J.; Ros-Díe, E. Evaluación de la capacidad de difusión tisular de antibióticos en isquemia de miembros inferiores. Enferm. Infecc. Microbiol. Clin. 2016, 34, 477–483. [Google Scholar] [CrossRef]
- Steib, A.; Jacoberger, B.; Von Bandel, M.; Beck, F.; Beller, J.P.; Boudjema, K.; Koffel, J.C.; Otteni, J.C. Concentrations in plasma and tissue penetration of ceftriaxone and ornidazole during liver transplantation. Antimicrob. Agents Chemother. 1993, 37, 1873–1876. [Google Scholar] [CrossRef]
- Klekner, A.; Bagyi, K.; Bognar, L.; Gaspar, A.; Andrasi, M.; Szabo, J. Effectiveness of cephalosporins in the sputum of patients with nosocomial bronchopneumonia. J. Clin. Microbiol. 2006, 44, 3418–3421. [Google Scholar] [CrossRef]
- Garazzino, S.; Aprato, A.; Baietto, L.; D’Avolio, A.; Maiello, A.; De Rosa, F.G.; Aloj, D.; Siccardi, M.; Biasibetti, A.; Massè, A.; et al. Ceftriaxone bone penetration in patients with septic non-union of the tibia. Int. J. Infect. Dis. 2011, 15, e415–e421. [Google Scholar] [CrossRef]
- Rybak, M. The pharmacokinetic profile of a new generation of parenteral cephalosporin. Am. J. Med. 1996, 100, 39S–44S. [Google Scholar] [CrossRef]
- Breilh, D.; Boselli, E.; Bel, J.C.; Chassard, D.; Saux, M.C.; Allaouchiche, B. Diffusion of cefepime into cancellous and cortical bone tissue. J. Chemother. 2003, 15, 134–138. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Q.; Zhao, L.; Shi, G.; Zhou, J. Blood-brain barrier penetration of cefepime after neurosurgery. Chin. Med. J. 2007, 120, 1176–1178. [Google Scholar] [CrossRef]
- Boselli, E.; Breilh, D.; Duflo, F.; Saux, M.-C.; Debon, R.; Chassard, D.; Allaouchiche, B. Steady-state plasma and intrapulmonary concentrations of cefepime administered in continuous infusion in critically Ill patients with severe nosocomial pneumonia. Crit. Care Med. 2003, 31, 2102–2106. [Google Scholar] [CrossRef]
- Craig, W.A. The pharmacology of meropenem, a new carbapenem antibiotic. Clin. Infect. Dis. 1997, 24 (Suppl. S2), S266–S275. [Google Scholar] [CrossRef]
- Varghese, J.M.; Jarrett, P.; Wallis, S.C.; Boots, R.J.; Kirkpatrick, C.M.J.; Lipman, J.; Roberts, J.A. Are Interstitial fluid concentrations of meropenem equivalent to plasma concentrations in critically Ill patients receiving continuous renal replacement therapy? J. Antimicrob. Chemother. 2015, 70, 528–533. [Google Scholar] [CrossRef]
- Hanberg, P.; Öbrink-Hansen, K.; Thorsted, A.; Bue, M.; Tøttrup, M.; Friberg, L.E.; Hardlei, T.F.; Søballe, K.; Gjedsted, J. Population pharmacokinetics of meropenem in plasma and subcutis from patients on extracorporeal membrane oxygenation treatment. Antimicrob. Agents Chemother. 2018, 62, e02390-17. [Google Scholar] [CrossRef]
- Germovsek, E.; Lutsar, I.; Kipper, K.; Karlsson, M.O.; Planche, T.; Chazallon, C.; Meyer, L.; Trafojer, U.M.T.; Metsvaht, T.; Fournier, I.; et al. Plasma and CSF pharmacokinetics of meropenem in neonates and young infants: Results from the NeoMero studies. J. Antimicrob. Chemother. 2018, 73, 1908–1916. [Google Scholar] [CrossRef]
- Benítez-Cano, A.; Luque, S.; Sorlí, L.; Carazo, J.; Ramos, I.; Campillo, N.; Curull, V.; Sánchez-Font, A.; Vilaplana, C.; Horcajada, J.P.; et al. Intrapulmonary concentrations of meropenem administered by continuous infusion in critically Ill patients with nosocomial pneumonia: A randomized pharmacokinetic trial. Crit. Care 2020, 24, 55. [Google Scholar] [CrossRef]
- Boselli, E.; Breilh, D.; Cannesson, M.; Xuereb, F.; Rimmelé, T.; Chassard, D.; Saux, M.-C.; Allaouchiche, B. Steady-state plasma and intrapulmonary concentrations of piperacillin/tazobactam 4 g/0.5 g administered to critically Ill patients with severe nosocomial pneumonia. Intensive Care Med. 2004, 30, 976–979. [Google Scholar] [CrossRef]
- Felton, T.W.; McCalman, K.; Malagon, I.; Isalska, B.; Whalley, S.; Goodwin, J.; Bentley, A.M.; Hope, W.W. Pulmonary penetration of piperacillin and tazobactam in critically Ill patients. Clin. Pharmacol. Ther. 2014, 96, 438–448. [Google Scholar] [CrossRef]
- Tomaselli, F.; Dittrich, P.; Maier, A.; Woltsche, M.; Matzi, V.; Pinter, J.; Nuhsbaumer, S.; Pinter, H.; Smolle, J.; Smolle-Jüttner, F.M. Penetration of piperacillin and tazobactam into pneumonic human lung tissue measured by in vivo microdialysis. Br. J. Clin. Pharmacol. 2003, 55, 620–624. [Google Scholar] [CrossRef]
- Jehl, F.; Muller-Serieys, C.; de Larminat, V.; Monteil, H.; Bergogne-Berezin, E. Penetration of piperacillin-tazobactam into bronchial secretions after multiple doses to intensive care patients. Antimicrob. Agents Chemother. 1994, 38, 2780–2784. [Google Scholar] [CrossRef]
- Cook, P.J.; Andrews, J.M.; Woodcock, J.; Wise, R.; Honeybourne, D. Concentration of amoxycillin and clavulanate in lung compartments in adults without pulmonary infection. Thorax 1994, 49, 1134–1138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joukhadar, C.; Frossard, M.; Mayer, B.X.; Brunner, M.; Klein, N.; Siostrzonek, P.; Eichler, H.G.; Müller, M. Impaired target site penetration of beta-lactams may account for therapeutic failure in patients with septic shock. Crit. Care Med. 2001, 29, 385–391. [Google Scholar] [CrossRef]
- Bue, M.; Sou, T.; Okkels, A.S.L.; Hanberg, P.; Thorsted, A.; Friberg, L.E.; Andersson, T.L.; Öbrink-Hansen, K.; Christensen, S. Population pharmacokinetics of piperacillin in plasma and subcutaneous tissue in patients on continuous renal replacement therapy. Int. J. Infect. Dis. 2020, 92, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Kinzig, M.; Sorgel, F.; Brismar, B.; Nord, C.E. Pharmacokinetics and tissue penetration of tazobactam and piperacillin in patients undergoing colorectal surgery. Antimicrob. Agents Chemother. 1992, 36, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Brunner, M.; Pernerstorfer, T.; Mayer, B.X.; Eichler, H.G.; Müller, M. Surgery and intensive care procedures affect the target site distribution of piperacillin. Crit. Care Med. 2000, 28, 1754–1759. [Google Scholar] [CrossRef]
- Wise, R.; O’Sullivan, N.; Johnson, J.; Andrews, J.M. Pharmacokinetics and tissue penetration of ampicillin and brobactam following oral administration of 2085P. Antimicrob. Agents Chemother. 1992, 36, 1002–1004. [Google Scholar] [CrossRef]
- Thabit, A.K.; Fatani, D.F.; Bamakhrama, M.S.; Barnawi, O.A.; Basudan, L.O.; Alhejaili, S.F. Antibiotic penetration into bone and joints: An updated review. Int. J. Infect. Dis. 2019, 81, 128–136. [Google Scholar] [CrossRef]
- Landersdorfer, C.B.; Kinzig, M.; Bulitta, J.B.; Hennig, F.F.; Holzgrabe, U.; Sörgel, F.; Gusinde, J. Bone penetration of amoxicillin and clavulanic acid evaluated by population pharmacokinetics and Monte Carlo simulation. Antimicrob. Agents Chemother. 2009, 53, 2569–2578. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Kinzig-Schippers, M.; Soergel, F.; Shah, P.M. Concentrations of piperacillin-tazobactam in human jaw and hip bone. J. Craniomaxillofac. Surg. 2008, 36, 468–472. [Google Scholar] [CrossRef]
- Falcone, M.; Menichetti, F.; Cattaneo, D.; Tiseo, G.; Baldelli, S.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Di Paolo, A.; Pai, M.P. Pragmatic options for dose optimization of ceftazidime/avibactam with aztreonam in complex patients. J. Antimicrob. Chemother. 2021, 76, 1025–1031. [Google Scholar] [CrossRef]
- Stein, G.E.; Yasin, F.; Smith, C.; Scharmen, A.; Havlichek, D.; Bill, C. A Pharmacokinetic/pharmacodynamic analysis of ceftaroline prophylaxis in patients with external ventricular drains. Surg. Infect. 2015, 16, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wu, Y.; Chen, B.; Zhou, J. Drug concentrations in the serum and cerebrospinal fluid of patients treated with cefoperazone/sulbactam after craniotomy. BMC Anesthesiol. 2015, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Le Turnier, P.; Grégoire, M.; Garot, D.; Guimard, T.; Duval, X.; Bernard, L.; Boutoille, D.; Dailly, É.; Navas, D.; Asseray, N. CSF Concentration of ceftriaxone following high-dose administration: Pharmacological data from two french cohorts. J. Antimicrob. Chemother. 2019, 74, 1753–1755. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Prange, H.W.; Kinzig, M.; Frank, A.; Dressel, A.; Scholz, P.; Kolenda, H.; Sörgel, F. Cerebrospinal fluid ceftazidime kinetics in patients with external ventriculostomies. Antimicrob. Agents Chemother. 1996, 40, 763–766. [Google Scholar] [CrossRef]
- Chen, X.-K.; Shi, H.-Y.; Leroux, S.; Xu, H.-Y.; Zhou, Y.; Zheng, Y.; Huang, X.; Li, Y.; Jacqz-Aigrain, E.; Zhao, W. Penetration of cefotaxime into cerebrospinal fluid in neonates and young infants. Antimicrob. Agents Chemother. 2018, 62, e02448-17. [Google Scholar] [CrossRef]
- Saunders, N.R.; Liddelow, S.A.; Dziegielewska, K.M. Barrier mechanisms in the developing brain. Front. Pharmacol. 2012, 3, 46. [Google Scholar] [CrossRef]
- Cousson, J.; Floch, T.; Guillard, T.; Vernet, V.; Raclot, P.; Wolak-Thierry, A.; Jolly, D. Lung Concentrations of ceftazidime administered by continuous versus intermittent infusion in patients with ventilator-associated pneumonia. Antimicrob. Agents Chemother. 2015, 59, 1905–1909. [Google Scholar] [CrossRef]
- EUCAST v_12.0_Breakpoint_Tables.pdf. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_12.0_Breakpoint_Tables.pdf (accessed on 7 April 2022).
- Nicolau, D.P.; Siew, L.; Armstrong, J.; Li, J.; Edeki, T.; Learoyd, M.; Das, S. Phase 1 study assessing the steady-state concentration of ceftazidime and avibactam in plasma and epithelial lining fluid following two dosing regimens. J. Antimicrob. Chemother. 2015, 70, 2862–2869. [Google Scholar] [CrossRef]
- Dimelow, R.; Wright, J.G.; MacPherson, M.; Newell, P.; Das, S. Population pharmacokinetic modelling of ceftazidime and avibactam in the plasma and epithelial lining fluid of healthy volunteers. Drugs R D 2018, 18, 221–230. [Google Scholar] [CrossRef]
- Caro, L.; Nicolau, D.P.; De Waele, J.J.; Kuti, J.L.; Larson, K.B.; Gadzicki, E.; Yu, B.; Zeng, Z.; Adedoyin, A.; Rhee, E.G. Lung penetration, bronchopulmonary pharmacokinetic/pharmacodynamic profile and safety of 3 g of ceftolozane/tazobactam administered to ventilated, critically Ill patients with pneumonia. J. Antimicrob. Chemother. 2020, 75, 1546–1553. [Google Scholar] [CrossRef]
- Chandorkar, G.; Huntington, J.A.; Gotfried, M.H.; Rodvold, K.A.; Umeh, O. Intrapulmonary penetration of ceftolozane/tazobactam and piperacillin/tazobactam in healthy adult subjects. J. Antimicrob. Chemother. 2012, 67, 2463–2469. [Google Scholar] [CrossRef]
- Langer, M.; Cantoni, P.; Bellosta, C.; Boccazzi, A. Penetration of ceftazidime into bronchial secretions in critically Ill patients. J. Antimicrob. Chemother. 1991, 28, 925–932. [Google Scholar] [CrossRef]
- Bressolle, F.; de la Coussaye, J.E.; Ayoub, R.; Fabre, D.; Gomeni, R.; Saissi, G.; Eledjam, J.J.; Galtier, M. Endotracheal and aerosol administrations of ceftazidime in patients with nosocomial pneumonia: Pharmacokinetics and absolute bioavailability. Antimicrob. Agents Chemother. 1992, 36, 1404–1411. [Google Scholar] [CrossRef]
- Roberts, J.A.; Udy, A.A.; Jarrett, P.; Wallis, S.C.; Hope, W.W.; Sharma, R.; Kirkpatrick, C.M.J.; Kruger, P.S.; Roberts, M.S.; Lipman, J. Plasma and target-site subcutaneous tissue population pharmacokinetics and dosing simulations of cefazolin in post-trauma critically Ill patients. J. Antimicrob. Chemother. 2015, 70, 1495–1502. [Google Scholar] [CrossRef]
- Skhirtladze-Dworschak, K.; Hutschala, D.; Reining, G.; Dittrich, P.; Bartunek, A.; Dworschak, M.; Tschernko, E.M. Cefuroxime plasma and tissue concentrations in patients undergoing elective cardiac surgery: Continuous vs. bolus application. A pilot study. Br. J. Clin. Pharmacol. 2019, 85, 818–826. [Google Scholar] [CrossRef]
- Hoffstedt, B.; Walder, M. Influence of serum protein binding and mode of administration on penetration of five cephalosporins into subcutaneous tissue fluid in humans. Antimicrob. Agents Chemother. 1981, 20, 783–786. [Google Scholar] [CrossRef]
- Bhalodi, A.A.; Housman, S.T.; Shepard, A.; Nugent, J.; Nicolau, D.P. Tissue pharmacokinetics of cefazolin in patients with lower limb infections. Antimicrob. Agents Chemother. 2013, 57, 5679–5683. [Google Scholar] [CrossRef]
- Douglas, A.; Udy, A.A.; Wallis, S.C.; Jarrett, P.; Stuart, J.; Lassig-Smith, M.; Deans, R.; Roberts, M.S.; Taraporewalla, K.; Jenkins, J.; et al. Plasma and tissue pharmacokinetics of cefazolin in patients undergoing elective and semielective abdominal aortic aneurysm open repair surgery. Antimicrob. Agents Chemother. 2011, 55, 5238–5242. [Google Scholar] [CrossRef]
- Sampol, E. Plasma, urine and skin pharmacokinetics of cefepime in burns patients. J. Antimicrob. Chemother. 2000, 46, 315–317. [Google Scholar] [CrossRef]
- Connors, J.E.; DiPiro, J.T.; Hayter, R.G.; Hooker, K.D.; Stanfield, J.A.; Young, T.R. Assessment of cefazolin and cefuroxime tissue penetration by using a continuous intravenous infusion. Antimicrob. Agents Chemother. 1990, 34, 1128–1131. [Google Scholar] [CrossRef]
- Matzneller, P.; Lackner, E.; Lagler, H.; Wulkersdorfer, B.; Österreicher, Z.; Zeitlinger, M. Single- and repeated-dose pharmacokinetics of ceftaroline in plasma and soft tissues of healthy volunteers for two different dosing regimens of ceftaroline fosamil. Antimicrob. Agents Chemother. 2016, 60, 3617–3625. [Google Scholar] [CrossRef] [Green Version]
- Barbour, A.; Schmidt, S.; Sabarinath, S.N.; Grant, M.; Seubert, C.; Skee, D.; Murthy, B.; Derendorf, H. Soft-tissue penetration of ceftobiprole in healthy volunteers determined by in vivo microdialysis. Antimicrob. Agents Chemother. 2009, 53, 2773–2776. [Google Scholar] [CrossRef]
- Stone, J.W.; Linong, G.; Andrews, J.M.; Wise, R. Cefixime, in-vitro activity, pharmacokinetics and tissue penetration. J. Antimicrob. Chemother. 1989, 23, 221–228. [Google Scholar] [CrossRef]
- Gergs, U.; Clauss, T.; Ihlefeld, D.; Weiss, M.; Pönicke, K.; Hofmann, G.O.; Neumann, J. Pharmacokinetics of ceftriaxone in plasma and bone of patients undergoing hip or knee surgery: Pharmacokinetics of ceftriaxone. J. Pharm. Pharmacol. 2014, 66, 1552–1558. [Google Scholar] [CrossRef]
- Raymakers, J.T.F.J.; Schaper, N.C.; Van Der Heyden, J.J.; Tordoir, J.H.M.; Kitslaar, P.J.E.H.M. Penetration of ceftazidime into bone from severely ischaemic limbs. J. Antimicrob. Chemother. 1998, 42, 543–545. [Google Scholar] [CrossRef]
- Yan, D.; Li, J.; Zhang, Z.; Zhu, H. Determination of cephazolin, ceftazidime, and ceftriaxone distribution in nucleus pulposus. Arch. Orthop. Trauma Surg. 2012, 132, 969–973. [Google Scholar] [CrossRef]
- Okamoto, M.P.; Chin, A.; Gill, M.A.; Yellin, A.E.; Berne, T.V.; Heseltine, P.N.; Appleman, M.D.; Knupp, C.A.; Sclar, D.A. Analysis of cefepime tissue penetration into human appendix. Pharmacotherapy 1991, 11, 353–358. [Google Scholar]
- Buijk, S.L.C.E. Pharmacokinetics of ceftazidime in serum and peritoneal exudate during continuous versus intermittent administration to patients with severe intra-abdominal infections. J. Antimicrob. Chemother. 2002, 49, 121–128. [Google Scholar] [CrossRef]
- Mattioli, F.; Fucile, C.; Del Bono, V.; Marini, V.; Parisini, A.; Molin, A.; Zuccoli, M.L.; Milano, G.; Danesi, R.; Marchese, A.; et al. Population pharmacokinetics and probability of target attainment of meropenem in critically Ill patients. Eur. J. Clin. Pharmacol. 2016, 72, 839–848. [Google Scholar] [CrossRef]
- Blassmann, U.; Roehr, A.C.; Frey, O.R.; Vetter-Kerkhoff, C.; Thon, N.; Hope, W.; Briegel, J.; Huge, V. Cerebrospinal fluid penetration of meropenem in neurocritical care patients with proven or suspected ventriculitis: A prospective observational study. Crit. Care 2016, 20, 343. [Google Scholar] [CrossRef]
- Lodise, T.P.; Nau, R.; Kinzig, M.; Drusano, G.L.; Jones, R.N.; Sörgel, F. Pharmacodynamics of ceftazidime and meropenem in cerebrospinal fluid: Results of population pharmacokinetic modelling and monte carlo simulation. J. Antimicrob. Chemother. 2007, 60, 1038–1044. [Google Scholar] [CrossRef]
- Nau, R.; Lassek, C.; Kinzig-Schippers, M.; Thiel, A.; Prange, H.W.; Sörgel, F. Disposition and elimination of meropenem in cerebrospinal fluid of hydrocephalic patients with external ventriculostomy. Antimicrob. Agents Chemother. 1998, 42, 2012–2016. [Google Scholar] [CrossRef] [Green Version]
- Mader, M.M.-D.; Czorlich, P.; König, C.; Fuhrmann, V.; Kluge, S.; Westphal, M.; Grensemann, J. Intrathecal penetration of meropenem and vancomycin administered by continuous infusion in patients suffering from ventriculitis—A retrospective analysis. Acta Neurochir. 2018, 160, 2099–2105. [Google Scholar] [CrossRef]
- Smith, P.B.; Cohen-Wolkowiez, M.; Castro, L.M.; Poindexter, B.; Bidegain, M.; Weitkamp, J.-H.; Schelonka, R.L.; Ward, R.M.; Wade, K.; Valencia, G.; et al. Population pharmacokinetics of meropenem in plasma and cerebrospinal fluid of infants with suspected or complicated intra-abdominal infections. Pediatr. Infect. Dis. J. 2011, 30, 844–849. [Google Scholar] [CrossRef]
- Boselli, E.; Breilh, D.; Saux, M.-C.; Gordien, J.-B.; Allaouchiche, B. Pharmacokinetics and lung concentrations of ertapenem in patients with ventilator-associated pneumonia. Intensive Care Med. 2006, 32, 2059–2062. [Google Scholar] [CrossRef]
- Lodise, T.P.; Sorgel, F.; Melnick, D.; Mason, B.; Kinzig, M.; Drusano, G.L. Penetration of meropenem into epithelial lining fluid of patients with ventilator-associated pneumonia. Antimicrob. Agents Chemother. 2011, 55, 1606–1610. [Google Scholar] [CrossRef]
- Frippiat, F.; Musuamba, F.T.; Seidel, L.; Albert, A.; Denooz, R.; Charlier, C.; Van Bambeke, F.; Wallemacq, P.; Descy, J.; Lambermont, B.; et al. Modelled target attainment after meropenem infusion in patients with severe nosocomial pneumonia: The PROMESSE study. J. Antimicrob. Chemother. 2015, 70, 207–216. [Google Scholar] [CrossRef]
- Roberts, J.A.; Kirkpatrick, C.M.J.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Meropenem dosing in critically Ill patients with sepsis and without renal dysfunction: Intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. J. Antimicrob. Chemother. 2009, 64, 142–150. [Google Scholar] [CrossRef]
- Conte, J.E.; Golden, J.A.; Kelley, M.G.; Zurlinden, E. Intrapulmonary pharmacokinetics and pharmacodynamics of meropenem. Int. J. Antimicrob. Agents 2005, 26, 449–456. [Google Scholar] [CrossRef]
- Wenzler, E.; Gotfried, M.H.; Loutit, J.S.; Durso, S.; Griffith, D.C.; Dudley, M.N.; Rodvold, K.A. Meropenem-RPX7009 concentrations in plasma, epithelial lining fluid, and alveolar macrophages of healthy adult subjects. Antimicrob. Agents Chemother. 2015, 59, 7232–7239. [Google Scholar] [CrossRef]
- van Hasselt, J.G.C.; Rizk, M.L.; Lala, M.; Chavez-Eng, C.; Visser, S.A.G.; Kerbusch, T.; Danhof, M.; Rao, G.; van der Graaf, P.H. Pooled population pharmacokinetic model of imipenem in plasma and the lung epithelial lining fluid. Br. J. Clin. Pharmacol. 2016, 81, 1113–1123. [Google Scholar] [CrossRef]
- Rizk, M.L.; Rhee, E.G.; Jumes, P.A.; Gotfried, M.H.; Zhao, T.; Mangin, E.; Bi, S.; Chavez-Eng, C.M.; Zhang, Z.; Butterton, J.R. Intrapulmonary pharmacokinetics of relebactam, a novel β-lactamase inhibitor, dosed in combination with imipenem-cilastatin in healthy subjects. Antimicrob. Agents Chemother. 2018, 62, e01411-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badia, J.R.; Soy, D.; Adrover, M.; Ferrer, M.; Sarasa, M.; Alarcón, A.; Codina, C.; Torres, A. Disposition of instilled versus nebulized tobramycin and imipenem in ventilated intensive care unit (ICU) patients. J. Antimicrob. Chemother. 2004, 54, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Verdier, M.C.; Seguin, P.; Le Touvet, B.; Cady, A.; Mallédant, Y.; Tribut, O. Ertapenem in plasma and peritoneal fluid from patients with severe intra-abdominal infections. J. Antimicrob. Chemother. 2011, 66, 1934–1936. [Google Scholar] [CrossRef] [PubMed]
- Karjagin, J.; Lefeuvre, S.; Oselin, K.; Kipper, K.; Marchand, S.; Tikkerberi, A.; Starkopf, J.; Couet, W.; Sawchuk, R.J. Pharmacokinetics of meropenem determined by microdialysis in the peritoneal fluid of patients with severe peritonitis associated with septic shock. Clin. Pharmacol. Ther. 2008, 83, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Boyadjiev, I.; Boulamery, A.; Simon, N.; Martin, C.; Bruguerolle, B.; Leone, M. Penetration of ertapenem into muscle measured by in vivo microdialysis in mechanically ventilated patients. Antimicrob. Agents Chemother. 2011, 55, 3573–3575. [Google Scholar] [CrossRef]
- Burkhardt, O. Penetration of ertapenem into skeletal muscle and subcutaneous adipose tissue in healthy volunteers measured by in vivo microdialysis. J. Antimicrob. Chemother. 2006, 58, 632–636. [Google Scholar] [CrossRef]
- Laethem, T.; De Lepeleire, I.; McCrea, J.; Zhang, J.; Majumdar, A.; Musson, D.; Rogers, D.; Li, S.; Guillaume, M.; Parneix-Spake, A.; et al. Tissue penetration by ertapenem, a parenteral carbapenem administered once daily, in suction-induced skin blister fluid in healthy young volunteers. Antimicrob. Agents Chemother. 2003, 47, 1439–1442. [Google Scholar] [CrossRef]
- Craig, W.A. Basic pharmacodynamics of antibacterials with clinical applications to the use of beta-lactams, glycopeptides, and linezolid. Infect. Dis. Clin. N. Am. 2003, 17, 479–501. [Google Scholar] [CrossRef]
- Álvarez, R.; López Cortés, L.E.; Molina, J.; Cisneros, J.M.; Pachón, J. Optimizing the clinical use of vancomycin. Antimicrob. Agents Chemother. 2016, 60, 2601–2609. [Google Scholar] [CrossRef]
- Pea, F. Teicoplanin and therapeutic drug monitoring: An update for optimal use in different patient populations. J. Infect. Chemother. 2020, 26, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Maserati, R.; Cruciani, M.; Azzini, M.; Carnevale, C.; Suter, F.; Concia, E. Teicoplanin in the therapy of staphylococcal neuroshunt infections. Int. J. Clin. Pharmacol. Res. 1987, 7, 207–213. [Google Scholar] [PubMed]
- Albanèse, J.; Léone, M.; Bruguerolle, B.; Ayem, M.L.; Lacarelle, B.; Martin, C. Cerebrospinal fluid penetration and pharmacokinetics of vancomycin administered by continuous infusion to mechanically ventilated patients in an intensive care unit. Antimicrob. Agents Chemother. 2000, 44, 1356–1358. [Google Scholar] [CrossRef]
- Li, X.; Wu, Y.; Sun, S.; Mei, S.; Wang, J.; Wang, Q.; Zhao, Z. Population pharmacokinetics of vancomycin in postoperative neurosurgical patients. J. Pharm. Sci. 2015, 104, 3960–3967. [Google Scholar] [CrossRef]
- Mounier, R.; Lobo, D.; Hulin, A.; Nebbad, B.; Cook, F.; Dhonneur, G. Is first-line vancomycin still the best option to treat Staphylococcus health care-associated meningitis? World Neurosurg. 2017, 99, 812.e1–812.e5. [Google Scholar] [CrossRef]
- Ricard, J.-D.; Wolff, M.; Lacherade, J.-C.; Mourvillier, B.; Hidri, N.; Barnaud, G.; Chevrel, G.; Bouadma, L.; Dreyfuss, D. Levels of vancomycin in cerebrospinal fluid of adult patients receiving adjunctive corticosteroids to treat pneumococcal meningitis: A Prospective multicenter observational study. Clin. Infect. Dis. 2007, 44, 250–255. [Google Scholar] [CrossRef]
- Jalusic, K.O.; Hempel, G.; Arnemann, P.-H.; Spiekermann, C.; Kampmeier, T.-G.; Ertmer, C.; Gastine, S.; Hessler, M. Population pharmacokinetics of vancomycin in patients with external ventricular drain-associated ventriculitis. Br. J. Clin. Pharmacol. 2021, 87, 2502–2510. [Google Scholar] [CrossRef]
- Tuon, F.F.; Yamada, C.H.; Cieslinski, J.; Dos Santos Oliveira, D.; Ribeiro, V.S.T.; Gasparetto, J.; Telles, J.P. Cerebrospinal fluid penetration of vancomycin during continuous infusion therapy in patients with nosocomial ventriculitis. Ther. Drug Monit. 2021, 43, 807–811. [Google Scholar] [CrossRef]
- Reiter, P.D.; Doron, M.W. Vancomycin Cerebrospinal fluid concentrations after intravenous administration in premature infants. J. Perinatol. Off. J. Calif. Perinat. Assoc. 1996, 16, 331–335. [Google Scholar]
- Mimoz, O.; Rolland, D.; Adoun, M.; Marchand, S.; Breilh, D.; Brumpt, I.; Debaene, B.; Couet, W. Steady-state trough serum and epithelial lining fluid concentrations of teicoplanin 12 Mg/Kg per day in patients with ventilator-associated pneumonia. Intensive Care Med. 2006, 32, 775–779. [Google Scholar] [CrossRef]
- Frank, U.K.; Schmidt-Eisenlohr, E.; Mlangeni, D.; Schindler, M.; Hoh, A.; Beyersdorf, F.; Daschner, F.D. Penetration of teicoplanin into heart valves and subcutaneous and muscle tissues of patients undergoing open-heart surgery. Antimicrob. Agents Chemother. 1997, 41, 2559–2561. [Google Scholar] [CrossRef]
- Stein, G.E.; Wells, E.M. The importance of tissue penetration in achieving successful antimicrobial treatment of nosocomial pneumonia and complicated skin and soft-tissue infections caused by methicillin-resistant Staphylococcus aureus: Vancomycin and linezolid. Curr. Med. Res. Opin. 2010, 26, 571–588. [Google Scholar] [CrossRef]
- Estes, K.S.; Derendorf, H. Comparison of the pharmacokinetic properties of vancomycin, linezolid, tigecyclin, and daptomycin. Eur. J. Med. Res. 2010, 15, 533–543. [Google Scholar] [CrossRef]
- Abraham, J.; Sinnollareddy, M.G.; Roberts, M.S.; Williams, P.; Peake, S.L.; Lipman, J.; Roberts, J.A. Plasma and interstitial fluid population pharmacokinetics of vancomycin in critically Ill patients with sepsis. Int. J. Antimicrob. Agents 2019, 53, 137–142. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Soy, D.; Llaurado-Serra, M.; Vaquer, S.; Castro, P.; Rodríguez, A.H.; Pontes, C.; Calvo, G.; Torres, A.; Martín-Loeches, I. Meropenem population pharmacokinetics in critically Ill patients with septic shock and continuous renal replacement therapy: Influence of residual diuresis on dose requirements. Antimicrob. Agents Chemother. 2015, 59, 5520–5528. [Google Scholar] [CrossRef]
- Lamer, C.; de Beco, V.; Soler, P.; Calvat, S.; Fagon, J.Y.; Dombret, M.C.; Farinotti, R.; Chastre, J.; Gibert, C. Analysis of vancomycin entry into pulmonary lining fluid by bronchoalveolar lavage in critically Ill patients. Antimicrob. Agents Chemother. 1993, 37, 281–286. [Google Scholar] [CrossRef]
- Harigaya, Y.; Bulitta, J.B.; Forrest, A.; Sakoulas, G.; Lesse, A.J.; Mylotte, J.M.; Tsuji, B.T. Pharmacodynamics of vancomycin at simulated epithelial lining fluid concentrations against methicillin-resistant Staphylococcus aureus (MRSA): Implications for dosing in MRSA pneumonia. Antimicrob. Agents Chemother. 2009, 53, 3894–3901. [Google Scholar] [CrossRef]
- Bue, M.; Tøttrup, M.; Hanberg, P.; Langhoff, O.; Birke-Sørensen, H.; Thillemann, T.M.; Andersson, T.L.; Søballe, K. Bone and subcutaneous adipose tissue pharmacokinetics of vancomycin in total knee replacement patients. Acta Orthop. 2018, 89, 95–100. [Google Scholar] [CrossRef]
- Safdar, N.; Andes, D.; Craig, W.A. In vivo pharmacodynamic activity of daptomycin. Antimicrob. Agents Chemother. 2004, 48, 63–68. [Google Scholar] [CrossRef]
- Vena, A.; Falcone, M.; Comandini, E.; Meledandri, M.; Novelli, A.; Campanile, F.; Stefani, S.; Venditti, M. Daptomycin plus trimethoprim/sulfamethoxazole combination therapy in post-neurosurgical meningitis caused by linezolid-resistant Staphylococcus epidermidis. Diagn. Microbiol. Infect. Dis. 2013, 76, 99–102. [Google Scholar] [CrossRef]
- Piva, S.; Di Paolo, A.; Galeotti, L.; Ceccherini, F.; Cordoni, F.; Signorini, L.; Togni, T.; De Nicolò, A.; Rasulo, F.A.; Fagoni, N.; et al. Daptomycin plasma and CSF levels in patients with healthcare-associated meningitis. Neurocrit. Care 2019, 31, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Suecof, L.A.; Sutherland, C.A.; Gao, L.; Kuti, J.L.; Nicolau, D.P. In vivo microdialysis study of the penetration of daptomycin into soft tissues in diabetic versus healthy volunteers. Antimicrob. Agents Chemother. 2008, 52, 3941–3946. [Google Scholar] [CrossRef] [PubMed]
- Traunmüller, F.; Schintler, M.V.; Metzler, J.; Spendel, S.; Mauric, O.; Popovic, M.; Konz, K.H.; Scharnagl, E.; Joukhadar, C. Soft Tissue and bone penetration abilities of daptomycin in diabetic patients with bacterial foot infections. J. Antimicrob. Chemother. 2010, 65, 1252–1257. [Google Scholar] [CrossRef] [Green Version]
- Montange, D.; Berthier, F.; Leclerc, G.; Serre, A.; Jeunet, L.; Berard, M.; Muret, P.; Vettoretti, L.; Leroy, J.; Hoen, B.; et al. Penetration of daptomycin into bone and synovial fluid in joint replacement. Antimicrob. Agents Chemother. 2014, 58, 3991–3996. [Google Scholar] [CrossRef]
- Miyadera, Y.; Naito, T.; Yamada, T.; Kawakami, J. Simple LC-MS/MS methods using core-shell octadecylsilyl microparticulate for the quantitation of total and free daptomycin in human plasma. Ther. Drug Monit. 2018, 40, 589–595. [Google Scholar] [CrossRef]
- Tascini, C.; Di Paolo, A.; Poletti, R.; Flammini, S.; Emdin, M.; Ciullo, I.; Tagliaferri, E.; Moter, A.; Menichetti, F. Daptomycin concentrations in valve tissue and vegetation in patients with bacterial endocarditis. Antimicrob. Agents Chemother. 2013, 57, 601–602. [Google Scholar] [CrossRef]
- Tascini, C.; Di Paolo, A.; Polillo, M.; Ferrari, M.; Lambelet, P.; Danesi, R.; Menichetti, F. Case report of a successful treatment of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and MRSA/vancomycin-resistant Enterococcus faecium Cholecystitis by Daptomycin. Antimicrob. Agents Chemother. 2011, 55, 2458–2459. [Google Scholar] [CrossRef]
- Putensen, C.; Ellger, B.; Sakka, S.G.; Weyland, A.; Schmidt, K.; Zoller, M.; Weiler, N.; Kindgen-Milles, D.; Jaschinski, U.; Weile, J.; et al. Current clinical use of intravenous fosfomycin in ICU patients in two european countries. Infection 2019, 47, 827–836. [Google Scholar] [CrossRef]
- Roussos, N.; Karageorgopoulos, D.E.; Samonis, G.; Falagas, M.E. Clinical Significance of the Pharmacokinetic and pharmacodynamic characteristics of fosfomycin for the treatment of patients with systemic infections. Int. J. Antimicrob. Agents 2009, 34, 506–515. [Google Scholar] [CrossRef]
- Pfausler, B.; Spiss, H.; Dittrich, P.; Zeitlinger, M.; Schmutzhard, E.; Joukhadar, C. Concentrations of fosfomycin in the cerebrospinal fluid of neurointensive care patients with ventriculostomy-associated ventriculitis. J. Antimicrob. Chemother. 2004, 53, 848–852. [Google Scholar] [CrossRef]
- Pfeifer, G.; Frenkel, C.; Entzian, W. Pharmacokinetic aspects of cerebrospinal fluid penetration of fosfomycin. Int. J. Clin. Pharmacol. Res. 1985, 5, 171–174. [Google Scholar] [PubMed]
- Kühnen, E.; Pfeifer, G.; Frenkel, C. Penetration of fosfomycin into cerebrospinal fluid across non-inflamed and inflamed meninges. Infection 1987, 15, 422–424. [Google Scholar] [CrossRef] [PubMed]
- Berthelot, G.; Bergogne-Berezin, E.; Kafe, H.; Daumal, M.; Gillon, J.C. Penetration of fosfomycin into bronchial secretions. Pathol. Biol. 1983, 31, 519–521. [Google Scholar]
- Matzi, V.; Lindenmann, J.; Porubsky, C.; Kugler, S.A.; Maier, A.; Dittrich, P.; Smolle-Jüttner, F.M.; Joukhadar, C. Extracellular concentrations of fosfomycin in lung tissue of septic patients. J. Antimicrob. Chemother. 2010, 65, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Joukhadar, C.; Klein, N.; Dittrich, P.; Zeitlinger, M.; Geppert, A.; Skhirtladze, K.; Frossard, M.; Heinz, G.; Müller, M. Target site penetration of fosfomycin in critically Ill patients. J. Antimicrob. Chemother. 2003, 51, 1247–1252. [Google Scholar] [CrossRef]
- Legat, F.J.; Maier, A.; Dittrich, P.; Zenahlik, P.; Kern, T.; Nuhsbaumer, S.; Frossard, M.; Salmhofer, W.; Kerl, H.; Müller, M. Penetration of fosfomycin into inflammatory lesions in patients with cellulitis or diabetic foot syndrome. Antimicrob. Agents Chemother. 2003, 47, 371–374. [Google Scholar] [CrossRef]
- Frossard, M.; Joukhadar, C.; Erovic, B.M.; Dittrich, P.; Mrass, P.E.; Van Houte, M.; Burgmann, H.; Georgopoulos, A.; Müller, M. Distribution and antimicrobial activity of fosfomycin in the interstitial fluid of human soft tissues. Antimicrob. Agents Chemother. 2000, 44, 2728–2732. [Google Scholar] [CrossRef]
- Sauermann, R.; Karch, R.; Langenberger, H.; Kettenbach, J.; Mayer-Helm, B.; Petsch, M.; Wagner, C.; Sautner, T.; Gattringer, R.; Karanikas, G.; et al. Antibiotic abscess penetration: Fosfomycin levels measured in pus and simulated concentration-time profiles. Antimicrob. Agents Chemother. 2005, 49, 4448–4454. [Google Scholar] [CrossRef]
- Falagas, M.E.; Kasiakou, S.K. Colistin: The revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin. Infect. Dis. 2005, 40, 1333–1341. [Google Scholar] [CrossRef]
- Zabidi, M.S.; Abu Bakar, R.; Musa, N.; Mustafa, S.; Wan Yusuf, W.N. Population pharmacokinetics of colistin methanesulfonate sodium and colistin in critically Ill patients: A systematic review. Pharmaceuticals 2021, 14, 903. [Google Scholar] [CrossRef]
- Bergen, P.J.; Li, J.; Nation, R.L. Dosing of colistin-back to basic PK/PD. Curr. Opin. Pharmacol. 2011, 11, 464–469. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, T.; Bustos, R.-H.; González, D.; Garzón, V.; García, J.-C.; Ramírez, D. An approach to measuring colistin plasma levels regarding the treatment of multidrug-resistant bacterial infection. Antibiotics 2019, 8, 100. [Google Scholar] [CrossRef]
- Imberti, R.; Cusato, M.; Villani, P.; Carnevale, L.; Iotti, G.A.; Langer, M.; Regazzi, M. Steady-state pharmacokinetics and BAL concentration of colistin in critically Ill patients after IV colistin methanesulfonate administration. Chest 2010, 138, 1333–1339. [Google Scholar] [CrossRef] [PubMed]
- Markou, N.; Fousteri, M.; Markantonis, S.L.; Boutzouka, E.; Tsigou, E.; Baltopoulo, G. Colistin penetration in the alveolar lining fluid of critically Ill patients treated with IV colistimethate sodium. Chest 2011, 139, 232–234. [Google Scholar] [CrossRef]
- Boisson, M.; Jacobs, M.; Grégoire, N.; Gobin, P.; Marchand, S.; Couet, W.; Mimoz, O. Comparison of intrapulmonary and systemic pharmacokinetics of colistin methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically Ill patients. Antimicrob. Agents Chemother. 2014, 58, 7331–7339. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Li Bassi, G.; Luna, C.M.; Martin-Loeches, I.; et al. Summary of the international clinical guidelines for the management of hospital-acquired and ventilator-acquired pneumonia. ERJ Open Res. 2018, 4, 00028-2018. [Google Scholar] [CrossRef]
- Luci, G.; Mattioli, F.; Falcone, M.; Di Paolo, A. Pharmacokinetics of non-β-lactam β-lactamase inhibitors. Antibiotics 2021, 10, 769. [Google Scholar] [CrossRef]
- Kanji, S.; Hayes, M.; Ling, A.; Shamseer, L.; Chant, C.; Edwards, D.J.; Edwards, S.; Ensom, M.H.H.; Foster, D.R.; Hardy, B.; et al. Reporting guidelines for clinical pharmacokinetic studies: The ClinPK statement. Clin. Pharmacokinet. 2015, 54, 783–795. [Google Scholar] [CrossRef]
- Mendeley Desktop, Version 1.19.8, © 2022 Mendeley Ltd. Available online: www.mendeley.com (accessed on 7 April 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]

| Drugs | Teicoplanin | Vancomycin |
|---|---|---|
| Daily dose | − LD 0.8 g q12h, MD 0.8 g A | − LD 1 g, MD 2 g CI − 1 g q12h − 10 mg/kg q8h |
| CSF | 0.1X (0.16–0.63X) B | |
| Lung tissue | 0.4X | |
| ELF | 1.46X | 0.2X |
| Bone | 0.23X (0.5 h) C | 0.13X (1 h), 0.4–0.57X(3 h) |
| Skin | 0.63X (2 h) | |
| ISF | 0.37X | |
| Myocardium | 0.25X (valves) | |
| Muscle | 0.25X | |
| References | [111,112] | [24,104,105,107,108,113,114,115] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finazzi, S.; Luci, G.; Olivieri, C.; Langer, M.; Mandelli, G.; Corona, A.; Viaggi, B.; Di Paolo, A. Tissue Penetration of Antimicrobials in Intensive Care Unit Patients: A Systematic Review—Part I. Antibiotics 2022, 11, 1164. https://doi.org/10.3390/antibiotics11091164
Finazzi S, Luci G, Olivieri C, Langer M, Mandelli G, Corona A, Viaggi B, Di Paolo A. Tissue Penetration of Antimicrobials in Intensive Care Unit Patients: A Systematic Review—Part I. Antibiotics. 2022; 11(9):1164. https://doi.org/10.3390/antibiotics11091164
Chicago/Turabian StyleFinazzi, Stefano, Giacomo Luci, Carlo Olivieri, Martin Langer, Giulia Mandelli, Alberto Corona, Bruno Viaggi, and Antonello Di Paolo. 2022. "Tissue Penetration of Antimicrobials in Intensive Care Unit Patients: A Systematic Review—Part I" Antibiotics 11, no. 9: 1164. https://doi.org/10.3390/antibiotics11091164