
A Retrospective Study of Risk Factors, Mortality, and Treatment Outcomes for Infections with Carbapenemase-Producing Enterobacterales in a Tertiary Hospital in Havana, Cuba

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Microbiological Study
2.2. Population Study
2.3. Risk Factors
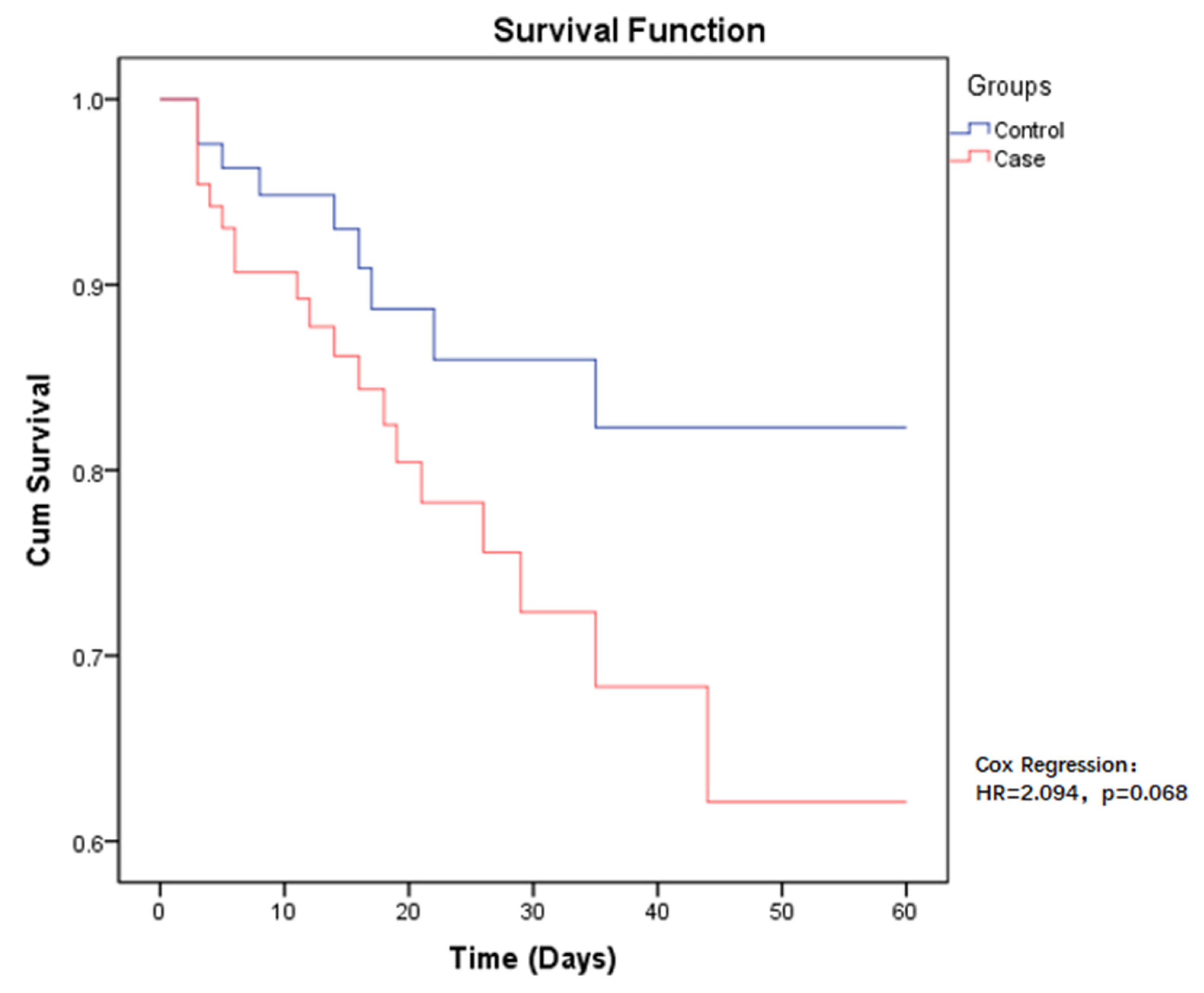
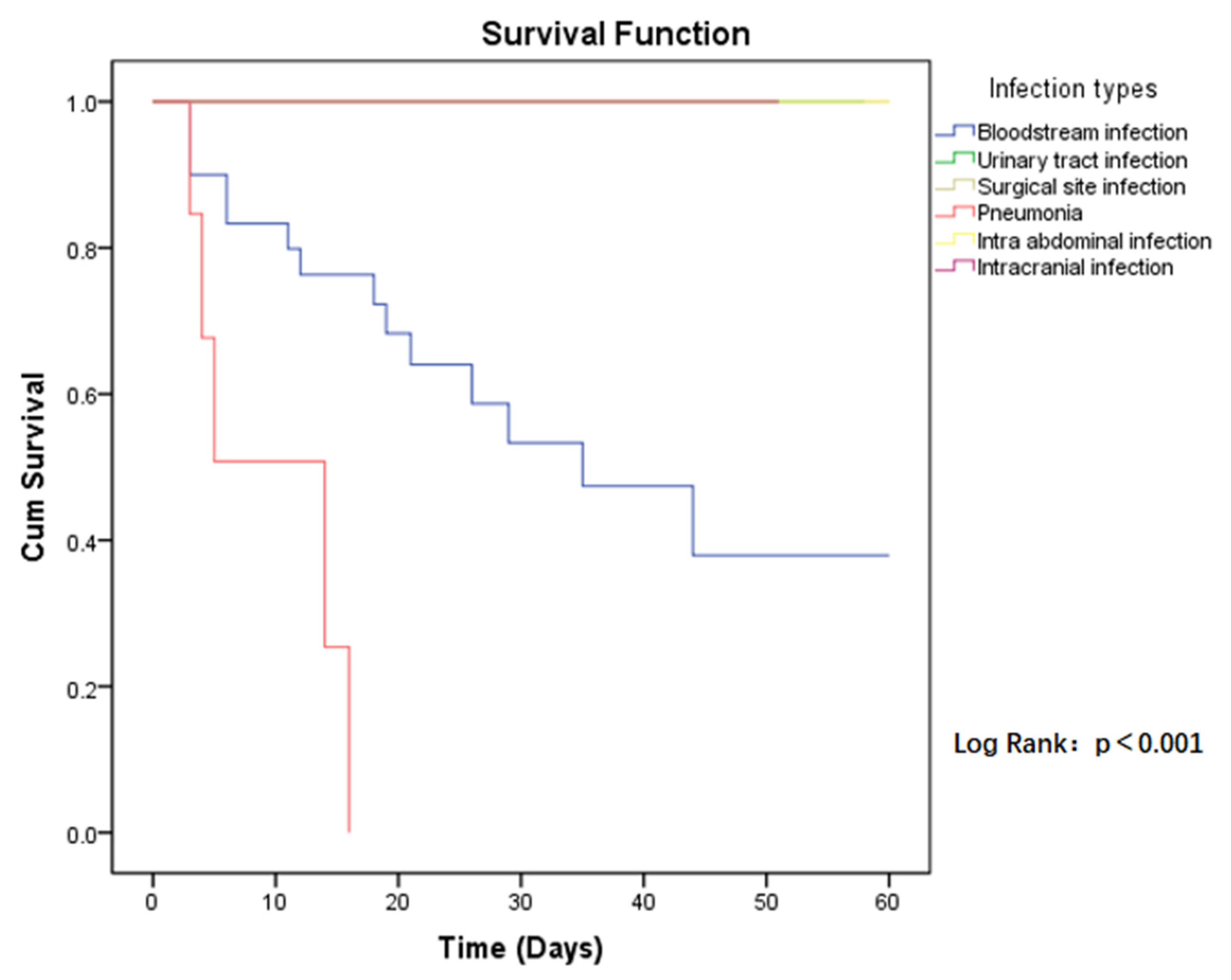
2.4. All-Cause 60-Day Mortality after CP-CRE Acquisition
2.5. Evaluation of Treatment Options for CP-CRE Infections
3. Discussion
4. Materials and Methods
4.1. Study Design and Description of the Institution
4.2. Microbiological Study
4.3. Description of Populations
- -
- Patients with community-acquired infections (infection diagnosis < 48 h).
- -
- Patients with positive culture by colonization or contaminated sample (asymptomatic and negatives in other additional testing).
- -
- Patients with hospital-acquired infections.
- -
- This study focused on the primary infection or first episode of CP-CRE-acquired infection during hospitalization if co-infections or recurrent infections occurred.
4.4. Data Collection
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yu, H.; Han, X.; Quiñones Pérez, D. La humanidad enfrenta un desastre: La resistencia antimicrobiana. Rev. Haban. Cienc. Méd. 2021, 20, e3850. [Google Scholar]
- Iredell, J.; Brown, J.; Tagg, K. Antibiotic resistance in Enterobacteriaceae: Mechanisms and clinical implications. BMJ 2016, 352, h6420. [Google Scholar] [CrossRef] [PubMed]
- Josa, D.F.; Bustos, G.; Torres, I.C.; Esparza, S.G. Evaluación de tres métodos de tamizaje para detección de Enterobacteriaceae productoras de carbapenemasas en hisopados rectales. Rev. Chil. Infectol. 2018, 35, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215 (Suppl. S1), S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Castanheira, M.; Deshpande, L.M.; Mendes, R.E.; Canton, R.; Sader, H.S.; Jones, R.N. Variations in the Occurrence of Resistance Phenotypes and Carbapenemase Genes Among Enterobacteriaceae Isolates in 20 Years of the SENTRY Antimicrobial Surveillance Program. Open Forum Infect. Dis. 2019, 6 (Suppl. S1), S23–S33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maseda, E.; Salgado, P.; Anillo, V.; Ruiz-Carrascoso, G.; Gómez-Gil, R.; Martín-Funke, C.; Jose Gimenez, M.; JoséGranizo, J.; Aguilar, L.; Gilsanz, F.; et al. Risk factors for colonization by carbapenemase-producing enterobacteria at admission to a Surgical ICU: A retrospective study. Enferm. Infecc. Microbiol. Clin. 2017, 35, 333–337. [Google Scholar] [CrossRef]
- Supliguicha Torres, M.; Supliguicha Torres, P.J.; Ortega, V.E.; Pacurucu, C.B.; Lema, J.P.; Santander, P.A. Factores de riesgo para la infección del tracto urinario por enterobacterias productoras de βlactamasas de espectro extendido. Arch. Venez. Farm. Ter. 2017, 36, 201–205. [Google Scholar]
- Alerta Epidemiológica: Emergencia e Incremento de Nuevas Combinaciones de Carbapenemasas en Enterobacterales en Latinoamérica y el Caribe; Organización Panamericana de la Salud/Organización Mundial de la Salud: Washington, DC, USA, 2021.
- Schwartz-Neiderman, A.; Braun, T.; Fallach, N.; Schwartz, D.; Carmeli, Y.; Schechner, V. Risk Factors for Carbapenemase-Producing Carbapenem-Resistant Enterobacteriaceae (CP-CRE) Acquisition Among Contacts of Newly Diagnosed CP-CRE Patients. Infect. Control Hosp. Epidemiol. 2016, 37, 1219–1225. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Zhang, Y.; Yao, X.; Xian, H.; Liu, Y.; Li, H.; Chen, H.; Wang, X.; Wang, R.; Zhao, C.; et al. Risk factors and clinical outcomes for carbapenem-resistant Enterobacteriaceae nosocomial infections. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1679–1689. [Google Scholar] [CrossRef]
- Satlin, M.J.; Jenkins, S.G.; Walsh, T.J. The Global Challenge of Carbapenem-Resistant Enterobacteriaceae in Transplant Recipients and Patients With Hematologic Malignancies. Clin. Infect. Dis. 2014, 58, 1274–1283. [Google Scholar] [CrossRef]
- Garbati, M.A.; Sakkijha, H.; Abushaheen, A. Infections due to Carbapenem Resistant Enterobacteriaceae among Saudi Arabian Hospitalized Patients: A Matched Case-Control Study. BioMed Res. Int. 2016, 2016, 3961684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suárez, T.B.; Bustamante, P.Y.; Hart, C.M.; Romero, G.M.M.; González, M.A.; Martínez, B.M.L. Caracterización de aislamientos intrahospitalarios de Klebsiella pneumoniae en un hospital terciario. Rev. Cuba. Med. 2015, 54, 323–336. [Google Scholar]
- García-Βncur, J.C.; Appel, T.M.; Esparza, G.; Gales, A.C.; Levy-Hara, G.; Cornistein, W.; Vegaf, S.; Nuñez, D.; Cuellar, L.; Bavestrello, L.; et al. Update on the epidemiology of carbapenemases in Latin America and the Caribbean. Expert Rev. Anti-Infect. Ther. 2021, 19, 197–213. [Google Scholar] [CrossRef] [PubMed]
- Van-Duin, D.; Doi, Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 2017, 8, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Quiñones, P.D.; Βncourt, G.Y.; Carmona, C.Y.; Pereda, N.N.; Álvarez, V.S.; Soeaung, M.; Kobayashi, N. Escherichia coli extraintestinal, resistencia antimicrobiana y producción de βlactamasas en aislados cubanos. Rev. Cuba. Med. Trop. 2020, 72, 1–18. [Google Scholar]
- Quiñones, D.; Aung, M.S.; Carmona, Y.; González, M.K.; Pereda, N.; Hidalgo, M.; Rivero, M.; Zayas, A.; Del Campo, R.; Urushibara, N.; et al. High Prevalence of CTX-M Type Extended-Spectrum Β-Lactamase Genes and Detection of NDM-1 Carbapenemase Gene in Extraintestinal Pathogenic Escherichia coli in Cuba. Pathogens 2020, 9, 65. [Google Scholar] [CrossRef] [Green Version]
- Malbrán, C.G. (Ed.) Alerta Epidemiológica: Emergencia de Enterobacterales Doble Productores de Carbapenemasas; Instituto Nacional de Enfermedades Infecciosas: Buenos Aires, Argentina, 2021. [Google Scholar]
- Actualización de Alerta por Aparecimiento de Aislamientos Productores de Carbapenemasas OXA-48-Like; Report No: TLGG-27-2021; Ministerio de Salud Pública y Asistencia Social de Guatemala: Ciudad de Guatemala, Guatemala, 2021.
- Nancy, M.T.; Miryan, F.; Sofía, B.; Mariel, B. Incremento en el Aislamiento de Bacilos Gramnegativos Resistentes a Antimicrobianos de Amplio Espectro en Hospitales de Paraguay; Ministerio de Salud Pública y Bienestar Social de Paraguay: Asunción, Paraguay, 2021. [Google Scholar]
- Findlay, J.; Poirel, L.; Kessler, J.; Kronenberg, A.; Nordmann, P. New Delhi Metallo-β-Lactamase–Producing Enterobacterales Bacteria, Switzerland, 2019–2020. Emerg. Infect. Dis. 2021, 27, 2628–2637. [Google Scholar] [CrossRef]
- Doi, Y.; Wachino, J.; Arakawa, Y. Aminoglycoside resistance: The emergence of acquired 16S ribosomal RNA methyltransferases. Infect. Dis. Clin. 2016, 30, 523–537. [Google Scholar] [CrossRef] [Green Version]
- Nordmann, P.; Poirel, L.; Walsh, T.R.; Livermore, D.M. The emerging NDM carbapenemases. Trends Microbiol. 2011, 19, 588–595. [Google Scholar] [CrossRef]
- Binsker, U.; Käsbohrer, A.; Hammerl, J.A. Global colistin use: A review of the emergence of resistant Enterobacterales and the impact on their genetic basis. FEMS Microbiol. Rev. 2021, 46, fuab049. [Google Scholar] [CrossRef]
- Tischendorf, J.; de Avila, R.A.; Safdar, N. Risk of infection following colonization with carbapenem-resistant Enterobactericeae: A systematic review. Am. J. Infect. Control 2016, 44, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrill, H.J.; Pogue, J.M.; Kaye, K.S.; LaPlante, K.L. Treatment Options for Carbapenem-Resistant Enterobacteriaceae Infections. Open Forum Infect. Dis. 2015, 2, ofv050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacheco, T.; Bustos, R.H.; González, D.; Garzón, V.; García, J.C.; Ramírez, D. An Approach to Measuring Colistin Plasma Levels Regarding the Treatment of Multidrug-Resistant Bacterial Infection. Antibiotics 2019, 8, 100. [Google Scholar] [CrossRef] [Green Version]
- Leng, B.; Yan, G.; Wang, C.; Shen, C.; Zhang, W.; Wang, W. Dose optimisation based on pharmacokinetic/pharmacodynamic target of tigecycline. J. Glob. Antimicrob. Resist. 2021, 25, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; He, L.; Hu, B.; Hu, J.; Huang, X.; Lai, G.; Li, Y.; Liu, Y.; Ni, Y.; Qiu, H.; et al. Laboratory diagnosis, clinical management and infection control of the infections caused by extensively drug-resistant Gram-negative bacilli: A Chinese consensus statement. Clin. Microbiol. Infect. 2016, 22, S15–S25. [Google Scholar] [CrossRef] [Green Version]
- Perez, F.; El Chakhtoura, N.G.; Papp-Wallace, K.M.; Wilson, B.M.; Bonomo, R.A. Treatment options for infections caused by carbapenem-resistant Enterobacteriaceae: Can we apply “precision medicine” to antimicrobial chemotherapy? Expert Opin. Pharm. 2016, 17, 761–781. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.; Fahrbach, K.; Zhao, Q.; Lodise, T. Association Between Carbapenem Resistance and Mortality Among Adult, Hospitalized Patients With Serious Infections Due to Enterobacteriaceae: Results of a Systematic Literature Review and Meta-analysis. Open Forum Infect. Dis. 2018, 5, ofy150. [Google Scholar] [CrossRef]
- Singh, N.; Yeh, P.J. Suppressive drug combinations and their potential to combat antibiotic resistance. J. Antibiot. 2017, 70, 1033–1042. [Google Scholar] [CrossRef]
- Biagi, M.; Wu, T.; Lee, M.; Patel, S.; Butler, D.; Wenzler, E. Searching for the Optimal Treatment for Metallo- and Serine-β-Lactamase Producing Enterobacteriaceae: Aztreonam in Combination with Ceftazidime-avibactam or Meropenem-vaborbactam. Antimicrob. Agents Chemother. 2019, 63, e01426-19. [Google Scholar] [CrossRef]
- Sader, H.S.; Carvalhaes, C.G.; Arends, S.J.R.; Castanheira, M.; Mendes, R.E. Aztreonam/avibactam activity against clinical isolates of Enterobacterales collected in Europe, Asia and Latin America in 2019. J. Antimicrob. Chemother. 2021, 76, 566–659. [Google Scholar] [CrossRef]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Methods | Carbapenemase Types | Species | |||||
|---|---|---|---|---|---|---|---|
| K. pneumoniae (Strains = 88) | E. cloacae (Strains = 16) | E. coli (Strains = 7) | K. aerogenes (Strains = 4) | S. marcescens (Strains = 4) | Others 1 (Strains = 5) | ||
| PCR (55 strains) | NDM | 38 | 5 | 4 | 1 | 1 | 3 |
| NDM + KPC | 2 | 0 | 0 | 1 | 0 | 0 | |
| Inmunocromatográfico CORIS (69 strains) | KPC | 0 | 0 | 0 | 0 | 0 | 0 |
| NDM | 48 | 11 | 3 | 2 | 3 | 2 | |
| VIM | 0 | 0 | 0 | 0 | 0 | 0 | |
| OXA-48 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Antibiotics 1 | % Resistance | ||||||
|---|---|---|---|---|---|---|---|
| K. pneumoniae (Strains = 88) | E. cloacae (Strains = 16) | E. coli (Strains = 7) | K. aerogenes (Strains = 4) | S. marcescens (Strains = 4) | Others 2 (Strains = 5) | Total (Strains = 124) | |
| SAM | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| TZP | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| CAZ | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| CTX | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| FEP | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| ATM | 97.7 | 93.8 | 57.1 | 75.0 | 100.0 | 80.0 | 93.5 |
| FOS | 73.9 | 75.0 | 14.3 | 100.0 | 75.0 | 80.0 | 71.8 |
| CIP | 88.6 | 87.5 | 57.1 | 100.0 | 75.0 | 100.0 | 87.1 |
| GEN | 92.0 | 100.0 | 71.4 | 100.0 | 100.0 | 100.0 | 92.8 |
| AMK | 93.2 | 93.8 | 57.1 | 100.0 | 100.0 | 100.0 | 91.9 |
| SXT | 95.5 | 100.0 | 57.1 | 100.0 | 75.0 | 100.0 | 93.5 |
| MRP | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| IMI | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 |
| CST 3 | 26.1 | 31.3 | 0.0 | 25.0 | - | 25.0 | 25.2 |
| TGC | 83.0 | 81.3 | 42.9 | 100.0 | 100.0 | 60.0 | 80.6 |
| Variables | Cases (n = 88) | Controls (n = 88) | p-Value |
|---|---|---|---|
| Mean Age ± SD (Range) | 55.5 ± 14.8 (20–87) | 53.2 ± 15.5 (22–86) | 0.31 |
| Services | |||
| Critical Care Unit (ICU y CCU) | 25 (28.4%) | 23 (26.1%) | 0.74 |
| Urology/Lithotripsy | 22 (25.0%) | 22 (25.0%) | 1 |
| General Surgery | 7 (8.0%) | 6 (6.8%) | 0.77 |
| Hematology | 4 (4.5%) | 4 (4.5%) | 1 |
| Nephrology | 4 (4.5%) | 4 (4.5%) | 1 |
| Internal medicine | 6 (6.8%) | 5 (5.7%) | 0.76 |
| Transplantation | 4 (4.5%) | 6 (6.8%) | 0.51 |
| Neurology/neurosurgery | 4 (4.5%) | 4 (4.5%) | 1 |
| Miscellaneous | 12 (13.6%) | 14 (15.9%) | 0.67 |
| Infection Sites | |||
| Bloodstream infection | 30 (34.1%) | 30 (34.1%) | 1 |
| Urinary tract infection | 30 (34.1%) | 31 (35.2%) | 0.87 |
| Surgical site infection | 18 (20.5%) | 18 (20.5%) | 1 |
| Pneumonia | 7 (8.0%) | 6 (6.8%) | 0.77 |
| Intra-abdominal infection | 2 (2.3%) | 2 (2.3%) | 1 |
| Intracranial infection | 1 (1.1%) | 1 (1.1%) | 1 |
| Factors | Cases (n = 88) | Controls (n = 88) | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|---|
| OR (IC 95%) | p-Valor | OR (IC 95%) | p-Valor | |||
| Clinical Characteristics | ||||||
| Mean Charlson Index score ± SD | 3.1 ± 1.9 | 3.1 ± 2.2 | 1.01 (0.88–1.17) | 0.86 | - | - |
| Average length of hospitalization before infection | 27.1 ± 20.0 | 18.1 ± 14.5 | 1.03 (1.01–1.05) | <0.01 | 1.00 (0.97–1.03) | 0.95 |
| Previously admitted within the last 6 months | 36 (40.9%) | 28(31.8%) | 1.48 (0.80–2.75) | 0.21 | - | - |
| Prolonged derivation (brain, thoracic, abdominal) 1 | 20 (22.7%) | 9 (10.2%) | 2.58 (1.10–6.05) | 0.03 | 0.93 (0.30–2.95) | 0.91 |
| Deep venous catheterization | 43 (48.9%) | 31 (35.2%) | 1.76 (0.96–3.22) | 0.07 | 0.52 (0.19–1.43) | 0.21 |
| Urinary catheters (>48 h) | 66 (75.0%) | 57 (64.8%) | 1.63 (0.85–3.13) | 0.14 | 1.52 (0.63–3.68) | 0.36 |
| Nasogastric tube | 36 (40.9%) | 20 (22.7%) | 2.35 (1.22–4.53) | 0.01 | 1.45 (0.37–5.76) | 0.60 |
| Mechanical ventilation | 26 (29.5%) | 14 (15.9%) | 2.22 (1.07–4.61) | 0.03 | 0.52 (0.12–2.23) | 0.34 |
| Surgery | 71 (80.7%) | 74 (84.1%) | 0.79 (0.36–1.72) | 0.55 | - | - |
| Dialysis | 9 (10.2%) | 10 (11.4%) | 0.89 (0.34–2.31) | 0.81 | - | - |
| Transfer from other health centers | 15 (17.0%) | 5 (5.7%) | 3.41 (1.18–9.84) | 0.02 | 2.98 (0.91–9.69) | 0.07 |
| Steroid use | 39 (44.3%) | 16 (18.2%) | 3.58 (1.80–7.11) | <0.01 | 3.22 (1.36–7.66) | <0.01 |
| Prior use of two or more antibiotics | 63 (71.6%) | 23 (26.1%) | 7.12 (3.67–13.83) | <0.01 | 4.04 (1.40–11.71) | 0.01 |
| Previous Antibiotic Use (with Course ≥ 7 days) | ||||||
| β-lactamase inhibitors | 20 (22.7%) | 14 (15.9%) | 1.56 (0.73–3.32) | 0.25 | - | - |
| Cephalosporin first or second generation | 8 (9.1%) | 4 (4.5%) | 2.10 (0.61–7.25) | 0.24 | - | - |
| Cephalosporin third or fourth generation | 53 (60.2%) | 26 (29.5%) | 3.61 (1.93–6.75) | <0.01 | 2.40 (1.06–5.44) | 0.04 |
| Aminoglycoside | 38 (43.2%) | 13 (14.8%) | 4.39 (2.13–9.05) | <0.01 | 2.06 (0.74–5.72) | 0.16 |
| Quinolone | 31 (35.2%) | 21 (23.9%) | 1.74 (0.90–3.35) | 0.1 | 0.78 (0.28–2.17) | 0.63 |
| Carbapenem | 27 (30.7%) | 4 (4.5%) | 9.30 (3.09–27.94) | <0.01 | 4.77 (1.17–19.35) | 0.03 |
| Sulfonamide | 11 (12.5%) | 6 (6.8%) | 1.95 (0.69–5.54) | 0.21 | - | - |
| Treatment Options 1 | Bloodstream Infection | Pneumonia | ||||||
|---|---|---|---|---|---|---|---|---|
| Survival (Case = 16) | Non-Survival (Case = 14) | PR | p-Value | Survival (Case = 2) | Non-Survival (Case = 5) | PR | p-Value | |
| Monotherapy | 3 (18.6%) | 5 (35.7%) | 1.53 (0.73–3.19) | 0.26 | 0 | 2 (40.0%) | 1.43 (0.61–3.32) | 0.48 |
| Colistin-based | 11 (68.8%) | 4 (28.6%) | 0.40 (0.16–0.99) | 0.03 | 0 | 3 (60.0%) | 1.75 (0.68–4.53) | 0.29 |
| Tigecycline-based | 0 | 2 (14.3%) | 1.93 (1.00–3.72) | 0.21 | 1 (50.0%) | 0 | 0.52 (0.13–1.96) | 0.28 |
| Colistin-tigecycline-based | 1 (6.25%) | 2 (14.3%) | 1.50 (0.61–3.71) | 0.45 | 1 (50.0%) | 0 | 0.52 (0.13–1.97) | 0.28 |
| Primer | Sequence (5′–3′) | Gene | Product Size (bp) |
|---|---|---|---|
| KPC-Fm | CGTCTAGTTCTGCTGTCTTG | blaKPC | 798 |
| KPC-Rm | CTTGTCATCCTTGTTAGGCG | ||
| NDM-F | GGTTTGGCGATCTGGTTTTC | blaNDM | 621 |
| NDM-R | CGGAATGGCTCATCACGATC | ||
| IMP-F | GGAATAGAGTGGCTTAAYTCTC | blaIMP | 232 |
| IMP-R | GGTTTAAYAAAACAACCACC | ||
| VIM-F | GATGGTGTTTGGTCGCATA | blaVIM | 390 |
| VIM-R | CGAATGCGCAGCACCAG | ||
| SPM-F | AAAATCTGGGTACGCAAACG | blaSPM | 271 |
| SPM-R | ACATTATCCGCTGGAACAGG | ||
| GIM-F | TCGACACACCTTGGTCTGAA | blaGIM | 477 |
| GIM-R | AACTTCCAACTTTGCCATGC | ||
| SIM-F | TACAAGGGATTCGGCATCG | blaSIM | 570 |
| SIM-R | TAATGGCCTGTTCCCATGTG | ||
| OXA-F | GCGTGGTTAAGGATGAACAC | blaOXA-48 | 438 |
| OXA-R | CATCAAGTTCAACCCAACCG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Hernández González, A.; Estévez Torres, G.; González Molina, M.K.; Hart Casares, M.; Han, X.; Baldoquín Rodríguez, W.; Quiñones Pérez, D. A Retrospective Study of Risk Factors, Mortality, and Treatment Outcomes for Infections with Carbapenemase-Producing Enterobacterales in a Tertiary Hospital in Havana, Cuba. Antibiotics 2022, 11, 942. https://doi.org/10.3390/antibiotics11070942
Yu H, Hernández González A, Estévez Torres G, González Molina MK, Hart Casares M, Han X, Baldoquín Rodríguez W, Quiñones Pérez D. A Retrospective Study of Risk Factors, Mortality, and Treatment Outcomes for Infections with Carbapenemase-Producing Enterobacterales in a Tertiary Hospital in Havana, Cuba. Antibiotics. 2022; 11(7):942. https://doi.org/10.3390/antibiotics11070942
Chicago/Turabian StyleYu, Haiyang, Alberto Hernández González, Gonzalo Estévez Torres, María Karla González Molina, Marcia Hart Casares, Xu Han, Waldemar Baldoquín Rodríguez, and Dianelys Quiñones Pérez. 2022. "A Retrospective Study of Risk Factors, Mortality, and Treatment Outcomes for Infections with Carbapenemase-Producing Enterobacterales in a Tertiary Hospital in Havana, Cuba" Antibiotics 11, no. 7: 942. https://doi.org/10.3390/antibiotics11070942