
Healthcare Professionals’ Knowledge and Beliefs on Antibiotic Prophylaxis in Cesarean Section: A Mixed-Methods Study in Benin

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Results
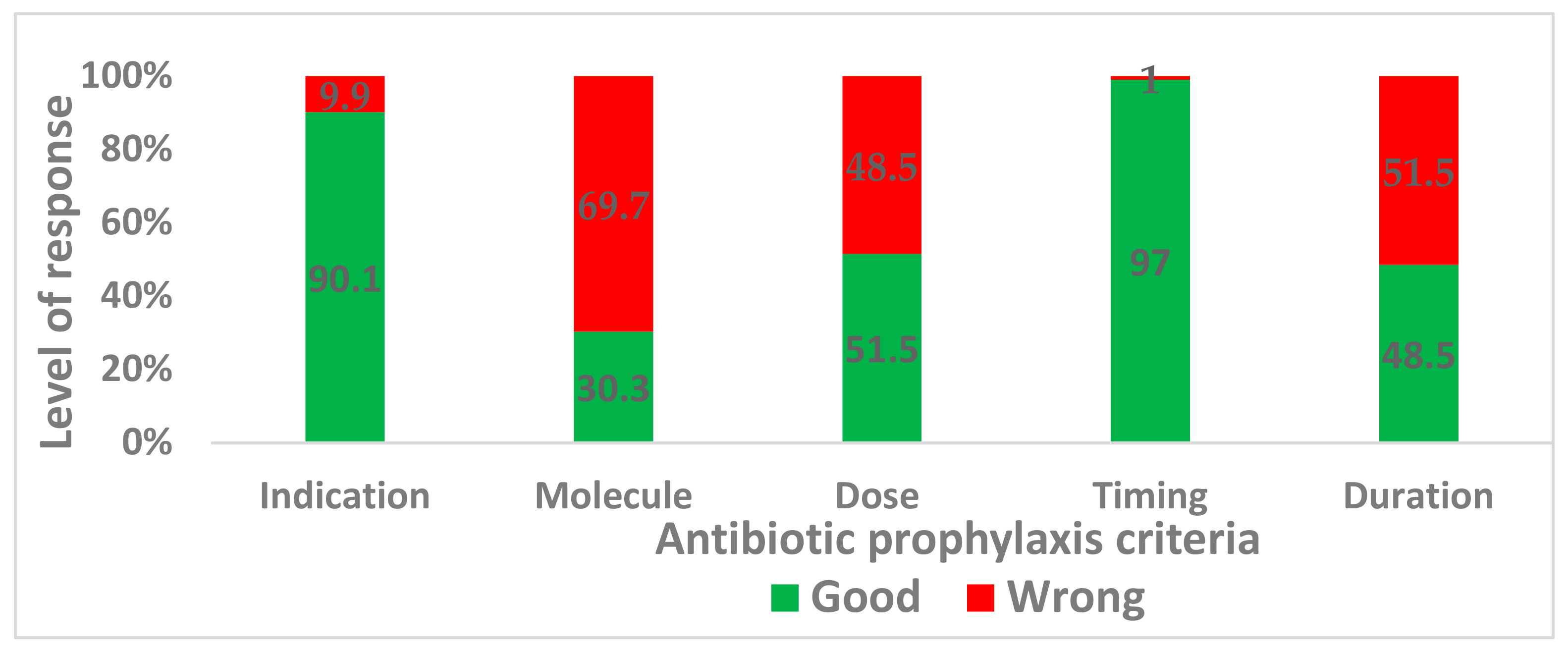
2.1. Assessment of the Level of Knowledge of Antibiotic Prophylaxis
2.2. Interviews
2.2.1. Patient Health Determinants
“But for me, it is above all the patients who do not wash themselves properly- the hygiene of the skin on which we are going to work on. The absence of shower before patients enter in the operating room. The conditions that must be met before the patients enters the operating room are not met.”(Gynecologist Medical Doctor 3, Hospital 2)
“Now, there are some women for whom we do not use gentamicin. But if the woman is not allergic to ampicillin, we will use both.”(Nurse Anesthetist 4, Hospital 1)
“We systematically administer 2 g of ampicillin and 160 mg of gentamicin if the woman has no history of hypertension.”(Nurse Anesthetist 2, Hospital 3)
2.2.2. Hospital-Related Determinants
“Yes, the working conditions. To start, the climatic conditions make it impossible to do things differently. And then the surgical units are also substandard—you couldn’t say that the unit is systematically sterile.”(Operating Room Nurse, Hospital 2)
“But that’s what’s cheaper, that’s why they put that in the kit to free themselves.”(Nurse Anesthetist 2, Hospital 3)
“We must also think about providing public hospitals with resources. Maybe it’s because they don’t have the financial means that they do pretty much.”(Nurse Anesthetist 3, Hospital 2)
“Yes, actually, at a given moment, you use what you have, and that’s it. If you see some Ciplox® (ciprofloxacin) in the box, you use it; if at another time, there isn’t any, you don’t use anything at all.”(Anesthetist Medical Doctor 2, Hospital 1)
“It’s here, in reanimation, that our doctors said, ‘No more ampicillin here.’ The antibiotic you should use is co-amoxiclav (amoxicillin + clavulanic acid); at least that’s what we use. That’s not a hospital consensus.”(Nurse Anesthetist 1, Hospital 1)
“But apparently it was the hospital managers who have left to some workshops; but they didn’t give us any feedback.”(Gynecologist Medical Doctor 1, Hospital 2)
“The gynecologists hold staff meetings every day, and we are invited to the Monday staff meeting. I think the communication methods need to be reviewed because when we say, ‘That’s what needs to be done,’ they come along and do things their way.”(Anesthetist Medical Doctor 1, Hospital 1)
“That’s why I don’t agree completely with my colleague, because she’s not aware of what is in the kit and she hasn’t been curious enough to ask.”(Gynecologist Medical Doctor 1, Hospital 2)
“The thing is that here we don’t get any more information about the patients. I don’t know whether there are infections afterwards because we don’t know anything about what happens after day one.”(Anesthetist Medical Doctor 2, Hospital 1)
“No, not that I know; but if there is a structure like that in place and it was never obvious to them before that they should look at how antibiotic prophylaxis is carried out on women, there is something wrong.”(Anesthetist Medical Doctor 2, Hospital 1)
2.2.3. Healthcare Professionals’ Individual Determinants
“Respecting that protocol, which, in my opinion, is good and it avoids patients having to make unnecessary expenditures, could even lessen resistance.”(Gynecologist Medical Doctor 1, Hospital 2)
“We do what we have seen others do. You cannot just decide to use a third-generation cephalosporin, for example. That’s not in line with what is done.”(Anesthetist Medical Doctor 4, Hospital 1)
“No, we draw up our own protocol based on what we have experienced in the service.”(Gynecologist Medical Doctor 2, Hospital 3)
“But none of those molecules are available here in Benin. So, we are resigned to that.”(Anesthetist Medical Doctor 2, Hospital 1)
“Sometimes, we exaggerate in the antibiotic prophylaxis here. Me, I often have trouble when we want to do clean intervention (for example the planned hernia intervention), and we put Ceftriaxone for prophylaxis.”(Nurse Anesthetist 2, Hospital 3)
“Antibiotic prophylaxis is based on what’s in the kit. We use the antibiotics that are available in the kit.”(Gynecologist Medical Doctor 1, Hospital 2)
“In the end, the surgeon (doctor) decides on the antibiotic, which we continue after the surgical unit until the time comes to stop and replace it with oral administration.”(Operating Room Nurse, Hospital 2)
“After the intervention, it is the gynecologist who defines whether we should continue the prophylaxis or not and marks it in the post-operative protocol.”(Nurse Anesthetist 2, Hospital 3)
“Except that the ampicillin, we use there, I don’t really agree with that. Even if we can go to ceftriaxone, it will be good”(Nurse Anesthetist 3, Hospital 3)
“Because what I was taught about antibiotic prophylaxis when I was in training is that you have to start low and then go up”(Nurse Anesthetist 2, Hospital 3)
2.2.4. Central Organizational and Structural Determinants (Policy Management)
“Their kit is useless; when it comes to antibiotic prophylaxis, it’s worthless.”(Anesthetist Medical Doctor 3, Hospital 1)
“In my opinion, there was no consultation of local healthcare workers about this business of fees exemption in cesarean. It’s a political matter. We were very hesitant at first because the basis for it is not clear.”(Anesthetist Medical Doctor 1, Hospital 1)
“We have available to us a prepacked kit that includes an antibiotic that is not indicated for prophylaxis.”(Anesthetist Medical Doctor 2, Hospital 1)
2.2.5. Patient Behavior Determinants
“Let me tell you that for some time now, most can no longer manage to pay. They say, ‘we can’t buy it,” and we say, ‘go and buy whatever you can.’ Sometimes some of them come back with two bottles, others with one bottle.”(Nurse Anesthetist 1, Hospital 1)
3. Discussion
4. Materials and Methods
4.1. Assessment of the Level of Knowledge of Antibiotic Prophylaxis
4.2. Interviews
4.3. Data Management and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Caesarean Section Rates Continue to Rise, amid Growing Inequalities in Access. Available online: https://www.who.int/news/item/16-06-2021-caesarean-section-rates-continue-to-rise-amid-growing-inequalities-in-access (accessed on 30 May 2022).
- De Nardo, P.; Gentilotti, E.; Nguhuni, B.; Vairo, F.; Chaula, Z.; Nicastri, E.; Nassoro, M.; Bevilacqua, N.; Ismail, A.; Savoldi, A.; et al. Post-caesarean section surgical site infections at a Tanzanian tertiary hospital: A prospective observational study. J. Hosp. Infect. 2016, 93, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.; Zhang, J.; Mikolajczyk, R.; Torloni, M.R.; Gülmezoglu, A.M.; Betran, A.P. Association between rates of caesarean section and maternal and neonatal mortality in the 21st century: A worldwide population-based ecological study with longitudinal data. BJOG Int. J. Obstet. Gynaecol. 2015, 123, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Schantz, C.; Aboubakar, M.; Traoré, A.B.; Ravit, M.; de Loenzien, M.; Dumont, A. Caesarean section in Benin and Mali: Increased recourse to technology due to suffering and under-resourced facilities. Reprod. Biomed. Soc. Online 2020, 10, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Richard, F.; Ouattara, F.; Zongo, S. Fear, guilt, and debt: An exploration of women’s experience and perception of cesarean birth in Burkina Faso, West Africa. Int. J. Women’s Health 2014, 6, 469–478. [Google Scholar] [CrossRef] [Green Version]
- UN-DESA. Sustainable Development goal 3. 2017. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 28 July 2020).
- Ravit, M.; Audibert, M.; Ridde, V.; de Loenzien, M.; Schantz, C.; Dumont, A. Removing user fees to improve access to caesarean delivery: A quasi-experimental evaluation in western Africa. BMJ Glob. Health 2018, 3, e000558. [Google Scholar] [CrossRef] [Green Version]
- Witter, S.; Team, F.; Boukhalfa, C.; Cresswell, J.A.; Daou, Z.; Filippi, V.; Ganaba, R.; Goufodji, S.; Lange, I.L.; Marchal, B.; et al. Cost and impact of policies to remove and reduce fees for obstetric care in Benin, Burkina Faso, Mali and Morocco. Int. J. Equity Health 2016, 15, 123. [Google Scholar] [CrossRef] [Green Version]
- Ouedraogo, T.L.; Kpozehouen, A.; Gléglé-Hessou, Y.; Makoutodé, M.; Saizonou, J.; Tchama-Bouraima, M. Évaluation de la mise en œuvre de la gratuité de la césarienne au Bénin. Santé Publique 2013, 25, 507–515. [Google Scholar] [CrossRef]
- Centre de Recherche en Reproduction Humaine et en Démographie. L’évaluation De La Polotique De Gratuité De La Césarienne Dabs Cinq Zones Sanitaires, Bénin. FEMhealth, March 2014. Available online: extension://elhekieabhbkpmcefcoobjddigjcaadp/https://www.abdn.ac.uk/smmsn/documents/femhealth-PAC00117_Policy_Document_Benin-FRENCHLO.pdf (accessed on 1 June 2022).
- UNICEF. Data Warehouse. UNICEF DATA. 2019. Available online: https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=.MNCH_CSEC..&startPeriod=2015&endPeriod=2018 (accessed on 1 June 2022).
- UNICEF. Maternal Mortality—UNICEF DATA. UNICEF DATA, September 2019. Available online: https://data.unicef.org/topic/maternal-health/maternal-mortality/ (accessed on 29 May 2022).
- Dossou, J.-P.; Cresswell, J.A.; Makoutodé, P.; De Brouwere, V.; Witter, S.; Filippi, V.; Kanhonou, L.G.; Goufodji, S.B.; Lange, I.L.; Lawin, L.; et al. ‘Rowing against the current’: The policy process and effects of removing user fees for caesarean sections in Benin. BMJ Glob. Health 2018, 3, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Mongbo, V.; Godin, I.; Mahieu, C.; Ouendo, E.M.; Ouédraogo, L. La césarienne dans le contexte de gratuité au Bénin. Santé Publique 2016, 28, 399–407. [Google Scholar] [CrossRef]
- Ravit, M.; Audibert, M.; Ridde, V.; de Loenzien, M.; Schantz, C.; Dumont, A. Do free caesarean section policies increase inequalities in Benin and Mali? Int. J. Equity Health 2018, 17, 71. [Google Scholar] [CrossRef] [Green Version]
- Dohou, A.M.; Buda, V.O.; Yemoa, L.A.; Anagonou, S.; Van Bambeke, F.; Van Hees, T.; Dossou, F.M.; Dalleur, O. Antibiotic Usage in Patients Having Undergone Caesarean Section: A Three-Level Study in Benin. Antibiotics 2022, 11, 617. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendation on Prophylactic Antibiotics for Women Undergoing Caesarean Section; World Health Organization: Geneva, Switzerland, 2021; pp. 1–64. Available online: https://apps.who.int/iris/handle/10665/341865 (accessed on 10 April 2022).
- De Tejada, B. Antibiotic Use and Misuse during Pregnancy and Delivery: Benefits and Risks. Int. J. Environ. Res. Public Health 2014, 11, 7993–8009. [Google Scholar] [CrossRef] [Green Version]
- Van Schalkwyk, J.; van Eyk, N. Antibiotic Prophylaxis in Obstetric Procedures. J. Obstet. Gynaecol. Can. 2017, 39, e293–e299. [Google Scholar] [CrossRef]
- Mylonas, I. Antibiotic chemotherapy during pregnancy and lactation period: Aspects for consideration. Arch. Gynecol. Obstet. 2011, 283, 7–18. [Google Scholar] [CrossRef]
- Gindre, S.; Carles, M.; Aknouch, N.; Jambou, P.; Dellamonica, P.; Raucoules-Aimé, M.; Grimaud, D. Antibioprophylaxie chirurgicale: Évaluation de l’application des recommandations et validation des kits d’antibioprophylaxie. Ann. Françaises D’anesthésie Et De Réanimation 2004, 23, 116–123. [Google Scholar] [CrossRef]
- Kayihura, V.; Osman, N.B.; Bugalho, A.; Bergström, S. Choice of antibiotics for infection prophylaxis in emergency cesarean sections in low-income countries: A cost-benefit study in Mozambique. Acta Obstet. Gynecol. Scand. 2003, 82, 636–641. [Google Scholar] [CrossRef]
- Ocran, I.; Tagoe, D.N.A. Knowledge and attitude of healthcare workers and patients on healthcare associated infections in a regional hospital in Ghana. Asian Pac. J. Trop. Dis. 2014, 4, 135–139. [Google Scholar] [CrossRef]
- Ravit, M.; Philibert, A.; Tourigny, C.; Traore, M.; Coulibaly, A.; Dumont, A.; Fournier, P. The Hidden Costs of a Free Caesarean Section Policy in West Africa (Kayes Region, Mali). Matern. Child Health J. 2015, 19, 1734–1743. [Google Scholar] [CrossRef] [Green Version]
- Baadani, A.M.; Baig, K.; Alfahad, W.A.; Aldalbahi, S.; Omrani, A.S. Physicians’ knowledge, perceptions, and attitudes toward antimicrobial prescribing in Riyadh, Saudi Arabia. Saudi Med. J. 2015, 36, 613–619. [Google Scholar] [CrossRef]
- Traore, I.A.; Dakouré, P.W.H.; Zaré, C.; Ki, K.B.; Kambou, T.; Joachim, S.; Nazinigouba, O. Evaluation Des Connaissances Et Des Pratiques Sur L’antibioprophylaxie Chirurgicale Dans La Ville De Bobo-Dioulasso (Burkina-Faso). Available online: https://web-saraf.net/Evaluation-des-connaissances-et.html (accessed on 25 May 2016).
- Tóth, H.; Fésűs, A.; Kungler-Gorácz, O.; Balázs, B.; Majoros, L.; Szarka, K.; Kardos, G. Utilization of Vector Autoregressive and Linear Transfer Models to Follow Up the Antibiotic Resistance Spiral in Gram-negative Bacteria From Cephalosporin Consumption to Colistin Resistance. Clin. Infect. Dis. 2018, 69, 1410–1421. [Google Scholar] [CrossRef]
- Nair, M.; Tripathi, S.; Mazumdar, S.; Mahajan, R.; Harshana, A.; Pereira, A.; Jimenez, C.; Halder, D.; Burza, S. Knowledge, attitudes, and practices related to antibiotic use in Paschim Bardhaman District: A survey of healthcare providers in West Bengal, India. PLoS ONE 2019, 14, e0217818. [Google Scholar] [CrossRef] [Green Version]
- Gouvêa, M.; Novaes, C.D.O.; Pereira, D.M.T.; Iglesias, A.C. Adherence to guidelines for surgical antibiotic prophylaxis: A review. Braz. J. Infect. Dis. 2015, 19, 517–524. [Google Scholar] [CrossRef] [Green Version]
- Liabsuetrakul, T.; Chongsuvivatwong, V.; Lumbiganon, P.; Lindmark, G. Obstetricians’ attitudes, subjective norms, perceived controls, and intentions on antibiotic prophylaxis in caesarean section. Soc. Sci. Med. 2003, 57, 1665–1674. [Google Scholar] [CrossRef]
- Vahdat, S.; Hamzehgardeshi, L.; Hessam, S.; Hamzehgardeshi, Z. Patient Involvement in Health Care Decision Making: A Review. Iran. Red. Crescent Med. J. 2014, 16, e12454. [Google Scholar] [CrossRef] [Green Version]
- Ray, R. Designing and Conducting Mixed Methods Research [Book Review]. Qual. Res. J. 2007, 7, 90–91. [Google Scholar] [CrossRef]
- Bengtsson, M. How to plan and perform a qualitative study using content analysis. NursingPlus Open 2016, 2, 8–14. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Number of HcPs, N | 33 |
| Hosp1 | 29 |
| Hosp2 | 04 |
| Hosp3 | 09 |
| Male | 17 |
| Female | 16 |
| Anesthetists MD | 03 |
| Obstetricians | 04 |
| Specialized anesthetists | 06 |
| Nurse anesthetists | 20 |
| Median age (years old) | 39.6 |
| (Min: 23–Max: 57) | |
| Median professional seniority (years) | 7.8 |
| (Min: 1–Max: 22) | |
| Criteria | Medical Doctor n = 13 (%) | Nurse n = 20 (%) | |
|---|---|---|---|
| Choice of antibiotic | Ampicillin | 2 (15.4) | 5 (25.0) |
| Amoxicillin + clavulanic acid | 6 (46.2) | 6 (30.0) | |
| Cefazoline | 3 (23.1) | 0 (0.0) | |
| Ceftriaxone | 2 (15.4) | 1 (5.0) | |
| Did not know | 0 (0.0) | 8 (40.0) | |
| Dose | Good | 9 (69.2) | 8 (40.0) |
| Wrong | 4 (30.8) | 10 (50.0) | |
| Duration | Good | 10 (76.9) | 6 (30.0) |
| Wrong | 3 (2.3) | 14 (70.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dohou, A.M.; Buda, V.O.; Anagonou, S.; Van Bambeke, F.; Van Hees, T.; Dossou, F.M.; Dalleur, O. Healthcare Professionals’ Knowledge and Beliefs on Antibiotic Prophylaxis in Cesarean Section: A Mixed-Methods Study in Benin. Antibiotics 2022, 11, 872. https://doi.org/10.3390/antibiotics11070872
Dohou AM, Buda VO, Anagonou S, Van Bambeke F, Van Hees T, Dossou FM, Dalleur O. Healthcare Professionals’ Knowledge and Beliefs on Antibiotic Prophylaxis in Cesarean Section: A Mixed-Methods Study in Benin. Antibiotics. 2022; 11(7):872. https://doi.org/10.3390/antibiotics11070872
Chicago/Turabian StyleDohou, Angèle Modupè, Valentina Oana Buda, Severin Anagonou, Françoise Van Bambeke, Thierry Van Hees, Francis Moïse Dossou, and Olivia Dalleur. 2022. "Healthcare Professionals’ Knowledge and Beliefs on Antibiotic Prophylaxis in Cesarean Section: A Mixed-Methods Study in Benin" Antibiotics 11, no. 7: 872. https://doi.org/10.3390/antibiotics11070872