
Safety and Efficacy of Ivermectin for the Prevention and Treatment of COVID-19: A Double-Blinded Randomized Placebo-Controlled Study

 ,
,  , , and
, , and
Abstract
:1. Background
2. Methods
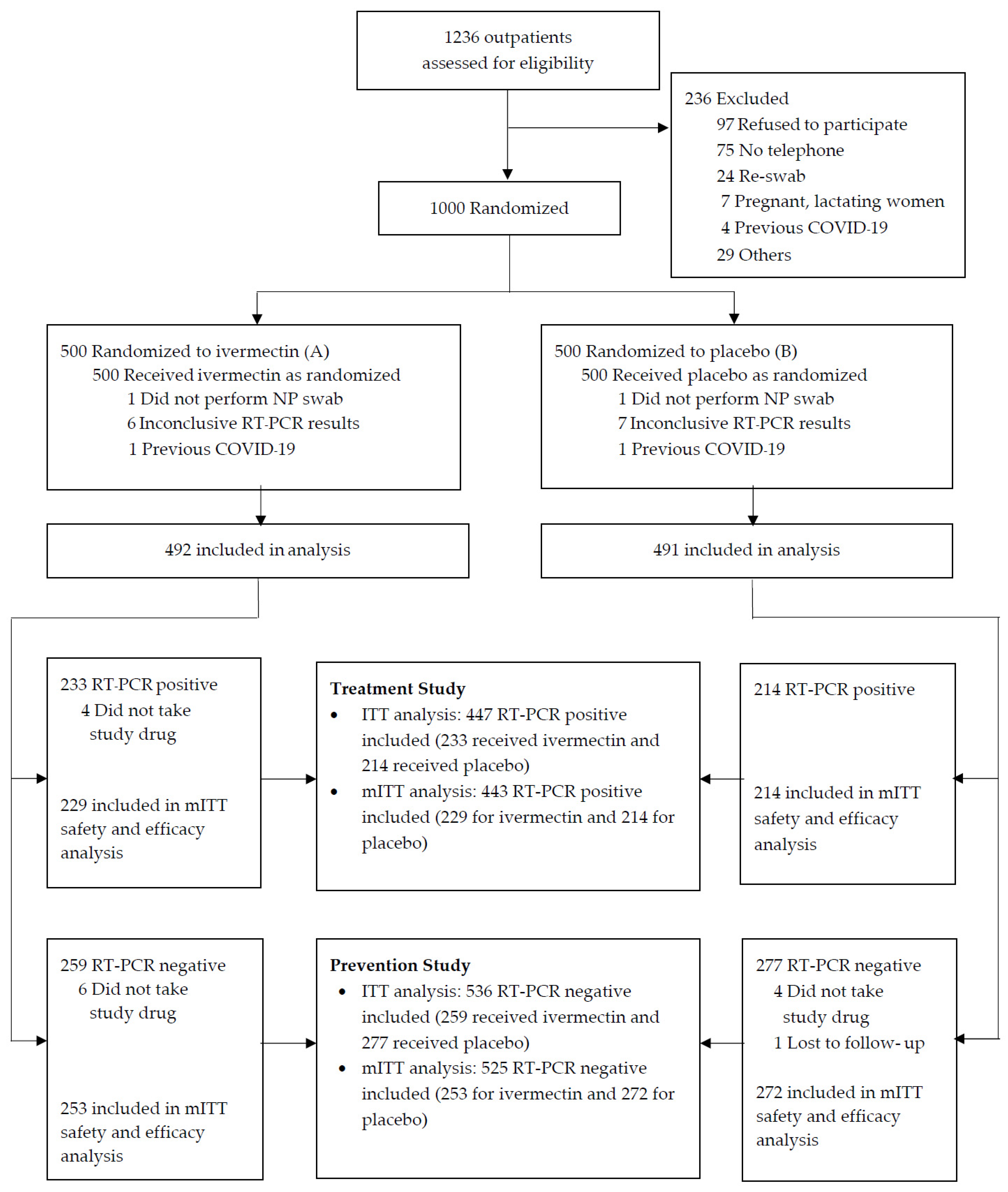
2.1. Study Design and Patients
2.2. Randomization and Masking
2.3. Interventions
2.4. Procedures
2.5. Outcome Measurement
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Primary Outcome of Ivermectin Prevention Study
3.2. Primary Outcomes of Ivermectin Treatment Study
3.3. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2022; Available online: https://covid19.who.int (accessed on 1 March 2022).
- Murray, C.J.L.; Piot, P. The Potential Future of the COVID-19 Pandemic: Will SARS-CoV-2 Become a Recurrent Seasonal Infection? JAMA 2021, 325, 1249–1250. [Google Scholar] [CrossRef] [PubMed]
- Rayner, C.R.; Dron, L.; Park, J.J.H.; Decloedt, E.H.; Cotton, M.F.; Niranjan, V.; Smith, P.F.; Dodds, M.G.; Brown, F.; Reis, G.; et al. Accelerating Clinical Evaluation of Repurposed Combination Therapies for COVID-19. Am. J. Trop. Med. Hyg. 2020, 103, 1364–1366. [Google Scholar] [CrossRef] [PubMed]
- Caly, L.; Druce, J.D.; Catton, M.G.; Jans, D.A.; Wagstaff, K.M. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antivir. Res. 2020, 178, 104787. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Song, Y.; Ci, X.; An, N.; Ju, Y.; Li, H.; Wang, X.; Han, C.; Cui, J.; Deng, X. Ivermectin inhibits LPS-induced production of inflammatory cytokines and improves LPS-induced survival in mice. Inflamm. Res. 2008, 57, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Popp, M.; Stegemann, M.; Metzendorf, M.I.; Gould, S.; Kranke, P.; Meybohm, P.; Skoetz, N.; Weibel, S. Ivermectin for preventing and treating COVID-19. Cochrane Database Syst. Rev. 2021, 7, CD015017. [Google Scholar] [CrossRef]
- Navarro, M.; Camprubi, D.; Requena-Mendez, A.; Buonfrate, D.; Giorli, G.; Kamgno, J.; Gardon, J.; Boussinesq, M.; Munoz, J.; Krolewiecki, A. Safety of high-dose ivermectin: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2020, 75, 827–834. [Google Scholar] [CrossRef]
- Abd-Elsalam, S.; Noor, R.A.; Badawi, R.; Khalaf, M.; Esmail, E.S.; Soliman, S.; Abd El Ghafar, M.S.; Elbahnasawy, M.; Moustafa, E.F.; Hassany, S.M.; et al. Clinical study evaluating the efficacy of ivermectin in COVID-19 treatment: A randomized controlled study. J. Med. Virol. 2021, 93, 5833–5838. [Google Scholar] [CrossRef]
- Ahmed, S.; Karim, M.M.; Ross, A.G.; Hossain, M.S.; Clemens, J.D.; Sumiya, M.K.; Phru, C.S.; Rahman, M.; Zaman, K.; Somani, J.; et al. A five-day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness. Int. J. Infect. Dis. 2021, 103, 214–216. [Google Scholar] [CrossRef]
- Ravikirti; Roy, R.; Pattadar, C.; Raj, R.; Agarwal, N.; Biswas, B.; Manjhi, P.K.; Rai, D.K.; Shyama; Kumar, A.; et al. Evaluation of Ivermectin as a Potential Treatment for Mild to Moderate COVID-19: A Double-Blind Randomized Placebo Controlled Trial in Eastern India. J. Pharm. Pharm. Sci. 2021, 24, 343–350. [Google Scholar] [CrossRef]
- Behera, P.; Patro, B.K.; Singh, A.K.; Chandanshive, P.D.; Ravikumar, S.R.; Pradhan, S.K.; Pentapati, S.S.K.; Batmanabane, G.; Mohapatra, P.R.; Padhy, B.M.; et al. Role of ivermectin in the prevention of SARS-CoV-2 infection among healthcare workers in India: A matched case-control study. PLoS ONE 2021, 16, e0247163. [Google Scholar] [CrossRef]
- WHO Working Group on the Clinical Characterisation and Management of COVID-19 Infection. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 2020, 20, e192–e197. [Google Scholar] [CrossRef]
- Shoumann, W.M.; Hegazy, A.A.; Nafae, R.M.; Ragab, M.I.; Samra, S.R.; Ibrahim, D.A.; Al-Mahrouky, T.H.; Sileem, A.E. Use of Ivermectin as a Potential Chemoprophylaxis for COVID-19 in Egypt: A Randomised Clinical Trial. J. Clin. Diagn. Res. 2021, 15, 6. [Google Scholar] [CrossRef]
- World Health Organization. Joint Intra-Action Review of the Public Health Response to COVID-19 in Thailand, 20–24 July 2020. Available online: https://www.who.int/docs/default-source/searo/thailand/iar-covid19-en.pdf (accessed on 1 March 2022).
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Pano-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Chesini, F.; Martini, D.; Roncaglioni, M.C.; Ojeda Fernandez, M.L.; Alvisi, M.F.; De Simone, I.; Rulli, E.; Nobili, A.; Casalini, G.; et al. High-dose ivermectin for early treatment of COVID-19 (COVER study): A randomised, double-blind, multicentre, phase II, dose-finding, proof-of-concept clinical trial. Int. J. Antimicrob. Agents 2022, 56, 106516. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Medina, E.; Lopez, P.; Hurtado, I.C.; Davalos, D.M.; Ramirez, O.; Martinez, E.; Diazgranados, J.A.; Onate, J.M.; Chavarriaga, H.; Herrera, S.; et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults with Mild COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1426–1435. [Google Scholar] [CrossRef]
- Vallejos, J.; Zoni, R.; Bangher, M.; Villamandos, S.; Bobadilla, A.; Plano, F.; Campias, C.; Chaparro Campias, E.; Medina, M.F.; Achinelli, F.; et al. Ivermectin to prevent hospitalizations in patients with COVID-19 (IVERCOR-COVID19) a randomized, double-blind, placebo-controlled trial. BMC Infect. Dis. 2021, 21, 635. [Google Scholar] [CrossRef]
- Reis, G.; Silva, E.; Silva, D.C.M.; Thabane, L.; Milagres, A.C.; Ferreira, T.S.; Dos Santos, C.V.Q.; Campos, V.H.S.; Nogueira, A.M.R.; de Almeida, A.; et al. Effect of Early Treatment with Ivermectin among Patients with Covid-19. N. Engl. J. Med. 2022, 386, 1721–1731. [Google Scholar] [CrossRef]
- Hill, A.; Mirchandani, M.; Pilkington, V. Ivermectin for COVID-19: Addressing Potential Bias and Medical Fraud. Open Forum. Infect. Dis. 2022, 9, ofab645. [Google Scholar] [CrossRef]
- Hassanipour, S.; Arab-Zozani, M.; Amani, B.; Heidarzad, F.; Fathalipour, M.; Martinez-de-Hoyo, R. The efficacy and safety of Favipiravir in treatment of COVID-19: A systematic review and meta-analysis of clinical trials. Sci. Rep. 2021, 11, 11022, Erratum in Sci. Rep. 2022, 12, 1996. [Google Scholar] [CrossRef]
- Smit, M.R.; Ochomo, E.O.; Aljayyoussi, G.; Kwambai, T.K.; Abong’o, B.O.; Chen, T.; Bousema, T.; Slater, H.C.; Waterhouse, D.; Bayoh, N.M.; et al. Safety and mosquitocidal efficacy of high-dose ivermectin when co-administered with dihydroartemisinin-piperaquine in Kenyan adults with uncomplicated malaria (IVERMAL): A randomised, double-blind, placebo-controlled trial. Lancet Infect. Dis. 2018, 18, 615–626. [Google Scholar] [CrossRef]
- Schmith, V.D.; Zhou, J.J.; Lohmer, L.R.L. The Approved Dose of Ivermectin Alone is not the Ideal Dose for the Treatment of COVID-19. Clin. Pharmacol. Ther. 2020, 108, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Krolewiecki, A.; Lifschitz, A.; Moragas, M.; Travacio, M.; Valentini, R.; Alonso, D.F.; Solari, R.; Tinelli, M.A.; Cimino, R.O.; Alvarez, L.; et al. Antiviral effect of high-dose ivermectin in adults with COVID-19: A proof-of-concept randomized trial. EClinicalMedicine 2021, 37, 100959. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://ddc.moph.go.th/viralpneumonia/index.php (accessed on 1 March 2022).
- Sirijatuphat, R.; Suputtamongkol, Y.; Angkasekwinai, N.; Horthongkham, N.; Chayakulkeeree, M.; Rattanaumpawan, P.; Kantakamalakul, W. Epidemiology, clinical characteristics, and treatment outcomes of patients with COVID-19 at Thailand’s university-based referral hospital. BMC Infect. Dis. 2021, 21, 382. [Google Scholar] [CrossRef] [PubMed]
- Guzzo, C.A.; Furtek, C.I.; Porras, A.G.; Chen, C.; Tipping, R.; Clineschmidt, C.M.; Sciberras, D.G.; Hsieh, J.Y.K.; Lasseter, K.C. Safety, tolerability, and pharmacokinetics of escalating high doses of ivermectin in healthy adult subjects. J. Clin. Pharmacol. 2002, 42, 1122–1133. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, A.B.; Berwanger, O.; Zampieri, F.G. Hydroxychloroquine with or without Azithromycin in Covid-19. Reply. N. Engl. J. Med. 2021, 384, 191. [Google Scholar]
- Roman, Y.M.; Burela, P.A.; Pasupuleti, V.; Piscoya, A.; Vidal, J.E.; Hernandez, A.V. Ivermectin for the treatment of COVID-19: A systematic review and meta-analysis of randomized controlled trials. Clin. Infect. Dis. 2021, 28, e434–e460. [Google Scholar]
- Andrew Hill, A.A.; Ahmed, S.; Asghar, A. Meta-Analysis of Randomized Trials of Ivermectin to Treat SARS-CoV-2 Infection; Research Square: Durham, NC, USA, 2021. [Google Scholar]
- Hellwig, M.D.; Maia, A.A. COVID-19 prophylaxis? Lower incidence associated with prophylactic administration of ivermectin. Int. J. Antimicrob. Agents 2021, 57, 106248. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total | Ivermectin | Placebo | p Value |
|---|---|---|---|---|
| n = 536 | n = 259 | n = 277 | ||
| Age (years) | ||||
| Mean (SD) | 37.6 (12.0) | 37.8 (12.6) | 37.4 (11.6) | 0.727 |
| Median (range) | 37 (18, 72) | 37 (18, 72) | 37 (18, 60) | 0.960 |
| Gender, n (%) | 0.930 | |||
| Male | 226 (42.2) | 110 (42.2) | 116 (42.0) | |
| Female | 310 (57.8) | 149 (57.5) | 161 (58.1) | |
| Body weight, kg | ||||
| Median (range) | 65.1 (35.3, 142.5) | 64.4 (35.3, 142.5) | 65.3 (37.8, 110.2) | 0.995 |
| Mean (SD) | 67.0 (15.9) | 67.3 (16.9) | 66.7 (14.9) | 0.672 |
| ≤90 kg | 487 (90.9) | 232 (89.6) | 255 (92.1) | 0.369 |
| >90 kg | 49 (9.1) | 27 (10.4) | 22 (7.9) | |
| Presence of underlying diseases, n (%) | 158 (29.5) | 73 (28.2) | 85 (30.7) | 0.570 |
| Hypertension | 47 (8.8) | 20 (7.7) | 27 (9.7) | 0.447 |
| Diabetes mellitus | 25 (4.7) | 10 (3.9) | 15 (5.4) | 0.420 |
| Dyslipidemia | 25 (4.7) | 10 (3.9) | 15 (5.4) | 0.420 |
| Coronary artery disease | 6 (1.1) | 5 (1.9) | 1 (0.4) | 0.112 |
| Chronic lung diseases | 1 (0.2) | 0 (0.0) | 1 (0.4) | 1.000 |
| Cerebrovascular disease | 2 (0.4) | 0 (0.0) | 2 (0.7) | 0.500 |
| Cancer | 7 (1.3) | 3 (1.2) | 4 (1.4) | 1.000 |
| Others | 97 (18.1) | 45 (17.4) | 52 (18.8) | 0.737 |
| Duration between last exposure to a COVID-19 patient and enrollment (n = 495) | 1.000 | |||
| Median (range) | 2 (0, 66) | 2 (0, 17) | 3 (0, 66) | 0.336 |
| ≤7 days | 443 (89.5) | 219 (89.4) | 224 (89.6) | 1.000 |
| >7 days | 52 (10.5) | 26 (10.6) | 26 (10.4) | |
| Exposure risk: household contact | 495 (92.4) | 245 (94.6) | 250 (90.3) | 0.073 |
| Presence of symptoms, n (%) | ||||
| Asymptomatic | 206 (38.4) | 104 (40.2) | 102 (36.8) | 0.477 |
| Symptomatic | 330 (61.6) | 155 (59.8) | 175 (63.2) | |
| Sore throat | 186 (34.7) | 91 (35.1) | 95 (34.3) | 0.856 |
| Cough | 136 (25.4) | 57 (22.0) | 79 (28.5) | 0.092 |
| Runny nose | 89 (16.6) | 43 (16.6) | 46 (16.6) | 1.000 |
| Fever | 73 (13.6) | 32 (12.4) | 41 (14.8) | 0.451 |
| Dyspnea | 27 (5.0) | 9 (3.5) | 18 (6.5) | 0.118 |
| Diarrhea | 19 (3.5) | 9 (3.5) | 10 (3.6) | 1.000 |
| Chest pain | 6 (1.1) | 2 (0.8) | 4 (1.4) | 0.687 |
| Vomiting | 5 (0.9) | 4 (1.5) | 1 (0.4) | 0.202 |
| Loss of taste/smell | 4 (0.7) | 0 (0.0) | 4 (1.4) | 0.124 |
| Others | 114 (21.3) | 52 (20.1) | 62 (22.4) | 0.528 |
| Duration of illness, (n = 330) | ||||
| Median (range) | 2 (0, 20) | 2 (0, 20) | 2 (0, 14) | 0.692 |
| <3 days | 191 (57.9) | 88 (56.8) | 103 (58.9) | 0.738 |
| ≥3 days | 139 (42.1) | 67 (43.2) | 72 (41.1) | |
| Previous COVID-19 vaccination, n (%) | 0.604 | |||
| No | 85 (15.9) | 45 (17.4) | 40 (14.4) | |
| Incomplete vaccine course (1 dose with last dose < 2 weeks prior) | 34 (6.3) | 13 (5.0) | 21 (7.6) | |
| Incomplete vaccine course (1 dose with last dose ≥ 2 weeks prior) | 185 (34.5) | 92 (35.5) | 93 (33.6) | |
| Completed vaccine course (2 doses with last dose < 2 weeks prior) | 64 (11.9) | 32 (12.4) | 32 (11.6) | |
| Completed vaccine course (2 doses with last dose ≥ 2 weeks prior or 3 doses with any duration) | 168 (31.3) | 77 (29.7) | 91 (32.9) | |
| Compliance with study medication | 0.884 | |||
| Full compliance, n (%) | 485 (90.5) | 235 (90.7) | 250 (90.3) | |
| Partial compliance, n (%) | 51 (9.5) | 24 (9.3) | 27 (9.7) |
| Primary Outcomes | Ivermectin | Placebo | p Value |
|---|---|---|---|
| ITT analysis (n = 536) | n = 259 | n = 277 | |
| Proportion of COVID-19 infection within 14 days, n (%) | 18 (6.95) | 19 (6.86) | 1.000 |
| Difference (95% CI) | 0.09% (−4.30–4.57) | ||
| Median (range) time to positive SARS-CoV-2 test (days) | 6 (3, 11) | 6 (1, 14) | 0.327 |
| Modified ITT analysis (n = 525) | n = 253 | n = 272 | |
| Proportion of COVID-19 infection within 14 days, n (%) | 12 (4.74) | 14 (5.15) | 0.844 |
| Difference (95% CI) | −0.41% (−4.28–3.53) | ||
| Median (range) time to positive SARS-CoV-2 test (days) | 6 (3, 11) | 4.5 (1, 14) | 0.374 |
| Ct value of participants who became positive within 14 days, mean (SD) * | |||
| N gene | 18.0 (2.8) | 16.8 (3.0) | 0.418 |
| E gene | 14.3 (2.9) | 13.3 (3.0) | 0.456 |
| RdRp gene | 18.9 (2.8) | 18.1 (2.8) | 0.674 |
| Characteristics | Total | Ivermectin | Placebo | p Value |
|---|---|---|---|---|
| n = 447 | n = 233 | n = 214 | ||
| Age (years) | ||||
| Mean (SD) | 39.5 (12.1) | 39.1 (12.0) | 39.8 (12.3) | 0.570 |
| Median (range) | 39 (18, 72) | 39 (18, 69) | 40 (18, 72) | 0.612 |
| Gender, n (%) | 0.566 | |||
| Male | 193 (43.2) | 104 (44.6) | 89 (41.6) | |
| Female | 254 (56.8) | 129 (55.4) | 125 (58.4) | |
| Body weight, kg | ||||
| Median (range) | 66.2 (36.3, 138.0) | 66.3 (36.3, 138.0) | 66.2 (36.6, 118.5) | 0.598 |
| Mean (SD) | 68.5 (16.1) | 68.1 (16.3) | 69.0 (15.9) | 0.608 |
| ≤90 kg, n (%) | 406 (90.8) | 214 (91.8) | 192 (89.7) | 0.512 |
| >90 kg, n (%) | 41 (9.2) | 19 (8.2) | 22 (10.3) | |
| Presence of underlying diseases, n (%) | 143 (32.0) | 70 (30.0) | 73 (34.1) | 0.363 |
| Hypertension | 50 (11.2) | 22 (9.4) | 28 (13.1) | 0.233 |
| Diabetes mellitus | 31 (6.9) | 14 (6.0) | 17 (7.9) | 0.460 |
| Dyslipidemia | 25 (5.6) | 12 (5.2) | 13 (6.1) | 0.686 |
| Coronary artery disease | 8 (1.8) | 4 (1.7) | 4 (1.9) | 1.000 |
| Chronic kidney disease | 2 (0.4) | 1 (0.4) | 1 (0.5) | 1.000 |
| Cirrhosis | 1 (0.2) | 1 (0.4) | 0 (0.0) | 1.000 |
| Chronic lung diseases | 1 (0.2) | 0 (0.0) | 1 (0.5) | 0.481 |
| Cerebrovascular disease | 1 (0.2) | 0 (0.0) | 1 (0.5) | 0.481 |
| Cancer | 1 (0.2) | 0 (0.0) | 1 (0.5) | 0.481 |
| Autoimmune disease | 2 (0.4) | 0 (0.0) | 2 (0.9) | 0.229 |
| Others | 62 (13.9) | 36 (15.5) | 26 (12.1) | 0.340 |
| Exposure risk: household contact, n (%) | 314 (70.2) | 158 (67.8) | 156 (72.9) | 0.256 |
| Duration between last exposure to a COVID-19 patient and enrollment (n = 313) | ||||
| Median (range) | 2 (0, 25) | 2.5 (0, 25) | 2 (0, 16) | 0.356 |
| ≤7 days, n (%) | 292 (93.3) | 146 (92.4) | 146 (94.2) | 0.653 |
| >7 days, n (%) | 21 (6.7) | 12 (7.6) | 9 (5.8) | |
| Presence of symptoms, n (%) | ||||
| Asymptomatic | 52 (11.6) | 24 (10.3) | 28 (13.1) | 0.379 |
| Symptomatic | 395 (88.4) | 209 (89.7) | 186 (86.9) | |
| Cough | 226 (50.6) | 129 (55.4) | 97 (45.3) | 0.037 |
| Sore throat | 210 (47.0) | 115 (49.4) | 95 (44.4) | 0.299 |
| Fever | 170 (38.0) | 90 (38.6) | 80 (37.4) | 0.845 |
| Runny nose | 156 (34.9) | 85 (36.5) | 71 (33.2) | 0.488 |
| Loss of taste/smell | 79 (17.7) | 34 (14.6) | 45 (21.0) | 0.083 |
| Dyspnea | 31 (6.9) | 21 (9.0) | 10 (4.7) | 0.093 |
| Diarrhea | 25 (5.6) | 12 (5.2) | 13 (6.1) | 0.686 |
| Chest pain | 5 (1.1) | 2 (0.9) | 3 (1.4) | 0.674 |
| Vomiting | 2 (0.4) | 1 (0.4) | 1 (0.5) | 1.000 |
| Others | 126 (28.2) | 70 (30.0) | 56 (26.2) | 0.400 |
| Duration of illness, (n = 394) | ||||
| Median (range) | 2 (0, 10) | 2 (0, 10) | 2 (0, 10) | 0.990 |
| <3 days, n (%) | 219 (55.6) | 115 (55.3) | 104 (55.9) | 0.919 |
| ≥3 days, n (%) | 175 (44.4) | 93 (44.7) | 82 (44.1) | |
| RT-PCR Ct value | ||||
| Mean (SD) | 20.2 (5.3) | 20.0 (5.2) | 20.4 (5.4) | 0.460 |
| <20, n (%) | 266 (59.5) | 141 (60.5) | 125 (58.4) | 0.700 |
| ≥20, n (%) | 181 (40.5) | 92 (39.5) | 89 (41.6) | |
| Oxygen saturation (%), mean (SD) | 97.9 (1.1) | 97.9 (1.0) | 97.9 (1.2) | 0.964 |
| Oxygen saturation < 96%, n (%) | 6 (1.3) | 1 (0.4) | 5 (2.3) | 0.109 |
| WHO clinical score, median (range) | 2 (1, 2) | 2 (1, 2) | 2 (1, 2) | 0.360 |
| Score 1, n (%) | 52 (11.6) | 24 (10.3) | 28 (13.1) | 0.379 |
| Score 2, n (%) | 395 (88.4) | 209 (89.7) | 186 (86.9) | |
| Previous vaccination, n (%) | 0.522 | |||
| No | 112 (25.1) | 65 (27.9) | 47 (22.0) | |
| Incomplete vaccine course (1 dose with last dose < 2 weeks prior) | 30 (6.7) | 17 (7.3) | 13 (6.1) | |
| Incomplete vaccine course (1 dose with last dose ≥ 2 weeks prior) | 184 (41.2) | 90 (38.6) | 94 (43.9) | |
| Completed vaccine course (2 doses with last dose < 2 weeks prior) | 25 (5.6) | 11 (4.7) | 14 (6.5) | |
| Completed vaccine course (2 doses with last dose ≥ 2 weeks prior or 3 doses with any duration) | 96 (21.5) | 50 (21.5) | 46 (21.5) | |
| Chest X-ray, n (%) | 0.993 | |||
| Normal | 264 (59.1) | 138 (59.2) | 126 (58.9) | |
| Unilateral infiltrate | 7 (1.6) | 4 (1.7) | 3 (1.4) | |
| Bilateral infiltrate | 6 (1.3) | 3 (1.3) | 3 (1.4) | |
| Not done | 170 (38.0) | 88 (37.8) | 82 (38.3) | |
| Admission type at baseline, n (%) | 0.072 | |||
| Quarantine hotel | 280 (62.6) | 145 (62.2) | 135 (63.1) | |
| Home isolation | 132 (29.5) | 67 (28.8) | 65 (30.4) | |
| Hospital | 33 (7.4) | 21 (9.0) | 12 (5.6) | |
| No admission | 1 (0.2) | 0 (0.0) | 1 (0.5) | |
| Unknown | 1 (0.2) | 0 (0.0) | 1 (0.5) | |
| Concomitant medication, n (%) | ||||
| Favipiravir | 435 (97.5) | 226 (97.4) | 209 (97.7) | 1.000 |
| Others | 3 (0.7) | 0 (0.0) | 3 (1.4) | 0.110 |
| Compliance with study medication, n (%) | 0.762 | |||
| Full compliance | 399 (89.3) | 209 (89.7) | 190 (88.8) | |
| Partial compliance | 48 (10.7) | 24 (10.3) | 24 (11.2) |
| Primary Outcomes | Ivermectin | Placebo | p Value |
|---|---|---|---|
| ITT analysis (n = 447) | n = 233 | n = 214 | |
| Proportion of participants with oxygen desaturation, n (%) ** | |||
| Day 3 | 2 (0.9) | 3 (1.4) | 0.674 |
| Day 7 | 2 (0.9) | 4 (1.9) | 0.433 |
| Day 14 | 6 (2.6) | 4 (1.9) | 0.753 |
| Change in WHO progression score from baseline | |||
| Day 3 | 0 (−3, 0) | 0 (−5, 0) | 0.462 |
| Day 7 | 0 (−4, 0) | 0 (−5, 0) | 0.256 |
| Day 14 | 1 (−5, 1) | 1 (−5, 1) | 0.348 |
| Absence of all symptoms, n (%) | |||
| Day 3 | 57 (24.5) | 44 (20.6) | 0.365 |
| Day 7 | 118 (50.6) | 115 (53.7) | 0.570 |
| Day 14 | 174 (74.7) | 176 (82.2) | 0.066 |
| Hospitalization due to clinical progression within 14 days, n (%) | 8 (3.4) | 4 (1.9) | 0.386 |
| 28-day mortality | 0 | 0 | - |
| Modified ITT analysis (n = 443) | n = 229 | n = 214 | |
| Proportion of participants with oxygen desaturation, n (%) ** | |||
| Day 3 | 2 (0.9) | 3 (1.4) | 0.676 |
| Day 7 | 2 (0.9) | 4 (1.9) | 0.435 |
| Day 14 | 6 (2.7) | 4 (1.9) | 0.752 |
| Change in WHO progression score from baseline | |||
| Day 3 | 0 (−3, 0) | 0 (−5, 0) | 0.436 |
| Day 7 | 0 (−4, 0) | 0 (−5, 0) | 0.239 |
| Day 14 | 1 (−5, 1) | 1 (−5, 1) | 0.501 |
| Absence of all symptoms, n (%) | |||
| Day 3 | 56 (24.5) | 44 (20.6) | 0.364 |
| Day 7 | 118 (51.5) | 115 (53.7) | 0.703 |
| Day 14 | 174 (76.0) | 176 (82.2) | 0.129 |
| Hospitalization due to clinical progression within 14 days, n (%) | 4 (1.7) | 4 (1.9) | 1.000 |
| 28-day mortality | 0 | 0 | - |
| AEs (mITT Population) | Ivermectin (n = 482) | Placebo (n = 486) | p Value | ||
|---|---|---|---|---|---|
| No. Events | No. Cases n (%) | No. Events | No. Cases n (%) | ||
| Total | 141 | 104 (21.6) | 144 | 92 (18.9) | 0.337 |
| Ocular problems | 28 | 27 (5.6) | 4 | 3 (0.6) | <0.001 |
| Diarrhea | 23 | 23 (4.8) | 21 | 19 (3.9) | 0.532 |
| Myalgia | 15 | 13 (2.7) | 19 | 17 (3.5) | 0.579 |
| Headache | 10 | 9 (1.9) | 25 | 22 (4.5) | 0.027 |
| Neurologic symptoms | 8 | 8 (1.7) | 11 | 10 (2.1) | 0.813 |
| Rash | 7 | 7 (1.5) | 4 | 4 (0.8) | 0.383 |
| Nausea/vomiting | 6 | 6 (1.2) | 12 | 11 (2.3) | 0.328 |
| Pruritus | 1 | 1 (0.2) | 3 | 3 (0.6) | 0.624 |
| Others | 43 | 40 (8.3) | 45 | 44 (9.1) | 0.732 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angkasekwinai, N.; Rattanaumpawan, P.; Chayakulkeeree, M.; Phoompoung, P.; Koomanachai, P.; Chantarasut, S.; Wangchinda, W.; Srinonprasert, V.; Thamlikitkul, V. Safety and Efficacy of Ivermectin for the Prevention and Treatment of COVID-19: A Double-Blinded Randomized Placebo-Controlled Study. Antibiotics 2022, 11, 796. https://doi.org/10.3390/antibiotics11060796
Angkasekwinai N, Rattanaumpawan P, Chayakulkeeree M, Phoompoung P, Koomanachai P, Chantarasut S, Wangchinda W, Srinonprasert V, Thamlikitkul V. Safety and Efficacy of Ivermectin for the Prevention and Treatment of COVID-19: A Double-Blinded Randomized Placebo-Controlled Study. Antibiotics. 2022; 11(6):796. https://doi.org/10.3390/antibiotics11060796
Chicago/Turabian StyleAngkasekwinai, Nasikarn, Pinyo Rattanaumpawan, Methee Chayakulkeeree, Pakpoom Phoompoung, Pornpan Koomanachai, Sorawit Chantarasut, Walaiporn Wangchinda, Varalak Srinonprasert, and Visanu Thamlikitkul. 2022. "Safety and Efficacy of Ivermectin for the Prevention and Treatment of COVID-19: A Double-Blinded Randomized Placebo-Controlled Study" Antibiotics 11, no. 6: 796. https://doi.org/10.3390/antibiotics11060796