
Self-Medication with Antibiotics: Prevalence, Practices and Related Factors among the Pakistani Public

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Results
2.1. Sociodemographic Characteristics of Study Participants
2.2. Reliability of the Instrument
2.2.1. Internal Consistency
2.2.2. Test–Retest Reliability
2.3. Practices and Knowledge about SMA
2.3.1. Prevalence of SMA among Study Participants
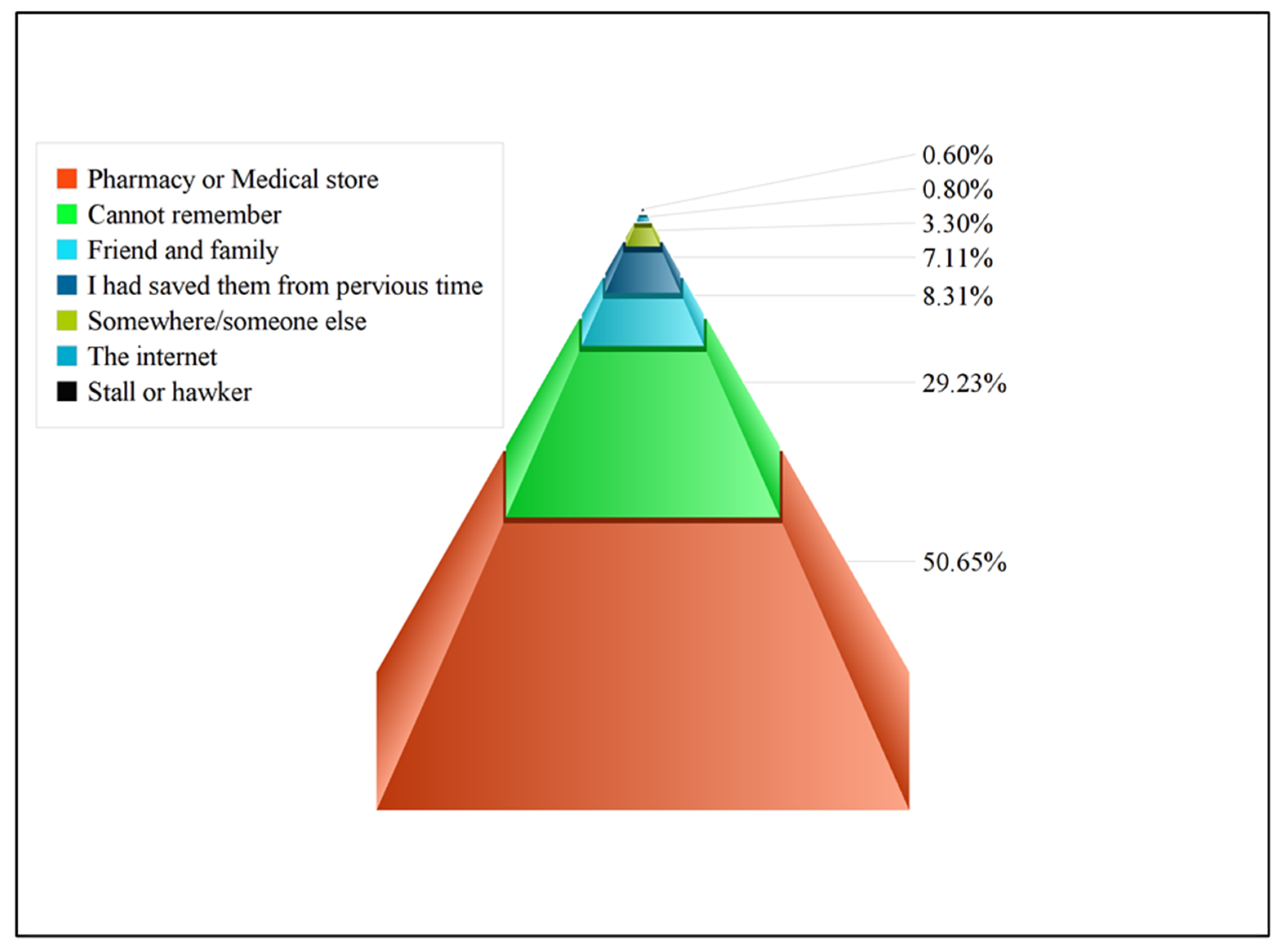
2.3.2. Commons Reasons for SMA and Common Sources for Obtaining Antibiotics
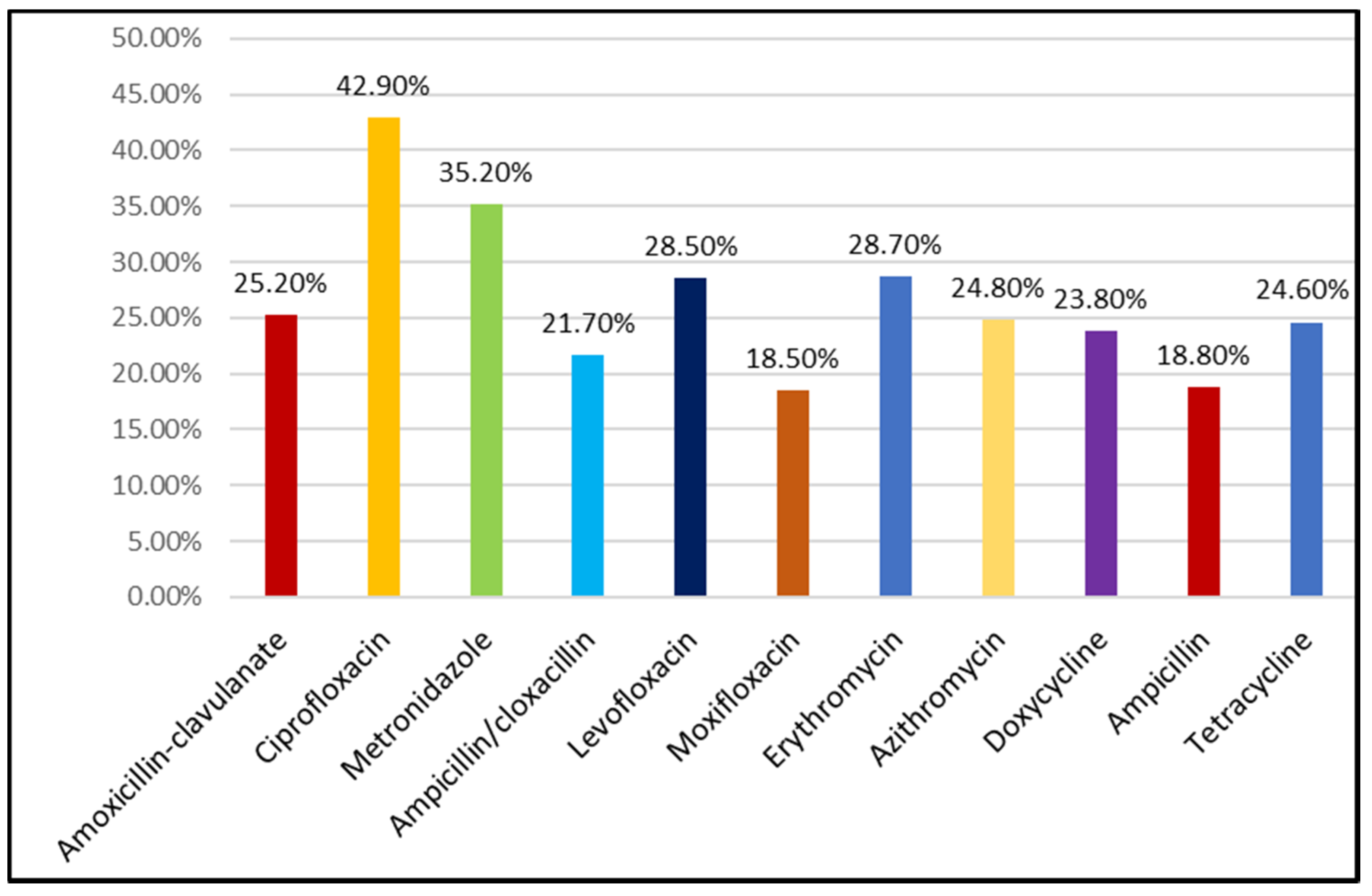
2.3.3. Trends in Antibiotic Usage
2.3.4. Knowledge, Attitude, and Practices towards SMA
2.3.5. Predictors of SMA
2.3.6. Public reported outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design and Settings
4.2. Study Population
4.3. Sample Size Calculation
4.4. Study Instrument
4.5. Data Collection
4.6. Statistical Analysis
4.7. Ethical Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guinovart, M.C.; Figueras, A.; Llop, J.C.; Llor, C. Obtaining antibiotics without prescription in Spain in 2014: Even easier now than 6 years ago. J. Antimicrob. Chemother. 2015, 70, 1270–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Widayati, A.; Suryawati, S.; de Crespigny, C.; Hiller, J.E. Self medication with antibiotics in Yogyakarta City Indonesia: A cross sectional population-based survey. BMC Res. Notes 2011, 4, 491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alghadeer, S.; Aljuaydi, K.; Babelghaith, S.; Alhammad, A.; Alarifi, M.N. Self-medication with antibiotics in Saudi Arabia. Saudi Pharm. J. 2018, 26, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Bilal, M.; Haseeb, A.; Khan, M.H.; Arshad, M.H.; Ladak, A.A.; Niazi, S.K.; Musharraf, M.D.; Manji, A.A. Self-Medication with Antibiotics among People Dwelling in Rural Areas of Sindh. J. Clin. Diagn. Res. JCDR 2016, 10, Oc08–Oc13. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- European Commission. Antibiotics Resistance. Survey Requested by the European Commission, Directorate-General for Health and Food Safety and Co-Ordinated by the Directorate-General for Communication. Available online: https://www.eusaferhealthcare.eu/wp-content/uploads/ebs_478_en-1-min.pdf (accessed on 1 January 2022).
- WHO. Antibiotic Resistance: Multi-Country Public Awareness Survey. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/194460 (accessed on 1 January 2022).
- Panasiuk, L.; Lukas, W.; Paprzycki, P.; Verheij, T.; Godycki-Ćwirko, M.; Chlabicz, S. Antibiotics in the treatment of upper respiratory tract infections in Poland. Is there any improvement? J. Clin. Pharm. Ther. 2010, 35, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Zajmi, D.; Berisha, M.; Begolli, I.; Hoxha, R.; Mehmeti, R.; Mulliqi-Osmani, G.; Kurti, A.; Loku, A.; Raka, L. Public knowledge, attitudes and practices regarding antibiotic use in Kosovo. Pharm. Pract. 2017, 15, 827. [Google Scholar] [CrossRef] [Green Version]
- Janssen, J.; Afari-Asiedu, S.; Monnier, A.; Abdulai, M.A.; Tawiah, T.; Wertheim, H.; Baltussen, R.; Asante, K.P. Exploring the economic impact of inappropriate antibiotic use: The case of upper respiratory tract infections in Ghana. Antimicrob. Resist. Infect. Control 2022, 11, 53. [Google Scholar] [CrossRef]
- Rijal, K.R.; Banjara, M.R.; Dhungel, B.; Kafle, S.; Gautam, K.; Ghimire, B.; Ghimire, P.; Dhungel, S.; Adhikari, N.; Shrestha, U.T. Use of antimicrobials and antimicrobial resistance in Nepal: A nationwide survey. Sci. Rep. 2021, 11, 11554. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E.; Stájer, A.; Baráth, Z. Antimicrobial Resistance in the Context of the Sustainable Development Goals: A Brief Review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 71–82. [Google Scholar] [CrossRef]
- WHO. International Organizations Unite on Critical Recommendations to Combat Drug-Resistant Infections and Prevent Staggering Number of Deaths Each Year. Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 10 February 2022).
- O’Neill, J. Review on Antimicrobial Resistance, December 2014. Available online: http://amr-review.org/ (accessed on 15 December 2021).
- Gajdács, M. The concept of an ideal antibiotic: Implications for drug design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.H.; Cohen, T.; Grad, Y.H.; Hanage, W.P.; O’Brien, T.F.; Lipsitch, M. Origin and proliferation of multiple-drug resistance in bacterial pathogens. Microbiol. Mol. Biol. Rev. 2015, 79, 101–116. [Google Scholar] [CrossRef] [Green Version]
- WHO. Antimicrobial Resistance: No Action Today, No Cure Tomorrow. Available online: https://www.who.int/dg/speeches/2011/WHD_20110407/en/ (accessed on 11 February 2022).
- Earnshaw, S.; Monnet, D.L.; Duncan, B.; O’Toole, J.; Ekdahl, K.; Goossens, H. European Antibiotic Awareness Day, 2008—The first Europe-wide public information campaign on prudent antibiotic use: Methods and survey of activities in participating countries. Eurosurveillance 2009, 14, 19280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aslam, A.; Gajdács, M.; Zin, C.S.; Ab Rahman, N.S.; Ahmed, S.I.; Zafar, M.Z.; Jamshed, S. Evidence of the Practice of Self-Medication with Antibiotics among the Lay Public in Low- and Middle-Income Countries: A Scoping Review. Antibiotics 2020, 9, 597. [Google Scholar] [CrossRef] [PubMed]
- Hadi, U.; Duerink, D.O.; Lestari, E.S.; Nagelkerke, N.J.; Werter, S.; Keuter, M.; Suwandojo, E.; Rahardjo, E.; van den Broek, P.; Gyssens, I.C. Survey of antibiotic use of individuals visiting public healthcare facilities in Indonesia. Int. J. Infect. Dis. 2008, 12, 622–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocan, M.; Obuku, E.A.; Bwanga, F.; Akena, D.; Richard, S.; Ogwal-Okeng, J.; Obua, C. Household antimicrobial self-medication: A systematic review and meta-analysis of the burden, risk factors and outcomes in developing countries. BMC Public Health 2015, 15, 742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uddin, T.M.; Chakraborty, A.J.; Khusro, A.; Zidan, B.R.M.; Mitra, S.; Emran, T.B.; Dhama, K.; Ripon, M.K.H.; Gajdács, M.; Sahibzada, M.U.K.; et al. Antibiotic resistance in microbes: History, mechanisms, therapeutic strategies and future prospects. J. Infect. Public Health 2021, 14, 1750–1766. [Google Scholar] [CrossRef]
- WHO. Report on Surveillance of Antibiotic Consumption. 2018. Available online: https://www.who.int/medicines/areas/rational_use/who-amr-amc-report-20181109.pdf (accessed on 14 February 2022).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Qidwai, W.; Krishanani, M.K.; Hashmi, S.; Afridi, M.; Ali, R.A. Private drug sellers’ education in improving prescribing practices. J. Coll. Physicians Surg. Pak. 2006, 16, 743–746. [Google Scholar]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Fatima, M.; Ahmad, Z.; Sajid, A.; Rehman, I.U.; Nadeem, M.U.; Javaid, Z.; Malik, M.; et al. Sale of WHO AWaRe groups antibiotics without a prescription in Pakistan: A simulated client study. J. Pharm. Policy Pract. 2020, 13, 26. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.J.; Khan, S.; Shah, N. Self-medication with antibiotics in urban areas of Peshawar. Gomal J. Med. Sci. 2011, 9, 19–22. [Google Scholar]
- Nazir, S.; Azim, M. Assessment of antibiotic self-medication practice among public in the northwestern region of Pakistan. Eur. J. Hosp. Pharm. 2017, 24, 200–203. [Google Scholar] [CrossRef] [PubMed]
- Michaelidou, M.; Karageorgos, S.A.; Tsioutis, C. Antibiotic Use and Antibiotic Resistance: Public Awareness Survey in the Republic of Cyprus. Antibiotics 2020, 9, 759. [Google Scholar] [CrossRef] [PubMed]
- Abduelkarem, A.R.; Othman, A.M.; Abuelkhair, Z.M.; Ghazal, M.M.; Alzouobi, S.B.; El Zowalaty, M.E. Prevalence Of Self-Medication with Antibiotics Among Residents in United Arab Emirates. Infect. Drug Resist. 2019, 12, 3445–3453. [Google Scholar] [CrossRef] [Green Version]
- Nyambega, J.O. Antibiotic use and misuse among adults in Magwagwa Ward, Nyamira County in Kenya. Age Ageing 2017, 18, 26–35. [Google Scholar] [CrossRef]
- Abdulraheem, I.; Adegboye, A.; Fatiregun, A. Self-medication with antibiotics: Empirical evidence from a Nigerian rural population. Br. J. Pharm. Res. 2016, 11, 1–13. [Google Scholar] [CrossRef]
- Albawani, S.M.; Hassan, Y.B.; Abd-Aziz, N.; Gnanasan, S. Self-medication with antibiotics in Sana’a City, Yemen. Trop. J. Pharm. Res. 2017, 16, 1195–1199. [Google Scholar] [CrossRef] [Green Version]
- Al-Qahtani, M.A.; Amin, H.S.; Al-Qahtani, A.A.; Alshahrani, A.M.; Alghamdi, H.A.; Althwayee, M.S.; Alzahrani, A.A. Self-medication with Antibiotics in a primary care setting in King Khalid University Hospital, Riyadh, Saudi Arabia. J. Family Community Med. 2018, 25, 95–101. [Google Scholar] [CrossRef]
- Bloom, G.; Merrett, G.B.; Wilkinson, A.; Lin, V.; Paulin, S. Antimicrobial resistance and universal health coverage. BMJ Glob. Health 2017, 2, e000518. [Google Scholar] [CrossRef]
- Abasaeed, A.; Vlcek, J.; Abuelkhair, M.; Kubena, A. Self-medication with antibiotics by the community of Abu Dhabi Emirate, United Arab Emirates. J. Infect. Dev. Ctries. 2009, 3, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Grigoryan, L.; Burgerhof, J.G.; Degener, J.E.; Deschepper, R.; Lundborg, C.S.; Monnet, D.L.; Scicluna, E.A.; Birkin, J.; Haaijer-Ruskamp, F.M. Determinants of self-medication with antibiotics in Europe: The impact of beliefs, country wealth and the healthcare system. J. Antimicrob. Chemother. 2008, 61, 1172–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramay, B.M.; Lambour, P.; Cerón, A. Comparing antibiotic self-medication in two socio-economic groups in Guatemala City: A descriptive cross-sectional study. BMC Pharmacol. Toxicol. 2015, 16, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamhour, A.; El-Kheir, A.; Salameh, P.; Hanna, P.A.; Mansour, H. Antibiotic knowledge and self-medication practices in a developing country: A cross-sectional study. Am. J. Infect. Control 2017, 45, 384–388. [Google Scholar] [CrossRef]
- Napolitano, F.; Izzo, M.T.; Di-Giuseppe, G.; Angelillo, I.F. Public knowledge, attitudes, and experience regarding the use of antibiotics in Italy. PLoS ONE 2013, 8, e84177. [Google Scholar] [CrossRef]
- Emeka, P.M.; Al-Omar, M.; Khan, T.M. Public attitude and justification to purchase antibiotics in the Eastern region Al Ahsa of Saudi Arabia. Saudi Pharm. J. 2014, 22, 550–554. [Google Scholar] [CrossRef] [Green Version]
- Aslam, A.; Zin, C.S.; Ab Rahman, N.S.; Gajdács, M.; Ahmed, S.I.; Jamshed, S. Self-Medication Practices with Antibiotics and Associated Factors among the Public of Malaysia: A Cross-Sectional Study. Drug Healthc. Patient Saf. Surg. 2021, 13, 171. [Google Scholar] [CrossRef]
- Ocan, M.; Bwanga, F.; Bbosa, G.S.; Bagenda, D.; Waako, P.; Ogwal-Okeng, J.; Obua, C. Patterns and predictors of self-medication in northern Uganda. PLoS ONE 2014, 9, e92323. [Google Scholar] [CrossRef]
- Malik, U.R.; Chang, J.; Hashmi, F.; Atif, N.; Basir, H.; Hayat, K.; Khan, F.U.; Kabba, J.A.; Lambojon, K.; Fang, Y. A Simulated Client Exploration of Nonprescription Dispensing of Antibiotics at Drugstores for Pediatric Acute Diarrhea and Upper Respiratory Infection in Lahore, Pakistan. Infect. Drug Resist. 2021, 14, 1129–1140. [Google Scholar] [CrossRef]
- Aslam, A.; Gajdács, M.; Zin, C.S.; Ab Rahman, N.S.; Ahmed, S.I.; Jamshed, S. Public Awareness and Practices towards Self-Medication with Antibiotics among the Malaysian Population. A Development of Questionnaire and Pilot-Testing. Antibiotics 2020, 9, 97. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.J.; Ahmad, H.; Rehan, R.B.; Najeeb, S.; Mumtaz, M.; Jilani, M.H.; Rabbani, M.S.; Alam, M.Z.; Farooq, S.; Kadir, M.M. Self-medication with antibiotics among non-medical university students of Karachi: A cross-sectional study. BMC Pharmacol. Toxicol. 2014, 15, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, H.; Cui, B.; Zhang, D.; Farrar, J.; Law, F.; Ba-Thein, W. Prior knowledge, older age, and higher allowance are risk factors for self-medication with antibiotics among university students in southern China. PLoS ONE 2012, 7, e41314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chanvatik, S.; Kosiyaporn, H.; Lekagul, A.; Kaewkhankhaeng, W.; Vongmongkol, V.; Thunyahan, A.; Tangcharoensathien, V. Knowledge and use of antibiotics in Thailand: A 2017 national household survey. PLoS ONE 2019, 14, e0220990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Rasheed, A.; Yagoub, U.; Alkhashan, H.; Abdelhay, O.; Alawwad, A.; Al-Aboud, A.; Battal, S.A. Prevalence and Predictors of Self-Medication with Antibiotics in Al Wazarat Health Center, Riyadh City, KSA. BioMed Res. Int. 2016, 2016, 3916874. [Google Scholar] [CrossRef] [Green Version]
- Pakistan, Govt. Second Phase of Census District Wise. Available online: https://web.archive.org/web/20170829164748/http://www.pbscensus.gov.pk/sites/default/files/DISTRICT_WISE_CENSUS_RESULTS_CENSUS_2017.pdf (accessed on 25 November 2021).
- Dicitionary, O. Oxford Learners Dictionary. Available online: https://www.oxfordlearnersdictionaries.com/definition/english/layperson?q=layperson (accessed on 25 January 2019).
- Charan, J.; Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [Green Version]
- Károlyházy, K.; Fazekas, B.; Fazekas, J.; Hermann, P.; Márton, K. Ebola virus disease: Awareness among dental students in Hungary. Acta Microbiol. Immunol. Hung. 2016, 63, 325–337. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Frequency (n) | Percentage (%) |
|---|---|---|
| Gender | ||
| Male | 267 | 55.6% |
| Female | 213 | 44.4% |
| Age (Years) | ||
| 21–25 yrs | 44 | 9.2% |
| 26–30 yrs | 95 | 19.8% |
| 31–40 yrs | 212 | 44.2% |
| Above 40 yrs | 129 | 26.8% |
| Marital status | ||
| Single | 114 | 23.7% |
| Married | 366 | 76.3% |
| Education | ||
| Primary school | 56 | 11.7% |
| Secondary school | 124 | 25.8% |
| Certificate/Diploma | 56 | 11.7% |
| Undergraduate degree/Bachelor’s degree | 170 | 35.4% |
| Postgraduate education | 74 | 15.4% |
| Income | ||
| Under PKR 10,000 | 15 | 3.1% |
| PKR 10,000 to 20,000 | 38 | 7.9% |
| Over PKR 20,000 | 427 | 89% |
| Occupation | ||
| Professional | 94 | 19.6% |
| Skilled labor | 21 | 4.4% |
| Manual labor | 19 | 4.0% |
| Administrative | 76 | 15.7% |
| Self-employed | 143 | 29.8% |
| Home duties | 93 | 19.4% |
| Unemployed | 23 | 4.8% |
| Pensioner | 11 | 2.3% |
| Children | ||
| No | 147 | 30.6% |
| Yes | 333 | 69.4% |
| Health Insurance | ||
| Yes | 29 | 6% |
| No | 434 | 90.4% |
| Not Sure | 17 | 3.6% |
| Characteristics | Prevalence of SMA | p-Value | ||
|---|---|---|---|---|
| Gender | Prescription Antibiotics (n, %) | Non-Prescription Antibiotics (n, %) | Cannot Remember (n, %) | |
| Male | 90 (18.8%) | 105 (21.9%) | 72 (15%) | 0.001 *** |
| Female | 74 (15.4%) | 51 (10.6%) | 88 (18.3%) | |
| Age (years) | ||||
| 21–25 yrs | 12 (2.5%) | 10 (2.1%) | 22 (4.6%) | 0.129 |
| 26–30 yrs | 33 (6.9%) | 31 (6.5%) | 31 (6.5%) | |
| 31–40 yrs | 64 (13.3%) | 74 (15.4%) | 74 (15.4%) | |
| Above 40 yrs | 41 (8.5%) | 55 (11.5%) | 33 (6.8%) | |
| Marital status | ||||
| Married | 128 (26.7%) | 130 (27.1%) | 108 (22.5%) | 0.003 ** |
| Single | 36 (7.5%) | 26 (5.4%) | 52 (10.8%) | |
| Education | ||||
| Primary school | 17 (3.5%) | 23 (4.8%) | 16 (3.3%) | 0.224 |
| Secondary school | 37 (7.7%) | 48 (10%) | 39 (8.1%) | |
| Certificate/Diploma | 13 (2.7%) | 21 (4.4%) | 22 (4.6%) | |
| Undergraduate degree | 63 (13.1%) | 50 (10.4%) | 57 (11.9%) | |
| Postgraduate education | 34 (7.1%) | 14 (2.9%) | 26 (5.5%) | |
| Income | ||||
| Under PKR 10,000 | 4 (0.8%) | 4 (0.8%) | 7 (1.5%) | 0.578 |
| PKR 10,000 to 20,000 | 11 (2.3%) | 12 (2.5%) | 15 (3.1%) | |
| Over PKR 20,000 | 149 (31.1%) | 140 (29.2%) | 138 (28.7%) | |
| Occupation | ||||
| Professional | 43 (9%) | 23 (4.8%) | 28 (5.8%) | 0.001 ** |
| Skilled labor | 3 (0.6%) | 13 (2.7%) | 5 (1%) | |
| Manual labor | 3 (0.6%) | 9 (1.9%) | 7 (1.5%) | |
| Administrative | 23 (4.8%) | 27 (5.6%) | 26 (5.4%) | |
| Self-employed | 55 (11.9%) | 53 (11%) | 35 (7.3%) | |
| Home duties | 29 (6%) | 27 (5.6%) | 37 (7.7%) | |
| Unemployed | 3 (0.6%) | 4 (0.8%) | 16 (3.3%) | |
| Pensioner | 5 (1%) | Nil | 6 (1.3%) | |
| Children | ||||
| Yes | 118 (24.5%) | 122 (25.4%) | 93 (19.4%) | 0.001 *** |
| No | 46 (9.6%) | 34 (7.1%) | 67 (14%) | |
| Insurance | ||||
| Yes | 7 (1.5%) | 15 (3.1%) | 7 (1.5%) | 0.686 |
| No | 145 (30.2%) | 144 (30%) | 145 (30.2%) | |
| Not sure | 4 (0.8%) | 5 (1%) | 8 (1.7%) | |
| Questions | Frequency (n) | Percentage (%) |
|---|---|---|
| Q. When do you think you should stop taking antibiotics once you have begun treatment? | ||
| When I feel better | 207 | 43.1% |
| When I have taken all the antibiotics as directed | 200 | 41.7% |
| Do not know/Unsure of the answer | 73 | 15.2% |
| Q. It is okay to use antibiotics that were given to you by a friend or family member if they were used to treat the same illness? | ||
| Yes | 198 | 41.3% |
| No | 168 | 35.0% |
| Do not know | 114 | 23.7% |
| Q. It is okay to buy the same antibiotics, or request the same antibiotics from a doctor if I am sick, and they helped me get better when I had the same symptoms before? | ||
| Yes | 256 | 53.3% |
| No | 120 | 25.0% |
| Do not know | 104 | 21.7% |
| Q. Do you think that the above mentioned conditions may be treated with antibiotics? (Mark more than one if you deem appropriate) | ||
| HIV/AIDS | 107 | 22.3% |
| Gonorrhea | 137 | 28.5% |
| Bladder infection or UTI | 193 | 40.2% |
| Diarrhea | 171 | 35.6% |
| Cold and Flu | 300 | 62.5% |
| Fever | 325 | 67.7% |
| Malaria | 114 | 23.8% |
| Measles | 97 | 20.2% |
| Skin or wound infection | 148 | 30.8% |
| Sore throat | 242 | 50.4% |
| Body aches | 211 | 44% |
| Headaches | 205 | 42.7% |
| Variable | COR (CI 95%) | p-Value | AOR (CI 95%) | p-value |
|---|---|---|---|---|
| Gender | ||||
| Male | 0.591 (0.375–0.931) | 0.023 * | 0.620 (0.383–1.005) | 0.052 |
| Female | Ref | Ref | ||
| Income | ||||
| Below PKR 10,000 | 0.940 (0.231–3.829) | 0.940 | 1.319 (0.301–5.780) | 0.713 |
| PKR 10,000–20,000 | 0.861 (0.368–2.015) | 0.051 | 2.657 (0.515–3.345) | 0.589 |
| Above PKR 20,000 | Ref | Ref | ||
| Health insurance | ||||
| No | 1.259 (0.331–4.782) | 0.736 | 1.174 (0.299–4.616) | 0.818 |
| Yes | 2.679 (0.545–13.157) | 0.025 * | 2.657 (0.515–13.696) | 0.243 |
| Not sure | Ref | Ref | ||
| Age | ||||
| 21–25 years | 0.895 (0352–2.271) | 0.815 | 0.552 (0.207–1.472) | 0.235 |
| 26–30 years | 0.794 (0.420–1.498) | 0.794 | 0.555 (0.281–1.096) | 0.090 |
| 31–40 years | 0.645 (0.381–1.090) | 0.050 | 0.550 (0.317–0.953) | 0.033 * |
| Above 40 years | Ref | Ref | Ref | Ref |
| Education | ||||
| Primary school | 0.304 (0.126–0.736) | 0.008 | 0.271 (0.101–0.730) | 0.010 * |
| Secondary school | 0.317 (0.149–0.676) | 0.003 | 0.325 (0.470.719) | 0.005 ** |
| Certificate/Diploma | 0.255 (0.101–0.646) | 0.004 | 0.250 (0.961–0.649) | 0.004 ** |
| Undergraduate degree | 0.519 (0.251–1.071) | 0.076 | 0.521 (0.250–1.087) | 0.082 |
| Postgraduate education | Ref | Ref | ||
| Demographic Characteristics | Statement Do You Intend to Self-Medicate again if the Same Symptoms Appear in the Future? | p-Value | ||
|---|---|---|---|---|
| Yes | No | Not Sure | ||
| Gender | ||||
| Male | 138 (28.7%) | 57 (11.9%) | 72 (15%) | 0.001 *** |
| Female | 63 (13.1%) | 69 (14.4%) | 81 (16.9%) | |
| Income | ||||
| Under PKR 10,000 | 9 (1.9%) | 2 (0.4%) | 4 (0.8%) | 0.001 *** |
| PKR 10,000 to 20,000 | 26 (5.4% | 9 (1.9%) | 3 (0.6%) | |
| Over PKR 20,000 | 166 (34.6%) | 115 (24%) | 146 (30.4%) | |
| Occupation | ||||
| Professional | 28 (5.8%) | 26 (5.4%) | 40 (8.3%) | 0.003 ** |
| Skilled labor | 12 (2.5%) | 5 (1%) | 4 (0.8%) | |
| Manual labor | 13 (2.7%) | 5 (1%) | 1 (0.2%) | |
| Administrative | 28 (5.8%) | 26 (5.4%) | 22 (4.6%) | |
| Self-employed | 67 (14%) | 30 (6.3%) | 46 (9.6%) | |
| Home duties | 35 (7.3%) | 24 (5%) | 34 (7.1%) | |
| Unemployed | 12 (2.5%) | 8 (1.7%) | 3 (0.6%) | |
| Pensioner | 6 (1.4%) | 2 (0.4%) | 3 (0.6%) | |
| How do you evaluate your symptoms after taking antibiotics? | ||||
| Better | Worse | Same as before | ||
| 350 (72.9%) | 22 (4.6%) | 108 (22.5%) | ||
| What do you think about practicing SMA to take care of your health? | ||||
| Good practice | Acceptable practice | Not acceptable practice | ||
| 92 (19.2%) | 220 (45.8%) | 168 (35%) | ||
| Do you feel that treating your symptoms with antibiotics proves to be economical? | ||||
| Yes, it’s economical | I cannot say | Not sure | Don’t know at all | |
| 184 (38.3%) | 130 (27.1%) | 88 (18.3%) | 78 (16.3%) | |
| On average, how much money (PKR) did you save one time when you self-medicate with antibiotics? | ||||
| Under PKR 500 | PKR 600 to 1000 | PKR 1000 to 1500 | Above PKR 1500 | I cannot say |
| 98 (20.4%) | 107 (22.3%) | 70 (14.6%) | 52 (10.9%) | 153 (31.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslam, A.; Zin, C.S.; Jamshed, S.; Rahman, N.S.A.; Ahmed, S.I.; Pallós, P.; Gajdács, M. Self-Medication with Antibiotics: Prevalence, Practices and Related Factors among the Pakistani Public. Antibiotics 2022, 11, 795. https://doi.org/10.3390/antibiotics11060795
Aslam A, Zin CS, Jamshed S, Rahman NSA, Ahmed SI, Pallós P, Gajdács M. Self-Medication with Antibiotics: Prevalence, Practices and Related Factors among the Pakistani Public. Antibiotics. 2022; 11(6):795. https://doi.org/10.3390/antibiotics11060795
Chicago/Turabian StyleAslam, Adeel, Che Suraya Zin, Shazia Jamshed, Norny Syafinaz Ab Rahman, Syed Imran Ahmed, Péter Pallós, and Márió Gajdács. 2022. "Self-Medication with Antibiotics: Prevalence, Practices and Related Factors among the Pakistani Public" Antibiotics 11, no. 6: 795. https://doi.org/10.3390/antibiotics11060795