
Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods

 , , ,
, , ,
Abstract
:1. The Emergence of Antimicrobial Resistance and Overlooked Pandemic
2. The Rationale for Performing Susceptibility Testing
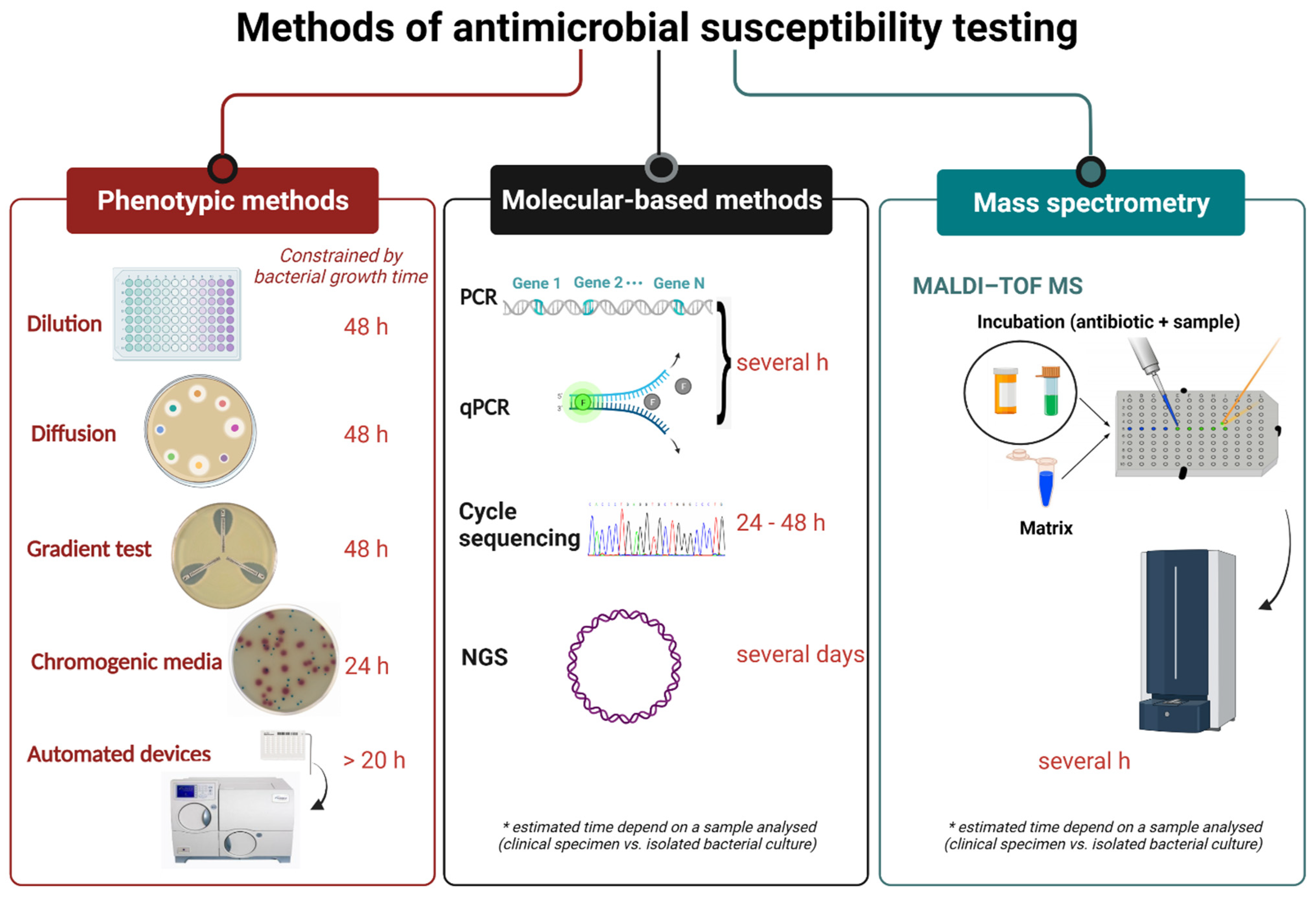
3. Commonly Used Techniques
3.1. Classical Methods
3.1.1. Dilution Methods: Broth Dilution and Agar Dilution
3.1.2. Antimicrobial Gradient Method
3.1.3. Disk Diffusion Test
3.1.4. Chromogenic Agar Media for Detection of Antimicrobial-Resistant Bacteria
3.1.5. Colourimetric Tests for Detection of Antimicrobial-Resistant Bacteria
4. Current Technologies for Rapid AST
4.1. Automated and Semi-Automated Devices Based on Microdilution Susceptibility Testing
- VITEK 2 Systems—The first generation of VITEK system with a turnaround time of 13 h was developed for enumeration and identification of bacteria and yeasts in 1973. The VITEK 2 System, the next-generation of an instrument, is a BMD-based AST system that uses 64-well plastic cards containing 17–20 antimicrobial agents. If the bacterial isolate is not previously identified, one card is used for bacterial identification (ID card) and the other for antimicrobial susceptibility testing (AST card). Two Vitek 2 instruments are available with test card (ID and AST) capacities of 60 cards (Vitek 2) and 120 cards (Vitek 2 XL). Results are reported in 4–18 h, containing MIC and category of susceptibility, whereas the detection of AMR is facilitated by the Advanced Expert System (AES). The currently available Vitek 2 Compact instruments can use 15, 30, and 60 cards. The main advantage of the Vitek 2 system with computer software is the determination of susceptibility of clinically important resistant pathogens, such as Staphylococcus aureus and Enterococcus faecalis, to an additional four to ten antibiotics [86,89,90].
- Phoenix System—The Phoenix System is widely accepted and used in clinical microbiology laboratories for identification testing (ID) and antimicrobial susceptibility testing (AST). The principle of determining the susceptibility is based on the use of an oxidation-reduction indicator (resazurin dye or Alamar blue) and the detection of bacterial growth in the presence of various concentrations of the antimicrobial agent. In the Phoenix instrument, a maximum of 100 tests can be performed by using Phoenix ID/AST combination panels (51 for ID and 85 for AST). The instrument performs automatic reading at 20 min intervals during incubation for up to 18 h and provides accurate and rapid susceptibility results with easy workflow for the laboratory worker. In 2014, the new panel for susceptibility of Gram-negative bacteria was introduced for the Phoenix system to be used in combination with the BD Bruker MALDI-TOF [91].
- MicroScan WalkAway plus System—The MicroScan WalkAway plus System provides accurate and rapid identification and susceptibility results for a wide range of Gram-positive and Gram-negative aerobic bacteria. The instrument utilises three types of panel configurations: combo panels, breakpoint combo panels, and MIC panels. There are two types of system: 40- and 96-panel capacity models. The panels are manually inoculated, rehydrated by the RENOK inoculator, and read automatically. The results are obtained after 4.5–18 h by reading of rapid panels [91].
- MicroScan AutoScan 4—The AutoScan 4 is a semiautomated instrument mostly used in smaller laboratories or for the testing of supplemental antimicrobial agents. The instrument provides simplified ID/AST testing in a highly reliable and affordable package. The system uses the off-line incubation of the conventional MicroScan AST panels. The panels are manually inoculated or with the MicroScan Renok instrument and read automatically [91].
- MicroScan WalkAway System—The first generation of the MicroScan WalkAway System available on the market is the AutoSCAN-3. The new versions of instruments Auto-ACAN-4 and AutoSCAN-WalkAway are improved and use dry panels that do not need refrigeration. The AutoSCAN-WalkAway system detects bacterial enzymatic activity and can process 96 panels at the same [86].
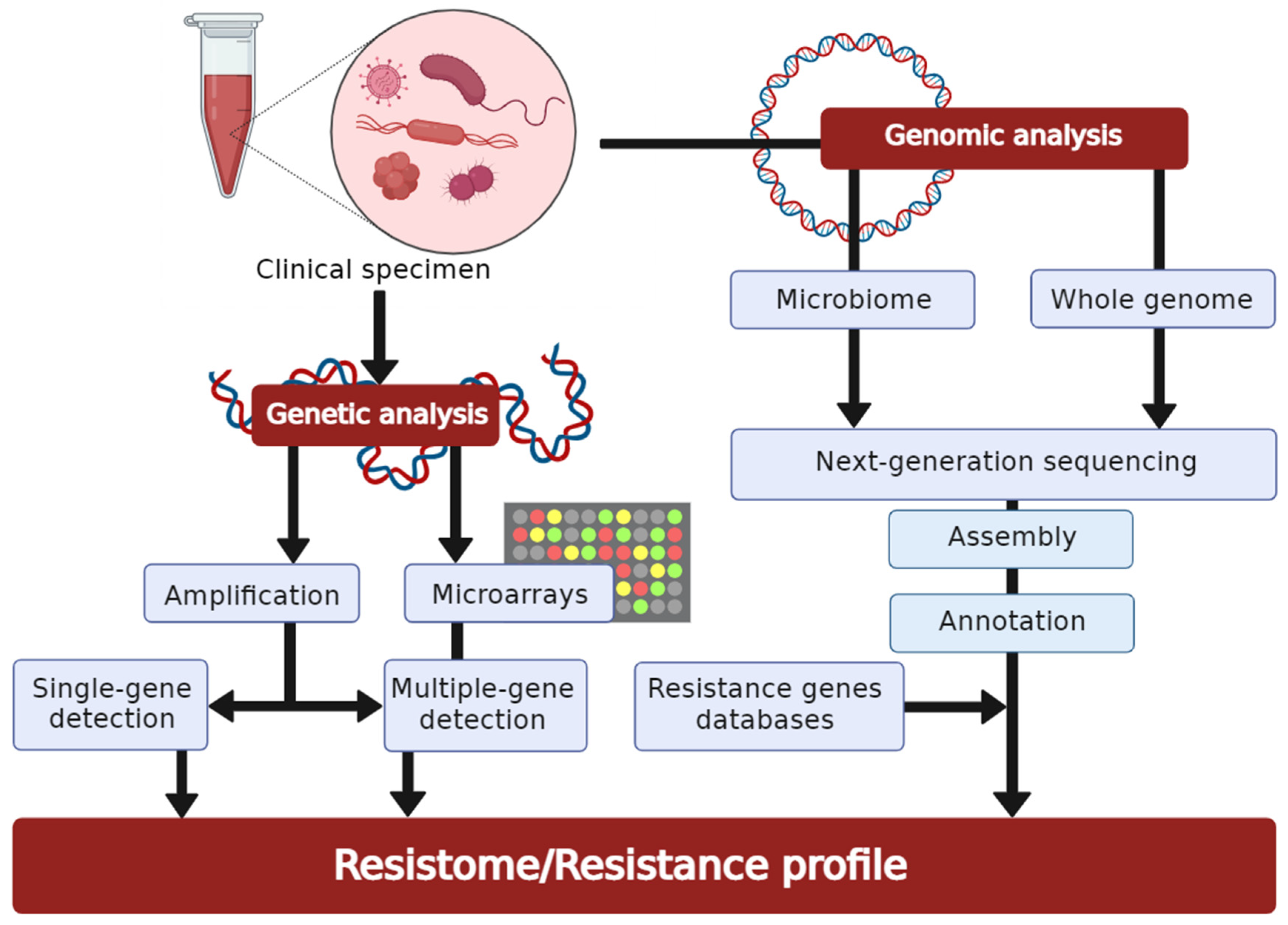
4.2. Molecular-Based Techniques for Resistance Detection
4.2.1. Polymerase Chain Reaction
4.2.2. DNA-Microarrays
4.2.3. Whole-Genome Sequencing in Antimicrobial Susceptibility Testing
4.3. Mass Spectrometry
5. Selection of Antimicrobial Drugs for Susceptibility Testing, Interpretation, and Reporting
6. Quality Assurance in Antimicrobial Susceptibility Testing
7. Near-Future Perspectives for Antimicrobial Susceptibility Testing
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J.V. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- WHO. Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 23 February 2022).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- WHO. New Report Calls for Urgent Action to Avert Antimicrobial Resistance Crisis. Available online: https://www.who.int/news/item/29-04-2019-new-report-calls-for-urgent-action-to-avert-antimicrobial-resistance-crisis (accessed on 23 February 2022).
- Mirzaei, R.; Goodarzi, P.; Asadi, M.; Soltani, A.; Aljanabi, H.A.A.; Jeda, A.S.; Dashtbin, S.; Jalalifar, S.; Mohammadzadeh, R.; Teimoori, A.; et al. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020, 72, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Tomczyk, S.; Taylor, A.; Brown, A.; de Kraker, M.E.A.; El-Saed, A.; Alshamrani, M.; Hendriksen, R.S.; Jacob, M.; Löfmark, S.; Perovic, O.; et al. Impact of the COVID-19 pandemic on the surveillance, prevention and control of antimicrobial resistance: A global survey. J. Antimicrob. Chemother. 2021, 76, 3045–3058. [Google Scholar] [CrossRef] [PubMed]
- Bengoechea, J.A.; Bamford, C.G. SARS-CoV-2, bacterial co-infections, and AMR: The deadly trio in COVID-19? EMBO Mol. Med. 2020, 12, e12560. [Google Scholar] [CrossRef] [PubMed]
- By 2050, Drug-Resistant Infections Could Cause Global Economic Damage on Par with 2008 Financial Crisis. Available online: https://www.worldbank.org/en/news/press-release/2016/09/18/by-2050-drug-resistant-infections-could-cause-global-economic-damage-on-par-with-2008-financial-crisis (accessed on 23 February 2022).
- Zhu, Y.; Huang, W.E.; Yang, Q. Clinical perspective of antimicrobial resistance in bacteria. Infect. Drug Resist. 2022, 15, 735–746. [Google Scholar] [CrossRef]
- Munita, J.M.; Arias, C.A. Mechanisms of antibiotic resistance. Microbiol. Spectr. 2016, 4, 464–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacconelli, E. Antimicrobial use: Risk driver of multidrug resistant microorganisms in healthcare settings. Curr. Opin. Infect. Dis. 2009, 22, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; Macdougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Executive Summary: Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Van Belkum, A.; Bachmann, T.T.; Lüdke, G.; Lisby, J.G.; Kahlmeter, G.; Mohess, A.; Becker, K.; Hays, J.P.; Woodford, N.; Mitsakakis, K.; et al. Developmental roadmap for antimicrobial susceptibility testing systems. Nat. Rev. Microbiol. 2018, 17, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Tebano, G.; Mouelhi, Y.; Zanichelli, V.; Charmillon, A.; Fougnot, S.; Lozniewski, A.; Thilly, N.; Pulcini, C. Selective reporting of antibiotic susceptibility testing results: A promising antibiotic stewardship tool. Expert Rev. Anti. Infect. Ther. 2020, 18, 251–262. [Google Scholar] [CrossRef] [PubMed]
- WHO. Monitoring and Evaluation of the Global Action Plan on Antimicrobial Resistance: Framework and Recommended Indicators. Available online: https://apps.who.int/iris/handle/10665/325006 (accessed on 23 February 2022).
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrob. Resist. Infect. Control 2021, 10, 63. [Google Scholar] [CrossRef]
- WHO. Antimicrobial Stewardship Interventions: A Practical Guide; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Klinker, K.P.; Hidayat, L.K.; DeRyke, C.A.; DePestel, D.D.; Motyl, M.; Bauer, K.A. Antimicrobial stewardship and antibiograms: Importance of moving beyond traditional antibiograms. Ther. Adv. Infect. Dis. 2021, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hebert, C.; Ridgway, J.; Vekhter, B.; Brown, E.C.; Weber, S.G.; Robicsek, A. Demonstration of the weighted-incidence syndromic combination antibiogram: An empiric prescribing decision Aid. Infect. Control Hosp. Epidemiol. 2012, 33, 381–388. [Google Scholar] [CrossRef]
- Khalili, H.; Izadpanah, M. Antibiotic regimens for treatment of infections due to multidrug-resistant Gram-negative pathogens: An evidence-based literature review. J. Res. Pharm. Pract. 2015, 4, 105. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standard Institute. M39-A4: Analysis and Presentation of Cumulative Antimicrobial Susceptibility Test Data: Approved Guideline, 4th ed.; Clinical and Laboratory Standard Institute: Wayne, PA, USA, 2014; ISBN 610.688.0700. [Google Scholar]
- Puzniak, L.; DePestel, D.D.; Srinivasan, A.; Ye, G.; Murray, J.; Merchant, S.; Andrew DeRyke, C.; Gupta, V. A combination antibiogram evaluation for Pseudomonas aeruginosa in respiratory and blood sources from intensive care unit (ICU) and Non-ICU Settings in U.S. Hospitals. Antimicrob. Agents Chemother. 2019, 63, e02564-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, Z.A.; Siddiqui, M.F.; Park, S. Current and emerging methods of antibiotic susceptibility testing. Diagnostics 2019, 9, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syal, K.; Mo, M.; Yu, H.; Iriya, R.; Jing, W.; Guodong, S.; Wang, S.; Grys, T.E.; Haydel, S.E.; Tao, N. Current and emerging techniques for antibiotic susceptibility tests. Theranostics 2017, 7, 1795–1805. [Google Scholar] [CrossRef]
- Jenkins, S.G.; Schuetz, A.N. Current concepts in laboratory testing to guide antimicrobial therapy. Mayo Clin. Proc. 2012, 87, 290–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, D.C.; Paton, T.F.; Mulroney, K.T.; Inglis, T.J.J.; Sutton, J.M.; Morgan, H. A fast impedance-based antimicrobial susceptibility test. Nat. Commun. 2020, 11, 5328. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. M07: Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically, 11th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; ISBN 1562388363. [Google Scholar]
- Golus, J.; Sawicki, R.; Widelski, J.; Ginalska, G. The agar microdilution method—A new method for antimicrobial susceptibility testing for essential oils and plant extracts. J. Appl. Microbiol. 2016, 121, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Vasilijević, B.; Mitić-Ćulafić, D.; Djekic, I.; Marković, T.; Knežević-Vukčević, J.; Tomasevic, I.; Velebit, B.; Nikolić, B. Antibacterial effect of Juniperus communis and Satureja montana essential oils against Listeria monocytogenes in vitro and in wine marinated beef. Food Control 2019, 100, 247–256. [Google Scholar] [CrossRef]
- Kowalska-Krochmal, B.; Dudek-Wicher, R. The minimum inhibitory concentration of antibiotics: Methods, interpretation, clinical relevance. Pathogens 2021, 10, 165. [Google Scholar] [CrossRef] [PubMed]
- Balouiri, M.; Sadiki, M.; Ibnsouda, S.K. Methods for in vitro evaluating antimicrobial activity: A review. J. Pharm. Anal. 2016, 6, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferro, B.E.; Van Ingen, J.; Wattenberg, M.; Van Soolingen, D.; Mouton, J.W. Time-kill kinetics of antibiotics active against rapidly growing mycobacteria. J. Antimicrob. Chemother. 2015, 70, 811–817. [Google Scholar] [CrossRef] [Green Version]
- Mueller, M.; De La Peña, A.; Derendorf, H. Issues in pharmacokinetics and pharmacodynamics of anti-infective agents: Kill curves versus MIC. Antimicrob. Agents Chemother. 2004, 48, 369–377. [Google Scholar] [CrossRef] [Green Version]
- Olajuyigbe, O.O.; Afolayan, A.J. In vitro antibacterial and time-kill evaluation of the Erythrina caffra Thunb. extract against bacteria associated with diarrhoea. Sci. World J. 2012, 2012, 738314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorgensen, J.H.; Ferraro, M.J. Antimicrobial susceptibility testing: A review of general principles and contemporary practices. Clin. Infect. Dis. 2009, 49, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Nikolić, B.; Vasilijević, B.; Mitić-Ćulafić, D.; Lesjak, M.; Vuković-Gačić, B.; Dukić, N.M.; Knežević-Vukčević, J. Screening of the antibacterial effect of Juniperus sibirica and Juniperus sabina essential oils in a microtitre plate-based MIC assay. Bot. Serb. 2016, 40, 43–48. [Google Scholar] [CrossRef]
- Foerster, S.; Desilvestro, V.; Hathaway, L.J.; Althaus, C.L.; Unemo, M. A new rapid resazurin-based microdilution assay for antimicrobial susceptibility testing of Neisseria gonorrhoeae. J. Antimicrob. Chemother. 2017, 72, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Galani, I.; Adamou, P.; Karaiskos, I.; Giamarellou, H.; Souli, M. Evaluation of ComASPTM Colistin (formerly SensiTestTM Colistin), a commercial broth microdilution-based method to evaluate the colistin minimum inhibitory concentration for carbapenem-resistant Klebsiella pneumoniae isolates. J. Glob. Antimicrob. Resist. 2018, 15, 123–126. [Google Scholar] [CrossRef]
- Wiegand, I.; Hilpert, K.; Hancock, R.E.W. Agar and broth dilution methods to determine the minimal inhibitory concentration (MIC) of antimicrobial substances. Nat. Protoc. 2008, 3, 163–175. [Google Scholar] [CrossRef]
- Mirajkar, C.J.; Gebhart, C.J. Comparison of agar dilution and antibiotic gradient strip test with broth microdilution for susceptibility testing of swine Brachyspira species. J. Vet. Diagn. Investig. 2016, 28, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 12.0. Available online: http://www.eucast.org/clinical_breakpoints/ (accessed on 23 February 2022).
- Shields, R.K.; Clancy, C.J.; Pasculle, A.W.; Press, E.G.; Haidar, G.; Hao, B.; Chen, L.; Kreiswirth, B.N.; Nguyen, M.H. Verification of Ceftazidime-Avibactam and Ceftolozane-Tazobactam Susceptibility Testing Methods against Carbapenem-Resistant Enterobacteriaceae and Pseudomonas aeruginosa. J. Clin. Microbiol. 2018, 56, e01093-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphries, R.M.; Hindler, J.A.; Magnano, P.; Wong-Beringer, A.; Tibbetts, R.; Miller, S.A. Performance of ceftolozane-tazobactam etest, MIC test strips, and disk diffusion compared to reference broth microdilution for-Lactam-Resistant Pseudomonas aeruginosa isolates. J. Clin. Microbiol. 2018, 56, e01633-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajic, I.; Ranin, L.; Kekic, D.; Opavski, N.; Smitran, A.; Mijac, V.; Jovanovic, S.; Hadnadjev, M.; Travar, M.; Mijovic, G. Tigecycline susceptibility of multidrug-resistant Acinetobacter baumannii from intensive care units in the western Balkans. Acta Microbiol. Immunol. Hung. 2020, 67, 176–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satlina, M.J. The search for a practical method for colistin susceptibility testing: Have we found it by going back to the future? J. Clin. Microbiol. 2018, 57, e01608-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jönsson, A.; Jacobsson, S.; Foerster, S.; Cole, M.J.; Unemo, M. Performance characteristics of newer MIC gradient strip tests compared with the Etest for antimicrobial susceptibility testing of Neisseria gonorrhoeae. APMIS 2018, 126, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Miftahussurur, M.; Fauzia, K.A.; Nusi, I.A.; Setiawan, P.B.; Syam, A.F.; Waskito, L.A.; Doohan, D.; Ratnasari, N.; Khomsan, A.; Adnyana, I.K.; et al. E-test versus agar dilution for antibiotic susceptibility testing of Helicobacter pylori: A comparison study. BMC Res. Notes 2020, 13, 22. [Google Scholar] [CrossRef]
- Akcali, S.; Cicek, C.; Surucuoglu, S.; Ozbakkaloglu, B. E-Test: An Alternative Method for Susceptibility Testing of Mycobacterium tuberculosis. Med. Princ. Pract. 2005, 14, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Dannaoui, E.; Espinel-Ingroff, A. Antifungal Susceptibly Testing by Concentration Gradient Strip Etest Method for Fungal Isolates: A Review. J. Fungi 2019, 5, 108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereckaite, L.; Tatarunas, V.; Giedraitiene, A. Current antimicrobial susceptibility testing for beta-lactamase-producing Enterobacteriaceae in clinical settings. J. Microbiol. Methods 2018, 152, 154–164. [Google Scholar] [CrossRef] [PubMed]
- Garrec, H.; Drieux-Rouzet, L.; Golmard, J.L.; Jarlier, V.; Robert, J. Comparison of nine phenotypic methods for detection of extended-spectrum β-lactamase production by Enterobacteriaceae. J. Clin. Microbiol. 2011, 49, 1048–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzel, M.; Afsar, Y.; Akdogan, D.; Moncheva, P.; Hristova, P.; Erdem, G. Evaluation of metallo-beta-lactamase production in multiple antibiotic-resistant Pseudomonas spp. and Acinetobacter baumannii strains. Biotechnol. Biotechnol. Equip. 2018, 32, 1285–1290. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Martinez, L.; Cantón Spain, R.; Stefani, S.; Skov, R.; Glupczynski, Y.; Nordmann, P.; Wootton, M.; Miriagou, V.; Skov Simonsen, G.; Zemlickova, H.; et al. EUCAST Guidelines for Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Resistance_mechanisms/EUCAST_detection_of_resistance_mechanisms_170711.pdf (accessed on 27 February 2022).
- Peter-Getzlaff, S.; Polsfuss, S.; Poledica, M.; Hombach, M.; Giger, J.; Böttger, E.C.; Zbinden, R.; Bloemberg, G.V. Detection of AmpC beta-lactamase in Escherichia coli: Comparison of three phenotypic confirmation assays and genetic analysis. J. Clin. Microbiol. 2011, 49, 2924–2932. [Google Scholar] [CrossRef] [Green Version]
- Yusof, A.; Engelhardt, A.; Karlsson, A.; Bylund, L.; Vidh, P.; Mills, K.; Wootton, M.; Walsh, T.R. Evaluation of a new etest vancomycin-teicoplanin strip for detection of glycopeptide-intermediate Staphylococcus aureus (GISA), in particular, heterogeneous GISA. J. Clin. Microbiol. 2008, 46, 3042–3047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heatley, N.G. A method for the assay of penicillin. Biochem. J. 1944, 38, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute. M02: Performance Standards for Antimicrobial Disk Susceptibility Tests, 13th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018; ISBN 1562387863. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Routine and Extended Internal Quality Control for MIC Determination and Disk Diffusion as Recommended by EUCAST, Version 12.0. Available online: http://www.eucast.org/ast_of_bacteria/quality_control/ (accessed on 23 February 2022).
- Le Page, S.; Dubourg, G.; Rolain, J.-M. Evaluation of the Scan® 1200 as a rapid tool for reading antibiotic susceptibility testing by the disc diffusion technique. J. Antimicrob. Chemother. 2016, 71, 3424–3431. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. M100: Performance Standards for Antimicrobial Susceptibility Testing, 32nd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2022; ISBN 9781684400331. [Google Scholar]
- Hombach, M.; Zbinden, R.; Böttger, E.C. Standardisation of disk diffusion results for antibiotic susceptibility testing using the sirscan automated zone reader. BMC Microbiol. 2013, 13, 225. [Google Scholar] [CrossRef] [Green Version]
- Idelevich, E.A.; Hoy, M.; Görlich, D.; Knaack, D.; Grünastel, B.; Peters, G.; Borowski, M.; Becker, K. Rapid phenotypic detection of microbial resistance in gram-positive bacteria by a real-time laser scattering method. Front. Microbiol. 2017, 8, 1064. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, J.H.; Barry, A.L.; Traczewski, M.M.; Sahm, D.F.; McElmeel, M.L.; Crawford, S.A. Rapid automated antimicrobial susceptibility testing of Streptococcus pneumoniae by use of the bioMerieux VITEK 2. J. Clin. Microbiol. 2000, 38, 2814–2818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coyle, M.B.; McGonagle, L.A.; Plorde, J.J.; Clausen, C.R.; Schoenknecht, F.D. Rapid antimicrobial susceptibility testing of isolates from blood cultures by direct inoculation and early reading of disk diffusion tests. J. Clin. Microbiol. 1984, 20, 473–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberman, D.F.; Robertson, R.G. Evaluation of a rapid Bauer-Kirby antibiotic susceptibility determination. Antimicrob. Agents Chemother. 1975, 7, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Van den Bijllaardt, W.; Buiting, A.G.; Mouton, J.W.; Muller, A.E. Shortening the incubation time for antimicrobial susceptibility testing by disk diffusion for Enterobacteriaceae: How short can it be and are the results accurate? Int. J. Antimicrob. Agents 2017, 49, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Hombach, M.; Jetter, M.; Blöchliger, N.; Kolesnik-Goldmann, N.; Böttger, E.C. Fully automated disc diffusion for rapid antibiotic susceptibility test results: A proof-of-principle study. J. Antimicrob. Chemother. 2017, 72, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Jonasson, E.; Matuschek, E.; Kahlmeter, G. The EUCAST rapid disc diffusion method for antimicrobial susceptibility testing directly from positive blood culture bottles. J. Antimicrob. Chemother. 2020, 75, 968–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Zone Diameter Breakpoints for Rapid Antimicrobial Susceptibility Testing (RAST) Directly from Blood Culture Bottles, Version 4.0. Available online: http://www.eucast.org/rapid_ast_in_blood_cultures/breakpoints_for_short_incubation/ (accessed on 23 February 2022).
- The European Committee on Antimicrobial Susceptibility Testing. Screening for ESBL and Carbapenemases in E. coli and K. pneumoniae for Epidemiological Purposes as Part of the RAST Procedure. EUCAST Guidelines for Detection of Resistance Mechanisms and Specific Resistance of Clinical and/or Epidemiological Importance. Available online: http://www.eucast.org/resistance_mechanisms/ (accessed on 23 February 2022).
- Idelevich, E.A.; Schüle, I.; Grünastel, B.; Wüllenweber, J.; Peters, G.; Becker, K. Rapid identification of microorganisms from positive blood cultures by MALDI-TOF mass spectrometry subsequent to very short-term incubation on solid medium. Clin. Microbiol. Infect. 2014, 20, 1001–1006. [Google Scholar] [CrossRef] [Green Version]
- Savage, T.J.; Rao, S.; Joerger, J.; Ozonoff, A.; McAdam, A.J.; Sandora, T.J. Predictive value of direct disk diffusion testing from positive blood cultures in a children’s hospital and its utility in antimicrobial stewardship. J. Clin. Microbiol. 2021, 59, e02445-20. [Google Scholar] [CrossRef]
- Ahman, J.; Matuschek, E.; Kahlmeter, G. The quality of antimicrobial discs from nine manufacturers-EUCAST evaluations in 2014 and 2017. Clin. Microbiol. Infect. 2019, 25, 346–352. [Google Scholar] [CrossRef] [Green Version]
- Aubry, B.; Lemarié, C.; Chenouard, R.; Kempf, M.; Eveillard, M.; Pailhoriès, H. Performance of penicillinase detection tests in Staphylococcus epidermidis: Comparison of different phenotypic methods. BMC Microbiol. 2020, 20, 240. [Google Scholar] [CrossRef]
- Merlino, J.; Leroi, M.; Bradbury, R.; Veal, D.; Harbour, C. New chromogenic identification and detection of Staphylococcus aureus and methicillin-resistant S. aureus. J. Clin. Microbiol. 2000, 38, 2378–2380. [Google Scholar] [CrossRef] [PubMed]
- Ledeboer, N.A.; Das, K.; Eveland, M.; Roger-Dalbert, C.; Mailler, S.; Chatellier, S.; Dunne, W.M. Evaluation of a novel chromogenic agar medium for isolation and differentiation of vancomycin-resistant Enterococcus faecium and Enterococcus faecalis isolates. J. Clin. Microbiol. 2007, 45, 1556–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glupczynski, Y.; Berhin, C.; Bauraing, C.; Bogaerts, P. Evaluation of a New Selective Chromogenic Agar Medium for Detection of Extended-Spectrum-Lactamase-Producing Enterobacteriaceae. J. Clin. Microbiol. 2007, 45, 501–505. [Google Scholar] [CrossRef] [Green Version]
- Samra, Z.; Bahar, J.; Madar-Shapiro, L.; Aziz, N.; Israel, S.; Bishara, J. Evaluation of CHROMagar KPC for rapid detection of carbapenem-resistant Enterobacteriaceae. J. Clin. Microbiol. 2008, 46, 3110–3111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, N.C.; Wareham, D.W. Evaluation of CHROMagar Acinetobacter for detection of enteric carriage of multidrug-resistant Acinetobacter baumannii in samples from critically ill patients. J. Clin. Microbiol. 2009, 47, 2249–2251. [Google Scholar] [CrossRef] [Green Version]
- Perry, J.D. A decade of development of chromogenic culture media for clinical microbiology in an era of molecular diagnostics. Clin. Microbiol. Rev. 2017, 30, 449–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kekic, D.; Gajic, I.; Opavski, N.; Kojic, M.; Vukotic, G.; Smitran, A.; Boskovic, L.; Stojkovic, M.; Ranin, L. Trends in molecular characteristics and antimicrobial resistance of group B streptococci: A multicenter study in Serbia, 2015–2020. Sci. Rep. 2021, 11, 540. [Google Scholar] [CrossRef] [PubMed]
- Tierney, D.; Copsey, S.D.; Morris, T.; Perry, J.D. A new chromogenic medium for isolation of Bacteroides fragilis suitable for screening for strains with antimicrobial resistance. Anaerobe 2016, 39, 168–172. [Google Scholar] [CrossRef]
- Abdul Momin, M.H.F.; Bean, D.C.; Hendriksen, R.S.; Haenni, M.; Phee, L.M.; Wareham, D.W. CHROMagar COL-APSE: A selective bacterial culture medium for the isolation and differentiation of colistin-resistant Gram-negative pathogens. J. Med. Microbiol. 2017, 66, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Poirel, L.; Dortet, L. Rapid Detection of Carbapenemase-producing Enterobacteriaceae. Emerg. Infect. Dis. 2012, 18, 1503. [Google Scholar] [CrossRef] [Green Version]
- Benkova, M.; Soukup, O.; Marek, J. Antimicrobial susceptibility testing: Currently used methods and devices and the near future in clinical practice. J. Appl. Microbiol. 2020, 129, 806–822. [Google Scholar] [CrossRef]
- Sader, H.S.; Fritsche, T.R.; Jones, R.N. Accuracy of three automated systems (MicroScan WalkAway, VITEK, and VITEK 2) for susceptibility testing of Pseudomonas aeruginosa against five broad-spectrum beta-lactam agents. J. Clin. Microbiol. 2006, 44, 1101–1104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fredborg, M.; Andersen, K.R.; Jørgensen, E.; Droce, A.; Olesen, T.; Jensen, B.B.; Rosenvinge, F.S.; Sondergaard, T.E. Real-time optical antimicrobial susceptibility testing. J. Clin. Microbiol. 2013, 51, 2047–2053. [Google Scholar] [CrossRef] [Green Version]
- Ligozzi, M.; Bernini, C.; Bonora, M.G.; De Fatima, M.; Zuliani, J.; Fontana, R. Evaluation of the VITEK 2 system for identification and antimicrobial susceptibility testing of medically relevant gram-positive cocci. J. Clin. Microbiol. 2002, 40, 1681–1686. [Google Scholar] [CrossRef] [Green Version]
- Spanu, T.; Sanguinetti, M.; Ciccaglione, D.; D’Inzeo, T.; Romano, L.; Leone, F.; Fadda, G. Use of the VITEK 2 System for rapid identification of clinical isolates of Staphylococci from bloodstream infections. J. Clin. Microbiol. 2003, 41, 4259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evangelista, A.T.; Karlowsky, J.A. Automated and Manual Systems for Antimicrobial Susceptibility Testing of Bacteria. In Manual of Commercial Methods in Clinical Microbiology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2016; pp. 414–432. [Google Scholar] [CrossRef]
- Zhou, M.; Wang, Y.; Liu, C.; Kudinha, T.; Liu, X.; Luo, Y.; Yang, Q.; Sun, H.; Hu, J.; Xu, Y.-C. Comparison of five commonly used automated susceptibility testing methods for accuracy in the China Antimicrobial Resistance Surveillance System (CARSS) hospitals. Infect. Drug Resist. 2018, 11, 1347–1358. [Google Scholar] [CrossRef] [Green Version]
- Bulik, C.C.; Fauntleroy, K.A.; Jenkins, S.G.; Abuali, M.; LaBombardi, V.J.; Nicolau, D.P.; Kuti, J.L. Comparison of meropenem MICs and susceptibilities for carbapenemase-producing Klebsiella pneumoniae isolates by various testing methods. J. Clin. Microbiol. 2010, 48, 2402. [Google Scholar] [CrossRef] [Green Version]
- Woodford, N.; Eastaway, A.T.; Ford, M.; Leanord, A.; Keane, C.; Quayle, R.M.; Steer, J.A.; Zhang, J.; Livermore, D.M. Comparison of BD Phoenix, Vitek 2, and MicroScan Automated Systems for detection and inference of mechanisms responsible for carbapenem resistance in Enterobacteriaceae. J. Clin. Microbiol. 2010, 48, 2999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchan, B.W.; Anderson, N.W.; Ledeboer, N.A. Comparison of BD Phoenix and bioMérieux Vitek 2 automated systems for the detection of macrolide-lincosamide-streptogramin B resistance among clinical isolates of Staphylococcus. Diagn. Microbiol. Infect. Dis. 2012, 72, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Richter, S.S.; Howard, W.J.; Weinstein, M.P.; Bruckner, D.A.; Hindler, J.F.; Saubolle, M.; Doern, G.V. Multicenter evaluation of the BD Phoenix Automated Microbiology System for antimicrobial susceptibility testing of Streptococcus species. J. Clin. Microbiol. 2007, 45, 2863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Arias, C.A.; Abbott, A.; Dien Bard, J.; Bhatti, M.M.; Humphries, R.M. Evaluation of the Vitek 2, Phoenix, and MicroScan for antimicrobial susceptibility testing of Stenotrophomonas maltophilia. J. Clin. Microbiol. 2021, 59, e0065421. [Google Scholar] [CrossRef]
- Schumacher, A.; Vranken, T.; Malhotra, A.; Arts, J.J.C.; Habibovic, P. In vitro antimicrobial susceptibility testing methods: Agar dilution to 3D tissue-engineered models. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 187–208. [Google Scholar] [CrossRef] [Green Version]
- Sekyere, J.O.; Asante, J. Emerging mechanisms of antimicrobial resistance in bacteria and fungi: Advances in the era of genomics. Future Microbiol. 2018, 13, 241–262. [Google Scholar] [CrossRef]
- Gajic, I.; Jovicevic, M.; Milic, M.; Kekic, D.; Opavski, N.; Zrnic, Z.; Dacic, S.; Pavlovic, L.; Mijac, V. Clinical and molecular characteristics of OXA-72-producing Acinetobacter baumannii ST636 outbreak at a neonatal intensive care unit in Serbia. J. Hosp. Infect. 2021, 112, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Rocchetti, T.T.; Martins, K.B.; Martins, P.Y.F.; de Oliveira, R.A.; Mondelli, A.L.; Fortaleza, C.M.C.B.; de Lourdes Ribeiro de Souza da Cunha, M. Detection of the mecA gene and identification of Staphylococcus directly from blood culture bottles by multiplex polymerase chain reaction. Braz. J. Infect. Dis. 2018, 22, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Simner, P.; Musser, K.; Mitchell, K.; Wise, M.; Lewis, S.; Yee, R.; Bergman, Y.; Good, C.; Abdelhamed, A.; Li, H.; et al. Multicenter Evaluation of the Acuitas AMR Gene Panel for Detection of an Extended Panel of Antimicrobial Resistance Genes among Bacterial Isolates. J. Clini. Microbiol. 2022, 60, e0209821. [Google Scholar] [CrossRef]
- Findlay, J.; Hopkins, K.L.; Meunier, D.; Woodford, N. Evaluation of three commercial assays for rapid detection of genes encoding clinically relevant carbapenemases in cultured bacteria. J. Antimicrob. Chemother. 2015, 70, 1338–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepheid|Molecular Testing of Healthcare Associated Infections. Available online: https://www.cepheid.com/en_US/tests/Healthcare-Associated-Infections (accessed on 16 March 2022).
- Confirmation-Check-Points Health. Available online: https://check-pointshealth.com/confirmation/ (accessed on 16 March 2022).
- Matsuda, K. PCR-based detection methods for single-nucleotide polymorphism or mutation: Real-time PCR and its substantial contribution toward technological refinement. Adv. Clin. Chem. 2017, 80, 45–72. [Google Scholar] [CrossRef] [PubMed]
- Charnock, C.; Samuelsen, Ø.; Nordlie, A.L.; Hjeltnes, B. Use of a commercially available microarray to characterize antibiotic-resistant clinical isolates of Klebsiella pneumoniae. Curr. Microbiol. 2018, 75, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-S.; Kang, G.-E.; Kim, H.-S.; Kim, H.S.; Song, W.; Lee, K.M. Evaluation of Verigene Blood Culture Test Systems for Rapid Identification of Positive Blood Cultures. Biomed Res. Int. 2016, 2016, 1081536. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, S.A.; Vasoo, S.; Patel, R. Evaluation of the Check-Points Check MDR CT103 and CT103 XL Microarray Kits by Use of Preparatory Rapid Cell Lysis. J. Clin. Microbiol. 2016, 54, 1368–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, A.É.I.; Stuchi, L.P.; Siqueira, N.M.G.; Henrique, J.B.; Vicentini, R.; Ribeiro, M.L.; Darrieux, M.; Ferraz, L.F.C. Selection and validation of reference genes for gene expression studies in Klebsiella pneumoniae using Reverse Transcription Quantitative real-time PCR. Sci. Rep. 2018, 8, 9001. [Google Scholar] [CrossRef] [PubMed]
- Shifman, O.; Steinberger-Levy, I.; Aloni-Grinstein, R.; Gur, D.; Aftalion, M.; Ron, I.; Mamroud, E.; Ber, R.; Rotem, S. A rapid antimicrobial susceptibility test for determining Yersinia pestis susceptibility to doxycycline by RT-PCR quantification of RNA markers. Front. Microbiol. 2019, 10, 754. [Google Scholar] [CrossRef] [Green Version]
- Hendriksen, R.S.; Bortolaia, V.; Tate, H.; Tyson, G.H.; Aarestrup, F.M.; McDermott, P.F. Using genomics to track global antimicrobial resistance. Front. Public Health 2019, 7, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faksri, K.; Kaewprasert, O.; Ong, R.T.H.; Suriyaphol, P.; Prammananan, T.; Teo, Y.Y.; Srilohasin, P.; Chaiprasert, A. Comparisons of whole-genome sequencing and phenotypic drug susceptibility testing for Mycobacterium tuberculosis causing MDR-TB and XDR-TB in Thailand. Int. J. Antimicrob. Agents 2019, 54, 109–116. [Google Scholar] [CrossRef]
- Yang, X.; Hashemi, M.M.; Andini, N.; Li, M.M.; Kuang, S.; Carroll, K.C.; Wang, T.H.; Yang, S. RNA markers for ultra-rapid molecular antimicrobial susceptibility testing in fluoroquinolone-treated Klebsiella pneumoniae. J. Antimicrob. Chemother. 2020, 75, 1747–1755. [Google Scholar] [CrossRef]
- Bhattacharyya, R.P.; Bandyopadhyay, N.; Ma, P.; Son, S.S.; Liu, J.; He, L.L.; Wu, L.; Khafizov, R.; Boykin, R.; Cerqueira, G.C.; et al. Simultaneous detection of genotype and phenotype enables rapid and accurate antibiotic susceptibility determination. Nat. Med. 2019, 25, 1858–1864. [Google Scholar] [CrossRef] [PubMed]
- Rossen, J.W.A.; Friedrich, A.W.; Moran-Gilad, J. Practical issues in implementing whole-genome-sequencing in routine diagnostic microbiology. Clin. Microbiol. Infect. 2018, 24, 355–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellington, M.J.; Ekelund, O.; Aarestrup, F.M.; Canton, R.; Doumith, M.; Giske, C.; Grundman, H.; Hasman, H.; Holden, M.T.G.; Hopkins, K.L.; et al. The role of whole genome sequencing in antimicrobial susceptibility testing of bacteria: Report from the EUCAST Subcommittee. Clin. Microbiol. Infect. 2017, 23, 2–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, Y.P.; Reddy, P.M. Advances in mass spectrometry for the identification of pathogens. Mass. Spectrom. Rev. 2011, 30, 1203–1224. [Google Scholar] [CrossRef]
- Oviaño, M.; de la Luna Ramírez, C.; Barbeyto, L.P.; Bou, G. Rapid direct detection of carbapenemase-producing Enterobacteriaceae in clinical urine samples by MALDI-TOF MS analysis. J. Antimicrob. Chemother. 2017, 72, 1350–1354. [Google Scholar] [CrossRef]
- Oviaño, M.; Rodríguez-Martínez, J.M.; Pascual, Á.; Bou, G. Rapid detection of the plasmid-mediated quinolone resistance determinant AAC(6’)-Ib-cr in Enterobacteriaceae by MALDI-TOF MS analysis. J. Antimicrob. Chemother. 2017, 72, 1074–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camara, J.E.; Hays, F.A. Discrimination between wild-type and ampicillin-resistant Escherichia coli by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Anal. Bioanal. Chem. 2007, 389, 1633–1638. [Google Scholar] [CrossRef] [PubMed]
- Griffin, P.M.; Price, G.R.; Schooneveldt, J.M.; Schlebusch, S.; Tilse, M.H.; Urbanski, T.; Hamilton, B.; Ventera, D. Use of matrix-assisted laser desorption ionization-time of flight mass spectrometry to identify vancomycin-resistant enterococci and investigate the epidemiology of an outbreak. J. Clin. Microbiol. 2012, 50, 2918–2931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sparbier, K.; Lange, C.; Jung, J.; Wieser, A.; Schubert, S.; Kostrzewa, M. MALDI biotyper-based rapid resistance detection by stable-isotope labeling. J. Clin. Microbiol. 2013, 51, 3741–3748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.S.; Eberl, T.; Sparbier, K.; Lange, C.; Kostrzewa, M.; Schubert, S.; Wieser, A. Rapid detection of antibiotic resistance based on mass spectrometry and stable isotopes. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 949–955. [Google Scholar] [CrossRef]
- Oviaño, M.; Barba, M.J.; Fernández, B.; Ortega, A.; Aracil, B.; Oteo, J.; Campos, J.; Bou, G. Rapid detection of OXA-48-producing Enterobacteriaceae by matrix-assisted laser desorption ionization-time of flight mass spectrometry. J. Clin. Microbiol. 2016, 54, 754–759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akyar, I.; Kaya Ayas, M.; Karatuna, O. Performance evaluation of MALDI-TOF MS MBT STAR-BL versus in-house Carba NP testing for the rapid detection of carbapenemase activity in Escherichia coli and Klebsiella pneumoniae Strains. Microb. Drug Resist. 2019, 25, 985–990. [Google Scholar] [CrossRef]
- Oviaño, M.; Gato, E.; Bou, G. Rapid detection of KPC-Producing Enterobacterales susceptible to imipenem/relebactam by using the MALDI-TOF MS MBT STAR-Carba IVD assay. Front. Microbiol. 2020, 11, 328. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.C.; Chung, C.Y.; Yeh, C.H.; Hsu, K.H.; Chin, Y.C.; Huang, S.S.; Liu, B.R.; Chen, H.A.; Hu, A.; Soo, P.C.; et al. Direct detection of carbapenemase-associated proteins of Acinetobacter baumannii using nanodiamonds coupled with matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. J. Microbiol. Methods 2018, 147, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Sparbier, K.; Schubert, S.; Kostrzewa, M. MBT-ASTRA: A suitable tool for fast antibiotic susceptibility testing? Methods 2016, 104, 48–54. [Google Scholar] [CrossRef]
- Maxson, T.; Taylor-Howell, C.L.; Minogue, T.D. Semi-quantitative MALDI-TOF for antimicrobial susceptibility testing in Staphylococcus aureus. PLoS ONE 2017, 12, e0183899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demirev, P.A.; Hagan, N.S.; Antoine, M.D.; Lin, J.S.; Feldman, A.B. Establishing drug resistance in microorganisms by mass spectrometry. J. Am. Soc. Mass Spectrom. 2013, 24, 1194–1201. [Google Scholar] [CrossRef]
- Idelevich, E.A.; Becker, K.; Reischl, U. New microbiological techniques in the diagnosis of bloodstream infections. Dtsch. Arztebl. Int. 2018, 115, 822–832. [Google Scholar] [CrossRef] [PubMed]
- Correa-Martínez, C.L.; Idelevich, E.A.; Sparbier, K.; Kostrzewa, M.; Becker, K. Rapid Detection of extended-spectrum β-lactamases (ESBL) and AmpC β-lactamases in Enterobacterales: Development of a screening panel using the MALDI-TOF MS-based direct-on-target microdroplet growth assay. Front. Microbiol. 2019, 10, 13. [Google Scholar] [CrossRef]
- Yoon, E.J.; Jeong, S.H. MALDI-TOF mass spectrometry technology as a tool for the rapid diagnosis of antimicrobial resistance in bacteria. Antibiotics 2021, 10, 982. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.H.; Dmitrieva, N.; Gales, A.C.; Petukhova, I.; Al-Obeid, S.; Rossi, F.; M Blondeau, J. Susceptibility testing and reporting of new antibiotics with a focus on tedizolid: An international working group report. Future Microbiol. 2017, 12, 1523–1532. [Google Scholar] [CrossRef] [Green Version]
- Truong, W.R.; Hidayat, L.; Bolaris, M.A.; Nguyen, L.; Yamaki, J. The antibiogram: Key considerations for its development and utilization. JAC-Antimicrob. Resist. 2021, 3, dlab060. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, C.; Patel, C.R.; Kale-Pradhan, P.B. A guide to bacterial culture identification and results interpretation. Pharm. Ther. 2019, 44, 192–200. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Intrinsic Resistance and Unusual Phenotypes, Version 3.3. Available online: http://www.eucast.org/expert_rules_and_intrinsic_resistance/ (accessed on 23 February 2022).
- Livermore, D.M.; Winstanley, T.G.; Shannon, K.P. Interpretative reading: Recognizing the unusual and inferring resistance mechanisms from resistance phenotypes. J. Antimicrob. Chemother. 2001, 48 (Suppl. 1), 87–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahlmeter, G.; Giske, C.G.; Kirn, T.J.; Sharp, S.E. Point-Counterpoint: Differences between the European Committee on Antimicrobial Susceptibility Testing and Clinical and Laboratory Standards Institute Recommendations for reporting antimicrobial susceptibility results. J. Clin. Microbiol. 2019, 57, e01129-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 9.0. Available online: https://www.eucast.org/ast_of_bacteria/previous_versions_of_documents/ (accessed on 23 February 2022).
- European Committee on Antimicrobial Susceptibility Testing. To Clinical Colleagues: On Recent Changes in Clinical Microbiology Susceptibility Reports—New Interpretation of Susceptibility Categories S, I and R. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Guidance_documents/To_clinical_colleagues_on_recent_changes_in_clinical_microbiology_susceptibility_reports_9_July2021.pdf (accessed on 27 February 2022).
- Brown, D.; Cantón, R.; Dubreuil, L.; Gatermann, S.; Giske, C.; MacGowan, A.; Martínez-Martínez, L.; Mouton, J.; Skov, R.; Steinbakk, M.; et al. Widespread implementation of EUCAST breakpoints for antibacterial susceptibility testing in Europe. Eurosurveillance 2015, 20, 21008. [Google Scholar] [CrossRef] [Green Version]
- European Committee on Antimicrobial Susceptibility Testing. General Consultation on Meningitis Breakpoints. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Consultation/2020/Meningitis_breakpoint_consultation_20200901.pdf (accessed on 27 February 2022).
- Van Hal, S.J.; Lodise, T.P.; Paterson, D.L. The clinical significance of vancomycin minimum inhibitory concentration in Staphylococcus aureus infections: A systematic review and meta-analysis. Clin. Infect. Dis. 2012, 54, 755–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graham, M.; Walker, D.A.; Haremza, E.; Morris, A.J. RCPAQAP audit of antimicrobial reporting in Australian and New Zealand laboratories: Opportunities for laboratory contribution to antimicrobial stewardship. J. Antimicrob. Chemother. 2018, 74, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; Seah, J.; Chan, A.; Downing, M.; Johnstone, J.; Matukas, L.M. Antimicrobial stewardship in the microbiology laboratory: Impact of selective susceptibility reporting on ciprofloxacin utilization and susceptibility of gram-negative isolates to ciprofloxacin in a hospital setting. J. Clin. Microbiol. 2016, 54, 2343–2347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramsamy, Y.; Muckart, D.J.J.; Han, K.S.S. Microbiological surveillance and antimicrobial stewardship minimise the need for ultrabroad-spectrum combination therapy for treatment of nosocomial infections in a trauma intensive care unit: An audit of an evidence-based empiric antimicrobial policy. S. Afr. Med. J. 2013, 103, 371. [Google Scholar] [CrossRef] [PubMed]
- Chetty, S.; Reddy, M.; Ramsamy, Y.; Naidoo, A.; Essack, S. Antimicrobial stewardship in South Africa: A scoping review of the published literature. JAC-Antimicrob. Resist. 2019, 1, dlz060. [Google Scholar] [CrossRef] [Green Version]
- Cantón, R.; Oliver, A.; Alós, J.I.; de Benito, N.; Bou, G.; Campos, J.; Calvo, J.; Canut, A.; Castillo, J.; Cercenado, E.; et al. Recommendations of the Spanish Antibiogram Committee (COESANT) for selecting antimicrobial agents and concentrations for in vitro susceptibility studies using automated systems. Enferm. Infecc. Microbiol. Clin. 2020, 38, 182–187. [Google Scholar] [CrossRef]
- Thursky, K.A.; Hardefeldt, L.Y.; Rajkhowa, A.; Ierano, C.; Bishop, J.; Hawes, L.; Biezen, R.; Saha, S.K.; Dowson, L.; Bailey, K.E.; et al. Antimicrobial stewardship in Australia: The role of qualitative research in programme development. JAC-Antimicrob. Resist. 2021, 3, dlab166. [Google Scholar] [CrossRef]
- Lim, J.M.; Singh, S.R.; Duong, M.C.; Legido-Quigley, H.; Hsu, L.Y.; Tam, C.C. Impact of national interventions to promote responsible antibiotic use: A systematic review. J. Antimicrob. Chemother. 2020, 75, 14–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matuschek, E.; Brown, D.F.J.; Kahlmeter, G. Development of the EUCAST disk diffusion antimicrobial susceptibility testing method and its implementation in routine microbiology laboratories. Clin. Microbiol. Infect. 2014, 20, O255–O266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahlmeter, G.; Brown, D. Chapter 9: Laboratory Control of Antimicrobial Therapy. In Antibiotic and Chemotherapy E-Book; Finch, R.G., Greenwood, D., Whitley, R.J., Norrby, S.R., Eds.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2010; pp. 115–122. ISBN 0702047651. [Google Scholar]
- Committee on Trade and Investment (CTI); Sub-Committee on Standards and Conformance (SCSC). Laboratory Guide: Methodologies for Antimicrobial Susceptibility Testing; APEC: Canberra, Australia, 2020; Available online: https://www.apec.org/Publications/2020/05/Laboratory-Guide---Methodologies-for-Antimicrobial-Susceptibility-Testing (accessed on 14 March 2022).
- Karatuna, O. Quality Assurance in Antimicrobial Susceptibility Testing. In Latest Research into Quality Control; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Disk Diffusion Test Manual, Version 10.0. Available online: http://www.eucast.org/ast_of_bacteria/disk_diffusion_methodology/ (accessed on 23 February 2022).
- Procop, G.W.; Church, D.L.; Hall, G.S.; Janda, W.M.; Koneman, E.W.; Schreckenberger, P.C.; Woods, G.L. (Eds.) Antimicrobial Susceptibility Testing. In Koneman’s Color Atlas and Textbook of Diagnostic Microbiology; Jones & Bartlett Learning: Burlington, MA, USA, 2020; pp. 1574–1719. ISBN 9781284322378. [Google Scholar]
- FDA. Antimicrobial Susceptibility Test (AST) Systems—Class II Special Controls Guidance for Industry and FDA; FDA: Silver Spring, MD, USA, 2007. Available online: https://www.fda.gov/medical-devices/guidance-documents-medical-devices-and-radiation-emitting-products/antimicrobial-susceptibility-test-ast-systems-class-ii-special-controls-guidance-industry-and-fda (accessed on 27 February 2022).
- ISO 20776-2:2021; Clinical Laboratory Testing and In Vitro Diagnostic Test Systems—Susceptibility Testing of Infectious Agents and Evaluation of Performance of Antimicrobial Susceptibility Test Devices—Part 2: Evaluation of Performance of Antimicrobial Susceptibility Test Devices Against Reference Broth Micro-Dilution. International Organization for Standardization—ISO: Geneva, Switzerland, 2021.
- Maurer, F.P.; Christner, M.; Hentschke, M.; Rohde, H. Advances in rapid identification and susceptibility testing of bacteria in the clinical microbiology laboratory: Implications for patient care and antimicrobial stewardship programs. Infect. Dis. Rep. 2017, 9, 18–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florio, W.; Baldeschi, L.; Rizzato, C.; Tavanti, A.; Ghelardi, E.; Lupetti, A. Detection of antibiotic-resistance by MALDI-TOF mass spectrometry: An expanding area. Front. Cell. Infect. Microbiol. 2020, 10, 616. [Google Scholar] [CrossRef] [PubMed]
- Soejima, T.; Minami, J.; Iwatsuki, K. The exclusive use of flow cytometry to evaluate the antibiotic-susceptibility. Biochim. Biophys. Acta-Gen. Subj. 2012, 1820, 1980–1986. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, U.; Wirz, D.; Daniels, A. Isothermal micro calorimetry—A new method for MIC determinations: Results for 12 antibiotics and reference strains of E. coli and S. aureus. BMC Microbiol. 2009, 9, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, D.; Veeraraghavan, B.; Elangovan, R.; Vivekanandan, P. Antibiotic resistance and epigenetics: More to it than meets the eye. Antimicrob. Agents Chemother. 2020, 64, e02225-19. [Google Scholar] [CrossRef]
- Marshall, R.L.; Lloyd, G.S.; Lawler, A.J.; Element, S.J.; Kaur, J.; Ciusa, M.L.; Ricci, V.; Tschumi, A.; Kühne, H.; Alderwick, L.J.; et al. New multidrug efflux inhibitors for gram-negative bacteria. MBio 2020, 11, e01340-20. [Google Scholar] [CrossRef] [PubMed]
- Den Blaauwen, T.; Andreu, J.M.; Monasterio, O. Bacterial cell division proteins as antibiotic targets. Bioorg. Chem. 2014, 55, 27–38. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Method | Advantage | Disadvantage | Comments |
|---|---|---|---|
| Broth dilution | Well-standardised | Time-consuming | Quantitative ** |
| Harmonised | Individual mistakes | ||
| Commercially available tests are easy to perform | |||
| Agar Dilution | Well-standardised | Time-consuming | Quantitative |
| Suitable for testing a large number of isolates | Limited concentration of antimicrobial agents | Possible automation in part | |
| Disk diffusion | Simple to perform | Time-consuming | Qualitative * |
| Low cost | No MIC value | ||
| Simple and fast interpretation | The inability for some antibiotics to be tested | ||
| The high number of test antibiotics per test | |||
| High flexibility in antibiotic selection | |||
| Detection of resistance patterns | |||
| Mass use and the possibility of automatisation | |||
| A number of a different use (AST, identification, screening, etc.) | |||
| Detection of heteroresistant population or contamination | |||
| Gradient test | Convenient and flexible | Relatively expensive | Quantitative |
| Simple to perform | Relatively long incubation | ||
| Does not require expertise | |||
| Detection of resistance patterns | |||
| Automated systems | Simple to perform | Relatively expensive | Semi-quantitative *** |
| Chromogenic media | Mass use and the possibility of automatisation | Not completely susceptible and specific | Qualitative with no interpretation criteria (S, I, R) |
| Simple to perform | Time-consuming | ||
| Simple and fast interpretation | Limited spectra or single antibiotic | ||
| Relatively expensive | |||
| Screening only or required confirmatory identification | |||
| No MIC value | |||
| MALDI-TOF MS | Rapid turnaround time | High cost of the MALDI-TOF MS | |
| Simple to perform | Need further optimisation for each species and antibiotic combination | ||
| Low sample volume requirements | No MIC value | ||
| Low per-sample costs | |||
| Genetic methods | Rapid | Limited spectra | Qualitative |
| Highly accurate | Limited throughput | Semi-quantitative | |
| Sensitive | High cost | ||
| Reproducible | |||
| Increased ability to detect slow-growing or non-cultivable organisms | |||
| Genomic methods | Highly accurate | High cost | Qualitative |
| Sensitive | Time-consuming | ||
| Increased ability to detect slow-growing or non-cultivable organisms | Challenging interpretation of results |
| Factor | Influence | Suggested Solutions |
|---|---|---|
| Media (depth of agar) | Thin media yield excessively large inhibition zones and vice versa. | Measure agar depth carefully. |
| Composition of medium | Affects rate of growth of organisms; affects activity and diffusion of antibiotics. | Follow guidelines for an appropriate choice of media; perform quality control. |
| Antibiotic disks (potency) | Deterioration in content leads to smaller inhibition zone sizes. | Use a new lot of disks or unopened cartridge. Maintain majority of disk stock at −20 °C, only keep maximum of 1 week supply at 4 °C (be cautious of β-lactams, clavulanic acid-containing disks and imipenem). |
| Antibiotic disks—spacing | Disks too close together will cause overlapping zones. A smaller plate accommodates fewer disks | Place fewer disks on a plate (especially with very susceptible organisms) |
| Timing of antibiotic disk application | If placed long after swabbing plates, small zones of inhibition may form. | Apply disks within 15 min. |
| Reference strains for QC | Incorrect reference strain used for specific AST will lead to incorrect zone diameters—false alarm. | Follow guidelines for an appropriate choice of QC strains; perform quality control. |
| Inoculum density | Larger zones of inhibition with a light inoculum and vice versa. | Use McFarland standard or calibrator to carefully measure inoculum density and perform colony counts. |
| Incubation time | In most cases, ideal 16–18 h; less time than recommended gives unreliable results. | Follow guidelines for appropriate incubation time. |
| Temperature | If <35 °C larger zones of inhibition are seen and MRSA may go undetected. | Follow guidelines for appropriate incubation temperature. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajic, I.; Kabic, J.; Kekic, D.; Jovicevic, M.; Milenkovic, M.; Mitic Culafic, D.; Trudic, A.; Ranin, L.; Opavski, N. Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics 2022, 11, 427. https://doi.org/10.3390/antibiotics11040427
Gajic I, Kabic J, Kekic D, Jovicevic M, Milenkovic M, Mitic Culafic D, Trudic A, Ranin L, Opavski N. Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics. 2022; 11(4):427. https://doi.org/10.3390/antibiotics11040427
Chicago/Turabian StyleGajic, Ina, Jovana Kabic, Dusan Kekic, Milos Jovicevic, Marina Milenkovic, Dragana Mitic Culafic, Anika Trudic, Lazar Ranin, and Natasa Opavski. 2022. "Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods" Antibiotics 11, no. 4: 427. https://doi.org/10.3390/antibiotics11040427