
The Blood–Brain Barrier and Pharmacokinetic/Pharmacodynamic Optimization of Antibiotics for the Treatment of Central Nervous System Infections in Adults
 , ,
, , 
Abstract
:1. Introduction
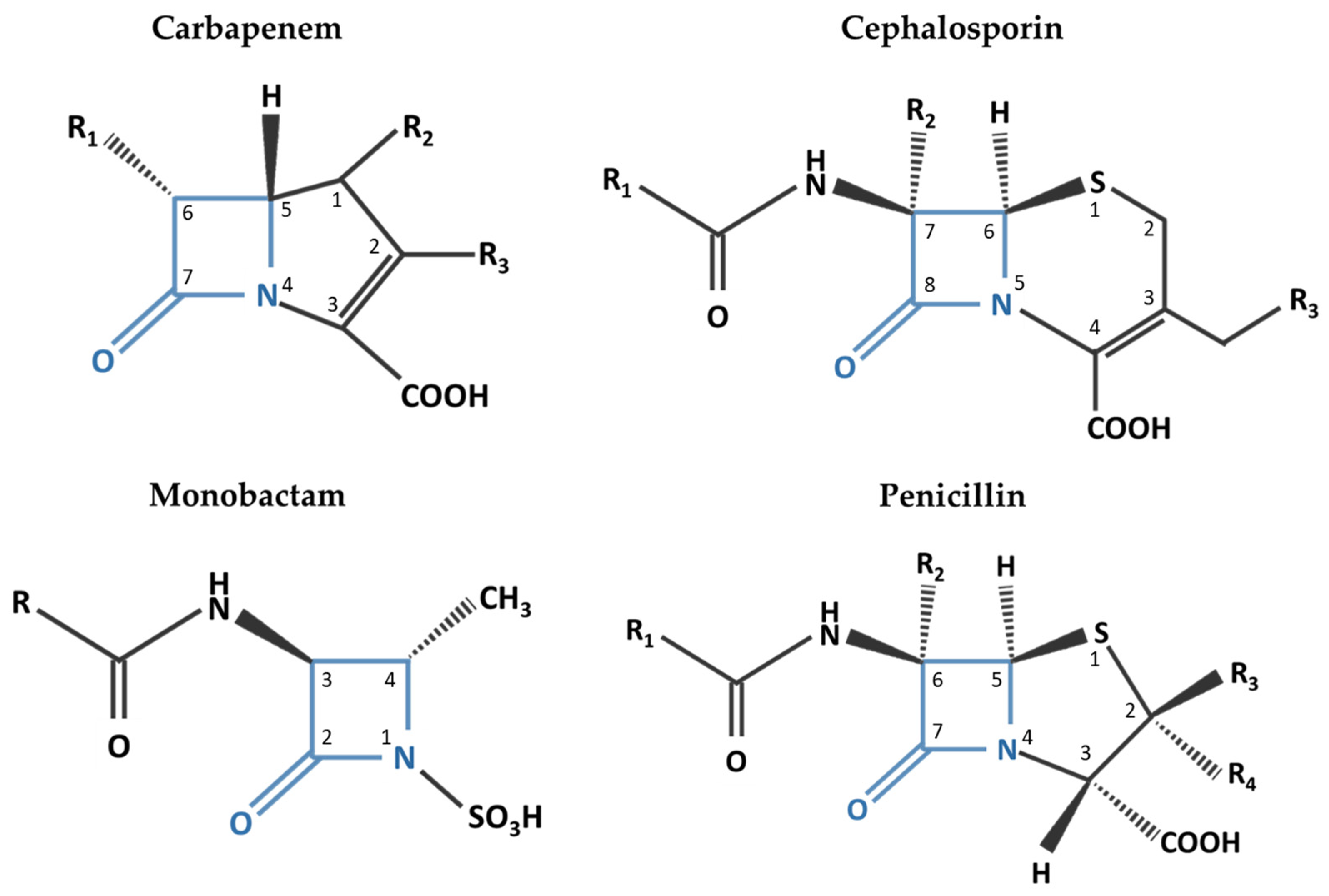
2. Beta-Lactam Antibiotics

{kind=link}
{kind=link}
| Drug | CSF/Serum a (%) | Serum Protein Binding | Primary Route of Elimination | Serum Elimination Half-Life | Serum Cmax | Systemic Dosing | Spectrum of Activity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S. pneumoniae | S. agalactiae | S. aureus MS/MR | H. influenzae | E. coli | P. aeruginosa | N. meningitidis | L. monocytogenes | |||||||
| Beta-lactams | ||||||||||||||
| Penicillin G | 5–10 | ~60% | Renal (58–85% unchanged) | 31 to 50 min | 400 mg/L | 4 million units IV every 4 h | + | + | −/− | − | − | − | + | + |
| Ampicillin | 13–14 | 15 to 18% | Renal (~90% unchanged) | 1 to 1.8 h | 109 to 150 mg/L | 2 g IV every 4 h | + | + | −/− | − | − | − | + | + |
| Nafcillin | <0.2–20 | ~90% (primarily albumin) | Feces, urine (30% unchanged) | 33 to 61 min | ~30 mg/L | 2 g IV every 4 h | + | + | +/− | − | − | − | − | − |
| Oxacillin | 1.0–2.8 | ~94% (primarily albumin) | Urine and bile (unchanged) | 20 to 30 min | 43 mg/L | 2 g IV every 4 h | + | + | +/− | − | − | − | − | − |
| Piperacillin | 1.8–32 | ~16% | Urine | ~1 h | 108.2 ± 31.7 mg/L c | NR | ||||||||
| Cefazolin | 0–4 | 80% | Urine (70–80% unchanged) | 1.8 h | 94 ± 30.33 mg/L | 2 g IV every 8 h (Novak 2021 CI: 6–12 g per day over 24 h | + | + | +/− | − | + | − | − | - |
| Cefoxitin d | 0.8–35 | 65 to 79% | Urine (85% unchanged) | 41 to 59 min | 110 mg/L | NR | ||||||||
| Cefuroxime e | 11.6–13.7 | 33 to 50% | Urine (66–100% unchanged) | ~1 to 2 h | 100 mg/L | NR | ||||||||
| Cefotaxime | 3–48 | 31 to 50% | Urine (60% unchanged) | 1 to 1.5 h | 214.4 mg/L | 8–12 g/day divided every 4–6 h | + b | + | +/− | + | + | v | + | − |
| Ceftriaxone | 0.6–94 | 85 to 95% | Urine (33–67% unchanged) | ~5 to 9 h | 280 ± 39 mg/L | 2 g IV every 12 h | + b | + | +/− | + | + | − | + | − |
| Ceftazidime | 2.7–15 | <10% | Urine (80-90% unchanged) | 1 to 2 h | 61.9 to 79 mg/L | 2 g IV every 8 h | − | + | −/− | + | + | + | + | − |
| Cefepime | 10 | ~20% | Urine (85% unchanged) | 2 h | 129 ± 27.1 mg/L | 2 g IV every 8 h CI: 0.5 g over 30 min followed by 4 g over 24 h | + | + | +/− | + | + | + | + | − |
| Ceftaroline | 0.5–4.3 | ~20% | Urine (88% unchanged) | 1.6 to 2.7 h | 22.3 ± 5.9 to 22.6 ± 2 mg/L | 600 mg every 8-12 h | + | + | +/+ | + | + | − | + | |
| Ceftolozane | 20–40 | 16 to 21% | Urine (>95% unchanged) | ~3 to 4 h | 73.9 ± 25.4 mg/L | Variable and limited data; 3 g ceftolozane–tazobactam over 1 h every 8 h Potential off-label doses up to 4.5 g and administration as prolonged infusion over 3 h or CI | + | + | −/− | + | + | + | ||
| Aztreonam | 1–37 | ~77% | Urine (60%–70% unchanged) Feces (~12%) | 2.1 h | 204 mg/L | 6–8 g/day divided every 6–8 h | − | - | −/− | + | + | + | + | − |
| Imipenem | 1–45 | ~20% | Urine (~70% unchanged) | ~60 min | 44.2 ± 13.26 mg/L | NR due to neurotoxic effects | ||||||||
| Meropenem | 10.7–21 | ~2% | Urine (~70% unchanged, ~28% inactive metabolite) Feces (2%) | 1 h | ~49 mg/L (39 to 58 mg/L) | 2 g IV every 8 h | + | +/− | + | + | + | + | + | |
| Beta-lactamase Inhibitors | ||||||||||||||
| Avibactam | 38 | 5.7 to 8.2% | Urine (97% unchanged) | 2.7 h | 12 to 15.5 mg/L | |||||||||
| Clavulanate | 6–17 | ~25% | Urine (25–40% unchanged) | 1 h | 2.4 ± 0.83 mg/L | |||||||||
| Sulbactam | 13.5 (Wang 2015) | 38% | Urine (75–80% unchanged) | 1 to 1.3 h | 48 to 88 mg/L | |||||||||
| Tazobactam | 3–74 | 30% | Urine (>80% unchanged) | ~2 to 3 h | 21.7 ± 7.8 mg/L | |||||||||
| Vaborbactam | ~33% | Urine (75–95% unchanged) | 1.68 h | 55.6 ± 11 mg/L | ||||||||||
Clinical Perspectives in Consideration of Beta-Lactam PK/PD Data
3. Vancomycin
Clinical Perspective in Consideration of Vancomycin PK/PD Data
4. Aminoglycosides
Clinical Perspective in Consideration of Aminoglycoside PK/PD Data
5. Linezolid
Clinical Perspective in Consideration of Linezolid PK/PD Data
6. Daptomycin
Clinical Perspective in Consideration of Daptomycin PK/PD Data
7. Metronidazole
Clinical Perspectives in Consideration of Metronidazole PK/PD Data
8. Fluoroquinolone
Clinical Perspectives in Consideration of PK/PD Data of Fluoroquinolones
9. Trimethoprim (TMP)/Sulfamethoxazole
Clinical Perspective in Consideration of TMP-SMX PK/PD Data
10. Tetracyclines
Clinical Perspective in Consideration of Doxycyline and Tigecycline PK/PD Data
11. Polymyxin B and Colistin
Clinical Perspectives in Consideration of Polymyxin PK/PD Data
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A
- AUC: Area under concentration time curve. It is the concentration of a drug in serum as a function of time. Technically, the concentration is measured at certain points in time, and mathematical rules are utilized to estimate the AUC. The measurement occurs via several biochemical means, such as chromatography, spectrometry, electrophoresis, etc. AUC correlates with efficacy of a drug.
- AUCCSF: area under the drug concentration–time curve in CSF
- AUCS: area under the drug concentration–time curve in serum
- AUCCSF/AUCS: The ratio of the diffusion of a drug from serum to CSF is determined by the ratio of the area of its concentration–time curve in CSF and that in serum after an intravenous administration. It is the most reliable measure of the penetration of a drug from serum to CSF.
- MIC: A pharmacodynamic parameter defining the susceptibility of bacterial colonies to different concentrations of the antimicrobial being evaluated. A standardized inoculum of bacteria is incubated in dilutions of the antibiotic being evaluated for efficacy. The MIC is the lowest concentration of the antimicrobial drug that inhibits growth of the bacterial organisms.
- Time-dependent antimicrobials: The killing rate is maximal at low multiples of the MIC, usually four to five times the MIC. Any concentration of the antimicrobial above that level will not lead to any faster or more extensive killing of the bacterial organisms. For those agents, bacterial regrowth will soon start after serum antimicrobial concentrations fall below the MIC. For time-dependent antimicrobials, time of the free (non-protein bound) drug exposure above the MIC (fT > MIC) is hence the most important metric that correlates with therapeutic efficacy. This is true of all beta-lactams, macrolides, and clindamycin.
- Concentration-dependent antimicrobials: Increasing the concentration of the antibiotic by increasing the dose will lead to a more extensive and rapid degree of bacterial killing, with a persistent effect of inhibition after the concentrations of those agents fall below the MIC. This phenomenon is called the post-antibiotic effect (see below). Aminoglycosides and fluoroquinolones are concentration-dependent killers. The best parameter to correlate with efficacy is the peak concentration of the drug over the MIC (Cpeak/MIC = Cmax/MIC).
- The efficacy of vancomycin, tetracyclines, and azithromycin is still best measured by the 24 h AUC/MIC due to their longer in vivo PAE, as compared to the beta-lactams, clindamycin, and macrolides (other than azithromycin).
- PAE (post-antibiotic effect) is the persistence of inhibitory effects of antimicrobials after their level in serum is below the MIC or the MBC
References
- Sunwoo, J.; Shin, H.; Lee, H.S.; Moon, J.; Lee, S.; Jung, K.; Park, K.; Jung, K.; Kim, M.; Lee, S.K.; et al. A hospital-based study on etiology and prognosis of bacterial meningitis in adults. Sci. Rep. 2021, 11, 6028. [Google Scholar] [CrossRef] [PubMed]
- Van de Beek, D.; de Gans, J.; Spanjaard, L.; Weisfelt, M.; Reitsma, J.B.; Vermeulen, M. Clinical features and prognostic factors in adults with bacterial meningitis. N. Engl. J. Med. 2004, 351, 1849–1859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auburtin, M.; Wolff, M.; Charpentier, J.; Varon, E.; Le Tulzo, Y.; Girault, C.; Mohammedi, I.; Renard, B.; Mourvillier, B.; Bruneel, F.; et al. Detrimental role of delayed antibiotic administration and penicillin-nonsusceptible strains in adult intensive care unit patients with pneumococcal meningitis: The PNEUMOREA prospective multicenter study. Crit. Care Med. 2006, 34, 2758–2765. [Google Scholar] [CrossRef] [PubMed]
- Proulx, N.; Fréchette, D.; Toye, B.; Chan, J.; Kravcik, S. Delays in the administration of antibiotics are associated with mortality from adult acute bacterial meningitis. QJM 2005, 98, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollay, M. Transport mechanisms in the choroid plexus. Fed. Proc. 1974, 33, 2064–2069. [Google Scholar] [PubMed]
- De Vries, H.E.; Kuiper, J.; De Boer, A.G.; Van Berkel, T.J.; Breimer, D.D. The blood-brain barrier in neuroinflammatory diseases. Pharmacol. Rev. 1997, 49, 143–156. [Google Scholar]
- Ehrlich, P. Über die Beziehungen von chemischer Constitution, Vertheilung und pharmakologischer Wirkung. In The Collected Papers of Paul Ehrlich; Himmelweit, F., Ed.; Pergamon: Oxford, UK, 2013; pp. 570–595. [Google Scholar]
- Tunkel, A.R.; Scheld, W.M. Bacterial Meningitis; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Quagliarello, V.J.; Long, W.J.; Scheld, W.M. Morphologic alterations of the blood-brain barrier with experimental meningitis in the rat. Temporal sequence and role of encapsulation. J. Clin. Investig. 1986, 77, 1084–1095. [Google Scholar] [CrossRef] [Green Version]
- Beach, J.E.; Perrott, J.; Turgeon, R.D.; Ensom, M.H.H. Penetration of Vancomycin into the Cerebrospinal Fluid: A Systematic Review. Clin. Pharmacokinet. 2017, 56, 1479–1490. [Google Scholar] [CrossRef]
- Nau, R.; Sörgel, F.; Eiffert, H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin. Microbiol. Rev. 2010, 23, 858–883. [Google Scholar] [CrossRef] [Green Version]
- Ricard, J.D.; Wolff, M.; Lacherade, J.C.; Mourvillier, B.; Hidri, N.; Barnaud, G.; Chevrel, G.; Bouadma, L.; Dreyfuss, D. Levels of vancomycin in cerebrospinal fluid of adult patients receiving adjunctive corticosteroids to treat pneumococcal meningitis: A prospective multicenter observational study. Clin. Infect. Dis. 2007, 44, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Gundamraj, S.; Hasbun, R. The Use of Adjunctive Steroids in Central Nervous Infections. Front. Cell. Infect. Microbiol. 2020, 10, 592017. [Google Scholar] [CrossRef] [PubMed]
- Andes, D.R.; Craig, W.A. Pharmacokinetics and pharmacodynamics of antibiotics in meningitis. Infect. Dis. Clin. N. Am. 1999, 13, 595–618. [Google Scholar] [CrossRef]
- Van de Beek, D.; Brouwer, M.C.; Thwaites, G.E.; Tunkel, A.R. Advances in treatment of bacterial meningitis. Lancet 2012, 380, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Heffernan, A.J.; Roberts, J.A. Dose optimisation of antibiotics used for meningitis. Curr. Opin. Infect. Dis. 2021, 34, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Kearney, B.P.; Aweeka, F.T. The penetration of anti-infectives into the central nervous system. Neurol. Clin. 1999, 17, 883–900. [Google Scholar] [CrossRef]
- Lutsar, I.; McCracken, G.H., Jr.; Friedland, I.R. Antibiotic pharmacodynamics in cerebrospinal fluid. Clin. Infect. Dis. 1998, 27, 1117–1127. [Google Scholar] [CrossRef] [Green Version]
- Lonsdale, D.O.; Udy, A.A.; Roberts, J.A.; Lipman, J. Antibacterial therapeutic drug monitoring in cerebrospinal fluid: Difficulty in achieving adequate drug concentrations. J. Neurosurg. 2013, 118, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Nadler, H.L.; Pitkin, D.H.; Sheikh, W. The postantibiotic effect of meropenem and imipenem on selected bacteria. J. Antimicrob. Chemother. 1989, 24 (Suppl. A), 225–231. Available online: https://www.ncbi.nlm.nih.gov/pubmed/2509416 (accessed on 5 December 2022). [CrossRef]
- LeBras, M.; Chow, I.; Mabasa, V.H.; Ensom, M.H. Systematic Review of Efficacy, Pharmacokinetics, and Administration of Intraventricular Aminoglycosides in Adults. Neurocrit. Care 2016, 25, 492–507. [Google Scholar] [CrossRef]
- Negus, S.S.; Banks, M.L. Pharmacokinetic-Pharmacodynamic (PKPD) Analysis with Drug Discrimination. Behav. Neurosci. Drug Discrim. 2016, 39, 245–259. [Google Scholar] [CrossRef]
- Kumta, N.; Roberts, J.A.; Lipman, J.; Wong, W.T.; Joynt, G.M.; Cotta, M.O. A Systematic Review of Studies Reporting Antibiotic Pharmacokinetic Data in the Cerebrospinal Fluid of Critically Ill Patients with Uninflamed Meninges. Antimicrob. Agents Chemother. 2020, 65, e01998-20. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Blei, C.; Eiffert, H. Intrathecal Antibacterial and Antifungal Therapies. Clin. Microbiol. Rev. 2020, 33, e00190-19. [Google Scholar] [CrossRef] [PubMed]
- Goto, R.; Horiuchi, Y.; Kawakami, H.; Chikada, A.; Yasuda, T.; Takeuchi, S.; Arai, N. Cerebrospinal fluid analysis is associated with enhancement on MRI in bacterial and tuberculous meningitis: A retrospective observational study. Clin. Neurol. Neurosurg. 2022, 212, 107036. [Google Scholar] [CrossRef]
- Lee, B.J.; Vu, B.N.; Seddon, A.N.; Hodgson, H.A.; Wang, S.K. Treatment Considerations for CNS Infections Caused by Vancomycin-Resistant Enterococcus faecium: A Focused Review of Linezolid and Daptomycin. Ann. Pharmacother. 2020, 54, 1243–1251. [Google Scholar] [CrossRef]
- Markantonis, S.L.; Markou, N.; Fousteri, M.; Sakellaridis, N.; Karatzas, S.; Alamanos, I.; Dimopoulou, E.; Baltopoulos, G. Penetration of colistin into cerebrospinal fluid. Antimicrob. Agents Chemother. 2009, 53, 4907–4910. [Google Scholar] [CrossRef] [Green Version]
- Piva, S.; Di Paolo, A.; Galeotti, L.; Ceccherini, F.; Cordoni, F.; Signorini, L.; Togni, T.; De Nicolò, A.; Rasulo, F.A.; Fagoni, N.; et al. Daptomycin Plasma and CSF Levels in Patients with Healthcare-Associated Meningitis. Neurocrit. Care 2019, 31, 116–124. [Google Scholar] [CrossRef]
- Pfausler, B.; Spiss, H.; Beer, R.; Kampl, A.; Engelhardt, K.; Schober, M.; Schmutzhard, E. Treatment of staphylococcal ventriculitis associated with external cerebrospinal fluid drains: A prospective randomized trial of intravenous compared with intraventricular vancomycin therapy. J. Neurosurg. 2003, 98, 1040–1044. [Google Scholar] [CrossRef] [Green Version]
- Tunkel, A.R.; Hasbun, R.; Bhimraj, A.; Byers, K.; Kaplan, S.L.; Scheld, W.M.; van de Beek, D.; Bleck, T.P.; Garton, H.J.L.; Zunt, J.R.; et al. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin. Infect. Dis. 2017, 64, e34–e65. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.W.; Wang, J.; Qiu, C.F.; Yang, Y.; Shi, Z.H.; Zhou, J.L. A case report of intraventricular and intrathecal tigecycline infusions for an extensively drug-resistant intracranial Acinetobacter baumannii infection. Medicine 2019, 98, e15139. [Google Scholar] [CrossRef]
- Lauretti, L.; D’Alessandris, Q.G.; Fantoni, M.; D’Inzeo, T.; Fernandez, E.; Pallini, R.; Scoppettuolo, G. First reported case of intraventricular tigecycline for meningitis from extremely drug-resistant Acinetobacter baumannii. J. Neurosurg. 2017, 127, 370–373. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zheng, W.; Shi, S. Spinal arachnoiditis followed by intrathecal tigecycline therapy for central nervous system infection by extremely drug-resistant Acinetobacter baumannii. J. Int. Med. Res. 2020, 48, 0300060520920405. [Google Scholar] [CrossRef] [PubMed]
- Long, W.; Yuan, J.; Liu, J.; Liu, J.; Wu, M.; Chen, X.; Peng, G.; Wu, C.; Zhang, C.; Wang, X.; et al. Multidrug Resistant Brain Abscess Due to Acinetobacter baumannii Ventriculitis Cleared by Intraventricular and Intravenous Tigecycline Therapy: A Case Report and Review of Literature. Front. Neurol. 2018, 9, 518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soto-Hernández, J.L.; Soto-Ramírez, A.; Pérez-Neri, I.; Angeles-Morales, V.; Cárdenas, G.; Barradas, V.A. Multidrug-resistant Klebsiella oxytoca ventriculitis, successfully treated with intraventricular tigecycline: A case report. Clin. Neurol. Neurosurg. 2020, 188, 105592. [Google Scholar] [CrossRef]
- Zhong, L.; Shi, X.; Su, L.; Liu, Z. Sequential intraventricular injection of tigecycline and polymyxin B in the treatment of intracranial Acinetobacter baumannii infection after trauma: A case report and review of the literature. Mil. Med. Res. 2020, 7, 23–29. [Google Scholar] [CrossRef] [PubMed]
- El Zahar, N.M.; Sutton, J.M.; Bartlett, M.G. Assessment of brain-to-blood drug distribution using liquid chromatography. Biomed. Chromatogr. 2021, 35, e5123. [Google Scholar] [CrossRef] [PubMed]
- Scheld, W.M. Rationale for optimal dosing of beta-lactam antibiotics in therapy for bacterial meningitis. Eur. J. Clin. Microbiol. 1984, 3, 579–591. [Google Scholar] [CrossRef]
- Veiga, R.P.; Paiva, J.A. Pharmacokinetics—pharmacodynamics issues relevant for the clinical use of beta-lactam antibiotics in critically ill patients. Crit Care 2018, 22, 233. [Google Scholar] [CrossRef] [Green Version]
- Abbott, N.J.; Romero, I.A. Transporting therapeutics across the blood-brain barrier. Mol. Med. Today 1996, 2, 106–113. Available online: https://www.ncbi.nlm.nih.gov/pubmed/8796867 (accessed on 5 December 2022). [CrossRef]
- Armstrong, T.; Fenn, S.J.; Hardie, K.R. JMM Profile: Carbapenems: A broad-spectrum antibiotic. J. Med. Microbiol. 2021, 70, 001462. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34889726 (accessed on 5 December 2022). [CrossRef]
- Neu, H.C. β-Lactam antibiotics: Structural relationships affecting in vitro activity and pharmacologic properties. Rev. Infect. Dis. 1986, 8 (Suppl. S3), S237–S259. [Google Scholar] [CrossRef] [PubMed]
- Nicoletti, G.; Russo, G.; Bonfiglio, G. Recent developments in carbapenems. Expert Opin. Investig. Drugs 2002, 11, 529–544. Available online: https://www.ncbi.nlm.nih.gov/pubmed/11922861 (accessed on 5 December 2022). [CrossRef] [PubMed]
- De Rosa, M.; Verdino, A.; Soriente, A.; Marabotti, A. The Odd Couple(s): An Overview of Beta-Lactam Antibiotics Bearing More Than One Pharmacophoric Group. Int. J. Mol. Sci. 2021, 22, 617. [Google Scholar] [CrossRef] [PubMed]
- Spector, R. Advances in understanding the pharmacology of agents used to treat bacterial meningitis. Pharmacology 1990, 41, 113–118. Available online: https://www.ncbi.nlm.nih.gov/pubmed/2277805 (accessed on 5 December 2022). [CrossRef]
- Dagan, R.; Velghe, L.; Rodda, J.L.; Klugman, K.P. Penetration of meropenem into the cerebrospinal fluid of patients with inflamed meninges. J. Antimicrob. Chemother. 1994, 34, 175–179. Available online: https://www.ncbi.nlm.nih.gov/pubmed/7961206 (accessed on 5 December 2022). [CrossRef]
- Di Paolo, A.; Gori, G.; Tascini, C.; Danesi, R.; Del Tacca, M. Clinical pharmacokinetics of antibacterials in cerebrospinal fluid. Clin. Pharmacokinet. 2013, 52, 511–542. [Google Scholar] [CrossRef]
- Täuber, M.G.; Sande, M.A. Principles in the treatment of bacterial meningitis. Am. J. Med. 1984, 76, 224–230. [Google Scholar] [CrossRef]
- Matzneller, P.; Burian, A.; Zeitlinger, M.; Sauermann, R. Understanding the Activity of Antibiotics in Cerebrospinal Fluid in vitro. Pharmacology 2016, 97, 233–244. [Google Scholar] [CrossRef]
- Jongmans, C.; Muller, A.E.; Van Den Broek, P.; Cruz De Almeida, B.M.; Van Den Berg, C.; Van Oldenrijk, J.; Bos, P.K.; Koch, B.C.P. An Overview of the Protein Binding of Cephalosporins in Human Body Fluids: A Systematic Review. Front. Pharmacol. 2022, 13, 900551. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Roberts, J.A.; Rello, J.; Paterson, D.L.; Lipman, J. The effects of hypoalbuminaemia on optimizing antibacterial dosing in critically ill patients. Clin. Pharmacokinet. 2011, 50, 99–110. [Google Scholar] [CrossRef]
- Nau, R.; Seele, J.; Djukic, M.; Eiffert, H. Pharmacokinetics and pharmacodynamics of antibiotics in central nervous system infections. Curr. Opin. Infect. Dis. 2018, 31, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Tunkel, A.R.; Hartman, B.J.; Kaplan, S.L.; Kaufman, B.A.; Roos, K.L.; Scheld, W.M.; Whitley, R.J. Practice guidelines for the management of bacterial meningitis. Clin. Infect. Dis. 2004, 39, 1267–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clumeck, N.; Thys, J.P.; Vanhoof, R.; Vanderlinden, M.P.; Butzler, J.P.; Yourassowsky, E. Amoxicillin entry into human cerebrospinal fluid: Comparison with ampicillin. Antimicrob. Agents Chemother. 1978, 14, 531–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burgess, D.S.; Frei, C.R.; Lewis Ii, J.S.; Fiebelkorn, K.R.; Jorgensen, J.H. The contribution of pharmacokinetic-pharmacodynamic modelling with Monte Carlo simulation to the development of susceptibility breakpoints for Neisseria meningitidis. Clin. Microbiol. Infect. 2007, 13, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Kanra, G. Experience with ampicillin/sulbactam in severe infections. J. Int. Med. Res. 2002, 30 (Suppl. S1), 20A–30A. [Google Scholar] [CrossRef]
- Stahl, J.P.; Bru, J.P.; Fredj, G.; Brammer, K.W.; Malleret, M.R.; Micoud, M. Penetration of sulbactam into the cerebrospinal fluid of patients with bacterial meningitis receiving ampicillin therapy. Rev. Infect. Dis. 1986, 8 (Suppl. S5), S612–S616. [Google Scholar] [CrossRef]
- Ullah, S.; Beer, R.; Fuhr, U.; Taubert, M.; Zeitlinger, M.; Kratzer, A.; Dorn, C.; Arshad, U.; Kofler, M.; Helbok, R.; et al. Brain Exposure to Piperacillin in Acute Hemorrhagic Stroke Patients Assessed by Cerebral Microdialysis and Population Pharmacokinetics. Neurocrit. Care 2020, 33, 740–748. [Google Scholar] [CrossRef] [Green Version]
- Nau, R.; Kinzig-Schippers, M.; Sörgel, F.; Schinschke, S.; Rössing, R.; Müller, C.; Kolenda, H.; Prange, H.W. Kinetics of piperacillin and tazobactam in ventricular cerebrospinal fluid of hydrocephalic patients. Antimicrob. Agents Chemother. 1997, 41, 987–991. [Google Scholar] [CrossRef] [Green Version]
- Novak, A.R.; Krsak, M.; Kiser, T.H.; Neumann, R.T.; Cava Prado, L.; Molina, K.C.; Mueller, S.W. Pharmacokinetic Evaluation of Cefazolin in the Cerebrospinal Fluid of Critically Ill Patients. Open Forum Infect. Dis. 2022, 9, ofab649. [Google Scholar] [CrossRef]
- Le Turnier, P.; Gregoire, M.; Deslandes, G.; Lakhal, K.; Deschanvres, C.; Lecomte, R.; Talarmin, J.P.; Dubée, V.; Bellouard, R.; Boutoille, D.; et al. Should we reconsider cefazolin for treating staphylococcal meningitis? A retrospective analysis of cefazolin and cloxacillin cerebrospinal fluid levels in patients treated for staphylococcal meningitis. Clin. Microbiol. Infect. 2020, 26, 1415.e1. [Google Scholar] [CrossRef]
- Nau, R.; Prange, H.W.; Muth, P.; Mahr, G.; Menck, S.; Kolenda, H.; Sörgel, F. Passage of cefotaxime and ceftriaxone into cerebrospinal fluid of patients with uninflamed meninges. Antimicrob. Agents Chemother. 1993, 37, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- Del Rio, M.A.; Chrane, D.; Shelton, S.; McCracken, G.H.J.; Nelson, J.D. Ceftriaxone versus ampicillin and chloramphenicol for treatment of bacterial meningitis in children. Lancet 1983, 321, 1241–1244. [Google Scholar] [CrossRef] [PubMed]
- Le Turnier, P.; El Helali, N.; Guilhaumou, R.; Pilmis, B.; Revest, M.; Velly, L.J.; Leroy, A.G.; Duval, X.; Lemaitre, F.; Gregoire, M.; et al. CSF concentration of cefotaxime in adult patients with pneumococcal meningitis: A multicentre retrospective study. J. Antimicrob. Chemother. 2021, 76, 2352–2355. [Google Scholar] [CrossRef] [PubMed]
- Dajani, A.S. Cefotaxime use in pediatric infections. Diagn. Microbiol. Infect. Dis. 1995, 22, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.F.; Darville, T.; Parks, J.A.; Enderlin, G. Safety profile and efficacy of cefotaxime for the treatment of hospitalized children. Clin. Infect. Dis. 1992, 14, 56–65. [Google Scholar] [CrossRef]
- Kassel, L.E.; Van Matre, E.T.; Foster, C.J.; Fish, D.N.; Mueller, S.W.; Sherman, D.S.; Wempe, M.F.; MacLaren, R.; Neumann, R.T.; Kiser, T.H.; et al. A Randomized Pharmacokinetic and Pharmacodynamic Evaluation of Every 8-Hour and 12-Hour Dosing Strategies of Vancomycin and Cefepime in Neurocritically ill Patients. Pharmacotherapy 2018, 38, 921–934. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Prange, H.W.; Kinzig, M.; Frank, A.; Dressel, A.; Scholz, P.; Kolenda, H.; Sörgel, F. Cerebrospinal fluid ceftazidime kinetics in patients with external ventriculostomies. Antimicrob. Agents Chemother. 1996, 40, 763–766. [Google Scholar] [CrossRef] [Green Version]
- Helfer, V.E.; Zavascki, A.P.; Zeitlinger, M.; de Araújo, B.V.; Dalla Costa, T. Population Pharmacokinetic Modeling and Probability of Target Attainment of Ceftaroline in Brain and Soft Tissues. Antimicrob. Agents Chemother. 2022, 66, e00741-22. Available online: https://www.ncbi.nlm.nih.gov/pubmed/36005769 (accessed on 5 December 2022). [CrossRef]
- Adkinson, N.F.J.; Saxon, A.; Spence, M.R.; Swabb, E.A. Cross-allergenicity and immunogenicity of aztreonam. Rev. Infect. Dis. 1985, 7 (Suppl. S4), S613–S621. [Google Scholar] [CrossRef]
- Georgopapadakou, N.H.; Smith, S.A.; Sykes, R.B. Mode of action of azthreonam. Antimicrob. Agents Chemother. 1982, 21, 950–956. [Google Scholar] [CrossRef] [Green Version]
- Patriarca, G.; Schiavino, D.; Lombardo, C.; Altomonte, G.; De Cinti, M.; Buonomo, A.; Nucera, E. Tolerability of aztreonam in patients with IgE-mediated hypersensitivity to beta-lactams. Int. J. Immunopathol. Pharmacol. 2008, 21, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Pérez Pimiento, A.; Gómez Martínez, M.; Mínguez Mena, A.; Trampal González, A.; de Paz Arranz, S.; Rodríguez Mosquera, M. Aztreonam and ceftazidime: Evidence of in vivo cross allergenicity. Allergy 1998, 53, 624–625. [Google Scholar] [CrossRef] [PubMed]
- Clark, P. Aztreonam. Obstet. Gynecol. Clin. N. Am. 1992, 19, 519–528. [Google Scholar] [CrossRef]
- Cunha, B.A. Aztreonam. Urology 1993, 41, 249–258. [Google Scholar] [CrossRef]
- Neu, H.C. Aztreonam: The first monobactam. Med. Clin. N. Am. 1988, 72, 555–566. [Google Scholar] [CrossRef]
- Sykes, R.B.; Bonner, D.P. Discovery and development of the monobactams. Rev. Infect. Dis. 1985, 7 (Suppl. S4), S579–S593. [Google Scholar] [CrossRef]
- Johnson, D.H.; Cunha, B.A. Aztreonam. Med. Clin. N. Am. 1995, 79, 733–743. [Google Scholar] [CrossRef]
- Pulcini, C.; Bush, K.; Craig, W.A.; Frimodt-Møller, N.; Grayson, M.L.; Mouton, J.W.; Turnidge, J.; Harbarth, S.; Gyssens, I.C.; The ESCMID Study Group for Antibiotic Policies. Forgotten antibiotics: An inventory in Europe, the United States, Canada, and Australia. Clin. Infect. Dis. 2012, 54, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Lentnek, A.L.; Williams, R.R. Aztreonam in the treatment of gram-negative bacterial meningitis. Rev. Infect. Dis. 1991, 13 (Suppl. S7), S586–S590. [Google Scholar] [CrossRef]
- Duma, R.J.; Berry, A.J.; Smith, S.M.; Baggett, J.W.; Swabb, E.A.; Platt, T.B. Penetration of aztreonam into cerebrospinal fluid of patients with and without inflamed meninges. Antimicrob. Agents Chemother. 1984, 26, 730–733. [Google Scholar] [CrossRef] [Green Version]
- De Sarro, A.; Ammendola, D.; Zappala, M.; Grasso, S.; De Sarro, G.B. Relationship between structure and convulsant properties of some beta-lactam antibiotics following intracerebroventricular microinjection in rats. Antimicrob. Agents Chemother. 1995, 39, 232–237. Available online: https://www.ncbi.nlm.nih.gov/pubmed/7695312 (accessed on 5 December 2022). [CrossRef] [PubMed]
- Klugman, K.P.; Dagan, R. PMC162697; Randomized comparison of meropenem with cefotaxime for treatment of bacterial meningitis. Meropenem Meningitis Study Group. Antimicrob. Agents Chemother. 1995, 39, 1140–1146. Available online: https://www.ncbi.nlm.nih.gov/pubmed/7625802 (accessed on 5 December 2022). [CrossRef] [PubMed] [Green Version]
- Margetis, K.; Dimaraki, E.; Charkoftaki, G.; Vryonis, E.; Markantonis, S.; Boutos, N.; Archontaki, H.; Sakas, D.E.; Valsami, G.; Skoutelis, A.; et al. Penetration of intact blood-brain barrier by doripenem. Antimicrob. Agents Chemother. 2011, 55, 3637–3638. Available online: https://www.ncbi.nlm.nih.gov/pubmed/21555772 (accessed on 5 December 2022). [CrossRef] [PubMed] [Green Version]
- Hashizume, T.; Ishino, F.; Nakagawa, J.; Tamaki, S.; Matsuhashi, M. Studies on the mechanism of action of imipenem (N-formimidoylthienamycin) in vitro: Binding to the penicillin-binding proteins (PBPs) in Escherichia coli and Pseudomonas aeruginosa, and inhibition of enzyme activities due to the PBPs in E. coli. J. Antibiot. 1984, 37, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Martínez, L. Extended-spectrum beta-lactamases and the permeability barrier. Clin. Microbiol. Infect. 2008, 14 (Suppl. S1), 82–89. [Google Scholar] [CrossRef] [Green Version]
- Sime, F.B.; Lassig-Smith, M.; Starr, T.; Stuart, J.; Pandey, S.; Parker, S.L.; Wallis, S.C.; Lipman, J.; Roberts, J.A. Cerebrospinal Fluid Penetration of Ceftolozane-Tazobactam in Critically Ill Patients with an Indwelling External Ventricular Drain. Antimicrob. Agents Chemother. 2020, 65, e01698-20. [Google Scholar] [CrossRef]
- Dinh, A.; Wyplosz, B.; Kernéis, S.; Lebeaux, D.; Bouchand, F.; Duran, C.; Béraud, G.; Lazaro, P.; Davido, B.; Hénard, S.; et al. Use of ceftolozane/tazobactam as salvage therapy for infections due to extensively drug-resistant Pseudomonas aeruginosa. Int. J. Antimicrob. Agents 2017, 49, 782–783. [Google Scholar] [CrossRef]
- Frattari, A.; Savini, V.; Polilli, E.; Cibelli, D.; Talamazzi, S.; Bosco, D.; Consorte, A.; Fazii, P.; Parruti, G. Ceftolozane-tazobactam and Fosfomycin for rescue treatment of otogenous meningitis caused by XDR Pseudomonas aeruginosa: Case report and review of the literature. IDCases 2018, 14, e00451. [Google Scholar] [CrossRef]
- McCreary, E.K.; Byers, K.E.; Fernandes, C.; Kline, E.G.; Nicolau, D.P.; Shields, R.K. Plasma and Cerebrospinal Fluid Therapeutic Drug Monitoring of Ceftolozane and Tazobactam During Treatment of Multidrug-Resistant Pseudomonas aeruginosa Meningitis. In Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2020; Volume 7, p. ofaa549. [Google Scholar] [CrossRef]
- Winans, S.A.; Guerrero-Wooley, R.; Park, S.H.; Hino, G.J.; Forland, S.C. Continuous infusion of ceftolozane-tazobactam resulted in high cerebrospinal fluid concentrations of ceftolozane in a patient with multidrug-resistant Pseudomonas aeruginosa meningitis. Infection 2021, 49, 355–359. [Google Scholar] [CrossRef]
- Gatti, M.; Virgili, G.; Cojutti, P.G.; Gaibani, P.; Conti, M.; Sturiale, C.; Pea, F.; Viale, P. Real-Time Optimization of Pharmacodynamic Target Attainment at Infection Site during Treatment of Post-Neurosurgical Ventriculitis Caused by Carbapenem-Resistant Gram Negatives with Ceftazidime-Avibactam-Based Regimens: A Report of Two Cases. Microorganisms 2022, 10, 154. [Google Scholar] [CrossRef]
- Holyk, A.; Belden, V.; Lee, J.J.; Musick, W.; Keul, R.; Britz, G.W.; Lin, J. Ceftazidime/avibactam use for carbapenem-resistant Klebsiella pneumoniae meningitis: A case report. J. Antimicrob. Chemother. 2018, 73, 254–256. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.; Edwards, N.J.; Rojas, L.J.; Rudin, S.D.; Marshall, S.H.; Cicco, I.D.; Bonomo, R.A.; Arias, C.; Tran, T.T. Ceftazidime-avibactam for the treatment of post-neurosurgical meningitis caused by a Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae. In Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2016; Volume 3. [Google Scholar]
- Yasmin, M.; Hanrahan, J.; Marshall, S.; Lodise, T.P.; Chen, L.; Perez, F.; Kreiswirth, B.; Bonomo, R.A. Using Therapeutic Drug Monitoring to Treat KPC-Producing Klebsiella pneumoniae Central Nervous System Infection with Ceftazidime/Avibactam. In Open Forum Infectious Diseases; Oxford University Press: New York, NY, USA, 2020; Volume 7, p. ofaa349. [Google Scholar] [CrossRef]
- Norrby, S.R. Role of cephalosporins in the treatment of bacterial meningitis in adults. Overview with special emphasis on ceftazidime. Am. J. Med. 1985, 79, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.E.; Yasin, F.; Smith, C.; Scharmen, A.; Havlichek, D.; Bill, C. A pharmacokinetic/pharmacodynamic analysis of ceftaroline prophylaxis in patients with external ventricular drains. Surg. Infect. 2015, 16, 169–173. [Google Scholar] [CrossRef]
- Wang, Q.; Wu, Y.; Chen, B.; Zhou, J. Drug concentrations in the serum and cerebrospinal fluid of patients treated with cefoperazone/sulbactam after craniotomy. BMC Anesthesiol. 2015, 15, 33. [Google Scholar] [CrossRef] [Green Version]
- Pea, F.; Viale, P.; Furlanut, M. Antimicrobial therapy in critically ill patients: A review of pathophysiological conditions responsible for altered disposition and pharmacokinetic variability. Clin. Pharmacokinet. 2005, 44, 1009–1034. [Google Scholar] [CrossRef] [PubMed]
- Sinnollareddy, M.G.; Roberts, M.S.; Lipman, J.; Roberts, J.A. β-Lactam Pharmacokinetics and Pharmacodynamics in Critically Ill Patients and Strategies for Dose Optimization: A Structured Review. Clin. Exp. Pharmacol. Physiol. 2012, 39, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Lutsar, I.; Ahmed, A.; Friedland, I.R.; Trujillo, M.; Wubbel, L.; Olsen, K.; McCracken, G.H., Jr. Pharmacodynamics and bactericidal activity of ceftriaxone therapy in experimental cephalosporin-resistant pneumococcal meningitis. Antimicrob. Agents Chemother. 1997, 41, 2414–2417. [Google Scholar] [CrossRef] [Green Version]
- Fratoni, A.J.; Nicolau, D.P.; Kuti, J.L. A guide to therapeutic drug monitoring of β-lactam antibiotics. Pharmacotherapy 2021, 41, 220–233. [Google Scholar] [CrossRef]
- Roberts, J.A.; Ulldemolins, M.; Roberts, M.S.; McWhinney, B.; Ungerer, J.; Paterson, D.L.; Lipman, J. Therapeutic drug monitoring of beta-lactams in critically ill patients: Proof of concept. Int. J. Antimicrob. Agents 2010, 36, 332–339. [Google Scholar] [CrossRef]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic initial β-lactam concentrations in select critically ill patients: Association between augmented renal clearance and low trough drug concentrations. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.; Alffenaar, J.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef] [PubMed]
- Hussein, K.; Bitterman, R.; Shofty, B.; Paul, M.; Neuberger, A. Management of post-neurosurgical meningitis: Narrative review. Clin. Microbiol. Infect. 2017, 23, 621–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barreto, E.F.; Webb, A.J.; Pais, G.M.; Rule, A.D.; Jannetto, P.J.; Scheetz, M.H. Setting the beta-lactam therapeutic range for critically ill patients: Is there a floor or even a ceiling? Crit. Care Explor. 2021, 3, e0446. [Google Scholar] [CrossRef] [PubMed]
- Hurkacz, M.; Dobrek, L.; Wiela-Hojeńska, A. Antibiotics and the Nervous System-Which Face of Antibiotic Therapy Is Real, Dr. Jekyll (Neurotoxicity) or Mr. Hyde (Neuroprotection)? Molecules 2021, 26, 7456. [Google Scholar] [CrossRef] [PubMed]
- Kuti, J.L.; Nightingale, C.H.; Knauft, R.F.; Nicolau, D.P. Pharmacokinetic properties and stability of continuous-infusion meropenem in adults with cystic fibrosis. Clin. Ther. 2004, 26, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Mattoes, H.M.; Kuti, J.L.; Drusano, G.L.; Nicolau, D.P. Optimizing antimicrobial pharmacodynamics: Dosage strategies for meropenem. Clin. Ther. 2004, 26, 1187–1198. [Google Scholar] [CrossRef]
- Huang, H.; Huang, S.; Zhu, P.; Xi, X. Continuous versus intermittent infusion of cefepime in neurosurgical patients with post-operative intracranial infections. Int. J. Antimicrob. Agents 2014, 43, 68–72. [Google Scholar] [CrossRef]
- Grégoire, M.; Dailly, E.; Le Turnier, P.; Garot, D.; Guimard, T.; Bernard, L.; Tattevin, P.; Vandamme, Y.M.; Hoff, J.; Lemaitre, F.; et al. High-Dose Ceftriaxone for Bacterial Meningitis and Optimization of Administration Scheme Based on Nomogram. Antimicrob. Agents Chemother. 2019, 63, e00634-19. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, A.; Dos Santos, C.; Cimbro, M. Postantibiotic effect of meropenem in combination with gentamicin or sparfloxacin on Gram-positive and Gram-negative organisms. Clin. Microbiol. Infect. 1998, 4, 431–435. [Google Scholar] [CrossRef]
- Marone, P.; Concia, E.; Maserati, R.; Suter, F.; Minoli, L.; Andreoni, M.; Fiori, G. Ceftazidime in the therapy of pseudomonal meningitis. Chemioterapia 1985, 4, 289–292. [Google Scholar]
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg. Infect. 2013, 14, 73–156. [Google Scholar] [CrossRef] [Green Version]
- Ichie, T.; Urano, K.; Suzuki, D.; Okada, T.; Kobayashi, N.; Hayashi, H.; Sugiura, Y.; Yamamura, K.; Sugiyama, T. Influence of cerebral fluid drainage on the pharmacokinetics of vancomycin in neurosurgical patients. Pharmazie 2015, 70, 404–409. [Google Scholar] [PubMed]
- Mrowczynski, O.D.; Langan, S.T.; Rizk, E.B. Intra-cerebrospinal fluid antibiotics to treat central nervous system infections: A review and update. Clin. Neurol. Neurosurg. 2018, 170, 140–158. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, J.D.; Fuursted, K.; Espersen, F.; Frimodt-Møller, N. Activities of vancomycin and teicoplanin against penicillin-resistant pneumococci in vitro and in vivo and correlation to pharmacokinetic parameters in the mouse peritonitis model. Antimicrob. Agents Chemother. 1997, 41, 1910–1915. [Google Scholar] [CrossRef] [Green Version]
- Larsson, A.J.; Walker, K.J.; Raddatz, J.K.; Rotschafer, J.C. The concentration-independent effect of monoexponential and biexponential decay in vancomycin concentrations on the killing of Staphylococcus aureus under aerobic and anaerobic conditions. J. Antimicrob. Chemother. 1996, 38, 589–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rybak, M.; Lomaestro, B.; Rotschafer, J.C.; Moellering, R.J.; Craig, W.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society of Infectious Diseases Pharmacists. Am. J. Health-Syst. Pharm. 2009, 66, 82–98. [Google Scholar] [CrossRef]
- Kumta, N.; Roberts, J.A.; Lipman, J.; Cotta, M.O. Antibiotic Distribution into Cerebrospinal Fluid: Can Dosing Safely Account for Drug and Disease Factors in the Treatment of Ventriculostomy-Associated Infections? Clin. Pharmacokinet. 2018, 57, 439–454. [Google Scholar] [CrossRef]
- Blassmann, U.; Hope, W.; Roehr, A.C.; Frey, O.R.; Vetter-Kerkhoff, C.; Thon, N.; Briegel, J.; Huge, V. CSF penetration of vancomycin in critical care patients with proven or suspected ventriculitis: A prospective observational study. J. Antimicrob. Chemother. 2019, 74, 991–996. [Google Scholar] [CrossRef]
- Schneider, F.; Gessner, A.; El-Najjar, N. Efficacy of Vancomycin and Meropenem in Central Nervous System Infections in Children and Adults: Current Update. Antibiotics 2022, 11, 173. [Google Scholar] [CrossRef]
- Albanèse, J.; Léone, M.; Bruguerolle, B.; Ayem, M.L.; Lacarelle, B.; Martin, C. Cerebrospinal fluid penetration and pharmacokinetics of vancomycin administered by continuous infusion to mechanically ventilated patients in an intensive care unit. Antimicrob. Agents Chemother. 2000, 44, 1356–1358. [Google Scholar] [CrossRef]
- Wang, Q.; Shi, Z.; Wang, J.; Shi, G.; Wang, S.; Zhou, J. Postoperatively administered vancomycin reaches therapeutic concentration in the cerebral spinal fluid of neurosurgical patients. Surg. Neurol. 2008, 69, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Vancomycin Hydrochloride Intravenous Injection [Package Insert]; Hospira Inc.: Lake Forest, IL, USA, 2021.
- Cunha, B.A.; Cunha, C.B. Pharmacokinetic considerations in selecting optimal antibiotic therapy for Mycoplasma pneumoniae encephalitis. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Rybak, M.J.; Albrecht, L.M.; Boike, S.C.; Chandrasekar, P.H. Nephrotoxicity of vancomycin, alone and with an aminoglycoside. J. Antimicrob. Chemother. 1990, 25, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, G.; Klastersky, J.; Coppens, L.; Daneau, D.; Nubourgh, Y. Gram-negative bacillary meningitis in neurosurgical patients. J. Neurosurg. 1983, 59, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Wald-Dickler, N.; Holtom, P.; Spellberg, B. Busting the Myth of “Static vs. Cidal”: A Systemic Literature Review. Clin. Infect. Dis. 2018, 66, 1470–1474. [Google Scholar] [CrossRef]
- McKinnell, J.A.; Arias, C.A. Editorial Commentary: Linezolid vs. Daptomycin for Vancomycin-Resistant Enterococci: The Evidence Gap Between Trials and Clinical Experience. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 879–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luque, S.; Grau, S.; Alvarez-Lerma, F.; Ferrández, O.; Campillo, N.; Horcajada, J.P.; Basas, M.; Lipman, J.; Roberts, J.A. Plasma and cerebrospinal fluid concentrations of linezolid in neurosurgical critically ill patients with proven or suspected central nervous system infections. Int. J. Antimicrob. Agents 2014, 44, 409–415. [Google Scholar] [CrossRef] [Green Version]
- Dietz, N.; Barra, M.; Zhang, M.; Zacharaiah, M.; Coumans, J.V. Acute myeloid leukemia with central nervous system extension and subdural seeding of vancomycin-resistant Enterococcus faecium after bilateral subdural hematomas treated with subdural daptomycin administration. Surg. Neurol. Int. 2019, 10, 171. [Google Scholar] [CrossRef] [PubMed]
- Frasca, K.L.; Schuster, M.G. Vancomycin-resistant enterococcal meningitis in an autologous stem cell transplant recipient cured with linezolid. Transpl. Infect. Dis. 2013, 15, E1–E4. [Google Scholar] [CrossRef]
- Knoll, B.M.; Hellmann, M.; Kotton, C.N. Vancomycin-resistant Enterococcus faecium meningitis in adults: Case series and review of the literature. Scand. J Infect Dis 2013, 45, 131–139. [Google Scholar] [CrossRef]
- Myrianthefs, P.; Markantonis, S.L.; Vlachos, K.; Anagnostaki, M.; Boutzouka, E.; Panidis, D.; Baltopoulos, G. Serum and cerebrospinal fluid concentrations of linezolid in neurosurgical patients. Antimicrob. Agents Chemother. 2006, 50, 3971–3976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, J.; Tang, J.; Li, D. Success of linezolid therapy for postneurosurgical ventriculitis due to vancomycin-resistant Enterococcus faecium: Case report and literature review. Chin. Neurosurg. J. 2016, 2, 46–49. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, Z.H.; Peloquin, C.A.; Ericsson, C.D. Successful treatment of vancomycin-resistant Enterococcus faecium meningitis with linezolid: Case report and literature review. Scand. J. Infect. Dis. 2001, 33, 375–379. [Google Scholar] [CrossRef]
- Steinmetz, M.P.; Vogelbaum, M.A.; De Georgia, M.A.; Andrefsky, J.C.; Isada, C. Successful treatment of vancomycin-resistant enterococcus meningitis with linezolid: Case report and review of the literature. Crit. Care Med. 2001, 29, 2383–2385. [Google Scholar] [CrossRef]
- Tsai, T.N.; Wu, C.P.; Peng, M.Y.; Giian, C.F.; Lee, S.Y.; Lu, J.J. Short course of linezolid treatment for vancomycin-resistant Enterococcus faecium meningitis. Int. J. Clin. Pract. 2006, 60, 740–741. [Google Scholar] [CrossRef] [PubMed]
- Zeana, C.; Kubin, C.J.; Della-Latta, P.; Hammer, S.M. Vancomycin-resistant Enterococcus faecium meningitis successfully managed with linezolid: Case report and review of the literature. Clin. Infect. Dis. 2001, 33, 477–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lich, B.F.; Conner, A.K.; Burks, J.D.; Glenn, C.A.; Sughrue, M.E. Intrathecal/Intraventricular Linezolid in Multidrug-Resistant Enterococcus faecalis Ventriculitis. J. Neurol. Surg. Rep. 2016, 77, e160–e161. [Google Scholar] [CrossRef] [Green Version]
- Entenza, J.M.; Giddey, M.; Vouillamoz, J.; Moreillon, P.; Mancini, S. Assessment of the in vitro synergy of daptomycin plus linezolid against multidrug-resistant enterococci. J. Glob. Antimicrob. Resist. 2014, 2, 306–308. [Google Scholar] [CrossRef]
- Krzysztofiak, A.; Bozzola, E.; Lancella, L.; Quondamcarlo, A.; Gesualdo, F.; Ugazio, A.G. Linezolid therapy of brain abscess. Pediatr. Infect. Dis. J. 2010, 29, 1063–1064. [Google Scholar] [CrossRef]
- ZYVOX(R) Intravenous Injection [Package Insert]; Pfizer Inc.: New York, NY, USA, 2013.
- Le, J.; Bookstaver, P.B.; Rudisill, C.N.; Hashem, M.G.; Iqbal, R.; James, C.L.; Sakoulas, G. Treatment of meningitis caused by vancomycin-resistant Enterococcus faecium: High-dose and combination daptomycin therapy. Ann. Pharmacother. 2010, 44, 2001–2006. [Google Scholar] [CrossRef]
- Taglietti, F.; Campanile, F.; Capone, A.; Di Caro, A.; Grilli, E.; Stazi, G.; Bertuccio, T.; Petrosillo, N.; Stefani, S. Daptomycin efficacy in the central nervous system of a patient with disseminated methicillin-resistant Staphylococcus aureus infection: A case report. J. Med. Case Rep. 2012, 6, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, S.W.; Kiser, T.H.; Anderson, T.A.; Neumann, R.T. Intraventricular daptomycin and intravenous linezolid for the treatment of external ventricular-drain-associated ventriculitis due to vancomycin-resistant Enterococcus faecium. Ann. Pharmacother. 2012, 46, e35. [Google Scholar] [CrossRef]
- Wang, J.S.; Muzevich, K.; Edmond, M.B.; Bearman, G.; Stevens, M.P. Central nervous system infections due to vancomycin-resistant enterococci: Case series and review of the literature. Int. J. Infect. Dis. 2014, 25, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubicin(R) Intravenous Injection [package insert]; Cubist Pharmaceuticals: Lexington, MA, USA, 2010.
- Craig, W.A.; Ebert, S.C. Killing and regrowth of bacteria in vitro: A review. Scand. J. Infect. Dis. Suppl. 1990, 74, 63–70. [Google Scholar] [PubMed]
- Nix, D.E.; Tyrrell, R.; Müller, M. Pharmacodynamics of metronidazole determined by a time-kill assay for Trichomonas vaginalis. Antimicrob. Agents Chemother. 1995, 39, 1848–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farmakiotis, D.; Zeluff, B. Metronidazole-Associated Encephalopathy. N. Engl. J. Med. 2016, 374, 1465. [Google Scholar] [CrossRef] [Green Version]
- Hobson-Webb, L.D.; Roach, E.S.; Donofrio, P.D. Metronidazole: Newly recognized cause of autonomic neuropathy. J. Child Neurol. 2006, 21, 429–431. [Google Scholar] [CrossRef]
- Kim, E.; Na, D.G.; Kim, E.Y.; Kim, J.H.; Son, K.R.; Chang, K.H. MR imaging of metronidazole-induced encephalopathy: Lesion distribution and diffusion-weighted imaging findings. Am. J. Neuroradiol. 2007, 28, 1652–1658. [Google Scholar] [CrossRef] [Green Version]
- Moosa, A.N.; Perkins, D. MRI of metronidazole induced cerebellar ataxia. J. Neurol. Neurosurg. Psychiatry 2010, 81, 754–755. [Google Scholar] [CrossRef]
- Patel, K.; Green-Hopkins, I.; Lu, S.; Tunkel, A.R. Cerebellar ataxia following prolonged use of metronidazole: Case report and literature review. Int. J. Infect. Dis. 2008, 12, e111–e114. [Google Scholar] [CrossRef]
- Bryan, C.S.; Huffman, L.J.; Del Bene, V.E.; Sanders, C.V.; Scalcini, M.C. Intravenous metronidazole therapy for Bacteroides fragilis meningitis. South. Med. J. 1979, 72, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, H.G.; Förster, D.; Muirhead, B. Metronidazole concentration of the cerebrospinal fluid from slightly inflamed meninges. Arzneim. Forsch. 1984, 34, 830–831. [Google Scholar]
- Jokipii, A.M.; Myllylä, V.V.; Hokkanen, E.; Jokipii, L. Penetration of the blood brain barrier by metronidazole and tinidazole. J. Antimicrob. Chemother. 1977, 3, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Warner, J.F.; Perkins, R.L.; Cordero, L. Metronidazole therapy of anaerobic bacteremia, meningitis, and brain abscess. Arch. Intern. Med. 1979, 139, 167–169. [Google Scholar] [CrossRef] [PubMed]
- Lamp, K.C.; Freeman, C.D.; Klutman, N.E.; Lacy, M.K. Pharmacokinetics and pharmacodynamics of the nitroimidazole antimicrobials. Clin. Pharmacokinet. 1999, 36, 353–373. [Google Scholar] [CrossRef]
- Frasca, D.; Dahyot-Fizelier, C.; Adier, C.; Mimoz, O.; Debaene, B.; Couet, W.; Marchand, S. Metronidazole and hydroxymetronidazole central nervous system distribution: 1. Microdialysis assessment of brain extracellular fluid concentrations in patients with acute brain injury. Antimicrob. Agents Chemother. 2014, 58, 1019–1023. [Google Scholar] [CrossRef] [Green Version]
- Frasca, D.; Dahyot-Fizelier, C.; Adier, C.; Mimoz, O.; Debaene, B.; Couet, W.; Marchand, S. Metronidazole and hydroxymetronidazole central nervous system distribution: 2. Cerebrospinal fluid concentration measurements in patients with external ventricular drain. Antimicrob. Agents Chemother. 2014, 58, 1024–1027. [Google Scholar] [CrossRef] [Green Version]
- Ralph, E.D. Clinical pharmacokinetics of metronidazole. Clin. Pharmacokinet. 1983, 8, 43–62. [Google Scholar] [CrossRef]
- Ralph, E.D.; Clarke, J.T.; Libke, R.D.; Luthy, R.P.; Kirby, W.M. Pharmacokinetics of metronidazole as determined by bioassay. Antimicrob. Agents Chemother. 1974, 6, 691–696. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.H.; Emmons, K.; Seligsohn, R. Pharmacokinetics of intravenous metronidazole at different dosages in healthy subjects. Int. J. Clin. Pharmacol. Ther. Toxicol. 1991, 29, 386–390. [Google Scholar]
- Alffenaar, J.W.C.; de Vries, P.M.; Luijckx, G.J.; van Soolingen, D.; van der Werf, T.S.; van Altena, R. Plasma and cerebrospinal fluid pharmacokinetics of moxifloxacin in a patient with tuberculous meningitis. Antimicrob. Agents Chemother. 2008, 52, 2293–2295. [Google Scholar] [CrossRef] [Green Version]
- Alffenaar, J.W.C.; van Altena, R.; Bökkerink, H.J.; Luijckx, G.J.; van Soolingen, D.; Aarnoutse, R.E.; van der Werf, T.S. Pharmacokinetics of moxifloxacin in cerebrospinal fluid and plasma in patients with tuberculous meningitis. Clin. Infect. Dis. 2009, 49, 1080–1082. [Google Scholar] [CrossRef]
- Wright, D.H.; Brown, G.H.; Peterson, M.L.; Rotschafer, J.C. Application of fluoroquinolone pharmacodynamics. J. Antimicrob. Chemother. 2000, 46, 669–683. [Google Scholar] [CrossRef]
- Donald, P.R. Cerebrospinal fluid concentrations of antituberculosis agents in adults and children. Tuberculosis 2010, 90, 279–292. [Google Scholar] [CrossRef]
- Kanellakopoulou, K.; Pagoulatou, A.; Stroumpoulis, K.; Vafiadou, M.; Kranidioti, H.; Giamarellou, H.; Giamarellos-Bourboulis, E.J. Pharmacokinetics of moxifloxacin in non-inflamed cerebrospinal fluid of humans: Implication for a bactericidal effect. J. Antimicrob. Chemother. 2008, 61, 1328–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pea, F.; Pavan, F.; Nascimben, E.; Benetton, C.; Scotton, P.G.; Vaglia, A.; Furlanut, M. Levofloxacin disposition in cerebrospinal fluid in patients with external ventriculostomy. Antimicrob. Agents Chemother. 2003, 47, 3104–3108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baggio, D.; Ananda-Rajah, M.R. Fluoroquinolone antibiotics and adverse events. Aust. Prescr. 2021, 44, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, R.F.; Davey, P.G.; Lambert, J.J. Antagonism of GABAA receptors by 4-quinolones. J. Antimicrob. Chemother. 1993, 31, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, S.; Alvi, U.; Soliven, B.; Rezania, K. Drugs That Induce or Cause Deterioration of Myasthenia Gravis: An Update. J. Clin. Med. 2021, 10, 1537. [Google Scholar] [CrossRef]
- Sutter, R.; Rüegg, S.; Tschudin-Sutter, S. Seizures as adverse events of antibiotic drugs: A systematic review. Neurology 2015, 85, 1332–1341. [Google Scholar] [CrossRef]
- Rodriguez-Cerrato, V.; McCoig, C.C.; Michelow, I.C.; Ghaffar, F.; Jafri, H.S.; Hardy, R.D.; Patel, C.; Olsen, K.; McCracken, G.H.J. Pharmacodynamics and bactericidal activity of moxifloxacin in experimental Escherichia coli meningitis. Antimicrob. Agents Chemother. 2001, 45, 3092–3097. [Google Scholar] [CrossRef] [Green Version]
- Nijland, H.M.J.; Ruslami, R.; Suroto, A.J.; Burger, D.M.; Alisjahbana, B.; van Crevel, R.; Aarnoutse, R.E. Rifampicin reduces plasma concentrations of moxifloxacin in patients with tuberculosis. Clin. Infect. Dis. 2007, 45, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Kemnic, T.R.; Coleman, M. Trimethoprim Sulfamethoxazole; StatPearls Publishing: Tampa, FL, USA, 2021. [Google Scholar]
- Brown, G.R. Cotrimoxazole-optimal dosing in the critically ill. Ann. Intensive Care 2014, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudley, M.N.; Levitz, R.E.; Quintiliani, R.; Hickingbotham, J.M.; Nightingale, C.H. Pharmacokinetics of trimethoprim and sulfamethoxazole in serum and cerebrospinal fluid of adult patients with normal meninges. Antimicrob. Agents Chemother. 1984, 26, 811–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levitz, R.E.; Quintiliani, R. Trimethoprim-sulfamethoxazole for bacterial meningitis. Ann. Intern. Med. 1984, 100, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Elmedani, S.; Albayati, A.; Udongwo, N.; Odak, M.; Khawaja, S. Trimethoprim-Sulfamethoxazole-Induced Aseptic Meningitis: A New Approach. Cureus 2021, 13, e15869. [Google Scholar] [CrossRef]
- BACTRIM(TM) Intravenous Injection [Package Insert]; Sun Pharmaceutical Industries Inc.: Cranbury, NJ, USA, 2020.
- Lee, D.H.; Palermo, B.; Chowdhury, M. Vancomycin-Resistant Enterococcus faecium Meningitis Successfully Treated with Daptomycin in Combination with Doxycycline and Linezolid: Case Report. Infect. Dis. Clin. Pract. 2011, 19, 55–58. Available online: https://journals.lww.com/infectdis/Fulltext/2011/01000/Vancomycin_Resistant_Enterococcus_faecium.14.aspx (accessed on 5 December 2022). [CrossRef]
- Agwuh, K.N.; MacGowan, A. Pharmacokinetics and pharmacodynamics of the tetracyclines including glycylcyclines. J. Antimicrob. Chemother. 2006, 58, 256–265. [Google Scholar] [CrossRef] [Green Version]
- Kang-Birken, S.L.; Castel, U.; Prichard, J.G. Oral doxycycline for treatment of neurosyphilis in two patients infected with human immunodeficiency virus. Pharmacother. 2010, 30, 418. [Google Scholar] [CrossRef]
- Psomas, K.C.; Brun, M.; Causse, A.; Atoui, N.; Reynes, J.; Le Moing, V. Efficacy of ceftriaxone and doxycycline in the treatment of early syphilis. Médecine Mal. Infect. 2012, 42, 15–19. [Google Scholar] [CrossRef]
- Meijer, L.A.; Ceyssens, K.G.; de Grève, B.I.; de Bruijn, W. Pharmacokinetics and bioavailability of doxycycline hyclate after oral administration in calves. Vet. Q. 1993, 15, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saivin, S.; Houin, G. Clinical pharmacokinetics of doxycycline and minocycline. Clin. Pharmacokinet. 1988, 15, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Yim, C.W.; Flynn, N.M.; Fitzgerald, F.T. Penetration of oral doxycycline into the cerebrospinal fluid of patients with latent or neurosyphilis. Antimicrob. Agents Chemother. 1985, 28, 347–348. [Google Scholar] [CrossRef] [Green Version]
- Dotevall, L.; Hagberg, L. Penetration of doxycycline into cerebrospinal fluid in patients treated for suspected Lyme neuroborreliosis. Antimicrob. Agents Chemother. 1989, 33, 1078–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pankey, G.A. Tigecycline. J. Antimicrob. Chemother. 2005, 56, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.E.; Craig, W.A. Tigecycline: A critical analysis. Clin. Infect. Dis. 2006, 43, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Yaghoubi, S.; Zekiy, A.O.; Krutova, M.; Gholami, M.; Kouhsari, E.; Sholeh, M.; Ghafouri, Z.; Maleki, F. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: Narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 1003–1022. [Google Scholar] [CrossRef] [PubMed]
- Prasad, P.; Sun, J.; Danner, R.L.; Natanson, C. Excess deaths associated with tigecycline after approval based on noninferiority trials. Clin. Infect. Dis. 2012, 54, 1699–1709. [Google Scholar] [CrossRef] [Green Version]
- Shen, F.; Han, Q.; Xie, D.; Fang, M.; Zeng, H.; Deng, Y. Efficacy and safety of tigecycline for the treatment of severe infectious diseases: An updated meta-analysis of RCTs. Int. J. Infect. Dis. 2015, 39, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Tasina, E.; Haidich, A.; Kokkali, S.; Arvanitidou, M. Efficacy and safety of tigecycline for the treatment of infectious diseases: A meta-analysis. Lancet Infect. Dis. 2011, 11, 834–844. [Google Scholar] [CrossRef]
- Yahav, D.; Lador, A.; Paul, M.; Leibovici, L. Efficacy and safety of tigecycline: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2011, 66, 1963–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhavnani, S.M.; Rubino, C.M.; Hammel, J.P.; Forrest, A.; Dartois, N.; Cooper, C.A.; Korth-Bradley, J.; Ambrose, P.G. Pharmacological and patient-specific response determinants in patients with hospital-acquired pneumonia treated with tigecycline. Antimicrob. Agents Chemother. 2012, 56, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Wang, R.; Liang, B.; Bai, N.; Liu, Y. Systematic review and meta-analysis of the effectiveness and safety of tigecycline for treatment of infectious disease. Antimicrob. Agents Chemother. 2011, 55, 1162–1172. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Vardakas, K.Z.; Tsiveriotis, K.P.; Triarides, N.A.; Tansarli, G.S. Effectiveness and safety of high-dose tigecycline-containing regimens for the treatment of severe bacterial infections. Int. J. Antimicrob. Agents 2014, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ray, L.; Levasseur, K.; Nicolau, D.P.; Scheetz, M.H. Cerebral spinal fluid penetration of tigecycline in a patient with Acinetobacter baumannii cerebritis. Ann. Pharmacother. 2010, 44, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Rodvold, K.A.; Gotfried, M.H.; Cwik, M.; Korth-Bradley, J.M.; Dukart, G.; Ellis-Grosse, E.J. Serum, tissue and body fluid concentrations of tigecycline after a single 100 mg dose. J. Antimicrob. Chemother. 2006, 58, 1221–1229. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, K.; Zhao, J.; Wang, Q.; Zhou, J. Intraventricular administration of tigecycline for the treatment of multidrug-resistant bacterial meningitis after craniotomy: A case report. J. Chemother. 2018, 30, 49–52. [Google Scholar] [CrossRef]
- De Pascale, G.; Pompucci, A.; Maviglia, R.; Spanu, T.; Bello, G.; Mangiola, A.; Scoppettuolo, G. Successful treatment of multidrug-resistant Acinetobacter baumannii ventriculitis with intrathecal and intravenous colistin. Minerva Anestesiol. 2010, 76, 957–960. [Google Scholar]
- Guo, W.; Guo, S.; Li, M.; Li, L.; Qu, Y. Successful treatment of extensively drug-resistant Acinetobacter baumannii ventriculitis with polymyxin B and tigecycline- a case report. Antimicrob. Resist. Infect. Control. 2018, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Regaieg, K.; Bahloul, M.; Turki, O.; Mnif, B.; Bouaziz, M. L’efficacité de l’association tigécycline–colistine dans le traitement d’une méningite à Acinetobacter baumannii multi-résistant. Médecine Mal. Infect. 2017, 47, 175–177. Available online: https://www.sciencedirect.com/science/article/pii/S0399077X16307661 (accessed on 5 December 2022). [CrossRef]
- Tsolaki, V.; Karvouniaris, M.; Manoulakas, E.; Kotlia, P.; Karadontas, V.; Fotakopoulos, G.; Zakynthinos, E.; Makris, D. Intraventricular CNS treatment with Colistin-Tigecycline combination: A case series. J. Crit. Care 2018, 47, 338–341. [Google Scholar] [CrossRef]
- Li, J.; Liu, Y.; Wu, G.; Wang, H.; Xu, X. Intravenous plus intraventricular tigecycline-amikacin therapy for the treatment of carbapenem-resistant Klebsiella pneumoniae ventriculitis: A case report. Med. 2022, 101, e29635. [Google Scholar] [CrossRef] [PubMed]
- Jaspan, H.B.; Brothers, A.W.; Campbell, A.J.P.; McGuire, J.K.; Browd, S.R.; Manley, T.J.; Pak, D.; Weissman, S.J. Multidrug-resistant Enterococcus faecium meningitis in a toddler: Characterization of the organism and successful treatment with intraventricular daptomycin and intravenous tigecycline. Pediatr. Infect. Dis. J. 2010, 29, 379–381. [Google Scholar] [CrossRef]
- Şahin, A.; Dalgic, N. Intraventricular Plus Intravenous Tigecycline for the Treatment of Daptomycin Nonsusceptible Vancomycin-Resistant Enterococci in an Infant with Ventriculoperitoneal Shunt Infection. World Neurosurg. 2019, 130, 470–473. [Google Scholar] [CrossRef]
- Mastroianni, A.; Greco, S.; Urso, F.; Mauro, M.V.; Vangeli, V. Does Tigecycline Have a Place in Therapy for Rickettsial Infection of the Central Nervous System? Infect. Chemother. 2022, 54, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Velkov, T.; Roberts, K.D.; Nation, R.L.; Thompson, P.E.; Li, J. Pharmacology of polymyxins: New insights into an ‘old’ class of antibiotics. Future Microbiol. 2013, 8, 711–724. [Google Scholar] [CrossRef] [Green Version]
- Bergen, P.J.; Landersdorfer, C.B.; Zhang, J.; Zhao, M.; Lee, H.J.; Nation, R.L.; Li, J. Pharmacokinetics and pharmacodynamics of ‘old’ polymyxins: What is new? Diagn. Microbiol. Infect. Dis. 2012, 74, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Guo, X.; Xie, D.; Dong, X.; Niu, J.; Chen, G. A Clinical Study on the Use of Intraventricular Polymyxin B Supplemented by Continuous External Ventricular Drainage in the Treatment of Drug-Resistant Gram-Negative Bacilli Intracranial Infection. Infect. Drug Resist. 2020, 13, 2963–2970. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Bliziotis, I.A.; Tam, V.H. Intraventricular or intrathecal use of polymyxins in patients with Gram-negative meningitis: A systematic review of the available evidence. Int. J. Antimicrob. Agents 2007, 29, 9–25. [Google Scholar] [CrossRef]
- Abodakpi, H.; Gohlke, J.; Chang, K.; Chow, D.S.; Tam, V.H. Analytical and functional determination of polymyxin B protein binding in serum. Antimicrob. Agents Chemother. 2015, 59, 7121–7123. [Google Scholar] [CrossRef] [Green Version]
- Avedissian, S.N.; Liu, J.; Rhodes, N.J.; Lee, A.; Pais, G.M.; Hauser, A.R.; Scheetz, M.H. A Review of the Clinical Pharmacokinetics of Polymyxin B. Antibiotics 2019, 8, 31. [Google Scholar] [CrossRef] [PubMed]


| Vancomycin Dose Requires Renal Dose Adjustment | IV: 30–60 mg/kg/Day ITT: 5–20 mg Daily IVT: 5–20 mg Daily |
| Indication/targeted organisms | Gram-positive organisms |
| PK/PD data |
|
| Linezolid Dose | IV/PO: 600 mg Twice Daily |
| Indication/targeted organisms | Vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus aureus (MRSA), and Propionibacterium acnes CNS infections |
| PK/PD data |
|
| Daptomycin Dose Requires Weight and Renal Dose Adjustment | IV: 6–10 mg/kg Once Daily IVT: 5 mg Daily or Every 48 h |
| Indication/targeted organisms | Vancomycin-resistant Enterococcus (VRE) and methicillin-resistant Staphylococcus aureus (MRSA) CNS infections |
| PK/PD data |
|
| Metronidazole dose Does not require renal adjustment; hepatic adjustment to 50% dose in severe impairment | Orally or intravenously (500 mg over 30 min every 8 h) |
| Indications/targeted organisms: | Anaerobic bacteria (Bacteroides fragilis, Prevotella species, Fusobacterium necrophorum, Clostridium difficile, Gardneralla vaginalis), protozoa, and microaerophilic bacteria. |
| PK/PD data | Serum/CSF Penetration: 18–103% CSF/Serum AUC ratio: 0.86–1.02 Serum Cmax: 6.2–40.6 mg/L CSF Cmax: 11.0–84.1 mg/L Protein Binding: <20% Elimination half-life: 3.1–16.4 h |
| Moxifloxacin Dose Requires no renal dose adjustment | IV or PO 400 mg daily (except possibly when co-administered with rifampin, then consider 800 mg daily) | |
| Indication/targeted organisms | Tuberculous Meningitis | |
| PK/PD Data for moxifloxacin | Serum/CSF penetration: Ratios ranged from 0.0913 to 0.741, depending on time after administration Peak ratio at 4–6 h CSF/serum AUC ratio: Uninflamed/mildly inflamed meninges: 0.45 Strongly inflamed meninges: 0.79 (0.79–0.94) Serum Cmax: Moxifloxacin 400 mg/day: 4.5 mg/L Moxifloxacin 800 mg/day: 2.45–3.65 mg/L Protein binding Moxifloxacin 400 mg/day: 50–60% in serum, 10% in CSF Moxifloxacin 800 mg/day: 40% in serum, 5% in CSF Elimination half-life: Moxifloxacin 400 mg/day: 4.55–12 h (5.52–6 h in CSF) Moxifloxacin 800 mg/day: 4.09 h (5.20 h CSF) | |
| Intracranial/spinal epidural abscess (MRSA) |
|
| Melioidosis (Burkholderia pseudomallei) |
|
| Meningitis (MRSA, Listeria monocytogenes, E. coli, Enterobacteriaceae) |
|
| Nocardiosis (off-label use, not recommended for monotherapy) |
|
| Toxoplasma gondii encephalitis |
|
| PK/PD Data |
CSF/serum concentrations:
|
| Doxycycline | Tigecycline | |
|---|---|---|
| Indication | Neurosyphilis (alternative) | Meningitis with MDR or XDR organisms (Acinetobacter baumannii or CRE Klebsiella) |
| Dose Requires no renal or hepatic dose adjustment | IV 200 mg every 12 h PO: 200 mg every 12 h No IVT/ITT administration |
|
| PK/PD Data |
|
| Dose | IV/IVT: 50,000 units once daily (in combination with systemic therapy) |
| Indication/targeted organisms | CSF Shunt-related meningitis (MDR Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae) |
| PD/PD Data | CSF/serum concentrations: No data available Percent protein binding: 58% Serum half-life: 9–11.5 h Cmax: 2–14 mcg/mL |
| Dose Requires weight and renal dose adjustment | IV/IVT: 10 mg once daily (Colistimethate sodium) |
| Indication/targeted organisms | Meningitis (MDR Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae) |
| PK/PD Data | CSF/serum concentrations: 0.05 Percent protein binding: No data available Serum half-life: 251 min Cmax: no data available |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haddad, N.; Carr, M.; Balian, S.; Lannin, J.; Kim, Y.; Toth, C.; Jarvis, J. The Blood–Brain Barrier and Pharmacokinetic/Pharmacodynamic Optimization of Antibiotics for the Treatment of Central Nervous System Infections in Adults. Antibiotics 2022, 11, 1843. https://doi.org/10.3390/antibiotics11121843
Haddad N, Carr M, Balian S, Lannin J, Kim Y, Toth C, Jarvis J. The Blood–Brain Barrier and Pharmacokinetic/Pharmacodynamic Optimization of Antibiotics for the Treatment of Central Nervous System Infections in Adults. Antibiotics. 2022; 11(12):1843. https://doi.org/10.3390/antibiotics11121843
Chicago/Turabian StyleHaddad, Nicholas, Maddie Carr, Steve Balian, James Lannin, Yuri Kim, Courtney Toth, and Jennifer Jarvis. 2022. "The Blood–Brain Barrier and Pharmacokinetic/Pharmacodynamic Optimization of Antibiotics for the Treatment of Central Nervous System Infections in Adults" Antibiotics 11, no. 12: 1843. https://doi.org/10.3390/antibiotics11121843