
Efficacy and Safety of Colistin versus Tigecycline for Multi-Drug-Resistant and Extensively Drug-Resistant Gram-Negative Pathogens—A Meta-Analysis

Abstract
:1. Introduction
2. Results
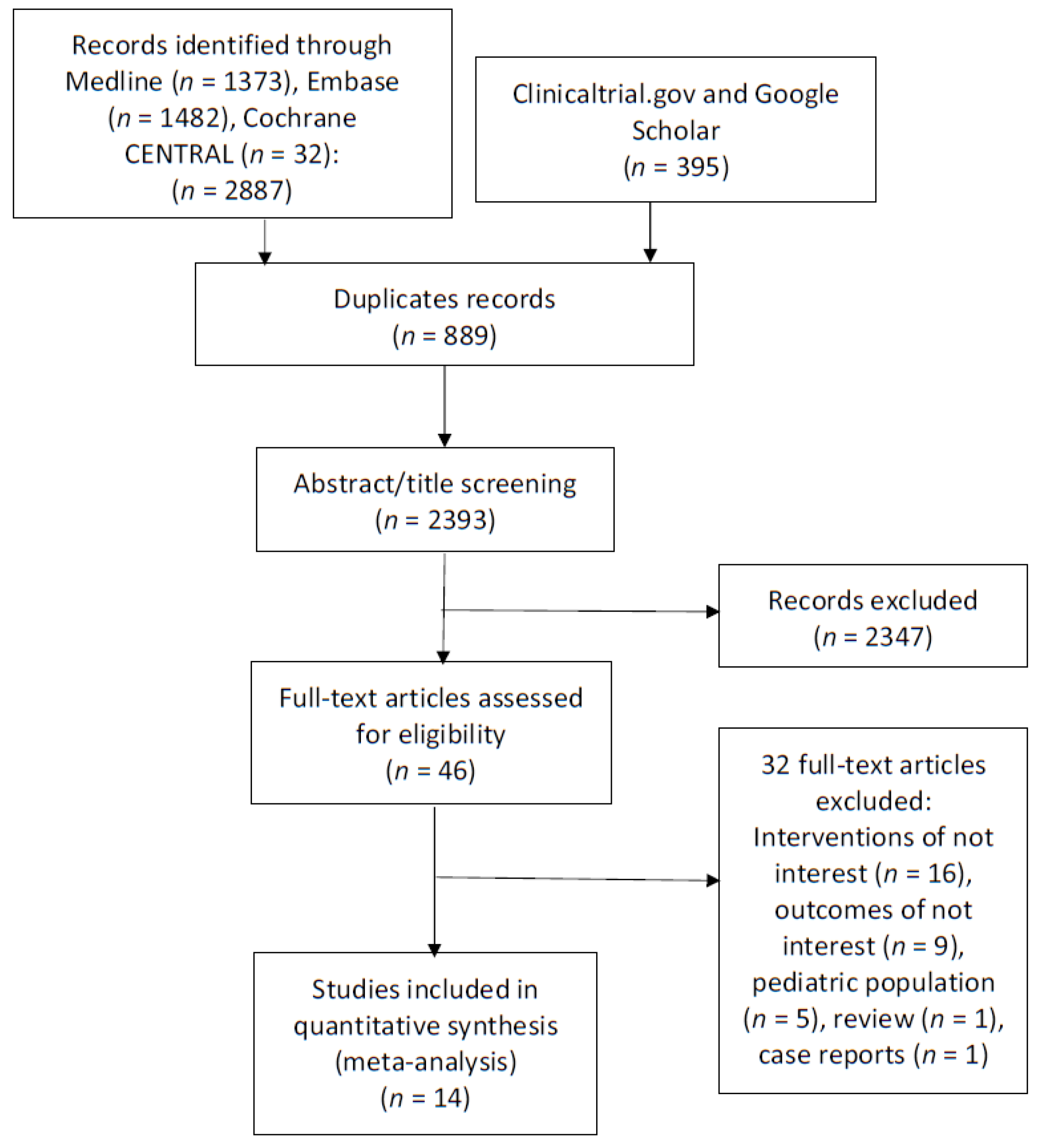
2.1. Search Strategy Results
2.2. Characteristics of Included Studies
2.3. Outcomes
2.3.1. Tigecycline Monotherapy versus Colistin Monotherapy
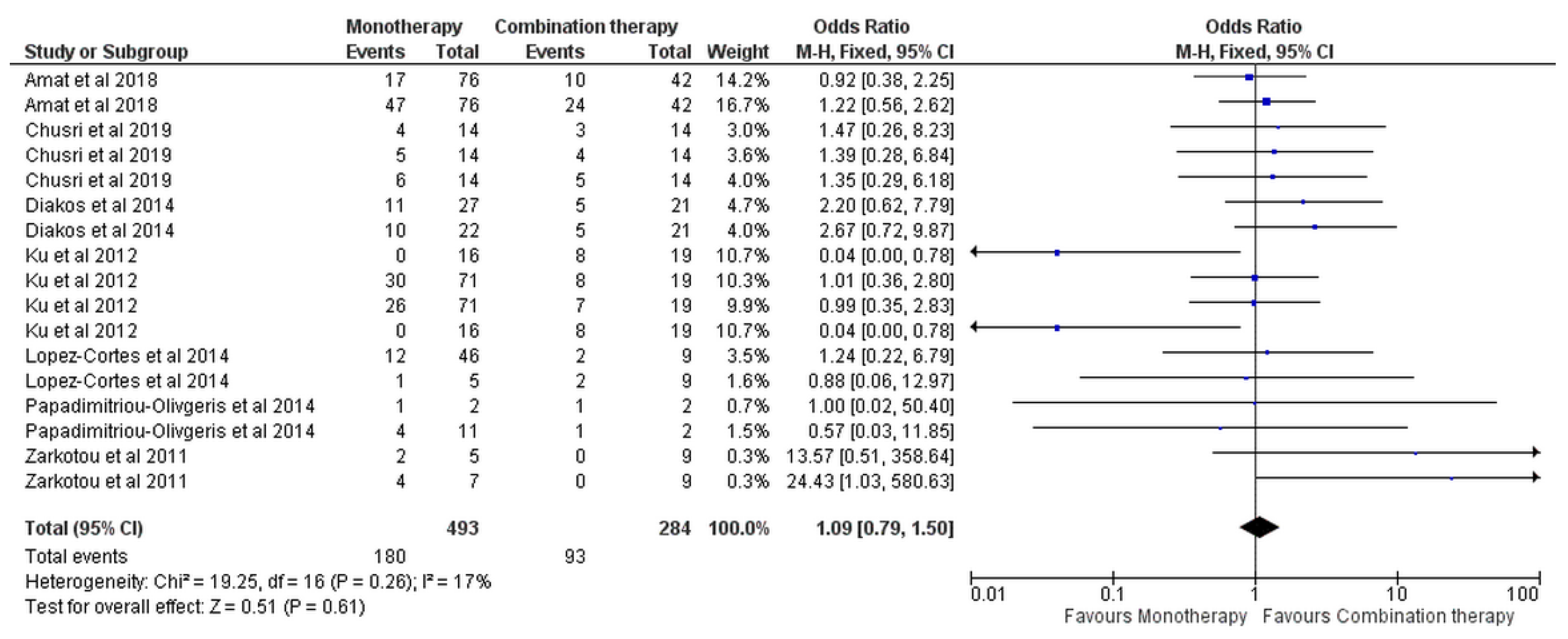
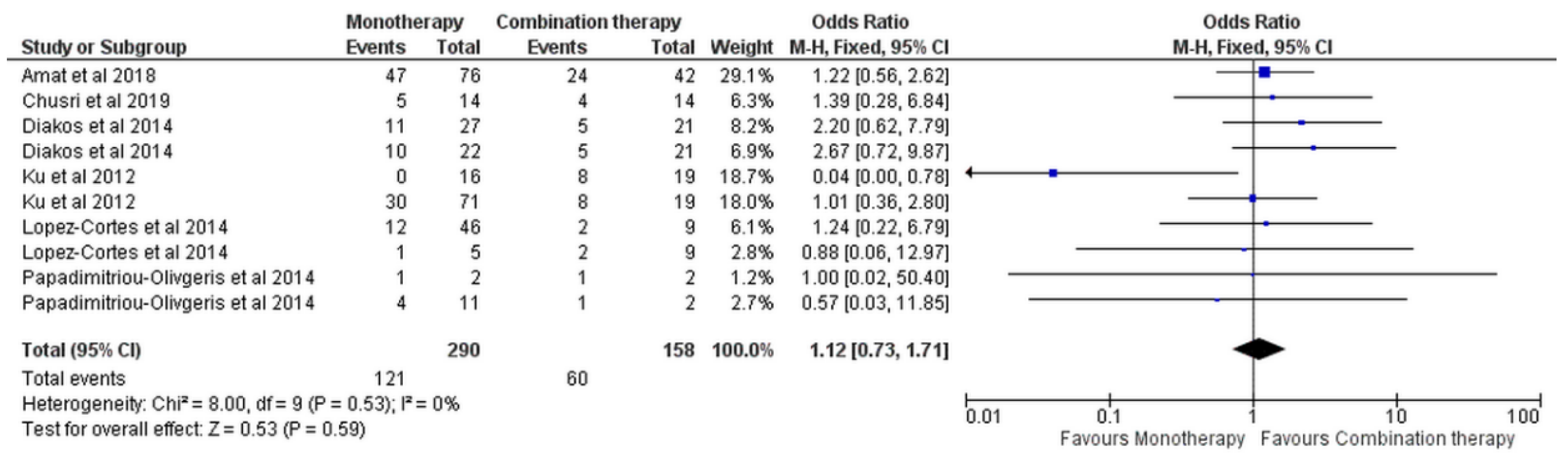
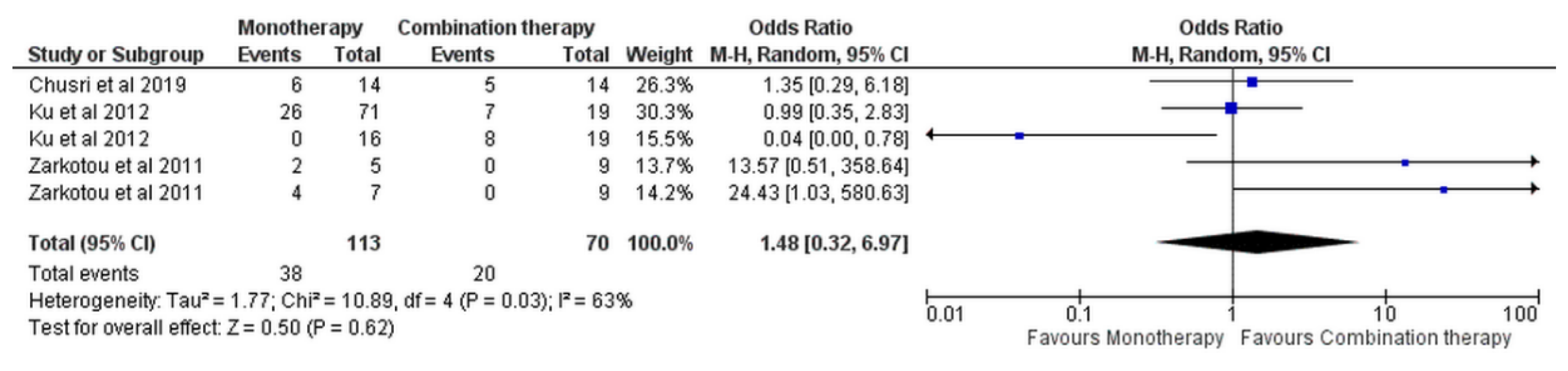
2.3.2. Monotherapy versus Combination Therapy
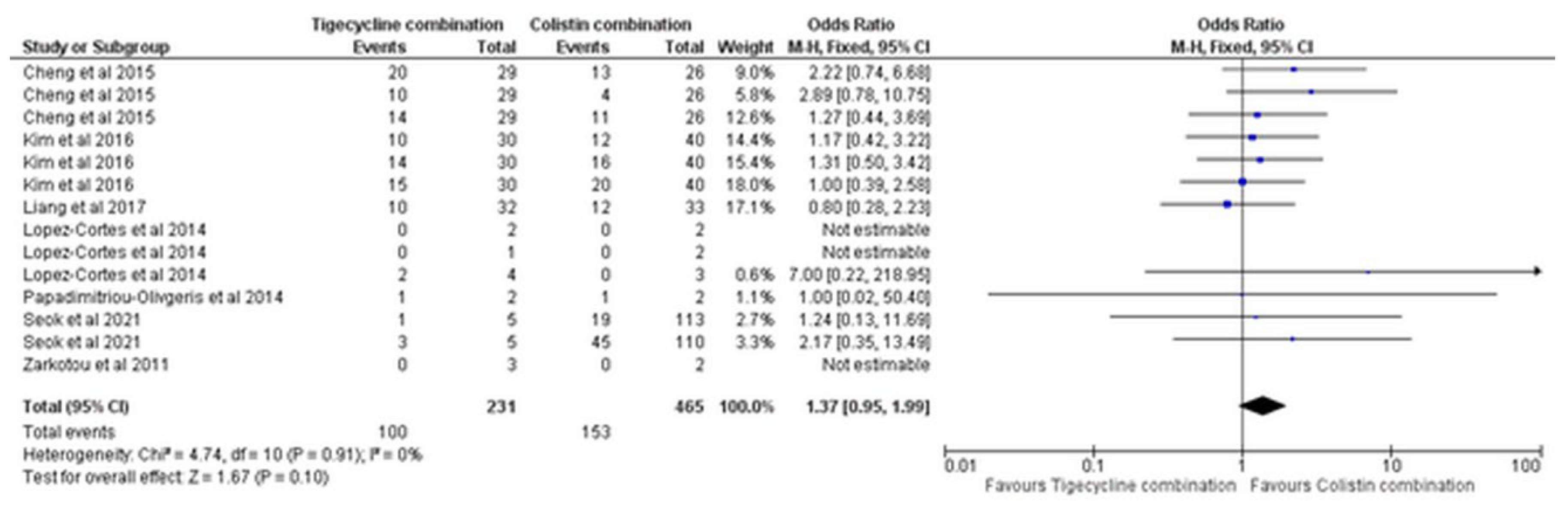
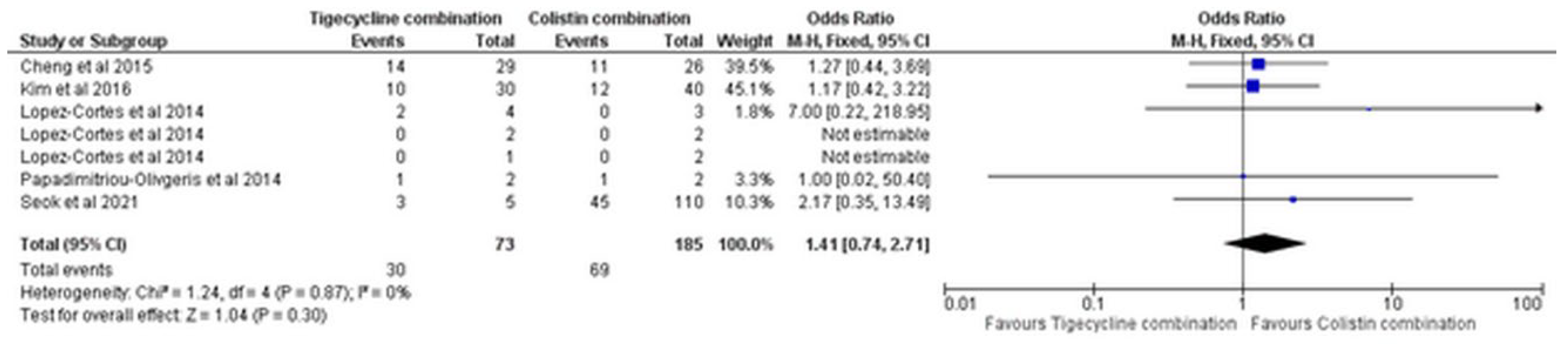
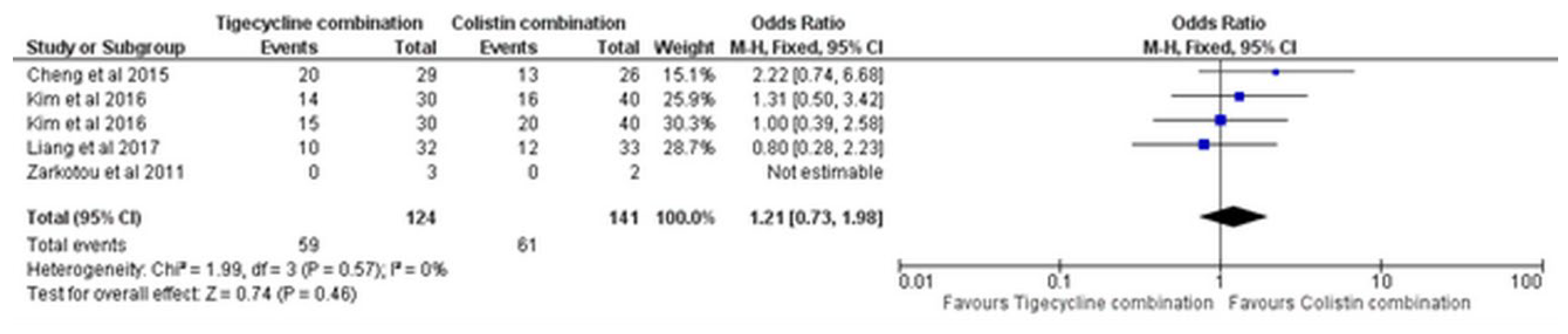
2.3.3. Tigecycline Combination versus Colistin Combination
2.3.4. Subgroup Analysis
Tigecycline Monotherapy versus Colistin Monotherapy
Monotherapy versus Combination Therapy
Tigecycline Combination versus Colistin Combination
2.4. Quality of Evidence
3. Discussion
4. Materials and Methods
4.1. Literature Search Strategy
4.2. Study Selection and Data Extraction
4.3. Outcomes of Meta-Analysis
4.4. Risk of Bias Assessment
4.5. Statistical Analysis
4.6. Quality of Evidence
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonomo, R.A.; Szabo, D. Mechanisms of multidrug resistance in Acinetobacter species and Pseudomonas aeruginosa. Clin. Infect. Dis. 2006, 43 (Suppl. S2), S49–S56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-Negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Ellis, P.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; Wood, G.; Kumar, A.; Simon, D.; et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Bavaro, D.F.; Belati, A.; Diella, L.; Stufano, M.; Romanelli, F.; Scalone, L.; Stolfa, S.; Ronga, L.; Maurmo, L.; Dell’Aera, M.; et al. Cefiderocol-Based Combination Therapy for “Difficult-to-Treat” Gram-Negative Severe Infections: Real-Life Case Series and Future Perspectives. Antibiotics 2021, 10, 652. [Google Scholar] [CrossRef]
- Daikos, G.L.; Tsaousi, S.; Tzouvelekis, L.S.; Anyfantis, I.; Psichogiou, M.; Argyropoulou, A.; Stefanou, I.; Sypsa, V.; Miriagou, V.; Nepka, M.; et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: Lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrob. Agents Chemother. 2014, 58, 2322–2328. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: An open-label, randomised controlled trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef]
- Fluit, A.C.; Florijn, A.; Verhoef, J.; Milatovic, D. Presence of tetracycline resistance determinants and susceptibility to tigecycline and minocycline. Antimicrob. Agents Chemother. 2005, 49, 1636–1638. [Google Scholar] [CrossRef] [Green Version]
- FDA Drug Safety Communication: Increased Risk of Death with Tygacil (tigecycline) Compared to Other Antibiotics Used to Treat Similar Infections. Available online: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-increased-risk-death-tygacil-tigecycline-compared-other-antibiotics (accessed on 21 October 2021).
- Bassetti, M.; Poulakou, G.; Giamarellou, H. Is there a future for tigecycline? Intensive Care Med. 2014, 40, 1039–1045. [Google Scholar] [CrossRef]
- Oliveira, P.R.; Carvalho, V.C.; Saconi, E.S.; Leonhardt, M.C.; Kojima, K.E.; Santos, J.S.; Rossi, F.; Lima, A.L.L.M. Tigecycline Versus Colistin in the Treatment of Carbapenem-resistant Acinetobacter baumannii Complex Osteomyelitis. J. Bone Jt. Infect. 2020, 5, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Chusri, S.; Singkhamanan, K.; Wanitsuwan, W. Adjunctive therapy of intravenous colistin to intravenous tigecycline for adult patients with non-bacteremic post-surgical intra-abdominal infection due to carbapenem-resistant Acinetobacter baumannii. J. Infect. Chemother. 2019, 25, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Papadimitriou-olivgeris, M.; Marangos, M.; Christofidou, M.; Fligou, F.; Bartzavali, C.; Panteli, E.S.; Vamvakopoulou, S.; Filos, K.S.; Anastassiou, E.D. Risk factors for infection and predictors of mortality among patients with KPC-producing Klebsiella pneumoniae bloodstream infections in the intensive care unit. Scand. J. Infect. Dis. 2014, 46, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Ku, K.; Pogue, J.M.; Moshos, J.; Bheemreddy, S.; Wang, Y.; Bhargava, A.; Campbell, M.; Khandker, N.; Lephart, P.R.; Chopra, T.; et al. Retrospective evaluation of colistin versus tigecycline for the treatment of Acinetobacter baumannii and/or carbapenem-resistant Enterobacteriaceae infections. Am. J. Infect. Control 2012, 40, 983–987. [Google Scholar] [CrossRef]
- Zarkotou, O.; Pournaras, S.; Tselioti, P.; Dragoumanos, V.; Pitiriga, V.; Ranellou, K.; Prekates, A. Predictors of mortality in patients with bloodstream infections caused by KPC-producing Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin. Microbiol. Infect. 2011, 17, 1798–1803. [Google Scholar] [CrossRef] [Green Version]
- Seok, H.; Choi, W.S.; Lee, S.; Moon, C.; Park, D.W.; Song, J.Y.; Cheong, H.J.; Kim, J.; Kim, J.Y.; Park, M.N.; et al. What is the optimal antibiotic treatment strategy for carbapenem-resistant Acinetobacter baumannii (CRAB)? A multicentre study in Korea. J. Glob. Antimicrob. Resist. 2021, 24, 429–439. [Google Scholar] [CrossRef]
- Amat, T.; Gutiérrez-Pizarraya, A.; Machuca, I.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Torre-Giménez, Á.; Garnacho-Montero, J.; Cisneros, J.M.; Torre-Cisneros, J. The combined use of tigecycline with high-dose colistin might not be associated with higher survival in critically ill patients with bacteraemia due to carbapenem-resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, 630–634. [Google Scholar] [CrossRef] [Green Version]
- Liang, C.-A.; Lin, Y.-C.; Lu, P.-L.; Chen, H.-C.; Chang, H.-L.; Sheu, C.-C. Antibiotic strategies and clinical outcomes in critically ill patients with pneumonia caused by carbapenem-resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, 908.e1–908.e7. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.; Moon, J.; Huh, J.W.; Choi, S.; Lim, C. Comparable Efficacy of Tigecycline versus Colistin Therapy for Multidrug-Resistant and Extensively Drug-Resistant Acinetobacter baumannii Pneumonia in Critically Ill Patients. PLoS ONE 2016, 11, e0150642. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Chuang, Y.; Sun, H.; Sheng, W.; Yang, C.; Liao, C.; Hsueh, P.; Yang, J.; Shen, N.; Wang, J.; et al. Excess Mortality Associated With Colistin-Tigecycline Compared with Colistin-Carbapenem Combination Therapy for Extensively Drug-Resistant. Crit. Care Med. 2015, 43, 1194–1204. [Google Scholar] [CrossRef]
- Chuang, Y.-C.; Cheng, C.-Y.; Sheng, W.-H.; Sun, H.-Y.; Wang, J.-T.; Chen, Y.-C.; Chang, S.-C. Effectiveness of tigecycline-based versus colistin-based therapy for treatment of pneumonia caused by multidrug-resistant Acinetobacter baumanniiin a critical setting: A matched cohort analysis. BMC Infect. Dis. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.H.; Ahn, H.L.; Han, O.Y.; La, H.O. Efficacy and Safety Profile Comparison of Colistin and Tigecycline on the Extensively Drug Resistant Acinetobacter baumannii. Biol. Pharm. Bull. 2014, 37, 340–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ló Pez-Corté, L.E.; Cisneros, J.M.; Ferná Ndez-Cuenca, F.; Bou, G.; Tomá, S.M.; Garnacho-Montero, J.; Pascual, A.; Martínez-Martínez, L.; Vila, J.; Pachó, J.; et al. Monotherapy versus combination therapy for sepsis due to multidrug-resistant Acinetobacter baumannii: Analysis of a multicentre prospective cohort. J. Antimicrob. Chemother. 2014, 69, 3119–3126. [Google Scholar] [CrossRef] [Green Version]
- Kengkla, K.; Kongpakwattana, K.; Saokaew, S.; Apisarnthanarak, A.; Chaiyakunapruk, N. Comparative efficacy and safety of treatment options for MDR and XDR Acinetobacter baumannii infections: A systematic review and network meta-analysis. J. Antimicrob. Chemother. 2018, 73, 22–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garnacho-Montero, J.; Dimopoulos, G.; Poulakou, G.; Akova, M.; Cisneros, J.M.; De Waele, J.; Petrosillo, N.; Seifert, H.; Timsit, J.F.; Vila, J.; et al. Task force on management and prevention of Acinetobacter baumannii infections in the ICU. Intensive Care Med. 2015, 41, 2057–2075. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Wolfensberger, A.; Nemeth, J.; Schreiber, P.W.; Sax, H.; Kuster, S.P. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci. Rep. 2019, 9, 15290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardakas, K.Z.; Mavroudis, A.D.; Georgiou, M.; Falagas, M.E. Intravenous colistin combination antimicrobial treatment vs. monotherapy: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 51, 535–547. [Google Scholar] [CrossRef]
- Mohsen, H.; Haddad, P.; Allam, A.; Hassan, A. Patterns in place of cancer death in the State of Qatar: A population-based study. PLoS ONE 2014, 9, e109615. [Google Scholar] [CrossRef] [Green Version]
- Eljaaly, K.; Bidell, M.R.; Gandhi, R.G.; Alshehri, S.; Enani, M.A.; Al-Jedai, A.; Lee, T.C. Colistin Nephrotoxicity: Meta-Analysis of Randomized Controlled Trials. Open Forum Infect. Dis. 2021, 8, ofab026. [Google Scholar] [CrossRef]
- Doremus, C.; Marcella, S.W.; Cai, B.; Echols, R.M. Utilization of Colistin Versus β-Lactam and β-Lactamase Inhibitor Agents in Relation to Acute Kidney Injury in Patients with Severe Gram-Negative Infections. Infect. Dis. Ther. 2022, 11, 187–199. [Google Scholar] [CrossRef]
- Tzouvelekis, L.S.; Markogiannakis, A.; Piperaki, E.; Souli, M.; Daikos, G.L. Treating infections caused by carbapenemase-producing Enterobacteriaceae. Clin. Microbiol. Infect. 2014, 20, 862–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batirel, A.; Balkan, I.I.; Karabay, O.; Agalar, C.; Akalin, S.; Alici, O.; Alp, E.; Altay, F.A.; Altin, N.; Arslan, F.; et al. Comparison of colistin-carbapenem, colistin-sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. Eur. J. Clin. Microbiol. 2014, 33, 1311–1322. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.-L.; Chen, Y.-H.; Lai, C.-C.; Tang, H.-J. Intravenous Colistin Monotherapy versus Combination Therapy against Carbapenem-Resistant Gram-Negative Bacteria Infections: Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, W.; Han, Y.; Zhao, J.; Wei, C.; Cui, J.; Wang, R.; Liu, Y. Tigecycline treatment experience against multidrug-resistant Acinetobacter baumannii infections: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2016, 47, 107–116. [Google Scholar] [CrossRef]
- Abdallah, M.; Olafisoye, O.; Cortes, C.; Urban, C.; Landman, D.; Quale, J. Activity of eravacycline against Enterobacteriaceae and Acinetobacter baumannii, including multidrug-resistant isolates, from New York City. Antimicrob. Agents Chemother. 2015, 59, 1802–1805. [Google Scholar] [CrossRef] [Green Version]
- Tumbarello, M.; Trecarichi, E.M.; Corona, A.; De Rosa, F.G.; Bassetti, M.; Mussini, C.; Menichetti, F.; Viscoli, C.; Campoli, C.; Venditti, M.; et al. Efficacy of Ceftazidime-Avibactam Salvage Therapy in Patients with Infections Caused by Klebsiella pneumoniae Carbapenemase-producing K. pneumoniae. Clin. Infect. Dis. 2019, 68, 355–364. [Google Scholar] [CrossRef] [Green Version]
- Belati, A.; Bavaro, D.F.; Diella, L.; De Gennaro, N.; Di Gennaro, F.; Saracino, A. Mero-penem/Vaborbactam Plus Aztreonam as a Possible Treatment Strategy for Bloodstream In-fections Caused by Ceftazidime/Avibactam-Resistant Klebsiella pneumoniae: A Retrospective Case Series and Literature Review. Antibiotics 2022, 11, 373. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Abou-Setta, A.M.; Beaupre, L.A.; Jones, C.A. Pain Management Interventions for Hip Fracture; Comparative Effectiveness Reviews, No. 30; Appendix I, Newcastle-Ottawa Scale Assessment of Cohort Studies; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011. [Google Scholar]
- Efthimiou, O. Practical guide to the meta-analysis of rare events. Evid. Based Mental Health 2018, 21, 72–76. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Chicester, UK, 2019. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Chicester, UK, 2020; Version 6.1; Available online: https://training.cochrane.org/handbook/current/chapter-10#_Ref521576299 (accessed on 24 October 2020).
- Abushanab, D.; Al-Badriyeh, D. Efficacy and Safety of Ibuprofen Plus Paracetamol in a Fixed-Dose Combination for Acute Postoperative Pain in Adults: Meta-Analysis and a Trial Sequential Analysis. CNS Drugs 2021, 35, 105–120. [Google Scholar] [CrossRef]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. Handbook for Grading the Quality of Evidence and the Strength of Recommendations Using the GRADE Approach. 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 31 October 2021).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design, Period | Country | Age (Mean ± Standard Deviation or Range), (Tigecycline/Colistin) | Site of Infection | Causative Pathogens | Sample Size (Tigecycline/Colistin) | Concomitant Antibiotics in Tigecycline Group | Concomitant Antibiotics in Colistin Group | Mean Duration of Therapy in Days (Tigecycline vs. Colistin) | Tigecycline Regimen | Colistin Regimen | Clinical Outcomes Reported | Baseline Charlson Comorbidity Index (Tigecycline vs. Colistin) | Major Comorbidities |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Oliveira et al., 2020 | Retrospective cohort study, 2007–2015 | Brazil | 46.8 ± 18.9/40.6 ± 19.1 | Osteomyelitis in non-critically ill patients | CRABc | 31/34 | NA | NA | 42 vs. 42.5 | Continuous dose: 50 mg intravenous every 12 h | Continuous dose: 2.5 mg/kg intravenous every 12 h | Remission, recurrence of infection, in-hospital mortality, liver enzymes abnormalities, renal impairment | Mean (range): 1 (0; 7) vs. 0 (0; 5) | Hypertension, diabetes, neoplasia, rheumatoid arthritis, HIV, immunodeficiency |
| Chusri et al., 2019 | Retrospective cohort study, 2012–2017 | Thailand | 45/46 | IAI in non-and critically ill patients | CRAB | 14/14 | Colistin | NA | 21 vs. 22 | Loading dose: 100 mg Continuous dose:50 mg every 12 h | Loading dose: 5 mg/kg or 300mg Continuous dose: 2.5 mg/kg/dose | Microbiological eradication; mortality at 14 days, 30 days, in hospital mortality; renal complications | NR | NR |
| Amat et al., 2018 | Retrospective cohort study,2010–2012 | Spain | 56 ± 13/58 ± 17 | Mixed in critically ill patients | CRAB | 42/76 | Colistin | NA | 14 vs. 14 | Loading dose 100 mg Continuous dose: 50 mg every 12 h | Continuous dose: 9 million IU every 24 h | Mortality at 14 days and 30 days | Mean (SD): 2.7 ± 2.4 vs. 2.6 ± 1.8 | Diabetes, COPD, immunosuppressed, liver cirrhosis, CKD |
| Liang et al., 2018 | Retrospective cohort study, 2010–2015 | Taiwan | 73.7 (62.8–82.0) (all patients) | Pneumonia in critically ill patients | CRAB- pneumonia | 159/67 | Meropenem, imipenem, sulbactam, colistin | Meropenem, imipenem, sulbactam | 14 vs. 14 | As per Sanford guide | As per Sanford guide | ICU and hospital mortality, treatment failure, recurrence | Total mean (range): 3 (2–4) (all patients) | Acute respiratory failure, septic shock, gastrointestinal bleeding, post operation |
| Kim et al., 2016 | Retrospective cohort study, 2009–2010 | Korea | 72 (64–76)/67 (57–75) | Mixed in critically ill patients | MDR/XDRAB pneumonia | 30/40 | Carbapenem, sulbactam, sulbactam+ minocycline+ rifampicin, rifampicin doxycycline | Carbapenem alone or with combination, sulbactam, rifampicin, sulbactam +rifampicin doxycycline | 11 vs. 12 | Loading dose: 100 mg Continuous dose: 50 mg every 12 h | Loading dose: 5 mg/kg Continuous dose:150 mg every 12 h | Clinical success, microbiology success, recurrence of infection, hospital mortality at 30 day, ICU mortality, in-hospital mortality, nephrotoxicity | NR | Hypertension, chronic pulmonary, kidney, liver diseases, diabetes, cancer, immunodeficiency |
| Cheng et al., 2015 | Prospective cohort, 2010–2013 | Taiwan | 62 vs. 62 | Bacteremia in critically ill patients | XDDRAb | 29/26 | Colistin | Carbapenem | 10 vs. 9 (median) | Loading dose:100 mg Continuous dose: 50 mg every 12 h | 2.5–5 mg/kg/day divided every 8 or 12 h | All cause mortality at 14 days, all cause in-hospital mortality, 30 days and on discharge, nephrotoxicity | median (IQR): 4 (3–5) vs. 3 (1–6) | CLD, CKD, lung, diseases, cancer, diabetes, stroke, liver cirrhosis, transplantation, CHF |
| Chuang et al., 2014 | Retrospective cohort study, 2009–2010 | Taiwan | 63.8 ± 17.9/63.7 ± 19.5 | Mixed in critically ill patient | MDRAB pneumonia | 175/119 | Aminoglycoside, sarbapenem, sulbactam | Aminoglycoside, sarbapenem, sulbactam | 13.1 vs. 14.6 | Loading dose: 100 mg Continuous dose:50 mg every 12 h. | 2.5–5 mg/kg/day divided doses every 8 or 12 h | In-hospital mortality, nephrotoxicity | NR | CVD, diabetes, CKD, liver cirrhosis, CLD, cancer, immunosuppressed |
| Daikos et al., 2014 | Retrospective cohort study, 2009–2010 | Greece | 62.7 ± 17.5 (all patients) | BSI, non- andcritically ill patients | CP-Kp | NR | Aminoglycoside, carbapenem | Aminoglycoside carbapenem | NR | 100–200 mg every 12h | 9 million IU every 8–12 h | All-cause mortality at 28 day | NR | Neutropenia, sepsis |
| Kwon et al., 2014 | Retrospective cohort study, 2009–2010 | Korea | 60.1 ± 12.3/59.0 ± 19.2 | Mixed in non- and critically ill patients | XDRAB | 16/39 | NA | NA | 13 vs. 15 | 50–100 mg every 24 h | 75–300 mg every 24 h | Clinical success, in-hospital mortality, side effects as nephrotoxicity | NR | Hypertension, kidney and liver diseases, diabetes, tuberculosis |
| Lopez-Cortes et al., 2014 | Prospective cohort study, 2010 | Spain | 60 (52–75) (all patients, median (IQR)) | Mixed in non- and critically ill patients | MDRAB | 5/46 (monotherapy) 22/23 (combination) | Colistin, carbapenem, aminoglycoside, rifampicin | Tigecycline, carbapenem, sulbactam, aminoglycoside | NR | NR | NR | Mortality at 14 and 30 day | NR | Diabetes, CLD, cancer, dialysis, immunodeficiency |
| Papadimitriou-Olivgeris et al., 2014 | Retrospective cohort study, NA | Greece | 55.2 ± 19.3 (all patients) | BSI in critically ill patients | KPC-Kp | 16\93 | NR | NR | NR | NR | NR | Mortality at 30 day | NR | Diabetes, COPD, cancer, CVD and CKD |
| Ku et al., 2012 | Retrospective study, 2009 | USA | 56.9 ± 19.1/60.2 ± 18.3 | Mixed in non- and critically ill patients | CRE | 16/71 monotherapy 19 (colistin-tigecycline combination) | Colistin | Tigecycline | 8.6 vs.. 8.3 | NR | NR | In hospital mortality and mortality in 3 months | Mean (SD): 3.4 ± 3.1 vs. 3.5 ± 3 | Diabetes, CVD. CLD, cancer, chronic liver disease, neurologic disease, |
| Zarkotou et al., 2011 | Prospective cohort study, 2008–2010 | Greece | 63.8 ± 19.9 (all patients) | BSI in non- and critically ill patients | KPC-Kp | 5/7 (monotherapy) 17/2 (combination) | Colistin, gentamicin, carbapenem, amikacin | Gentamicin | NR | NR | NR | Microbiological response, failure, and Indeterminate, mortality in 14 days and all-cause in-hospital mortality, BSI-mortality | NR | NR |
| Seok et al., 2021 | Prospective cohort study, 2015–2016 | Korea | 67.0 ± 14.9 (all patients) | Mixed in critically ill patients | CRAB | 12/171 | NA | Carbapenem, minocycline, rifampin, sulbactam, | NA | NA | NA | Mortality at 7 and 28-day, clinical success, microbiocidal response at 14 and 28-day, nephrotoxicity and hepatoxicity | NA | Diabetes, CVD, neuromuscular diseases, CKD, liver disease, COPD, asthma, transplantation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abushanab, D.; Nasr, Z.G.; Al-Badriyeh, D. Efficacy and Safety of Colistin versus Tigecycline for Multi-Drug-Resistant and Extensively Drug-Resistant Gram-Negative Pathogens—A Meta-Analysis. Antibiotics 2022, 11, 1630. https://doi.org/10.3390/antibiotics11111630
Abushanab D, Nasr ZG, Al-Badriyeh D. Efficacy and Safety of Colistin versus Tigecycline for Multi-Drug-Resistant and Extensively Drug-Resistant Gram-Negative Pathogens—A Meta-Analysis. Antibiotics. 2022; 11(11):1630. https://doi.org/10.3390/antibiotics11111630
Chicago/Turabian StyleAbushanab, Dina, Ziad G. Nasr, and Daoud Al-Badriyeh. 2022. "Efficacy and Safety of Colistin versus Tigecycline for Multi-Drug-Resistant and Extensively Drug-Resistant Gram-Negative Pathogens—A Meta-Analysis" Antibiotics 11, no. 11: 1630. https://doi.org/10.3390/antibiotics11111630