
Antibiotics to Prevent Surgical Site Infection (SSI) in Oral Surgery: Survey among Italian Dentists

 , , , and
, , , and
Abstract
:1. Introduction
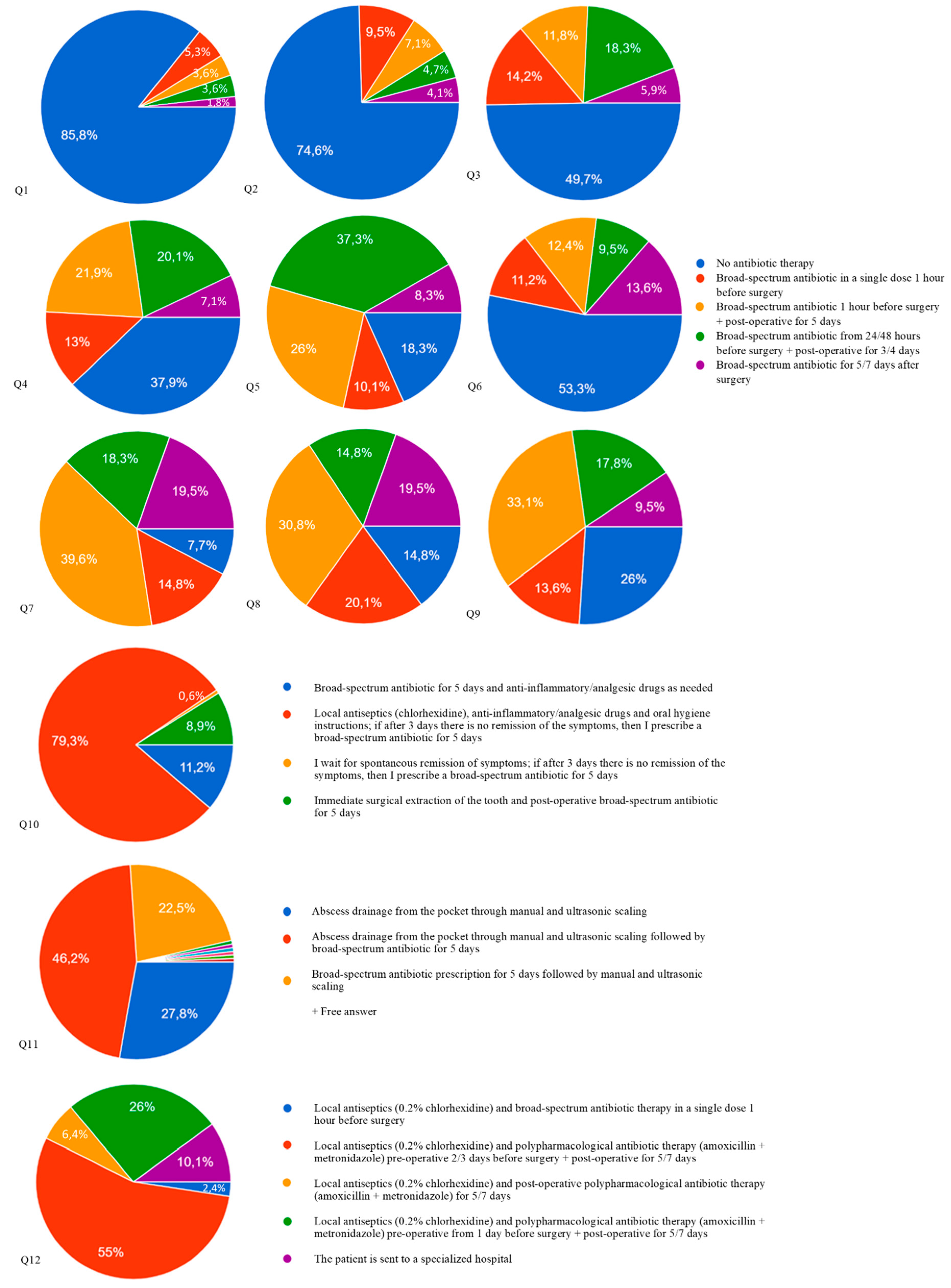
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oberoi, S.S.; Dhingra, C.; Sharma, G.; Sardana, D. Antibiotics in dental practice: How justified are we. Int. Dent. J. 2015, 65, 4–10. [Google Scholar] [CrossRef] [PubMed]
- D′Agostino, S.; Dolci, M. Antibiotic therapy in oral surgery: A cross sectional survey among Italian dentists. J. Biol. Regul. Homeost. Agents. 2020, 34, 1549–1552. [Google Scholar]
- Tebano, G.; Dyar, O.J.; Beovic, B.; Béraud, G.; Thilly, N.; Pulcini, C. ESCMID Study Group for Antimicrobial stewardship (ESGAP). Defensive medicine among antibiotic stewards: The international ESCMID AntibioLegalMap survey. J. Antimicrob. Chemother. 2018, 73, 1989–1996. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net)-Annual Epidemiological Report 2019; ECDC: Stockholm, Sweden, 2020.
- Bratzler, D.W.; Dellinger, E.P.; Olsen, K.M.; Perl, T.M.; Auwaerter, P.G.; Bolon, M.K.; Fish, D.N.; Napolitano, L.M.; Sawyer, R.G.; Slain, D.; et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am. J. Health Syst. Pharm. 2013, 70, 195–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enzler, M.J.; Berbari, E.; Osmon, D.R. Antimicrobial prophylaxis in adults. Mayo Clin. Proc. 2011, 86, 686–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, W.; Williams, D.; Pulcini, C.; Sanderson, S.; Calfon, P.; Verma, M. The Essential Role of the Dental Team in Reducing Antibiotic Resistance; FDI World Dental Federation: Geneva, Italy, 2020. [Google Scholar]
- The Medicines Utilisation Monitoring Centre. National Report on Antibiotics Use in Italy; Italian Medicines Agency: Rome, Italy, 2020. [Google Scholar]
- Della Polla, G.; Bianco, A.; Mazzea, S.; Napolitano, F.; Angelillo, I.F. Preoperative Antibiotic Prophylaxis in Elective Minor Surgical Procedures among Adults in Southern Italy. Antibiotics 2020, 9, 713. [Google Scholar] [CrossRef]
- Walsh, L.J.; Ford, P.J.; McGuire, T.; van Driel, M.; Hollingworth, S.A. Trends in Australian dental prescribing of antibiotics: 2005–2016. Aust Dent. J. 2021, 23, 1–5. [Google Scholar]
- Carlet, J.; Collignon, P.; Goldmann, D.; Goossens, H.; Gyssens, I.C.; Harbarth, S.; Jarlier, V.; Levy, S.B.; N’Doye, B.; Pittet, D.; et al. Society’s failure to protect a precious resource: Antibiotics. Lancet 2011, 378, 369–371. [Google Scholar] [CrossRef]
- Barone, A.; Chatelain, S.; Derchi, G.; Di Spirito, F.; Martuscelli, R.; Porzio, M.; Sbordone, L. Antibiotic’s effectiveness after erupted tooth extractions: A retrospective study. Oral Dis. 2020, 26, 967–973. [Google Scholar] [CrossRef]
- Cinquini, C.; Marchionni, S.; Derchi, G.; Miccoli, M.; Gabriele, M.; Barone, A. Non-impacted tooth extractions and antibiotic treatment: A RCT study. Oral Dis. 2021, 27, 1042–1051. [Google Scholar] [CrossRef]
- Wilson, W.; Taubert, K.A.; Gewitz, M.; Lockhart, P.B.; Baddour, L.M.; Levison, M.; Bolger, A.; Cabell, C.H.; Takahashi, M.; Baltimore, R.S. Prevention of infective endocarditis: Guidelines from the American Heart Association: A guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 2007, 116, 1736–1754. [Google Scholar] [PubMed] [Green Version]
- Thornhill, M.H.; Gibson, T.B.; Cutler, E.; Dayer, M.J.; Chu, V.H.; Lockhart, P.B.; O′Gara, P.T.; Baddour, L.M. Antibiotic Prophylaxis and Incidence of Endocarditis Before and After the 2007 AHA Recommendations. J. Am. Coll. Cardiol. 2018, 72, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.J.; Calip, G.S.; Zhou, J.; Rowan, S.; Gross, A.E.; Hershow, R.C.; Perez, R.I.; McGregor, J.C.; Evans, C.T. Assessment of the Appropriateness of Antibiotic Prescriptions for Infection Prophylaxis Before Dental Procedures, 2011 to 2015. JAMA Netw. Open. 2019, 2, e193909. [Google Scholar] [CrossRef] [Green Version]
- Arteagoitia, I.; Ramos, E.; Santamaria, G.; Barbier, L.; Alvarez, J.; Santamaria, J. Amoxicillin/clavulanic acid 2000/125 mg to prevent complications due to infection following completely bone-impacted lower third molar removal: A clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 8–16. [Google Scholar] [CrossRef]
- Kamolratanakul, P.; Jansisyanont, P. A review of antibiotic prophylaxis protocols in oral and maxillofacial surgery. J. Oral Maxillofac. Surg. Med. Pathol. 2018, 30, 395–404. [Google Scholar] [CrossRef]
- Lodi, G.; Azzi, L.; Varoni, E.M.; Pentenero, M.; Del Fabbro, M.; Carrassi, A.; Sardella, A.; Manfredi, M. Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst Rev. 2021, 2, CD003811. [Google Scholar]
- Sancho-Puchades, M.; Herráez-Vilas, J.M.; Berini-Aytés, L.; Gay-Escoda, C. Antibiotic prophylaxis to prevent local infection in Oral Surgery: Use or abuse? Med. Oral Patol. Oral Cir. Bucal. 2009, 14, E28–E33. [Google Scholar] [PubMed]
- Romandini, M.; De Tullio, I.; Congedi, F.; Kalemaj, Z.; D’Ambrosio, M.; Laforí, A.; Quaranta, C.; Buti, J.; Perfetti, G. Antibiotic prophylaxis at dental implant placement: Which is the best protocol? A systematic review and network meta-analysis. J. Clin. Periodontol. 2019, 46, 382–395. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database Syst. Rev. 2013, 7, CD004152. [Google Scholar] [CrossRef]
- Rodríguez Sánchez, F.; Rodríguez Andrés, C.; Arteagoitia, I. Which antibiotic regimen prevents implant failure or infection after dental implant surgery? A systematic review and meta-analysis. J. Craniomaxillofac. Surg. 2018, 46, 722–736. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Sánchez, F.; Arteagoitia, I.; Rodríguez Andrés, C.; Caiazzo, A. Antibiotic prophylaxis habits in oral implant surgery among dentists in Italy: A cross-sectional survey. BMC Oral Health. 2019, 19, 265. [Google Scholar] [CrossRef]
- Rodríguez Sánchez, F.; Arteagoitia, I.; Rodríguez Andrés, C.; Bruers, J. Antibiotic prophylaxis prescribing habits in oral implant surgery in the Netherlands: A cross-sectional survey. BMC Oral Health. 2019, 19, 281. [Google Scholar] [CrossRef] [Green Version]
- Arteagoitia, I.; Rodríguez-Andrés, C.; Rodríguez-Sánchez, F. Antibiotic prophylaxis habits in dental implant surgery among dentists in Spain. A cross-sectional survey. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e608–e618. [Google Scholar] [CrossRef]
- Lund, B.; Hultin, M.; Tranaeus, S.; Naimi-Akbar, A.; Klinge, B. Complex systematic review-Perioperative antibiotics in conjunction with dental implant placement. Clin. Oral Implants Res. 2015, 26 (Suppl. S11), 1–14. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Passi, L.; Moretti, R. Retrospective analysis of 736 implants inserted without antibiotic therapy. J. Oral Maxillofac. Surg. 2007, 65, 2321–2323. [Google Scholar] [CrossRef] [PubMed]
- Bernabeu-Mira, J.C.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Prescription of Antibiotic Prophylaxis for Dental Implant Surgery in Healthy Patients: A Systematic Review of Survey-Based Studies. Front Pharmacol. 2021, 11, 588333. [Google Scholar] [CrossRef]
- Martin, E.T.; Kaye, K.S.; Knott, C.; Nguyen, H.; Santarossa, M.; Evans, R.; Bertran, E.; Jaber, L. Diabetes and Risk of Surgical Site Infection: A Systematic Review and Meta-analysis. Infect. Control Hosp. Epidemiol. 2016, 37, 88–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barasch, A.; Safford, M.M.; Litaker, M.S.; Gilbert, G.H. Risk factors for oral postoperative infection in patients with diabetes. Spec. Care Dentist 2008, 28, 159–166. [Google Scholar] [CrossRef]
- Krishnan, B.; Prasad, G.A.; Saravanan, R.; Madhan, B.; Kadhiravan, T. Do preoperative glycosylated hemoglobin (HbA1C) and random blood glucose levels predict wound healing complications following exodontia in type 2 diabetes mellitus patients?-a prospective observational study. Clin. Oral Investig. 2021, 25, 179–185. [Google Scholar] [CrossRef]
- Power, D.J.; Sambrook, P.J.; Goss, A.N. The healing of dental extraction sockets in insulin-dependent diabetic patients: A prospective controlled observational study. Aust. Dent. J. 2019, 64, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Dar-Odeh, N.S.; Abu-Hammad, O.A.; Al-Omiri, M.K.; Khraisat, A.S.; Shehabi, A.A. Antibiotic prescribing practices by dentists: A review. Ther. Clin. Risk Manag. 2010, 6, 301–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura-Egea, J.J.; Gould, K.; Şen, B.H.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjäderhane, L.; Dummer, P.M.H. European Society of Endodontology position statement: The use of antibiotics in endodontics. Int. Endod. J. 2018, 51, 20–25. [Google Scholar] [CrossRef] [Green Version]
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. [Google Scholar] [CrossRef]
- Khouly, I.; Braun, R.S.; Silvestre, T.; Musa, W.; Miron, R.J.; Demyati, A. Efficacy of antibiotic prophylaxis in intraoral bone grafting procedures: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 250–263. [Google Scholar] [CrossRef] [PubMed]
- Klinge, A.; Khalil, D.; Klinge, B.; Lund, B.; Naimi-Akbar, A.; Tranaeus, S.; Hultin, M. Prophylactic antibiotics for staged bone augmentation in implant dentistry. Acta Odontol. Scand. 2020, 78, 64–73. [Google Scholar] [CrossRef] [Green Version]
- Salgado-Peralvo, A.O.; Mateos-Moreno, M.V.; Velasco-Ortega, E.; Peña-Cardelles, J.F.; Kewalramani, N. Preventive antibiotic therapy in bone augmentation procedures in oral implantology: A systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 22, S2468–S7855. [Google Scholar]
- Chrcanovic, B.R.; Martins, M.D.; Wennerberg, A. Immediate placement of implants into infected sites: A systematic review. Clin Implant Dent. Relat. Res. 2015, 17 (Suppl. S1), e1–e16. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N° | % | ||
|---|---|---|---|
| Gender | Male | 120 | 71 |
| Female | 49 | 29 | |
| Educational qualification | Degree in Dentistry | 140 | 82.84 |
| Degree in Medicine and Surgery specialized in Odontostomatology | 20 | 11.83 | |
| Degree in Medicine and Surgery | 9 | 5.33 | |
| Years of professional experience | <5 | 33 | 19.53 |
| 5–10 | 46 | 27.22 | |
| 10–15 | 13 | 7.69 | |
| >15 | 77 | 45.56 | |
| Dental speciality | Oral surgery | 43 | 25.44 |
| Orthodontics | 8 | 4.73 | |
| Pediatric Dentistry | 4 | 2.37 | |
| None | 117 | 69.23 | |
| Region | Northern Italy | 40 | 23.67 |
| Central Italy | 95 | 56.21 | |
| Southern and Insular Italy | 34 | 20.12 | |
| Employment | Private practice | 103 | 60.95 |
| Hospital clinic | 12 | 7.1 | |
| Both | 54 | 31.95 |
| Question | Answer | % |
|---|---|---|
| C1 | Always, even with no visible plaque and calculus deposits | 27.8 |
| Only in case of abundant plaque and calculus deposits | 57.4 | |
| Not always, even in case of abundant plaque and calculus deposits | 14.2 | |
| Never | 0.6 | |
| C2 | Yes | 57.4 |
| No | 42.6 | |
| C3 | Yes | 17.8 |
| No | 82.2 | |
| C4 | Yes | 83.4 |
| No | 16.6 | |
| C5 | Yes | 42.6 |
| No | 57.4 | |
| C6 | Yes | 54.4 |
| No | 45.6 | |
| C8 | Yes | 74.6 |
| No | 25.4 | |
| C9 | Yes, I feel very informed | 26.6 |
| I am quite informed but I feel the need to further master this issue | 66.9 | |
| I think I am not adequately informed | 6.5 | |
| C10 | Not so widespread | 5.3 |
| Medium widespread | 26 | |
| Very widespread | 47.3 | |
| Extremely widespread | 21.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lollobrigida, M.; Pingitore, G.; Lamazza, L.; Mazzucchi, G.; Serafini, G.; De Biase, A. Antibiotics to Prevent Surgical Site Infection (SSI) in Oral Surgery: Survey among Italian Dentists. Antibiotics 2021, 10, 949. https://doi.org/10.3390/antibiotics10080949
Lollobrigida M, Pingitore G, Lamazza L, Mazzucchi G, Serafini G, De Biase A. Antibiotics to Prevent Surgical Site Infection (SSI) in Oral Surgery: Survey among Italian Dentists. Antibiotics. 2021; 10(8):949. https://doi.org/10.3390/antibiotics10080949
Chicago/Turabian StyleLollobrigida, Marco, Gianluca Pingitore, Luca Lamazza, Giulia Mazzucchi, Giorgio Serafini, and Alberto De Biase. 2021. "Antibiotics to Prevent Surgical Site Infection (SSI) in Oral Surgery: Survey among Italian Dentists" Antibiotics 10, no. 8: 949. https://doi.org/10.3390/antibiotics10080949