Recent Trends in Biosensing and Diagnostic Methods for Novel Cancer Biomarkers

 , and
, and
Abstract
:1. Introduction
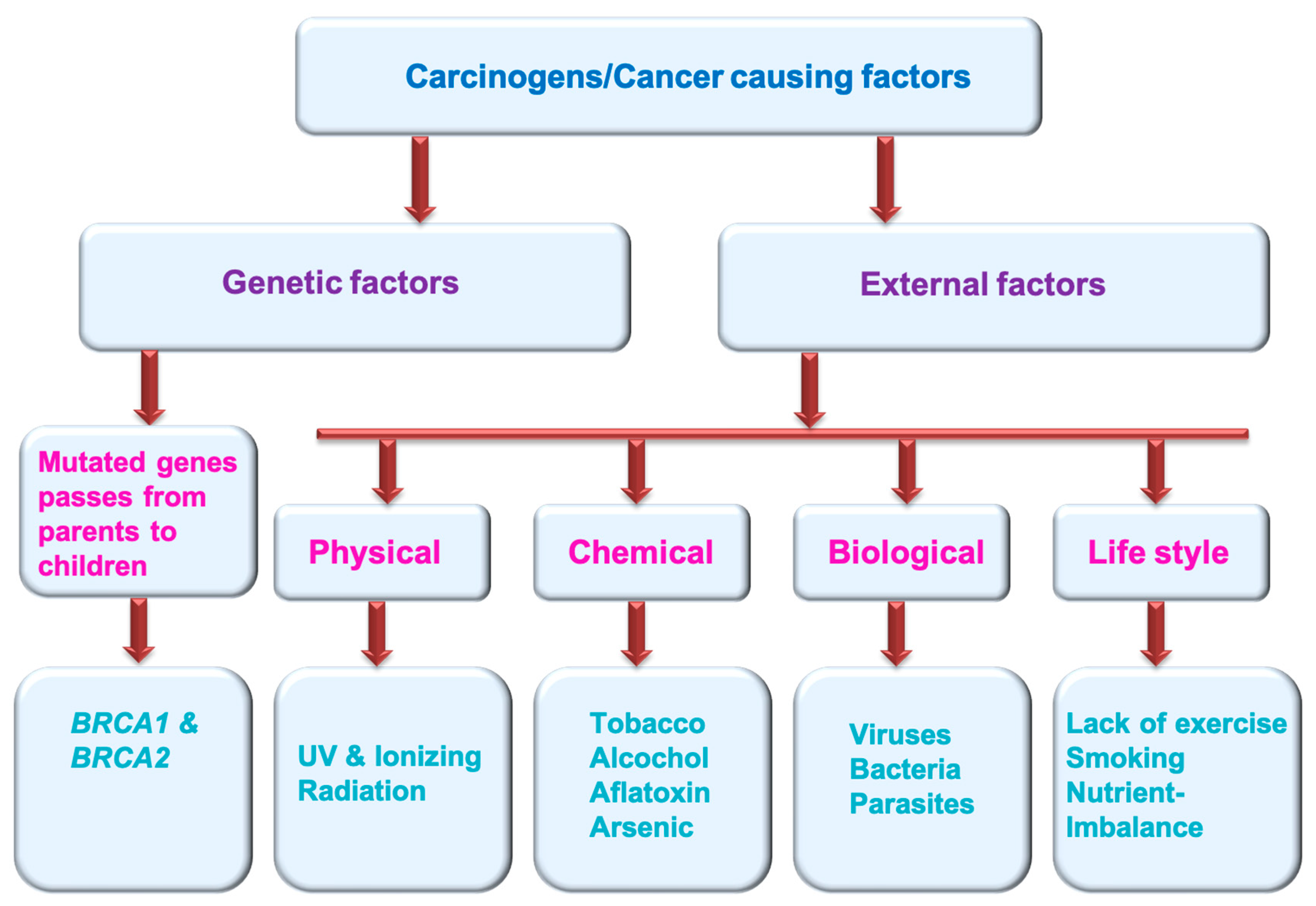
1.1. Cancer
1.2. Importance of Cancer Diagnostics
1.3. Traditional Screening Techniques
1.3.1. Advantages of Traditional Cancer Screening
- It can help to detect the cancer before it spreads, when it is easier to treat.
- It can provide an advantage of early detection, which might lead to lesser recovery time and no intense treatment.
- It can provide a better chance of survival.
- It offers flexibility to start early treatment before symptoms appear.
1.3.2. Limitations of Traditional Cancer Screening
- Sometimes a false-positive test result suggests a cancer-positive status, even though no cancer is present.
- Sometimes false-negative test results may not detect cancer, even though it is present.
- Some screening tests might lead to more detection tests and procedures that can be painful.
- Over-diagnosis causes needless anxiety.
- Some screenings might cause potential issues (e.g., colon cancer screening may cause tear in colon lining).
- These screening methods are high cost.
2. Cancer Biomarkers
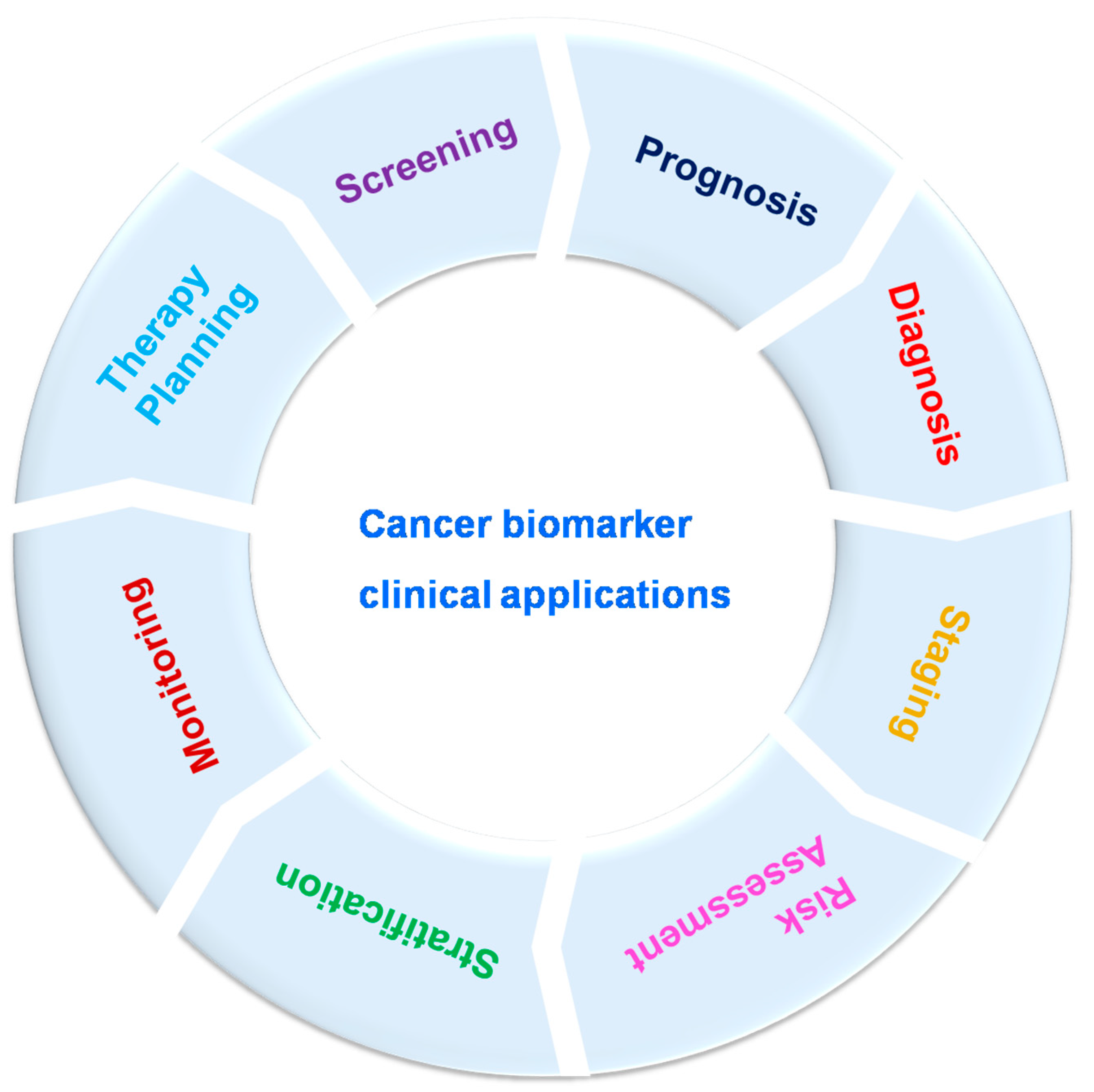
2.1. Clinical Significance of Cancer Biomarkers
2.2. Identification of Novel Cancer Biomarkers
2.3. Cancer Biomarkers Currently Used in Clinical Settings
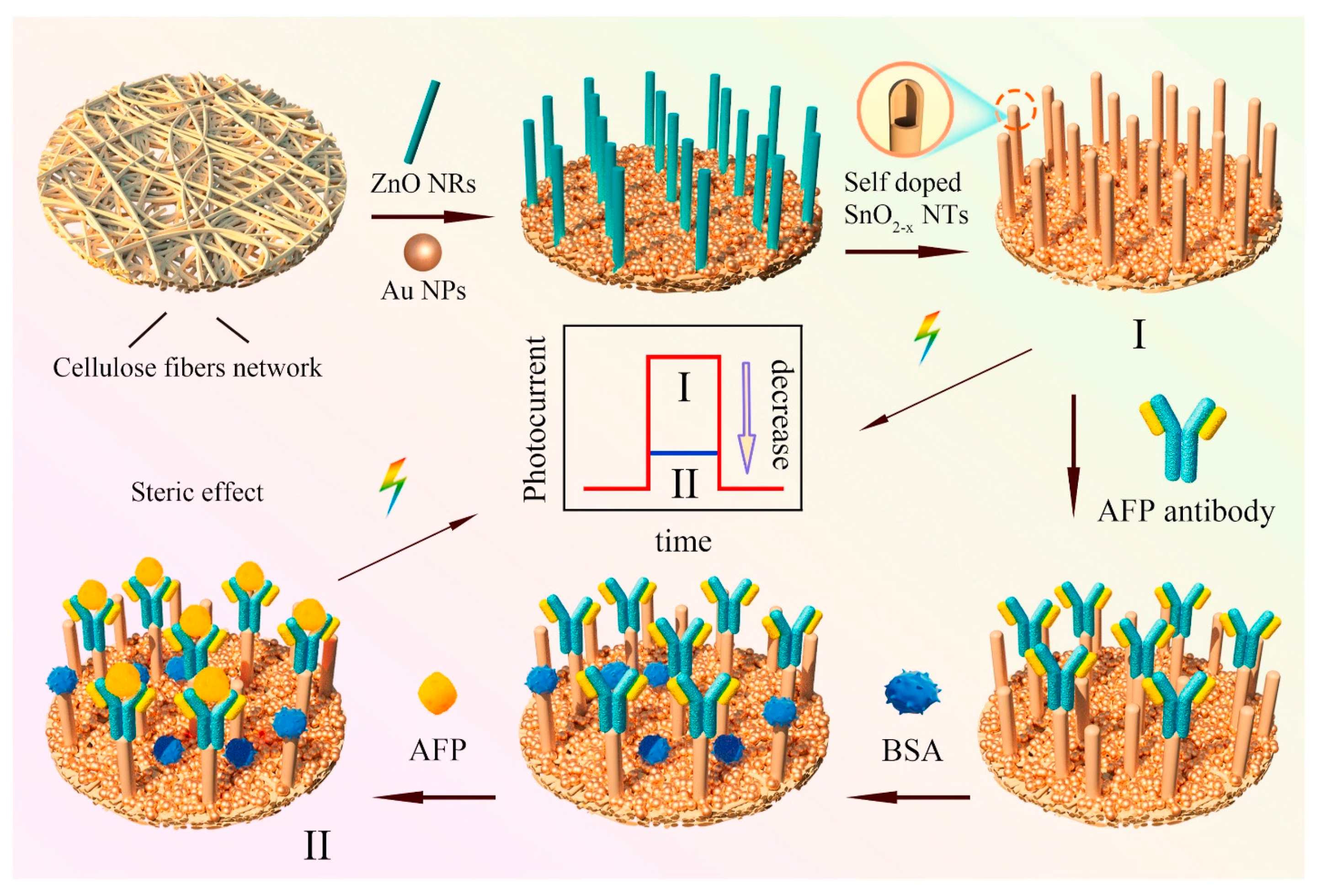
2.3.1. AFP (Alpha-Fetoprotein)
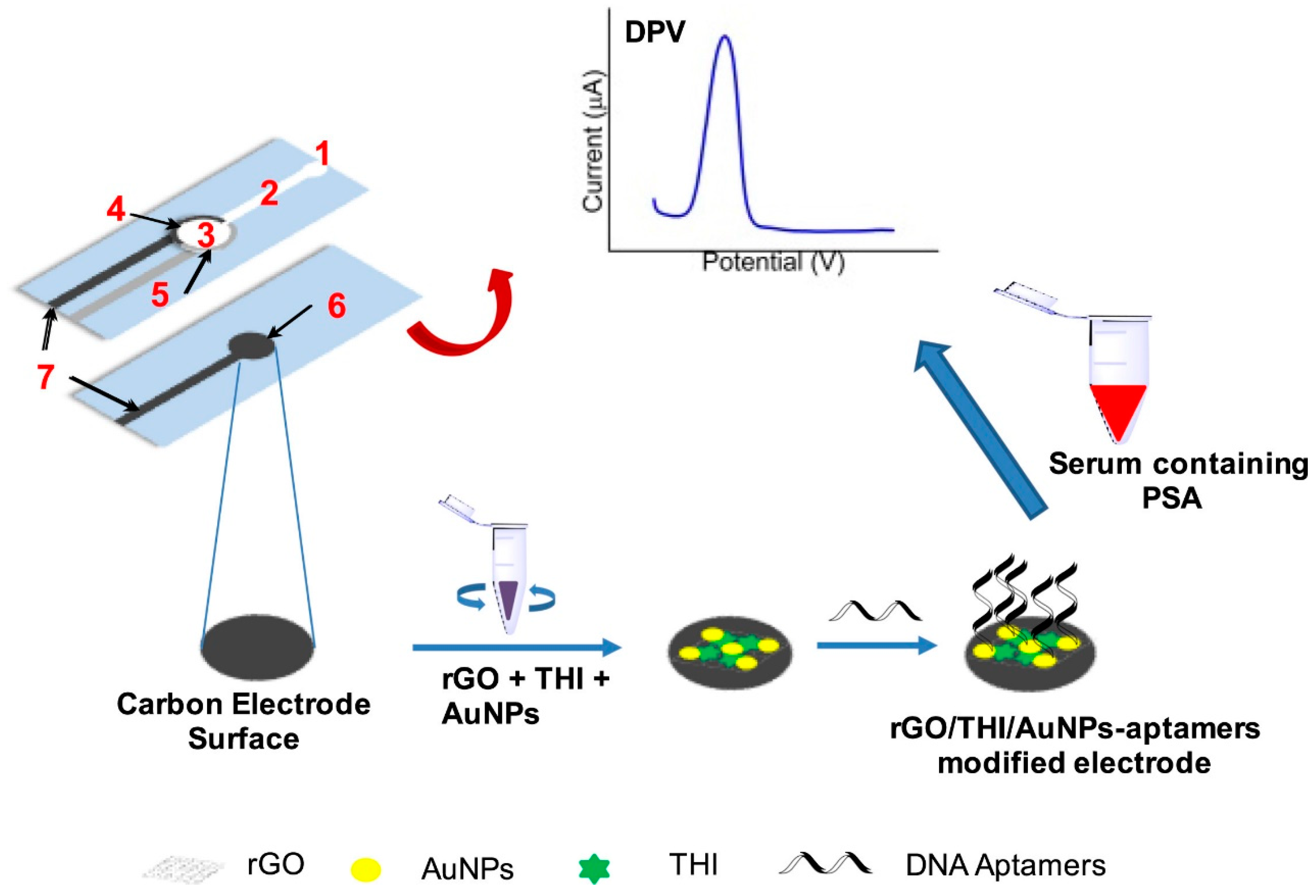
2.3.2. PSA (Prostate Specific Antigen)
2.3.3. RCAS1 (Receptor-Binding Cancer Antigen)
2.3.4. CA 15-3 (Cancer Antigen 15-3)
2.3.5. Cancer–Testis (CT) Antigens
2.3.6. CA 125
2.3.7. CA 19-9
2.3.8. Nse (Neuron-Specific Enolase)
2.3.9. Tdt (Terminal Deoxynucleotidyl Transferase)
2.3.10. CYFRA21-1
3. Importance of Finding Novel Bio-Sensing Methods to Detect Cancer Biomarkers

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor/Cancer Biomarker | Type of Cancer/Infected Location | Application | References |
|---|---|---|---|
| AFP | Liver (HCC) | Identifying recurrence, treatment monitoring, disease diagnosis | [144,145,146,147] |
| PSA | Prostate gland | Screening, identifying recurrence, treatment monitoring, disease diagnosis | [148,149,150] |
| CA 15-3 | Breast | Treatment monitoring | [103,151,152] |
| CT antigens | Prostate, liver, lung,bladder, skin | Diagnosis, prognosis | [105,106] |
| CA27.29 | Breast | Monitoring | [69,153] |
| RCAS1 | Stomach | Detection, prognosis | [96,97,98] |
| CA 19-9 | Pancreas, colon | Treatment monitoring | [122,154] |
| CEA (Carcinoembryonic antigen) | Colon, liver | Screening, Identifying recurrence, Treatment monitoring, Disease prognosis | [155,156] |
| Calcitonin | Thyroid gland | Treatment monitoring, Disease prognosis | [157] |
| ER & PgR (Estrogen, progesterone receptors) | Breast | Stratification | [158,159,160] |
| HER2 | Lung, breast | Monitoring therapy | [64,161,162,163] |
| CA 125 | Ovary | Prognosis, identifying recurrence, treatment monitoring, disease diagnosis | [88,89] |
| HCG-β | Ovary, testis | Diagnosis, staging, identifying recurrence, treatment monitoring | [164,165] |
| Tdt | Blood/leukemia | Diagnosis | [129] |
| NSe | Lung | Prognosis | [125,166] |
| Thyroglobulin | Thyroid | Treatment monitoring | [167,168] |
| PCA3 | Prostate gland | Prognosis | [169] |
| NY-eSO-1 | Skin/melanoma | Progression monitoring | [170] |
| EGFR | Lung | Diagnosis and monitoring therapy | [171,172] |
| KRAS, ALK | Lung | Diagnosis and monitoring therapy | [173,174] |
| CD30 | Blood/Leukemia | Diagnosis and prognosis | [175,176] |
| NMP 22 | Bladder | Screening, treatment monitoring, disease prognosis | [177,178] |
| CYFRA21-1 | Esophagus | Prognosis, Treatment monitoring | [179,180,181] |
| BCL2 | Blood and breast | Diagnosis, treatment plan | [182,183,184] |
| BCR-ABL fusion gene | Bone marrow, blood | Prognosis, treatment determination, monitoring | [185,186] |
| CD20 | Blood | Treatment determination | [187] |
| CD22 | Blood | Treatment determination, diagnosis | [188] |
| CD25 | Blood | Treatment determination | [189] |
| FGFR2 & FGFR3 | Bladder | Treatment determination, therapy | [190,191] |
| Fibrin-fibrinogen | Bladder | Treatment determination, monitoring | [192,193] |
| SMRP | Leukemia | Progression monitoring | [194,195] |
| ROS1 | Lung | Treatment determination | [196] |
| OVA1 | Ovary | Prognosis | [197] |
| VMA | Brain | Diagnosis | [198] |
4. Analytical Diagnostics Methodologies for Cancer Biomarkers Screening
Electrochemical Sensing Methodologies
5. Conclusions and Future Perspectives
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AFP | Alpha-fetoprotein |
| PSA | Prostate-specific antigen |
| RCAS1 | Receptor-binding cancer antigen |
| CA 15-3 | Cancer antigen 15-3 |
| CT antigen | Cancer–testis antigen |
| CA 125 | Cancer antigen 125 |
| CA 19-9 | Cancer antigen 19-9 |
| Nse | Neuron-specific enolase |
| Tdt | Terminal deoxynucleotidyl transferase |
| CYFRA21-1 | Cytokeratin-19 fragments |
| Carcinoma | Epithelial cell cancer |
| Sarcoma | Connective tissue/bone cancer |
| Lymphoma | Lymphatic system cancer |
| Myeloma | Plasma cell cancer |
| Leukemia | Blood cancer |
| BRCA1 | Breast cancer gene 1 |
| BRCA2 | Breast cancer gene 2 |
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Yabroff, K.R.; Wu, X.C.; Negoita, S.; Stevens, J.; Coyle, L.; Zhao, J.; Mumphrey, B.J.; Jemal, A.; Ward, K.C. Association of the COVID-19 Pandemic with Patterns of Statewide Cancer Services. J. Natl. Cancer Inst. 2022, 114, 907–909. [Google Scholar] [CrossRef]
- Patel, A. Benign vs Malignant Tumors. JAMA Oncol. 2020, 6, 1488. [Google Scholar] [CrossRef]
- WHO Cancer and Carcinogens. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer) (accessed on 11 November 2022).
- Croswell, J.M.; Ransohoff, D.F.; Kramer, B.S. Principles of Cancer Screening: Lessons from History and Study Design Issues. Semin. Oncol. 2010, 37, 202–215. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, W.; Walter, F.M.; Rubin, G.; Neal, R.D. Improving early diagnosis of symptomatic cancer. Nat. Rev. Clin. Oncol. 2016, 13, 740–749. [Google Scholar] [CrossRef]
- Patel, J.; Patel, P. Biosensors and Biomarkers: Promising Tools for Cancer Diagnosis. Int. J. Biosens. Bioelectron. 2017, 3, 00072. [Google Scholar] [CrossRef] [Green Version]
- Neal, R.D.; Tharmanathan, P.; France, B.; Din, N.U.; Cotton, S.; Fallon-Ferguson, J.; Hamilton, W.; Hendry, A.; Hendry, M.; Lewis, R.; et al. Is Increased Time to Diagnosis and Treatment in Symptomatic Cancer Associated with Poorer Outcomes? Systematic Review. Br. J. Cancer 2015, 112, S92–S107. [Google Scholar] [CrossRef] [Green Version]
- Summerfield, C.; Smith, L.; Todd, O.; Renzi, C.; Lyratzopoulos, G.; Neal, R.D.; Jones, D. The Effect of Older Age and Frailty on the Time to Diagnosis of Cancer: A Connected Bradford Electronic Health Records Study. Cancers 2022, 14, 5666. [Google Scholar] [CrossRef] [PubMed]
- Elliss-Brookes, L.; McPhail, S.; Ives, A.; Greenslade, M.; Shelton, J.; Hiom, S.; Richards, M. Routes to Diagnosis for Cancer—Determining the Patient Journey Using Multiple Routine Data Sets. Br. J. Cancer 2012, 107, 1220–1226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, K. Earlier Diagnosis: The Importance of Cancer Symptoms. Lancet Oncol. 2020, 21, 6–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, M.P.T.; Cheyne, L.; Darby, M.; Plant, P.; Milton, R.; Robson, J.M.; Gill, A.; Malhotra, P.; Ashford-Turner, V.; Rodger, K.; et al. Lung Cancer Stage-Shift Following a Symptom Awareness Campaign. Thorax 2018, 73, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Power, E.; Wardle, J. Change in Public Awareness of Symptoms and Perceived Barriers to Seeing a Doctor Following Be Clear on Cancer Campaigns in England. Br. J. Cancer 2015, 112, S22–S26. [Google Scholar] [CrossRef] [PubMed]
- Loud, J.T.; Murphy, J. Cancer Screening and Early Detection in the 21 St Century. Semin. Oncol. Nurs. 2017, 33, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Hewitt, K.; Son, J.; Glencer, A.; Borowsky, A.D.; Cooperberg, M.R.; Esserman, L.J. The Evolution of Our Understanding of the Biology of Cancer Is the Key to Avoiding Overdiagnosis and Overtreatment. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2463–2474. [Google Scholar] [CrossRef]
- Loomans-Kropp, H.A.; Umar, A. Cancer Prevention and Screening: The next Step in the Era of Precision Medicine. Npj Precis. Oncol. 2019, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shieh, Y.; Eklund, M.; Madlensky, L.; Sawyer, S.D.; Thompson, C.K.; Fiscalini, A.S.; Ziv, E.; Van’t Veer, L.J.; Esserman, L.J.; Tice, J.A. Breast Cancer Screening in the Precision Medicine Era: Risk-Based Screening in a Population-Based Trial. J. Natl. Cancer Inst. 2017, 109, djw290. [Google Scholar] [CrossRef] [Green Version]
- Esserman, L.J. The WISDOM Study: Breaking the Deadlock in the Breast Cancer Screening Debate. Npj Breast Cancer 2017, 3, 34. [Google Scholar] [CrossRef]
- Henley, S.J.; King, J.B.; German, R.R.; Richardson, L.C.; Plescia, M.; Centers for Disease Control and Prevention (CDC). Surveillance of Screening-Detected Cancers. MMWR Surveill. Summ. 2010, 59, 1–25. [Google Scholar]
- Negoita, S.; Feuer, E.J.; Mariotto, A.; Cronin, K.A.; Petkov, V.I.; Hussey, S.K.; Benard, V.; Henley, S.J.; Anderson, R.N.; Fedewa, S.; et al. Annual Report to the Nation on the Status of Cancer, Part II: Recent Changes in Prostate Cancer Trends and Disease Characteristics. Cancer 2018, 124, 2801–2814. [Google Scholar] [CrossRef] [Green Version]
- Elmore, L.W.; Greer, S.F.; Daniels, E.C.; Saxe, C.C.; Melner, M.H.; Krawiec, G.M.; Cance, W.G.; Phelps, W.C. Blueprint for Cancer Research: Critical Gaps and Opportunities. CA A Cancer J. Clin. 2021, 71, 107–139. [Google Scholar] [CrossRef]
- Schiffman, J.D.; Fisher, P.G.; Gibbs, P. Early Detection of Cancer: Past, Present, and Future. Am. Soc. Clin. Oncol. Educ. Book 2015, 35, 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, S.; Stark, D.D.; Brady, T.J.; Wittenberg, J.; Ferrucci, J.T. Dynamic Spin-Echo MRI of Liver Cancer Using Gadolinium-DTPA: Animal Investigation. AJR Am. J. Roentgenol. 1986, 147, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Lyman, D.F.; Bell, A.; Black, A.; Dingerdissen, H.; Cauley, E.; Gogate, N.; Liu, D.; Joseph, A.; Kahsay, R.; Crichton, D.J.; et al. Modeling and Integration of N-Glycan Biomarkers in a Comprehensive Biomarker Data Model. Glycobiology 2022, 32, 855–870. [Google Scholar] [CrossRef]
- Alimirzaie, S.; Bagherzadeh, M.; Akbari, M.R. Liquid Biopsy in Breast Cancer: A Comprehensive Review. Clin. Genet. 2019, 95, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Nikanjam, M.; Kato, S.; Kurzrock, R. Liquid Biopsy: Current Technology and Clinical Applications. J. Hematol. Oncol. 2022, 15, 1–14. [Google Scholar] [CrossRef]
- Chen, X.; Gole, J.; Gore, A.; He, Q.; Lu, M.; Min, J.; Yuan, Z.; Yang, X.; Jiang, Y.; Zhang, T.; et al. Non-Invasive Early Detection of Cancer Four Years before Conventional Diagnosis Using a Blood Test. Nat. Commun. 2020, 11, 3475. [Google Scholar] [CrossRef] [PubMed]
- Hall, I.J.; Tangka, F.K.L.; Sabatino, S.A.; Thompson, T.D.; Graubard, B.I.; Breen, N. Patterns and Trends in Cancer Screening in the United States. Prev. Chronic Dis. 2018, 15, 170465. [Google Scholar] [CrossRef] [Green Version]
- Pulumati, A.; Pulumati, A.; Dwarakanath, B.S.; Verma, A.; Papineni, R.V.L. Technological advancements in cancer diagnostics: Improvements and limitations. Cancer Rep. 2023, 6, e1764. [Google Scholar] [CrossRef]
- Gamble, P.; Jaroensri, R.; Wang, H.; Tan, F.; Moran, M.; Brown, T.; Flament-Auvigne, I.; Rakha, E.A.; Toss, M.; Dabbs, D.J.; et al. Determining Breast Cancer Biomarker Status and Associated Morphological Features Using Deep Learning. Commun. Med. 2021, 1, 14. [Google Scholar] [CrossRef]
- Zygulska, A.L.; Pierzchalski, P. Novel Diagnostic Biomarkers in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 852. [Google Scholar] [CrossRef] [PubMed]
- Porzycki, P.; Ciszkowicz, E. Modern Biomarkers in Prostate Cancer Diagnosis. Cent. Eur. J. Urol. 2020, 73, 300–306. [Google Scholar] [CrossRef]
- Atallah, G.A.; Aziz, N.H.A.; Teik, C.K.; Shafiee, M.N.; Kampan, N.C. New Predictive Biomarkers for Ovarian Cancer. Diagnostics 2021, 11, 465. [Google Scholar] [CrossRef] [PubMed]
- Molina, M.A.; Diatricch, L.C.; Quintana, M.C.; Melchers, W.J.G.; Andralojc, K.M. Cervical Cancer Risk Profiling: Molecular Biomarkers Predicting the Outcome of HrHPV Infection. Expert Rev. Mol. Diagn. 2020, 20, 1099–1120. [Google Scholar] [CrossRef]
- Hussain, T.; Nguyen, Q.T. Molecular Imaging for Cancer Diagnosis and Surgery. Adv. Drug Deliv. Rev. 2014, 66, 90. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.; Finkelstein, D.M.; Barrios, C.; Martin, M.; Iwata, H.; Hegg, R.; Glaspy, J.; Periañez, A.M.; Tonkin, K.; Deleu, I.; et al. Adjuvant Denosumab in Early Breast Cancer (D-CARE): An International, Multicentre, Randomised, Controlled, Phase 3 Trial. Lancet Oncol. 2020, 21, 60–72. [Google Scholar] [CrossRef]
- Taouli, B.; Beer, A.J.; Chenevert, T.; Collins, D.; Lehman, C.; Matos, C.; Padhani, A.R.; Rosenkrantz, A.B.; Shukla-Dave, A.; Sigmund, E.; et al. Diffusion-Weighted Imaging Outside the Brain: Consensus Statement From an ISMRM-Sponsored Workshop. J. Magn. Reason. Imaging 2016, 44, 521–540. [Google Scholar] [CrossRef]
- Padhani, A.R.; Liu, G.; Mu-Koh, D.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; Van Cauteren, M.; Collins, D.; et al. Diffusion-Weighted Magnetic Resonance Imaging as a Cancer Biomarker: Consensus and Recommendations. Neoplasia 2009, 1, 102–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altintas, Z.; Tothill, I. Biomarkers and Biosensors for the Early Diagnosis of Lung Cancer. Sens. Actuators B Chem. 2013, 188, 988–998. [Google Scholar] [CrossRef]
- del Sol, A.; Balling, R.; Hood, L.; Galas, D. Diseases as Network Perturbations. Curr. Opin. Biotechnol. 2010, 21, 566–571. [Google Scholar] [CrossRef]
- Sarhadi, V.K.; Armengol, G. Molecular Biomarkers in Cancer. Biomolecules 2022, 12, 1021. [Google Scholar] [CrossRef]
- Jayanthi, V.S.A.; Das, A.B.; Saxena, U. Recent Advances in Biosensor Development for the Detection of Cancer Biomarkers. Biosens. Bioelectron. 2017, 91, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Tothill, I.E. Biosensors for Cancer Markers Diagnosis. Semin. Cell Dev. Biol. 2009, 20, 55–62. [Google Scholar] [CrossRef]
- Fong, Z.V.; Winter, J.M. Biomarkers in Pancreatic Cancer: Diagnostic, Prognostic, and Predictive. Cancer J. 2012, 18, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Basil, C.F.; Zhao, Y.; Zavaglia, K.; Jin, P.; Panelli, M.C.; Voiculescu, S.; Mandruzzato, S.; Lee, H.M.; Seliger, B.; Freedman, R.S.; et al. Common Cancer Biomarkers. Cancer Res. 2006, 66, 2953–2961. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, S.G.; Ray, R.; Karmakar, P. Exosomal miRNAs—a diagnostic biomarker acting as a guiding light in the diagnosis of prostate cancer. Funct. Integr. Genom. 2023, 23, 23. [Google Scholar] [CrossRef]
- Henry, N.L.; Hayes, D.F. Cancer Biomarkers. Mol. Oncol. 2012, 6, 140–146. [Google Scholar] [CrossRef] [Green Version]
- Somerfield, M.R. Clinical Practice Guidelines for the Use of Tumor Markers in Breast and Colorectal Cancer. Adopted on May 17, 1996 by the American Society of Clinical Oncology. J. Clin. Oncol. 1996, 14, 2843–2877. [Google Scholar] [CrossRef]
- Meindl, A. Comprehensive Analysis of 989 Patients with Breast or Ovarian Cancer Provides BRCA1 and BRCA2 Mutation Profiles and Frequencies for the German Population. Int. J. Cancer 2002, 97, 472–480. [Google Scholar] [CrossRef]
- Easton, D.F.; Ford, D.; Bishop, D.T.; Haites, N.; Milner, B.; Allan, L.; Easton, D.F.; Ponder, B.A.J.; Peto, J.; Smith, S.; et al. Breast and Ovarian Cancer Incidence in BRCA1-Mutation Carriers. Breast Cancer Linkage Consortium. Am. J. Hum. Genet. 1995, 56, 265. [Google Scholar]
- Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W.; Kemper, A.R.; et al. Screening for Prostate Cancer USPreventive Services task force recommendation Statement. JAMA-J. Am. Med. Assoc. 2018, 319, 1901–1913. [Google Scholar] [CrossRef]
- Lin, K.; Lipsitz, R.; Miller, T.; Janakiraman, S. Benefits and Harms of Prostate-Specific Antigen Screening for Prostate Cancer: An Evidence Update for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2008, 149, 192–199. [Google Scholar] [CrossRef]
- Calonge, N.; Petitti, D.B.; Dewitt, T.G.; Dietrich, A.J.; Gregory, K.D.; Harris, R.; Isham, G.J.; Lefevre, M.L.; Leipzig, R.; Loveland-Cherry, C.; et al. Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2008, 149, 185–191. [Google Scholar] [CrossRef]
- Van’t Veer, L.J.; Paik, S.; Hayes, D.F. Gene Expression Profiling of Breast Cancer: A New Tumor Marker. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 1631–1635. [Google Scholar] [CrossRef] [PubMed]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A Multigene Assay to Predict Recurrence of Tamoxifen-Treated, Node-Negative Breast Cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Detection and Localization of Surgically Resectable Cancers with a Multi-Analyte Blood Test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [Green Version]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.M.M.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Li, B.; Gao, Q.; Luo, Y.; Ming, L. Prognostic Value of Epithelial-Mesenchymal Transition Circulating Tumor Cells in Female Breast Cancer: A Meta-Analysis. Front. Oncol. 2022, 12, 1024783. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Kawai, K.; Nozawa, H.; Sasaki, K.; Murono, K.; Emoto, S.; Ozawa, T.; Yokoyama, Y.; Nagai, Y.; Anzai, H.; et al. Clinical Impact of Primary Tumor Sidedness and Sex on Unresectable Post-Recurrence Survival in Resected Pathological Stage II-III Colorectal Cancers: A Nationwide Multicenter Retrospective Study. BMC Cancer 2022, 22, 1–10. [Google Scholar] [CrossRef]
- Allegra, C.J.; Jessup, J.M.; Somerfield, M.R.; Hamilton, S.R.; Hammond, E.H.; Hayes, D.F.; McAllister, P.K.; Morton, R.F.; Schilsky, R.L. American Society of Clinical Oncology Provisional Clinical Opinion: Testing for KRAS Gene Mutations in Patients with Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 2091–2096. [Google Scholar] [CrossRef] [Green Version]
- Thuss-Patience, P.C.; Shah, M.A.; Ohtsu, A.; Van Cutsem, E.; Ajani, J.A.; Castro, H.; Mansoor, W.; Chung, H.C.; Bodoky, G.; Shitara, K.; et al. Trastuzumab Emtansine versus Taxane Use for Previously Treated HER2-Positive Locally Advanced or Metastatic Gastric or Gastro-Oesophageal Junction Adenocarcinoma (GATSBY): An International Randomised, Open-Label, Adaptive, Phase 2/3 Study. Lancet Oncol. 2017, 18, 640–653. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in Combination with Chemotherapy versus Chemotherapy Alone for Treatment of HER2-Positive Advanced Gastric or Gastro-Oesophageal Junction Cancer (ToGA): A Phase 3, Open-Label, Randomised Controlled Trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef] [PubMed]
- Sawaki, M.; Taira, N.; Uemura, Y.; Saito, T.; Baba, S.; Kobayashi, K.; Kawashima, H.; Tsuneizumi, M.; Sagawa, N.; Bando, H.; et al. Adjuvant Trastuzumab without Chemotherapy for Treating Early HER2-Positive Breast Cancer in Older Patients: A Propensity Score-Adjusted Analysis of a Prospective Cohort Study. Breast 2022, 66, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Perez, E.A.; Ballman, K.V.; Tenner, K.S.; Thompson, E.A.; Badve, S.S.; Bailey, H.; Baehner, F.L. Association of Stromal Tumor-Infiltrating Lymphocytes with Recurrence-Free Survival in the N9831 Adjuvant Trial in Patients with Early-Stage HER2-Positive Breast Cancer. JAMA Oncol. 2016, 2, 56–64. [Google Scholar] [CrossRef]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1673–1684. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Gan, M.; Lin, Z.; Deng, Q.; Deng, J.; Zeng, B.; Shi, Y.; Ming, J. Clinical Features and Prognosis Analysis of Hormone Receptor-Positive, HER2-Negative Breast Cancer with Differential Expression Levels of Estrogen and Progesterone Receptors: A 10-Year Retrospective Study. Breast J. 2022, 2022, 5469163. [Google Scholar] [CrossRef]
- Abe, O.; Abe, R.; Enomoto, K.; Kikuchi, K.; Koyama, H.; Masuda, H.; Nomura, Y.; Ohashi, Y.; Sakai, K.; Sugimachi, K.; et al. Relevance of Breast Cancer Hormone Receptors and Other Factors to the Efficacy of Adjuvant Tamoxifen: Patient-Level Meta-Analysis of Randomised Trials. Lancet 2011, 378, 771–784. [Google Scholar] [CrossRef] [Green Version]
- Teutsch, S.M.; Bradley, L.A.; Palomaki, G.E.; Haddow, J.E.; Piper, M.; Calonge, N.; Dotson, W.D.; Douglas, M.P.; Berg, A.O. The Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Initiative: Methods of the EGAPP Working Group. Genet. Med. Off. J. Am. Coll. Med. Genet. 2009, 11, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Hanash, S.M.; Pitteri, S.J.; Faca, V.M. Mining the Plasma Proteome for Cancer Biomarkers. Nature 2008, 452, 571–579. [Google Scholar] [CrossRef]
- Mighton, C.; Shickh, S.; Aguda, V.; Krishnapillai, S.; Adi-Wauran, E.; Bombard, Y. From the Patient to the Population: Use of Genomics for Population Screening. Front. Genet. 2022, 13, 893832. [Google Scholar] [CrossRef]
- Kohsaka, S.; Tada, Y.; Ando, M.; Nakaguro, M.; Shirai, Y.; Ueno, T.; Kojima, S.; Hirai, H.; Saigusa, N.; Kano, S.; et al. Identification of Novel Prognostic and Predictive Biomarkers in Salivary Duct Carcinoma via Comprehensive Molecular Profiling. Npj Precis. Oncol. 2022, 6, 82. [Google Scholar] [CrossRef]
- Wang, N.; Zhang, H.; Li, D.; Jiang, C.; Zhao, H.; Teng, Y. Identification of Novel Biomarkers in Breast Cancer via Integrated Bioinformatics Analysis and Experimental Validation. Bioengineered 2021, 12, 12431. [Google Scholar] [CrossRef]
- Wu, M.; Li, Q.; Wang, H. Identification of Novel Biomarkers Associated with the Prognosis and Potential Pathogenesis of Breast Cancer via Integrated Bioinformatics Analysis. Technol. Cancer Res. Treat. 2021, 20, 1533033821992081. [Google Scholar] [CrossRef]
- Li, C.-J.; Lin, L.-T.; Chu, P.-Y.; Chiang, A.-J.; Tsai, H.-W.; Chiu, Y.-H.; Huang, M.-S.; Wen, Z.-H.; Tsui, K.-H.; Li, C.-J.; et al. Identification of Novel Biomarkers and Candidate Drug in Ovarian Cancer. J. Pers. Med. 2021, 11, 316. [Google Scholar] [CrossRef]
- Islam, S.U.; Ahmed, M.B.; Ahsan, H.; Lee, Y.S. Role of Biomarkers in Personalized Medicine. In Cancer Biomarkers in Diagnosis and Therapeutics; Springer: Singapore, 2022; pp. 249–275. [Google Scholar] [CrossRef]
- Janjua, K.A.; Shahzad, R.; Shehzad, A. Development of Novel Cancer Biomarkers for Diagnosis and Prognosis. In Cancer Biomarkers in Diagnosis and Therapeutics; Springer: Singapore, 2022; pp. 277–343. [Google Scholar] [CrossRef]
- Bohunicky, B.; Mousa, S.A. Biosensors: The New Wave in Cancer Diagnosis. Nanotechnol. Sci. Appl. 2011, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Prabhakar, B.; Shende, P.; Augustine, S. Current Trends and Emerging Diagnostic Techniques for Lung Cancer. Biomed. Pharmacother. 2018, 106, 1586–1599. [Google Scholar] [CrossRef]
- Chen, M.; Wu, D.; Tu, S.; Yang, C.; Chen, D.J.; Xu, Y. A Novel Biosensor for the Ultrasensitive Detection of the LncRNA Biomarker MALAT1 in Non-Small Cell Lung Cancer. Sci. Rep. 2021, 11, 3666. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.K.; Bandal, H.; Satyanarayana, M.; Goud, K.Y.; Gobi, K.V.; Jayaramudu, T.; Amalraj, J.; Kim, H. Recent Trends in Electrochemical Sensors for Vital Biomedical Markers Using Hybrid Nanostructured Materials. Adv. Sci. 2020, 7, 1902980. [Google Scholar] [CrossRef]
- Ferraro, S.; Bussetti, M.; Bassani, N.; Rossi, R.S.; Incarbone, G.P.; Bianchi, F.; Maggioni, M.; Runza, L.; Ceriotti, F.; Panteghini, M. Definition of Outcome-Based Prostate-Specific Antigen (PSA) Thresholds for Advanced Prostate Cancer Risk Prediction. Cancers 2021, 13, 3381. [Google Scholar] [CrossRef]
- Thompson, I.M.; Ankerst, D.P. Prostate-Specific Antigen in the Early Detection of Prostate Cancer. CMAJ Can. Med. Assoc. J. 2007, 176, 1853–1858. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Liu, H.; Liu, Z.; Liu, C.; Zhang, A.; Li, N. Analysis of Serum Alpha-Fetoprotein (AFP) and AFP-L3 Levels by Protein Microarray. J. Int. Med. Res. 2018, 46, 4297–4305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, Q.; Song, J.; Yang, W.; Wang, H.; Huo, Q.; Yang, J.; Yu, X.; Liu, Y.; Xu, C.; Bao, H. The Effect of CA125 on Metastasis of Ovarian Cancer: Old Marker New Function. Oncotarget 2017, 8, 50015–50022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, T.; Rustin, G.J. Role of Tumour Markers in Monitoring Epithelial Ovarian Cancer. Br. J. Cancer 2000, 82, 1535–1538. [Google Scholar] [CrossRef] [Green Version]
- Chianca, M.; Panichella, G.; Fabiani, I.; Giannoni, A.; L’Abbate, S.; Aimo, A.; Del Franco, A.; Vergaro, G.; Grigoratos, C.; Castiglione, V.; et al. Bidirectional Relationship Between Cancer and Heart Failure: Insights on Circulating Biomarkers. Front. Cardiovasc. Med. 2022, 9, 936654. [Google Scholar] [CrossRef]
- Tuxen, M.K.; Sölétormos, G.; Dombernowsky, P. Tumor Markers in the Management of Patients with Ovarian Cancer. Cancer Treat. Rev. 1995, 21, 215–245. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.S.; Humphrey, P.A.; Catalona, W.J. The Early Detection of Prostate Carcinoma with Prostate Specific Antigen: The Washington University Experience. Cancer 1997, 80, 1852–1856. [Google Scholar] [CrossRef]
- Bill-Axelson, A.; Holmberg, L.; Ruutu, M.; Häggman, M.; Andersson, S.-O.; Bratell, S.; Spångberg, A.; Busch, C.; Nordling, S.; Garmo, H.; et al. Radical Prostatectomy versus Watchful Waiting in Early Prostate Cancer. N. Engl. J. Med. 2005, 352, 1977–1984. [Google Scholar] [CrossRef] [Green Version]
- Jaffee, E.M.; Van Dang, C.; Agus, D.B.; Alexander, B.M.; Anderson, K.C.; Ashworth, A.; Barker, A.D.; Bastani, R.; Bhatia, S.; Bluestone, J.A.; et al. Future Cancer Research Priorities in the USA: A Lancet Oncology Commission. Lancet Oncol. 2017, 18, e653–e706. [Google Scholar] [CrossRef]
- National Cancer Institute. Prostate-Specific Antigen (PSA) Test—NCI; National Cancer Institute: Bethesda, MD, USA, 2022. [Google Scholar]
- Kim, J.H.; Suh, Y.J.; Park, D.; Yim, H.; Kim, H.; Kim, H.J.; Yoon, D.S.; Hwang, K.S. Technological Advances in Electrochemical Biosensors for the Detection of Disease Biomarkers. Biomed. Eng. Lett. 2021, 11, 309–334. [Google Scholar] [CrossRef]
- Dutsch-Wicherek, M.; Tomaszewska, R.; Lazar, A.; Wicherek, L.; Skladzien, J. The Association between RCAS1 Expression in Laryngeal and Pharyngeal Cancer and Its Healthy Stroma with Cancer Relapse. BMC Cancer 2009, 9, 35. [Google Scholar] [CrossRef] [Green Version]
- Kazmierczak, W.; Lazar, A.; Tomaszewska, R.; Popiela, T.J.; Koper, K.; Wicherek, L.; Dutsch-Wicherek, M. Analysis of the Intensity of Immune Cell Infiltration and Immunoreactivity of RCAS1 in Diffuse Large B-Cell Lymphoma of the Palatine Tonsil and Its Microenvironment. Cell Tissue Res. 2015, 361, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Kubokawa, M.; Nakashima, M.; Yao, T.; Ito, K.I.; Harada, N.; Nawata, H.; Watanabe, T. Aberrant Intracellular Localization of RCAS1 Is Associated with Tumor Progression of Gastric Cancer. Int. J. Oncol. 2001, 19, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Okabe, Y.; Nagayama, M.; Nishinakagawa, T.; Taira, T.; Kawahara, A.; Hattori, S.; MacHida, K.; Ishida, Y.; Kaji, R.; et al. Accuracy of Differential Diagnosis for Pancreatic Cancer Is Improved in the Combination of RCAS1 and CEA Measurements and Cytology in Pancreatic Juice. Med. Mol. Morphol. 2011, 44, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J. Serum Tumor Markers in Breast Cancer: Are They of Clinical Value? Clin. Chem. 2006, 52, 345–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasan, D. Diagnostic Impact of CEA and CA 15-3 on Chemotherapy Monitoring of Breast Cancer Patients. J. Circ. Biomark. 2022, 11, 57–63. [Google Scholar] [CrossRef]
- Tampellini, M.; Berruti, A.; Gerbino, A.; Buniva, T.; Torta, M.; Gorzegno, G.; Faggiuolo, R.; Cannone, R.; Farris, A.; Destefanis, M.; et al. Relationship between CA 15-3 Serum Levels and Disease Extent in Predicting Overall Survival of Breast Cancer Patients with Newly Diagnosed Metastatic Disease. Br. J. Cancer 1997, 75, 698–702. [Google Scholar] [CrossRef]
- Lian, M.; Zhang, C.; Zhang, D.; Chen, P.; Yang, H.; Yang, Y.; Chen, S.; Hong, G. The Association of Five Preoperative Serum Tumor Markers and Pathological Features in Patients with Breast Cancer. J. Clin. Lab. Anal. 2019, 33, e22875. [Google Scholar] [CrossRef]
- Bast, J.; Ravdin, P.; Hayes, D.F.; Bates, S.; Fritsche, H.J.; Jessup, J.M.; Kemeny, N.; Locker, G.Y.; Mennel, R.G.; Somerfield, M.R. 2000 Update of Recommendations for the Use of Tumor Markers in Breast and Colorectal Cancer: Clinical Practice Guidelines of the American Society of Clinical Oncology. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2001, 19, 1865–1878. [Google Scholar] [CrossRef]
- Lin, M.J.; Svensson-Arvelund, J.; Lubitz, G.S.; Marabelle, A.; Melero, I.; Brown, B.D.; Brody, J.D. Cancer Vaccines: The next Immunotherapy Frontier. Nat. Cancer 2022, 3, 911–926. [Google Scholar] [CrossRef]
- Chow, S.; Berek, J.S.; Dorigo, O. Development of Therapeutic Vaccines for Ovarian Cancer. Vaccines 2020, 8, 657. [Google Scholar] [CrossRef] [PubMed]
- Jäger, E.; Chen, Y.T.; Drijfhout, J.W.; Karbach, J.; Ringhoffer, M.; Jäger, D.; Arand, M.; Wada, H.; Noguchi, Y.; Stockert, E.; et al. Simultaneous Humoral and Cellular Immune Response against Cancer-Testis Antigen NY-ESO-1: Definition of Human Histocompatibility Leukocyte Antigen (HLA)-A2-Binding Peptide Epitopes. J. Exp. Med. 1998, 187, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, K.; Hamada, T.; Uenaka, A.; Wada, H.; Sato, E.; Isobe, M.; Asagoe, K.; Yamasaki, O.; Shiku, H.; Ritter, G.; et al. Induction of Immune Response against NY-ESO-1 by CHP-NY-ESO-1 Vaccination and Immune Regulation in a Melanoma Patient. Cancer Immunol. Immunother. 2008, 57, 1429–1437. [Google Scholar] [CrossRef]
- Jäger, E.; Stockert, E.; Zidianakis, Z.; Chen, Y.T.; Karbach, J.; Jäger, D.; Arand, M.; Ritter, G.; Old, L.J.; Knuth, A. Humoral Immune Responses of Cancer Patients against “Cancer-Testis” Antigen NY-ESO-1: Correlation with Clinical Events. Int. J. Cancer 1999, 84, 506–510. [Google Scholar] [CrossRef]
- Karbach, J.; Neumann, A.; Atmaca, A.; Wahle, C.; Brand, K.; Von Boehmer, L.; Knuth, A.; Bender, A.; Ritter, G.; Old, L.J.; et al. Efficient in Vivo Priming by Vaccination with Recombinant NY-ESO-1 Protein and CpG in Antigen Naive Prostate Cancer Patients. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 861–870. [Google Scholar] [CrossRef] [Green Version]
- Stockert, E.; Jäger, E.; Chen, Y.T.; Scanlan, M.J.; Gout, I.; Karbach, J.; Arand, M.; Knuth, A.; Old, L.J. A Survey of the Humoral Immune Response of Cancer Patients to a Panel of Human Tumor Antigens. J. Exp. Med. 1998, 187, 1349–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, N.; Ikeda, H.; Shiku, H. [Targeting Cancer Antigen (MAGE-A4, NY-ESO -1) for Immunotherapy]. Nihon Rinsho. Jpn. J. Clin. Med. 2012, 70, 2125–2129. [Google Scholar]
- Raza, A.; Merhi, M.; Inchakalody, V.P.; Krishnankutty, R.; Relecom, A.; Uddin, S.; Dermime, S. Unleashing the Immune Response to NY-ESO-1 Cancer Testis Antigen as a Potential Target for Cancer Immunotherapy. J. Transl. Med. J. Transl. Med. 2020, 18, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Babaier, A.; Mal, H.; Alselwi, W.; Ghatage, P. Low-Grade Serous Carcinoma of the Ovary: The Current Status. Diagnostics 2022, 12, 458. [Google Scholar] [CrossRef]
- Neesham, D. Ovarian Cancer Screening. Aust. Fam. Physician 2007, 36, 126–128. [Google Scholar]
- Menon, U.; Gentry-Maharaj, A.; Hallett, R.; Ryan, A.; Burnell, M.; Sharma, A.; Lewis, S.; Davies, S.; Philpott, S.; Lopes, A.; et al. Sensitivity and Specificity of Multimodal and Ultrasound Screening for Ovarian Cancer, and Stage Distribution of Detected Cancers: Results of the Prevalence Screen of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol. 2009, 10, 327–340. [Google Scholar] [CrossRef] [Green Version]
- Wong, N.K.; Easton, R.L.; Panico, M.; Sutton-Smith, M.; Morrison, J.C.; Lattanzio, F.A.; Morris, H.R.; Clark, G.F.; Dell, A.; Patankar, M.S. Characterization of the Oligosaccharides Associated with the Human Ovarian Tumor Marker CA125. J. Biol. Chem. 2003, 278, 28619–28634. [Google Scholar] [CrossRef] [Green Version]
- White, B.; Patterson, M.; Karnwal, S.; Brooks, C.L. Crystal Structure of a Human MUC16 SEA Domain Reveals Insight into the Nature of the CA125 Tumor Marker. Proteins Struct. Funct. Bioinform. 2022, 90, 1210–1218. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Ren, S.-F.; Jiang, W.; Lu, J.-Q.; Zhang, X.-Y.; Li, X.-P.; Cao, R.; Xu, C.-J. CA125-Tn ELISA Assay Improves Specificity of Pre-Operative Diagnosis of Ovarian Cancer among Patients with Elevated Serum CA125 Levels. Ann. Transl. Med. 2021, 9, 788. [Google Scholar] [CrossRef] [PubMed]
- Seelenmeyer, C.; Wegehingel, S.; Lechner, J.; Nickel, W. The Cancer Antigen CA125 Represents a Novel Counter Receptor for Galectin-1. J. Cell Sci. 2003, 116, 1305–1318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, L.; Fang, J.; Han, X.; Zhai, X.; Song, Y.; Lu, Y.; Zhang, Q.; Ma, R. Prognostic Value of CEA, CA19-9, CA125, CA724, and CA242 in Serum and Ascites in Pseudomyxoma Peritonei. Front. Oncol. 2021, 11, 594763. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Li, Y.; Li, C.; Yang, J.; Liu, D.; Wang, H.; Xu, R.; Zhang, Y.; Wei, Q. An ultrasensitive split-type electrochemical immunosensor based on controlled-release strategy for detection of CA19-9. Biosens. Bioelectron. 2023, 227, 115180. [Google Scholar] [CrossRef]
- Poruk, K.E.; Firpo, M.A.; Adler, D.G.; Mulvihill, S.J. Screening for Pancreatic Cancer: Why, How, and Who? Ann. Surg. 2013, 257, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Badheeb, M.; Abdelrahim, A.; Esmail, A.; Umoru, G.; Abboud, K.; Al-Najjar, E.; Rasheed, G.; Alkhulaifawi, M.; Abudayyeh, A.; Abdelrahim, M. Pancreatic Tumorigenesis: Precursors, Genetic Risk Factors and Screening. Curr. Oncol. 2022, 29, 8693–8719. [Google Scholar] [CrossRef] [PubMed]
- Hatzakis, K.D.; Froudarakis, M.E.; Bouros, D.; Tzanakis, N.; Karkavitsas, N.; Siafakas, N.M. Prognostic Value of Serum Tumor Markers in Patients with Lung Cancer. Respiration 2002, 69, 25–29. [Google Scholar] [CrossRef]
- Ferrigno, D.; Buccheri, G.; Giordano, C. Neuron-Specific Enolase Is an Effective Tumour Marker in Non-Small Cell Lung Cancer (NSCLC). Lung Cancer 2003, 41, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Gazdar, A.F.; Carney, D.N.; Nau, M.M.; Minna, J.D. Characterization of Variant Subclasses of Cell Lines Derived from Small Cell Lung Cancer Having Distinctive Biochemical, Morphological, and Growth Properties. Cancer Res. 1985, 45, 2924–2930. [Google Scholar] [PubMed]
- Isgrò, M.A.; Bottoni, P.; Scatena, R. Neuron-Specifi c Enolase as a Biomarker: Biochemical and Clinical Aspects. Adv. Exp. Med. Biol. 2015, 867, 125–143. [Google Scholar] [CrossRef]
- Tian, Z.; Liang, C.; Zhang, Z.; Wen, H.; Feng, H.; Ma, Q.; Liu, D.; Qiang, G. Prognostic Value of Neuron-Specific Enolase for Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. World J. Surg. Oncol. 2020, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Campagnari, F.; Bombardieri, E.; de Braud, F.; Baldini, L.; Maiolo, A.T. Terminal Deoxynucleotidyl Transferase, Tdt, as a Marker for Leukemia and Lymphoma Cells. Int. J. Biol. Markers 1987, 2, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Shang, H.; Zheng, Z.; Li, H.; Chen, W.; Xu, J. Self-activation of symbiotic multi-DNA machines transducing exponentially amplified fluorescence for ultrasensitively signaling of terminal deoxynucleotidyl transferase activity. Sens. Actuators B. Chem 2023, 380, 133400. [Google Scholar] [CrossRef]
- Sur, M.; AlArdati, H.; Ross, C.; Alowami, S. TdT Expression in Merkel Cell Carcinoma: Potential Diagnostic Pitfall with Blastic Hematological Malignancies and Expanded Immunohistochemical Analysis. Mod. Pathol. 2007, 20, 1113–1120. [Google Scholar] [CrossRef] [Green Version]
- Mathewson, R.C.; Kjeldsberg, C.R.; Perkins, S.L. Detection of Terminal Deoxynucleotidyl Transferase (TdT) in Nonhematopoietic Small Round Cell Tumors of Children. Pediatr. Pathol. Lab. Med. J. Soc. Pediatr. Pathol. Affil. Int. Paediatr. Pathol. Assoc. 1997, 17, 835–844. [Google Scholar]
- Chapman, M.H.; Sandanayake, N.S.; Andreola, F.; Dhar, D.K.; Webster, G.J.; Dooley, J.S.; Pereira, S.P. Circulating CYFRA 21-1 Is a Specific Diagnostic and Prognostic Biomarker in Biliary Tract Cancer. J. Clin. Exp. Hepatol. 2011, 1, 6–12. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, D.; Li, L.; Pu, D.; Zhou, P.; Jing, Y.; Yu, H.; Wang, Y.; Zhu, Y.; He, Y.; et al. The Important Role of Circulating CYFRA21-1 in Metastasis Diagnosis and Prognostic Value Compared with Carcinoembryonic Antigen and Neuron-Specific Enolase in Lung Cancer Patients. BMC Cancer 2017, 17, 96. [Google Scholar] [CrossRef] [Green Version]
- Dal Bello, M.G.; Filiberti, R.A.; Alama, A.; Orengo, A.M.; Mussap, M.; Coco, S.; Vanni, I.; Boccardo, S.; Rijavec, E.; Genova, C.; et al. The Role of CEA, CYFRA21-1 and NSE in Monitoring Tumor Response to Nivolumab in Advanced Non-Small Cell Lung Cancer (NSCLC) Patients. J. Transl. Med. 2019, 17, 74. [Google Scholar] [CrossRef] [Green Version]
- Rapellino, M.; Niklinski, J.; Pecchio, F.; Furman, M.; Baldi, S.; Chyczewski, L.; Ruffini, E.; Chyczewska, E. CYFRA 21-1 as a Tumour Marker for Bronchogenic Carcinoma. Eur. Respir. J. 1995, 8, 407–410. [Google Scholar] [CrossRef] [Green Version]
- Dall’Olio, F.G.; Abbati, F.; Facchinetti, F.; Massucci, M.; Melotti, B.; Squadrilli, A.; Buti, S.; Formica, F.; Tiseo, M.; Ardizzoni, A. CEA and CYFRA 21-1 as Prognostic Biomarker and as a Tool for Treatment Monitoring in Advanced NSCLC Treated with Immune Checkpoint Inhibitors. Ther. Adv. Med. Oncol. 2020, 12, 1758835920952994. [Google Scholar] [CrossRef]
- Hayakawa, T.; Naruse, S.; Kitagawa, M.; Ishiguro, H.; Kondo, T.; Kurimoto, K.; Fukushima, M.; Takayama, T.; Horiguchi, Y.; Kuno, N.; et al. A Prospective Multicenter Trial Evaluating Diagnostic Validity of Multivariate Analysis and Individual Serum Marker in Differential Diagnosis of Pancreatic Cancer from Benign Pancreatic Diseases. Int. J. Pancreatol. Off. J. Int. Assoc. Pancreatol. 1999, 25, 23–29. [Google Scholar] [CrossRef]
- Chen, G.; Yu, M.; Cao, J.; Zhao, H.; Dai, Y.; Cong, Y.; Qiao, G. Identification of Candidate Biomarkers Correlated with Poor Prognosis of Breast Cancer Based on Bioinformatics Analysis. Bioengineered 2021, 12, 5149–5161. [Google Scholar] [CrossRef]
- Kumar, S.; Mohan, A.; Guleria, R. Biomarkers in Cancer Screening, Research and Detection: Present and Future: A Review. Biomarkers 2008, 11, 385–405. [Google Scholar] [CrossRef]
- Chatterjee, S.K.; Zetter, B.R. Cancer Biomarkers: Knowing the Present and Predicting the Future. Future Oncol. 2005, 1, 37–50. [Google Scholar] [CrossRef]
- Hayes, D.F. Biomarker Validation and Testing. Mol. Oncol. 2015, 9, 960–966. [Google Scholar] [CrossRef]
- Hayes, D.F.; Bast, R.C.; Desch, C.E.; Fritsche, H.; Kemeny, N.E.; Jessup, J.M.; Locker, G.Y.; Macdonald, J.S.; Mennel, R.G.; Norton, L.; et al. Tumor Marker Utility Grading System: A Framework to Evaluate Clinical Utility of Tumor Markers. J. Natl. Cancer Inst. 1996, 88, 1456–1466. [Google Scholar] [CrossRef] [Green Version]
- Hamanishi, J.; Mandai, M.; Ikeda, T.; Minami, M.; Kawaguchi, A.; Murayama, T.; Kanai, M.; Mori, Y.; Matsumoto, S.; Chikuma, S.; et al. Safety and Antitumor Activity of Anti-PD-1 Antibody, Nivolumab, in Patients with Platinum-Resistant Ovarian Cancer. J. Clin. Oncol. 2015, 33, 4015–4022. [Google Scholar] [CrossRef]
- Johnson, P.J.; Williams, R.; Johnson, P.J. Serum Alpha-Fetoprotein Estimations and Doubling Time in Hepatocellular Carcinoma: Influence of Therapy and Possible Value in Early Detection. J. Natl. Cancer Inst. 1980, 64, 1329–1332. [Google Scholar] [CrossRef] [PubMed]
- Ye, K.; Fan, Q.; Yuan, M.; Wang, D.; Xiao, L.; Long, G.; Chen, R.; Fang, T.; Li, Z.; Zhou, L. Prognostic Value of Postoperative Circulating Tumor DNA in Patients with Early- and Intermediate-Stage Hepatocellular Carcinoma. Front. Oncol. 2022, 12, 834992. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Ho, D.W.Y.; Lee, N.P.Y.; Sun, S.; Lam, B.; Wong, K.F.; Yi, X.; Lau, G.K.; Ng, E.W.Y.; Poon, T.C.W.; et al. Enhanced Detection of Early Hepatocellular Carcinoma by Serum SELDI-TOF Proteomic Signature Combined with Alpha-Fetoprotein Marker. Ann. Surg. Oncol. 2010, 17, 2518–2525. [Google Scholar] [CrossRef] [Green Version]
- Vickers, A.J.; Brewster, S.F. PSA Velocity and Doubling Time in Diagnosis and Prognosis of Prostate Cancer. Br. J. Med. Surg. Urol. 2012, 5, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Bjartell, A.S. Next-Generation Prostate-Specific Antigen Test: Ready to Use? Eur. Urol. 2013, 64, 700–702. [Google Scholar] [CrossRef]
- Dunn, M.W. Prostate Cancer Screening. Semin. Oncol. Nurs. 2017, 33, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Molina, R.; Barak, V.; Van Dalen, A.; Duffy, M.J.; Einarsson, R.; Gion, M.; Goike, H.; Lamerz, R.; Nap, M.; Sölétormos, G.; et al. Tumor Markers in Breast Cancer- European Group on Tumor Markers Recommendations. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2005, 26, 281–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leja, M.; Linē, A. Early Detection of Gastric Cancer beyond Endoscopy—New Methods. Best Pract. Res. Clin. Gastroenterol. 2021, 50–51, 101731. [Google Scholar] [CrossRef]
- Jensen, J.L.; Maclean, G.D.; Suresh, M.R.; Almeida, A.; Jette, D.; Lloyd, S.; Bodnar, D.; Krantz, M.; Longenecker, B.M. Possible Utility of Serum Determinations of CA 125 and CA 27.29 in Breast Cancer Management. Int. J. Biol. Markers 1991, 6, 1–6. [Google Scholar] [CrossRef]
- Ludwig, J.A.; Weinstein, J.N. Biomarkers in Cancer Staging, Prognosis and Treatment Selection. Nat. Rev. Cancer 2005, 5, 845–856. [Google Scholar] [CrossRef]
- von Kleist, S. The Clinical Value of the Tumor Markers CA 19/9 and Carcinoembryonic Antigen (CEA) in Colorectal Carcinomas: A Critical Comparison. Int. J. Biol. Markers 1986, 1, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, F.; Odagiri, H.; Fujimoto, H.; Kawamura, T.; Ishimori, A. [Clinical evaluation of four tumor markers (CEA, TPA, CA50 and CA72-4) in colorectal cancer]. Rinsho Byori. Jpn. J. Clin. Pathol. 1992, 40, 523–528. [Google Scholar]
- Bae, Y.J.; Schaab, M.; Kratzsch, J. Calcitonin as Biomarker for the Medullary Thyroid Carcinoma. Recent Results Cancer Res. Fortschr. Der Krebsforschung. Prog. Dans Les Rech. Sur Le Cancer 2015, 204, 117–137. [Google Scholar] [CrossRef]
- Paik, S.; Tang, G.; Shak, S.; Kim, C.; Baker, J.; Kim, W.; Cronin, M.; Baehner, F.L.; Watson, D.; Bryant, J.; et al. Gene Expression and Benefit of Chemotherapy in Women with Node-Negative, Estrogen Receptor-Positive Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2006, 24, 3726–3734. [Google Scholar] [CrossRef] [PubMed]
- Porras, L.; Gorse, F.; Thiombane, N.K.; Gaboury, L.; Mader, S. CAXII Is a Surrogate Marker for Luminal Breast Tumors Regulated by ER and GATA3. Cancers 2022, 14, 5453. [Google Scholar] [CrossRef]
- McGuire, W.L.; Horwitz, K.B.; Pearson, O.H.; Segaloff, A. Current Status of Estrogen and Progesterone Receptors in Breast Cancer. Cancer 1977, 39, 2934–2947. [Google Scholar] [CrossRef]
- Varadan, V.; Kamalakaran, S.; Gilmore, H.; Banerjee, N.; Janevski, A.; Miskimen, K.L.S.; Williams, N.; Basavanhalli, A.; Madabhushi, A.; Lezon-Geyda, K.; et al. Brief-Exposure to Preoperative Bevacizumab Reveals a TGF-β Signature Predictive of Response in HER2-Negative Breast Cancers. Int. J. Cancer 2016, 138, 747–757. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L.; et al. Signatures of Mutational Processes in Human Cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, A.N.; Mathur, R.; Farooque, A.; Verma, A.; Dwarakanath, B.S. Cancer Biomarkers—Current Perspectives. Indian J. Med. Res. 2010, 132, 129–149. [Google Scholar]
- Perrier D’Hauterive, S.; Berndt, S.; Tsampalas, M.; Charlet-Renard, C.; Dubois, M.; Bourgain, C.; Hazout, A.; Foidart, J.M.; Geenen, V. Dialogue between Blastocyst HCG and Endometrial LH/HCG Receptor: Which Role in Implantation? Gynecol. Obstet. Investig. 2007, 64, 156–160. [Google Scholar] [CrossRef]
- Kurtzman, J.T.; Wilson, H.; Rao, C.V. A Proposed Role for HCG in Clinical Obstetrics. Semin. Reprod. Med. 2001, 19, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Adewole, I.F.; Newlands, E.S. Neuron-Specific Enolase (NSE) as a Tumour Marker and Comparative Evaluation with Carcinoembryonic Antigen (CEA) in Small-Cell Lung Cancer. Med. Oncol. Tumor Pharmacother. 1987, 4, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Darmawan, B.; Sari, M.; Susilo, S.; Kartamihardja, A.H.S. Preradioactive Iodine Thyroglobulin Levels as Predictors of Metastasis in Well-Differentiated Thyroid Carcinoma Patients. World J. Nucl. Med. 2022, 21, 296–301. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Robbins, R.J.; Spencer, C.A.; Braverman, L.E.; Pacini, F.; Wartofsky, L.; Haugen, B.R.; Sherman, S.I.; Cooper, D.S.; Braunstein, G.D.; et al. A Consensus Report of the Role of Serum Thyroglobulin as a Monitoring Method for Low-Risk Patients with Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2003, 88, 1433–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gils, M.P.M.Q.; Cornel, E.B.; Hessels, D.; Peelen, W.P.; Witjes, J.A.; Mulders, P.F.A.; Rittenhouse, H.G.; Schalken, J.A. Molecular PCA3 Diagnostics on Prostatic Fluid. Prostate 2007, 67, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Al-Khadairi, G.; Roelands, J.; Hendrickx, W.; Dermime, S.; Bedognetti, D.; Decock, J. NY-ESO-1 Based Immunotherapy of Cancer: Current Perspectives. Front. Immunol. 2018, 9, 947. [Google Scholar] [CrossRef]
- Ellison, G.; Zhu, G.; Moulis, A.; Dearden, S.; Speake, G.; McCormack, R. EGFR Mutation Testing in Lung Cancer: A Review of Available Methods and Their Use for Analysis of Tumour Tissue and Cytology Samples. J. Clin. Pathol. 2013, 66, 79–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Cunha Santos, G.; Shepherd, F.A.; Tsao, M.S. EGFR Mutations and Lung Cancer. Annu. Rev. Pathol. 2011, 6, 49–69. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.; Lee, T.; Lee, S.H.; Choi, Y.L.; Han, J. Clinicopathologic Characteristics of EGFR, KRAS, and ALK Alterations in 6595 Lung Cancers. Oncotarget 2016, 7, 23874. [Google Scholar] [CrossRef]
- Warth, A.; Penzel, R.; Lindenmaier, H.; Brandt, R.; Stenzinger, A.; Herpel, E.; Goeppert, B.; Thomas, M.; Herth, F.J.F.; Dienemann, H.; et al. EGFR, KRAS, BRAF and ALK Gene Alterations in Lung Adenocarcinomas: Patient Outcome, Interplay with Morphology and Immunophenotype. Eur. Respir. J. 2014, 43, 872–883. [Google Scholar] [CrossRef] [Green Version]
- Pierce, J.M.R.; Mehta, A. Diagnostic, Prognostic and Therapeutic Role of CD30 in Lymphoma. Expert Rev. Hematol. 2017, 10, 29–37. [Google Scholar] [CrossRef] [PubMed]
- van der Weyden, C.A.; Pileri, S.A.; Feldman, A.L.; Whisstock, J.; Prince, H.M. Understanding CD30 Biology and Therapeutic Targeting: A Historical Perspective Providing Insight into Future Directions. Blood Cancer J. 2017, 7, e603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Kumar, R.; Gupta, N.P. Comparison of NMP22 BladderChek Test and Urine Cytology for the Detection of Recurrent Bladder Cancer. Jpn. J. Clin. Oncol. 2006, 36, 172–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibar, Y.; Goktas, S.; Kilic, S.; Yaman, H.; Onguru, O.; Peker, A.F. Prognostic Value of Cytology, Nuclear Matrix Protein 22 (NMP22) Test, and Urinary Bladder Cancer II (UBC II) Test in Early Recurrent Transitional Cell Carcinoma of the Bladder. Ann. Clin. Lab. Sci. 2006, 36, 31–38. [Google Scholar] [PubMed]
- Mei, X.; Zhu, X.; Zuo, L.; Wu, H.; Guo, M.; Liu, C. Predictive Significance of CYFRA21-1, Squamous Cell Carcinoma Antigen and Carcinoembryonic Antigen for Lymph Node Metastasis in Patients with Esophageal Squamous Cancer. Int. J. Biol. Markers 2019, 34, 200–204. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Ide, H.; Eguchi, R.; Hayashi, K.; Takasaki, K.; Watanabe, S. CYFRA 21–1 as a Tumor Marker for Squamous Cell Carcinoma of the Esophagus. Dis. Esophagus 1998, 11, 35–39. [Google Scholar] [CrossRef]
- Brockmann, J.G.; St Nottberg, H.; Glodny, B.; Heinecke, A.; Senninger, N.J. CYFRA 21-1 Serum Analysis in Patients with Esophageal Cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2000, 6, 4249–4252. [Google Scholar]
- McCarthy, B.A.; Boyle, E.; Xue, P.W.; Guzowski, D.; Paul, S.; Catera, R.; Trott, J.; Yan, X.J.; Croce, C.M.; Damle, R.; et al. Surface Expression of Bcl-2 in Chronic Lymphocytic Leukemia and Other B-Cell and Lymphomas without a Breakpoint t(14;18). Mol. Med. 2008, 14, 618–627. [Google Scholar] [CrossRef] [Green Version]
- Dawson, S.J.; Makretsov, N.; Blows, F.M.; Driver, K.E.; Provenzano, E.; Le Quesne, J.; Baglietto, L.; Severi, G.; Giles, G.G.; McLean, C.A.; et al. BCL2 in Breast Cancer: A Favourable Prognostic Marker across Molecular Subtypes and Independent of Adjuvant Therapy Received. Br. J. Cancer 2010, 103, 668–675. [Google Scholar] [CrossRef]
- Kulsoom, B.; Shamsi, T.S.; Afsar, N.A.; Memon, Z.; Ahmed, N.; Hasnain, S.N. Bax, Bcl-2, and Bax/Bcl-2 as Prognostic Markers in Acute Myeloid Leukemia: Are We Ready for Bcl-2-Directed Therapy? Cancer Manag. Res. 2018, 10, 403–416. [Google Scholar] [CrossRef] [Green Version]
- Gaafar, T.M.; Raafat, I.I.; Aly, A.A.; Abd El-Ghaffar Mohamed, N.; Farid, R.J.; Saad, N.E.; El-Hawary, R.; Mostafaa, N.; Ahmed, M.M. Detection of BCR/ABL Translocation in Bone Marrow Derived Mesenchymal Stem Cells in Egyptian CML Patients. Open Access Maced. J. Med. Sci. 2015, 3, 231–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.Q.; Voelkerding, K.V.; Sabatini, L.; Chen, X.R.; Huang, J.; Meisner, L.F. Extensive Amplification of Bcr/Abl Fusion Genes Clustered on Three Marker Chromosomes in Human Leukemic Cell Line K-562. Leukemia 1995, 9, 858–862. [Google Scholar] [PubMed]
- Boyd, S.D.; Natkunam, Y.; Allen, J.R.; Warnke, R.A. Selective Immunophenotyping for Diagnosis of B-Cell Neoplasms: Immunohistochemistry and Flow Cytometry Strategies and Results. Appl. Immunohistochem. Mol. Morphol. 2013, 21, 116–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsushita, K.; Margulies, I.; Onda, M.; Nagata, S.; Stetler-Stevenson, M.; Kreitman, R.J. Soluble CD22 as a Tumor Marker for Hairy Cell Leukemia. Blood 2008, 112, 2272–2277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.; Ran, Q.; Xu, B.; Luo, X.; Song, S.; Xu, D.; Zhang, X. Role of CD25 Expression on Prognosis of Acute Myeloid Leukemia: A Literature Review and Meta-Analysis. PLOS ONE 2020, 15, e0236124. [Google Scholar] [CrossRef] [PubMed]
- Casadei, C.; Dizman, N.; Schepisi, G.; Cursano, M.C.; Basso, U.; Santini, D.; Pal, S.K.; De Giorgi, U. Targeted Therapies for Advanced Bladder Cancer: New Strategies with FGFR Inhibitors. Ther. Adv. Med. Oncol. 2019, 11, 1758835919890285. [Google Scholar] [CrossRef] [Green Version]
- Knowles, M.A. Role of FGFR3 in Urothelial Cell Carcinoma: Biomarker and Potential Therapeutic Target. World J. Urol. 2007, 25, 581–593. [Google Scholar] [CrossRef] [Green Version]
- Topsakal, M.; Karadeniz, T.; Anaç, M.; Dönmezer, S.; Besisik, A. Assessment of Fibrin-Fibrinogen Degradation Products (Accu-Dx) Test in Bladder Cancer Patients. Eur. Urol. 2001, 39, 287–291. [Google Scholar] [CrossRef]
- Glas, A.S.; Roos, D.; Deutekom, M.; Zwinderman, A.H.; Bossuyt, P.M.M.; Kurth, K.H. Tumor Markers in the Diagnosis of Primary Bladder Cancer. A Systematic Review. J. Urol. 2003, 169, 1975–1982. [Google Scholar] [CrossRef]
- Robinson, B.W.S.; Creaney, J.; Lake, R.; Nowak, A.; Musk, A.W.; De Klerk, N.; Winzell, P.; Hellstrom, K.E.; Hellstrom, I. Soluble Mesothelin-Related Protein—A Blood Test for Mesothelioma. Lung Cancer 2005, 49, S109–S111. [Google Scholar] [CrossRef]
- Kaeding, A.J.; Barwe, S.P.; Gopalakrishnapillai, A.; Ries, R.E.; Alonzo, T.A.; Gerbing, R.B.; Correnti, C.; Loken, M.R.; Broderson, L.E.; Pardo, L.; et al. Mesothelin Is a Novel Cell Surface Disease Marker and Potential Therapeutic Target in Acute Myeloid Leukemia. Blood Adv. 2021, 5, 2350–2361. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Büttner, R.; Al-Dayel, F.; Dietel, M.; Elmberger, G.; Kerr, K.; López-Ríos, F.; Marchetti, A.; Öz, B.; Pauwels, P.; et al. Testing for ROS1 in Non-Small Cell Lung Cancer: A Review with Recommendations. Virchows Arch. Int. J. Pathol. 2016, 469, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Nolen, B.M.; Lokshin, A.E. Biomarker Testing for Ovarian Cancer: Clinical Utility of Multiplex Assays. Mol. Diagn. Ther. 2013, 17, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Jelski, W.; Mroczko, B. Molecular and Circulating Biomarkers of Brain Tumors. Int. J. Mol. Sci. 2021, 22, 7039. [Google Scholar] [CrossRef] [PubMed]
- Ouhibi, A.; Raouafi, A.; Lorrain, N.; Guendouz, M.; Raouafi, N.; Moadhen, A. Functionalized SERS Substrate Based on Silicon Nanowires for Rapid Detection of Prostate Specific Antigen. Sens. Actuators B Chem. 2021, 330, 129352. [Google Scholar] [CrossRef]
- Mishra, S.; Kim, E.-S.; Sharma, P.K.; Wang, Z.-J.; Yang, S.-H.; Kaushik, A.K.; Wang, C.; Li, Y.; Kim, N.-Y. Tailored Biofunctionalized Biosensor for the Label-Free Sensing of Prostate-Specific Antigen. ACS Appl. Bio Mater. 2020, 3, 7821–7830. [Google Scholar] [CrossRef]
- Ribeiro, J.A.; Sales, M.G.F.; Pereira, C.M. Electrochemistry-Assisted Surface Plasmon Resonance Biosensor for Detection of CA 15–3. Anal. Chem. 2021, 93, 7815–7824. [Google Scholar] [CrossRef]
- Yu, H.; Tan, X.; Sun, S.; Zhang, L.; Gao, C.; Ge, S. Engineering Paper-Based Visible Light-Responsive Sn-Self Doped Domed SnO2 Nanotubes for Ultrasensitive Photoelectrochemical Sensor. Biosens. Bioelectron. 2021, 185, 113250. [Google Scholar] [CrossRef]
- Wu, Q.; Li, N.; Wang, Y.; Liu, Y.; Xu, Y.; Wei, S.; Wu, J.; Jia, G.; Fang, X.; Chen, F.; et al. A 2D Transition Metal Carbide MXene-Based SPR Biosensor for Ultrasensitive Carcinoembryonic Antigen Detection. Biosens. Bioelectron. 2019, 144, 111697. [Google Scholar] [CrossRef]
- Mo, G.; He, X.; Zhou, C.; Ya, D.; Feng, J.; Yu, C.; Deng, B. A Novel ECL Sensor Based on a Boronate Affinity Molecular Imprinting Technique and Functionalized SiO2@CQDs/AuNPs/MPBA Nanocomposites for Sensitive Determination of Alpha-Fetoprotein. Biosens. Bioelectron. 2019, 126, 558–564. [Google Scholar] [CrossRef]
- Li, S.; Liu, X.; Liu, S.; Guo, M.; Liu, C.; Pei, M. Fluorescence Sensing Strategy Based on Aptamer Recognition and Mismatched Catalytic Hairpin Assembly for Highly Sensitive Detection of Alpha-Fetoprotein. Anal. Chim. Acta 2021, 1141, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Mo, G.; He, X.; Qin, D.; Meng, S.; Wu, Y.; Deng, B. Spatially-Resolved Dual-Potential Sandwich Electrochemiluminescence Immunosensor for the Simultaneous Determination of Carbohydrate Antigen 19–9 and Carbohydrate Antigen 24-2. Biosens. Bioelectron. 2021, 178, 113024. [Google Scholar] [CrossRef] [PubMed]
- Bahari, D.; Babamiri, B.; Salimi, A. An Eco-Friendly MIP-Solid Surface Fluorescence Immunosensor for Detection of CA 19-9 Tumor Marker Using Ni Nanocluster as an Emitter Labels. J. Iran. Chem. Soc. 2020, 17, 2283–2291. [Google Scholar] [CrossRef]
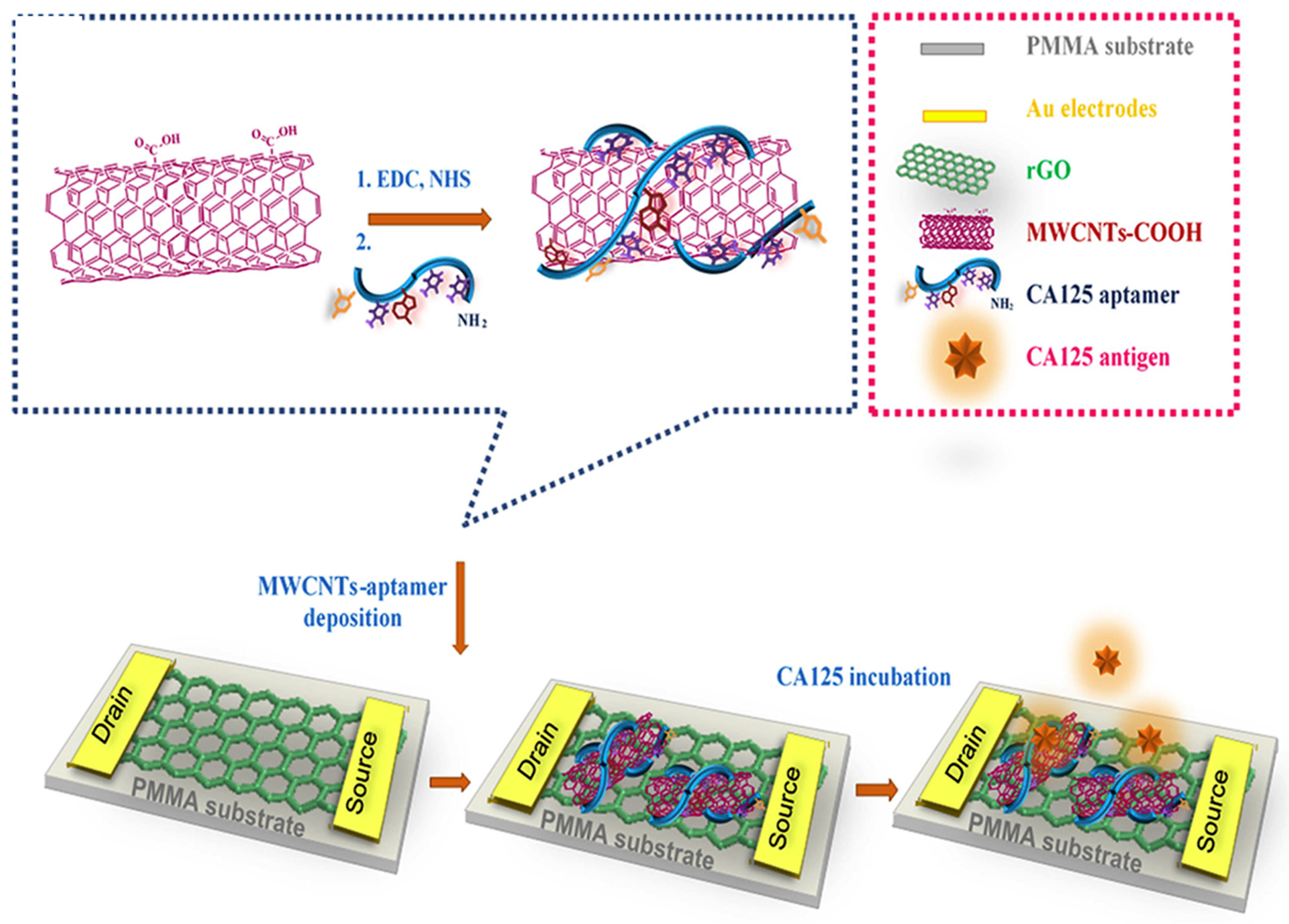
- Mansouri Majd, S.; Salimi, A. Ultrasensitive Flexible FET-Type Aptasensor for CA 125 Cancer Marker Detection Based on Carboxylated Multiwalled Carbon Nanotubes Immobilized onto Reduced Graphene Oxide Film. Anal. Chim. Acta 2018, 1000, 273–282. [Google Scholar] [CrossRef]
- Szymańska, B.; Lukaszewski, Z.; Hermanowicz-Szamatowicz, K.; Gorodkiewicz, E. A Biosensor for Determination of the Circulating Biomarker CA125/MUC16 by Surface Plasmon Resonance Imaging. Talanta 2020, 206, 120187. [Google Scholar] [CrossRef]
- Bai, Y.; Zhang, H.; Zhao, L.; Wang, Y.; Chen, X.; Zhai, H.; Tian, M.; Zhao, R.; Wang, T.; Xu, H.; et al. A Novel Aptasensor Based on HCR and G-Quadruplex DNAzyme for Fluorescence Detection of Carcinoembryonic Antigen. Talanta 2021, 221, 121451. [Google Scholar] [CrossRef]
- Yılmaz, M.; Bakhshpour, M.; Göktürk, I.; Pişkin, A.K.; Denizli, A. Quartz Crystal Microbalance (QCM) Based Biosensor Functionalized by HER2/Neu Antibody for Breast Cancer Cell Detection. Chemosensors 2021, 9, 80. [Google Scholar] [CrossRef]
- Tanaka, S.; Wadati, H.; Sato, K.; Yasuda, H.; Niioka, H. Red-Fluorescent Pt Nanoclusters for Detecting and Imaging HER2 in Breast Cancer Cells. ACS Omega 2020, 5, 23718–23723. [Google Scholar] [CrossRef]
- Xie, Y.; Si, S.; Deng, C.; Wu, H. A Sensitive “Turn-on” Fluorescent Biosensor for the Detection of Biomarkers Based on Three-Dimensional DNA Walker. Talanta 2023, 253, 124071. [Google Scholar] [CrossRef]
- Hu, S.; Xu, H.; Zhou, B.; Xu, S.; Shen, B.; Dong, B.; Yin, Z.; Xu, S.; Sun, L.; Lv, J.; et al. Double Stopband Bilayer Photonic Crystal Based Upconversion Fluorescence PSA Sensor. Sens. Actuators B Chem. 2021, 326, 128816. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, X.; Wang, X.; Yang, M.; Xu, F.; Hou, C.; Huo, D. A Fluorescent Biosensor Based on Prismatic Hollow Metal-Polydopamine Frameworks and 6-Carboxyfluorescein (FAM)-Labeled Protein Aptamer for CA15-3 Detection. Sens. Actuators B Chem. 2021, 329, 129249. [Google Scholar] [CrossRef]
- Othman, H.O.; Salehnia, F.; Fakhri, N.; Hassan, R.; Hosseini, M.; Faizullah, A.; Ganjali, M.R.; Kazem Aghamir, S.M. A Highly Sensitive Fluorescent Immunosensor for Sensitive Detection of Nuclear Matrix Protein 22 as Biomarker for Early Stage Diagnosis of Bladder Cancer. RSC Adv. 2020, 10, 28865–28871. [Google Scholar] [CrossRef] [PubMed]
- Othman, H.O.; Salehnia, F.; Hosseini, M.; Hassan, R.; Faizullah, A.; Ganjali, M.R. Fluorescence Immunoassay Based on Nitrogen Doped Carbon Dots for the Detection of Human Nuclear Matrix Protein NMP22 as Biomarker for Early Stage Diagnosis of Bladder Cancer. Microchem. J. 2020, 157, 104966. [Google Scholar] [CrossRef]
- Satyanarayana, M.; Yugender Goud, K.; Koteshwara Reddy, K.; Vengatajalabathy Gobi, K. Conducting Polymer-Layered Carbon Nanotube as Sensor Interface for Electrochemical Detection of Dacarbazine In-Vitro. Electrocatalysis 2017, 8, 214–223. [Google Scholar] [CrossRef]
- Goud, K.Y.; Satyanarayana, M.; Hayat, A.; Gobi, K.V.; Marty, J.L. Nanomaterial-Based Electrochemical Sensors in Pharmaceutical Applications. In Nanoparticles in Pharmacotherapy; Elsevier: Amsterdam, The Netherlands, 2019; pp. 195–216. ISBN 9780128165041. [Google Scholar]
- Kummari, S.; Sunil Kumar, V.; Vengatajalabathy Gobi, K. Facile Electrochemically Reduced Graphene Oxide-Multi-walled Carbon Nanotube Nanocomposite as Sensitive Probe for In-vitro Determination of Nitrofurantoin in Biological Fluids. Electroanalysis 2020, 32, 2452–2462. [Google Scholar] [CrossRef]
- Shekher, K.; Sampath, K.; Vandini, S.; Satyanarayana, M.; Vengatajalabathy Gobi, K. Gold Nanoparticle Assimilated Polymer Layer on Carbon Nanotube Matrices for Sensitive Detection of Serotonin in Presence of Dopamine In-Vitro. Inorg. Chim. Acta 2023, 549, 121399. [Google Scholar] [CrossRef]
- Yang, H.; Xu, Y.; Hou, Q.; Xu, Q.; Ding, C. Magnetic Antifouling Material Based Ratiometric Electrochemical Biosensor for the Accurate Detection of CEA in Clinical Serum. Biosens. Bioelectron. 2022, 208, 114216. [Google Scholar] [CrossRef]
- Pacheco, J.G.; Silva, M.S.V.; Freitas, M.; Nouws, H.P.A.; Delerue-Matos, C. Molecularly Imprinted Electrochemical Sensor for the Point-of-Care Detection of a Breast Cancer Biomarker (CA 15-3). Sens. Actuators B Chem. 2018, 256, 905–912. [Google Scholar] [CrossRef] [Green Version]
- Wei, B.; Mao, K.; Liu, N.; Zhang, M.; Yang, Z. Graphene Nanocomposites Modified Electrochemical Aptamer Sensor for Rapid and Highly Sensitive Detection of Prostate Specific Antigen. Biosens. Bioelectron. 2018, 121, 41–46. [Google Scholar] [CrossRef]
- Farzin, L.; Sadjadi, S.; Shamsipur, M.; Sheibani, S.; Mousazadeh, M. hasan Employing AgNPs Doped Amidoxime-Modified Polyacrylonitrile (PAN-Oxime) Nanofibers for Target Induced Strand Displacement-Based Electrochemical Aptasensing of CA125 in Ovarian Cancer Patients. Mater. Sci. Eng. C 2019, 97, 679–687. [Google Scholar] [CrossRef]
- Shekari, Z.; Zare, H.R.; Falahati, A. Dual Assaying of Breast Cancer Biomarkers by Using a Sandwich–Type Electrochemical Aptasensor Based on a Gold Nanoparticles–3D Graphene Hydrogel Nanocomposite and Redox Probes Labeled Aptamers. Sens. Actuators B Chem. 2021, 332, 129515. [Google Scholar] [CrossRef]
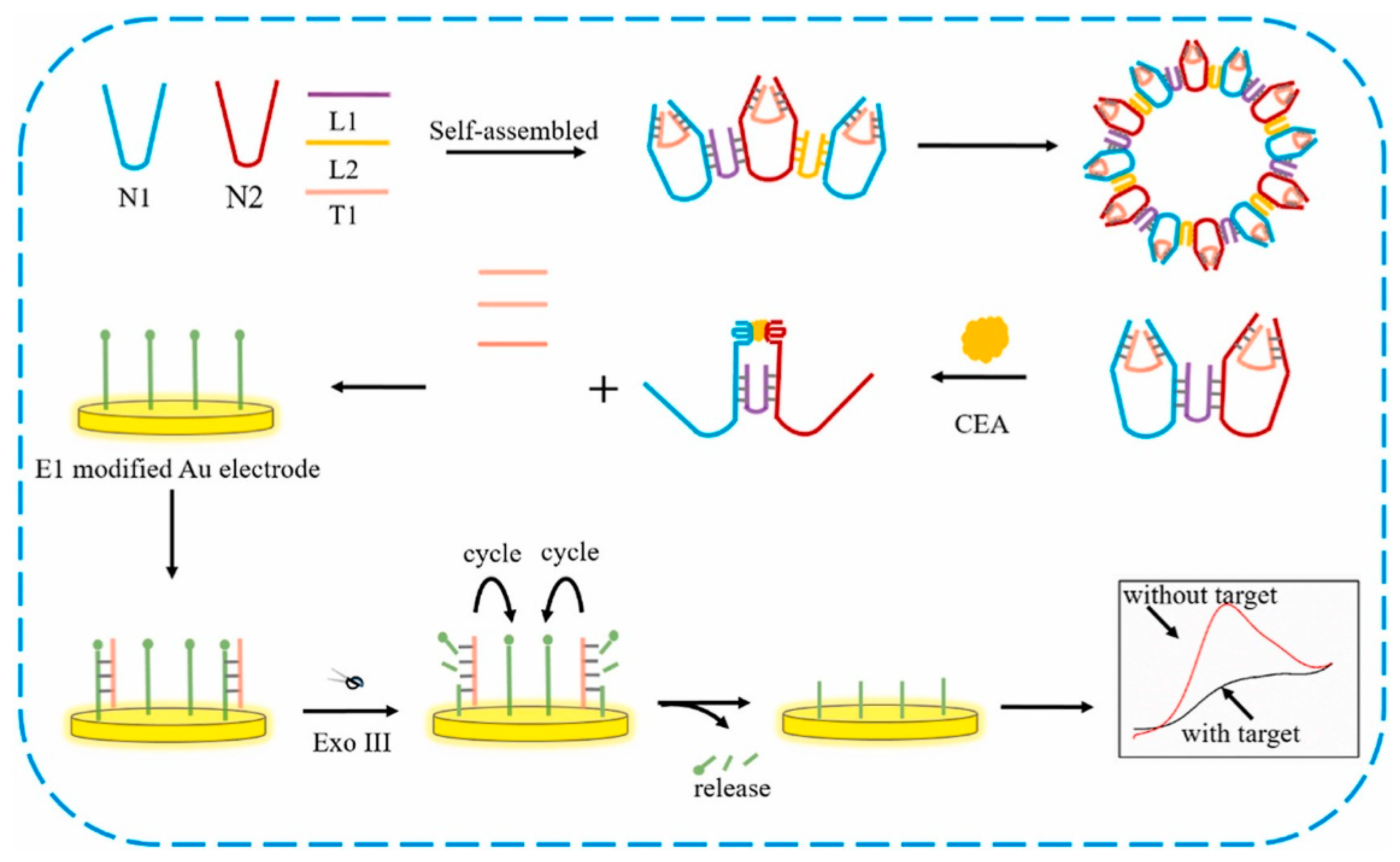
- Ji, Y.; Guo, J.; Ye, B.; Peng, G.; Zhang, C.; Zou, L. An Ultrasensitive Carcinoembryonic Antigen Electrochemical Aptasensor Based on 3D DNA Nanoprobe and Exo III. Biosens. Bioelectron. 2022, 196, 113741. [Google Scholar] [CrossRef] [PubMed]
- Taheri, N.; Khoshsafar, H.; Ghanei, M.; Ghazvini, A.; Bagheri, H. Dual-Template Rectangular Nanotube Molecularly Imprinted Polypyrrole for Label-Free Impedimetric Sensing of AFP and CEA as Lung Cancer Biomarkers. Talanta 2022, 239, 123146. [Google Scholar] [CrossRef]
- Upan, J.; Youngvises, N.; Tuantranont, A.; Karuwan, C.; Banet, P.; Aubert, P.H.; Jakmunee, J. A Simple Label-Free Electrochemical Sensor for Sensitive Detection of Alpha-Fetoprotein Based on Specific Aptamer Immobilized Platinum Nanoparticles/Carboxylated-Graphene Oxide. Sci. Rep. 2021, 11, 13969. [Google Scholar] [CrossRef]
- Castaño-Guerrero, Y.; Romaguera-Barcelay, Y.; Moreira, F.T.C.; Brito, W.R.; Fortunato, E.; Sales, M.G.F. Poly(Thionine)-Modified Screen-Printed Electrodes for CA 19-9 Detection and Its Properties in Raman Spectroscopy. Chemosensors 2022, 10, 92. [Google Scholar] [CrossRef]
- Yola, M.L.; Atar, N. Carbohydrate Antigen 19-9 Electrochemical Immunosensor Based on 1D-MoS2 Nanorods/LiNb3O8 and Polyoxometalate-Incorporated Gold Nanoparticles. Microchem. J. 2021, 170, 106643. [Google Scholar] [CrossRef]
- Rebelo, T.S.C.R.; Costa, R.; Brandão, A.T.S.C.; Silva, A.F.; Sales, M.G.F.; Pereira, C.M. Molecularly Imprinted Polymer SPE Sensor for Analysis of CA-125 on Serum. Anal. Chim. Acta 2019, 1082, 126–135. [Google Scholar] [CrossRef]
- Wang, M.; Hu, M.; Li, Z.; He, L.; Song, Y.; Jia, Q.; Zhang, Z.; Du, M. Construction of Tb-MOF-on-Fe-MOF Conjugate as a Novel Platform for Ultrasensitive Detection of Carbohydrate Antigen 125 and Living Cancer Cells. Biosens. Bioelectron. 2019, 142, 111536. [Google Scholar] [CrossRef]
- Freitas, M.; Nouws, H.P.A.; Delerue-Matos, C. Electrochemical Sensing Platforms for HER2-ECD Breast Cancer Biomarker Detection. Electroanalysis 2019, 31, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Shen, C.; Yang, M.; Rasooly, A. Polycytosine DNA Electric-Current-Generated Immunosensor for Electrochemical Detection of Human Epidermal Growth Factor Receptor 2 (HER2). Anal. Chem. 2018, 90, 4764–4769. [Google Scholar] [CrossRef]
- Wang, W.; Han, R.; Chen, M.; Luo, X. Antifouling Peptide Hydrogel Based Electrochemical Biosensors for Highly Sensitive Detection of Cancer Biomarker HER2 in Human Serum. Anal. Chem. 2021, 93, 7355–7361. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, J.G.; Rebelo, P.; Freitas, M.; Nouws, H.P.A.; Delerue-Matos, C. Breast Cancer Biomarker (HER2-ECD) Detection Using a Molecularly Imprinted Electrochemical Sensor. Sens. Actuators B Chem. 2018, 273, 1008–1014. [Google Scholar] [CrossRef]
- Díaz-Fernández, A.; Miranda-Castro, R.; De-los-Santos-Álvarez, N.; Lobo-Castañón, M.J.; Estrela, P. Impedimetric Aptamer-Based Glycan PSA Score for Discrimination of Prostate Cancer from Other Prostate Diseases. Biosens. Bioelectron. 2021, 175, 112872. [Google Scholar] [CrossRef] [PubMed]
- Hasanzadeh, M.; Tagi, S.; Solhi, E.; Mokhtarzadeh, A.; Shadjou, N.; Eftekhari, A.; Mahboob, S. An Innovative Immunosensor for Ultrasensitive Detection of Breast Cancer Specific Carbohydrate (CA 15-3) in Unprocessed Human Plasma and MCF-7 Breast Cancer Cell Lysates Using Gold Nanospear Electrochemically Assembled onto Thiolated Graphene Quantum Dots. Int. J. Biol. Macromol. 2018, 114, 1008–1017. [Google Scholar] [CrossRef] [PubMed]
- Rong, S.; Zou, L.; Zhu, Y.; Zhang, Z.; Liu, H.; Zhang, Y.; Zhang, H.; Gao, H.; Guan, H.; Dong, J.; et al. 2D/3D Material Amplification Strategy for Disposable Label-Free Electrochemical Immunosensor Based on RGO-TEPA@Cu-MOFs@SiO2@AgNPs Composites for NMP22 Detection. Microchem. J. 2021, 168, 106410. [Google Scholar] [CrossRef]
- Zhao, S.; Zhang, Y.; Ding, S.; Fan, J.; Luo, Z.; Liu, K.; Shi, Q.; Liu, W.; Zang, G. A Highly Sensitive Label-Free Electrochemical Immunosensor Based on AuNPs-PtNPs-MOFs for Nuclear Matrix Protein 22 Analysis in Urine Sample. J. Electroanal. Chem. 2019, 834, 33–42. [Google Scholar] [CrossRef]
- Li, S.; Yue, S.; Yu, C.; Chen, Y.; Yuan, D.; Yu, Q. A Label-Free Immunosensor for the Detection of Nuclear Matrix Protein-22 Based on a Chrysanthemum-like Co-MOFs/CuAu NWs Nanocomposite. Analyst 2019, 144, 649–655. [Google Scholar] [CrossRef]
- Goud, K.Y.; Reddy, K.K.; Khorshed, A.; Kumar, V.S.; Mishra, R.K.; Oraby, M.; Ibrahim, A.H.; Kim, H.; Gobi, K.V. Electrochemical Diagnostics of Infectious Viral Diseases: Trends and Challenges. Biosens. Bioelectron. 2021, 180, 113112. [Google Scholar] [CrossRef]
- Ruiz-Valdepeñas Montiel, V.; Sempionatto, J.R.; Esteban-Fernández de Ávila, B.; Whitworth, A.; Campuzano, S.; Pingarrón, J.M.; Wang, J. Delayed Sensor Activation Based on Transient Coatings: Biofouling Protection in Complex Biofluids. J. Am. Chem. Soc. 2018, 140, 14050–14053. [Google Scholar] [CrossRef]
- Ghafar-Zadeh, E. Wireless Integrated Biosensors for Point-of-Care Diagnostic Applications. Sensors 2015, 15, 3236–3261. [Google Scholar] [CrossRef] [Green Version]






| No. | Biomarker | Recognition | Method | Linear Range | LOD | Ref. |
|---|---|---|---|---|---|---|
| 1 | AFP | SiO2@CQDs/AuNPs/MPBA | ECL | 0.001–1000 ng/mL | 0.0004 ng/mL | [204] |
| 2 | AFP | 1D SnO2 NTs | PEC | 10 pg mL−1–200 ng mL−1 | 3.84 pg mL−1 | [202] |
| 3 | AFP | aptamer-MCHA | Fluorescence | 0.1 ng mL−1–10 mgmL−1 | 0.033 ng. mL −1 | [205] |
| 4 | CA 19-9 | luminol-AgNPs@ZIF-67 | ECL | 0.0001–10 U/mL | 31 μU/mL | [206] |
| 5 | CA 19-9 | Ni NCs-Ab2 | Fluorescence | 0.001–48 ng mL−1 | 0.00013 ng mL−1 | [207] |
| 6 | CA 125 | rGO-based FET-type aptasensor | Fluorescence | 1.0 × 10−9-1.0 U/mL | 5.0 × 10−10 U/mL | [208] |
| 7 | CA 125 | CA 125/MUC16 | SPRI | 2.2–150 U/ml | - | [209] |
| 8 | CEA | Ti3C2-MXene/AuNPs/SPA | SPR | 2 × 10−16–2 × 10−8 M | 0.07 fM | [203] |
| 9 | CEA | HCR and G-quadruplex DNAzyme | Fluorescence | 0.25–1.5 nM | 0.2 nM | [210] |
| 10 | HER2 | nanoparticle coated QCM | QCM | 10–500 cells/mL | 10 cells/mL | [211] |
| 11 | HER2 | PtAmi | Fluorescence | - | - | [212] |
| 12 | HER2 | 3D DNA walker | Fluorescence | 0.5–5 ng mL−1 | 0.01 ng mL−1 | [213] |
| 13 | PSA | NaYF4:Yb3+, Er3+ UCNPs and NaYF4:Yb3+, Er3+@NaYF4:Yb3+ UCNPs | Fluorescence | 0.1 ng/mL–10 ng/mL | 0.01 ng/mL | [214] |
| 14 | PSA | anti-PSA/MCH/ AgNPs/SiNWs | SERS | 0.1–20 μg·L−1 | 0.1 μg·L−1 | [199] |
| 15 | PSA | IDC | FET | 0.1−10.0 μL/mL | - | [200] |
| 16 | CA-15-3 | PHMPF | Fluorescence | 2.56 × 10−5–1.28 U mL−1 | 2.56 × 10−5 U mL−1 | [215] |
| 17 | CA-15-3 | SPR gold substrates | SPR | - | 0.0998 U mL−1 | [201] |
| 18 | NMP 22 | orange emitting quantum dot CdTe/CdS | Fluorescence | 2–22 pg mL−1 | 0.05 pg mL−1 | [216] |
| 19 | NMP 22 | NCDs | Fluorescence | 1.3–16.3 ng/mL | 0.047 ng/mL | [217] |
| No. | Biomarker | Recognition | Method | Linear Range | LOD | Ref. |
|---|---|---|---|---|---|---|
| 1 | AFP | PtNPs/GO-COOH | SWV | 3.0–30 ng mL−1 | 1.22 ng mL−1 | [229] |
| 2 | AFP | FTO/PPy-MO DMIP | EIS | 10–104 pg mL−1 | 3.3 pg mL−1 | [228] |
| 3 | CA 19-9 | Au-SPE/TH | DPV | 0.010–10 U/mL | - | [230] |
| 4 | CA 19-9 | 1DMoS2 nanorods/LiNb3O8 and AuNPs@POM | DPV | 0.1–10.0 µU mL− 1 | 0.030 µU mL− 1 | [231] |
| 5 | CA 125 | MIP@AuSPE | SWV | 0.01 and 500 U/mL | 0.1 U/mL | [232] |
| 6 | CA 125 | ITO/Ag NPs–PAN-oxime NFs/aptamer/c-DNA–MB | DPV | 0.01 to 350 UmL−1 | 0.0042 UmL−1 | [225] |
| 7 | CA 125 | Tb-MOF-on- Fe-MOF | EIS | 1 × 102−1 × 105 cell·mL−1 | 19 cell·mL−1 | [233] |
| 8 | CEA | MXC-Fe3O4-Ru | DPV | 1 pg/mL–1 μg/mL | 0.62 pg/mL | [222] |
| 9 | CEA | IEC-BA | DPV | - | 4.88 fg mL−1 | [227] |
| 10 | HER2 | SPCE-MWCNT/AuNP | LSV | 7.5 and 50 ng/mL | 0.16 ng/mL | [234] |
| 11 | HER2 | polycytosine DNA (dC20) | SWV | 0.001−1 ng/mL | 0.5 pg/mL | [235] |
| 12 | HER2 | GCE/PEDOT/Gel/Ab/HER2 | DPV | 0.1 ng mL−1–1.0 μg mL−1 | 45 pg mL−1 | [236] |
| 13 | HER2 | MIP-AuSPE | DPV | 10–70 ng/mL | 1.6 ng/L | [237] |
| 14 | PSA | AuNPs/rGO/THI-aptamer | DPV | 0.05 to 200 ng mL−1 | 10 pg mL−1 | [224] |
| 15 | PSA | aptamer PSAG-1 | EIS | 0.64–62.5 ng/mL | - | [238] |
| 16 | CA-15-3 | AuNPs/3DGH | DPV | 5.0 × 10–2–100.0 U mL–1 | - | [226] |
| 17 | CA-15-3 | MIP/Au-SPE | DPV | 5–50 U mL−1 | 1.5 U mL−1 | [223] |
| 18 | CA-15-3 | CysA/Au NSs/GQDs | SWV | 0.16–125 U/mL | 0.11 U/ml | [239] |
| 19 | NMP 22 | Cu-MOFs@SiO2@AgNPs | DPV | 0.1 pg∙mL−1–1000 ng∙mL−1 | 33.33 fg∙mL−1 | [240] |
| 20 | NMP 22 | AuNPs-PtNPs-MOFs | DPV | 0.005 ng·mL−1 –20 ng·mL−1 | 1.7 pg·mL−1 | [241] |
| 21 | NMP 22 | Co-MOFs/CuAu NWs | Amperometric | 0.1 pg mL−1–1 ng mL−1 | 33 fg mL−1 | [242] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao Bommi, J.; Kummari, S.; Lakavath, K.; Sukumaran, R.A.; Panicker, L.R.; Marty, J.L.; Yugender Goud, K. Recent Trends in Biosensing and Diagnostic Methods for Novel Cancer Biomarkers. Biosensors 2023, 13, 398. https://doi.org/10.3390/bios13030398
Rao Bommi J, Kummari S, Lakavath K, Sukumaran RA, Panicker LR, Marty JL, Yugender Goud K. Recent Trends in Biosensing and Diagnostic Methods for Novel Cancer Biomarkers. Biosensors. 2023; 13(3):398. https://doi.org/10.3390/bios13030398
Chicago/Turabian StyleRao Bommi, Jagadeeswara, Shekher Kummari, Kavitha Lakavath, Reshmi A. Sukumaran, Lakshmi R. Panicker, Jean Louis Marty, and Kotagiri Yugender Goud. 2023. "Recent Trends in Biosensing and Diagnostic Methods for Novel Cancer Biomarkers" Biosensors 13, no. 3: 398. https://doi.org/10.3390/bios13030398