Design and Implementation of a Wearable Accelerometer-Based Motion/Tilt Sensing Internet of Things Module and Its Application to Bed Fall Prevention


Abstract
:1. Introduction
2. Materials and Methods
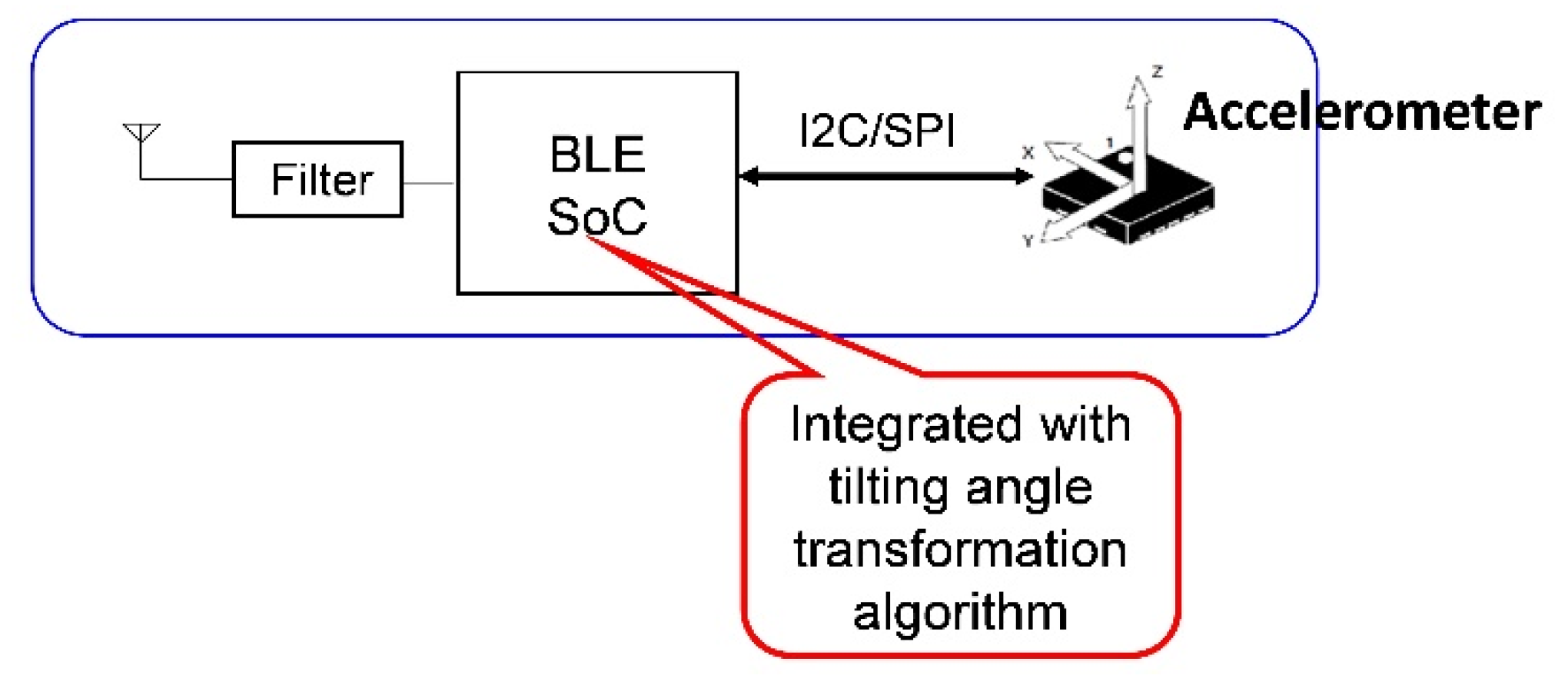
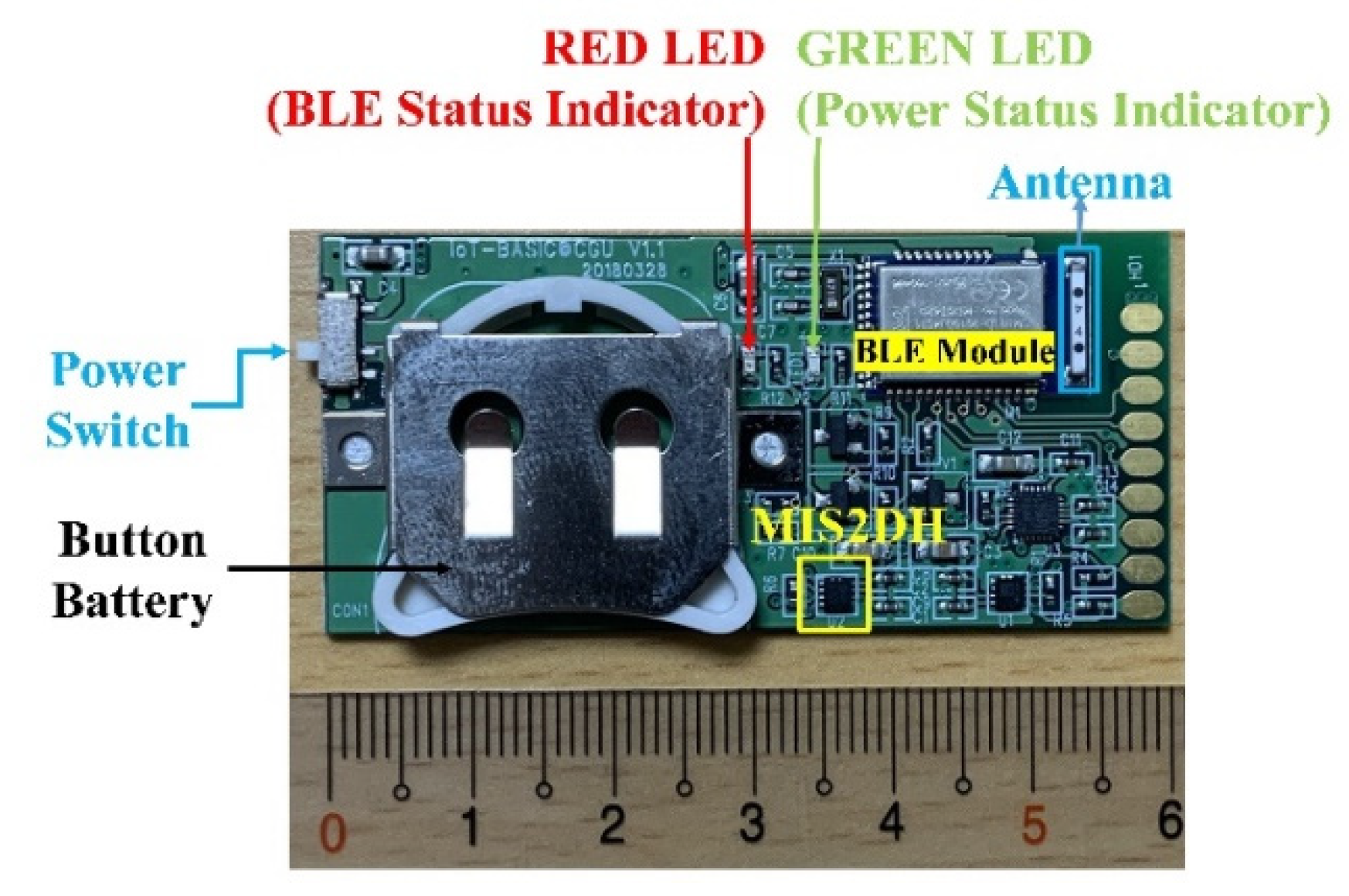
2.1. Design and Implementation of the BASIC Module
2.2. Over-the-Air Feature Configuration of the BASIC Module
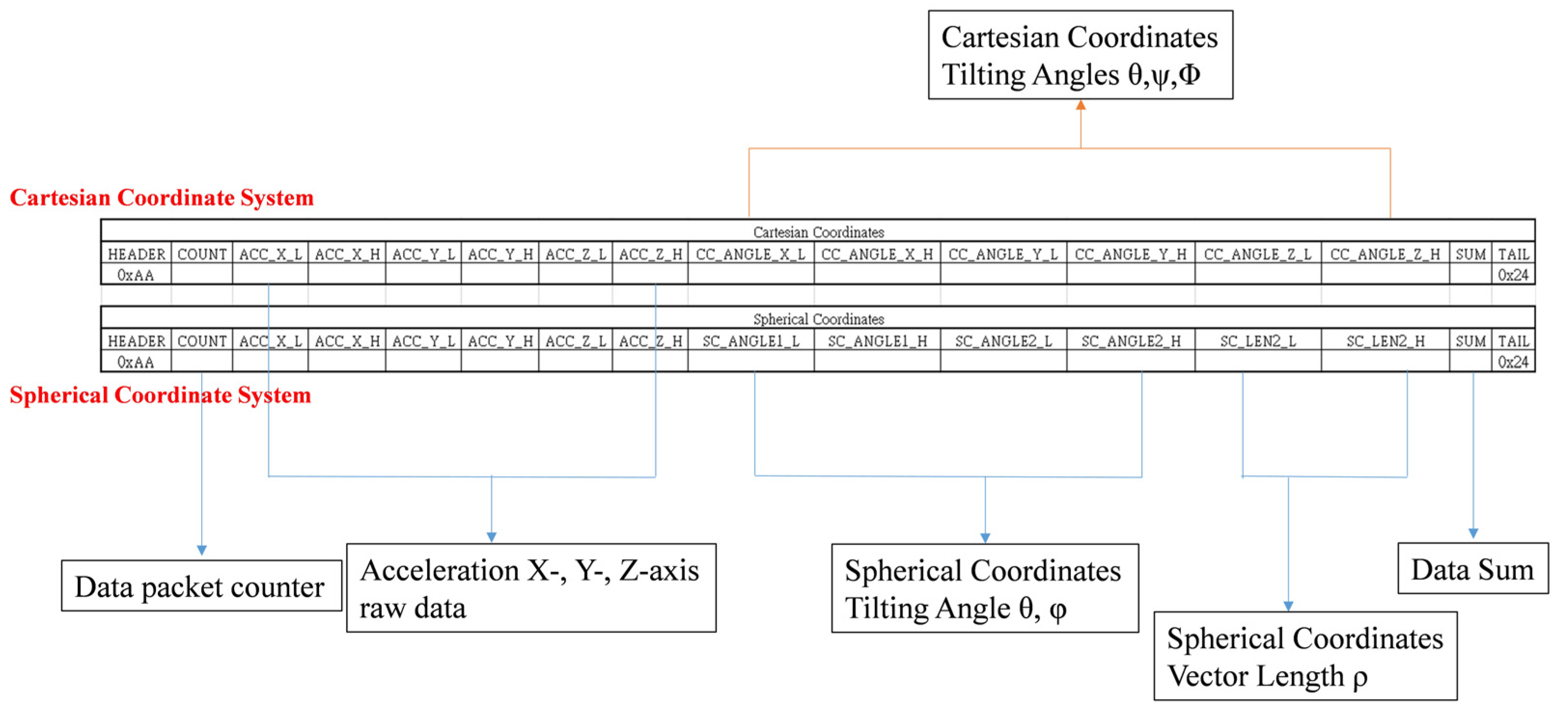
2.3. Data Packet Deign of the BASIC Module
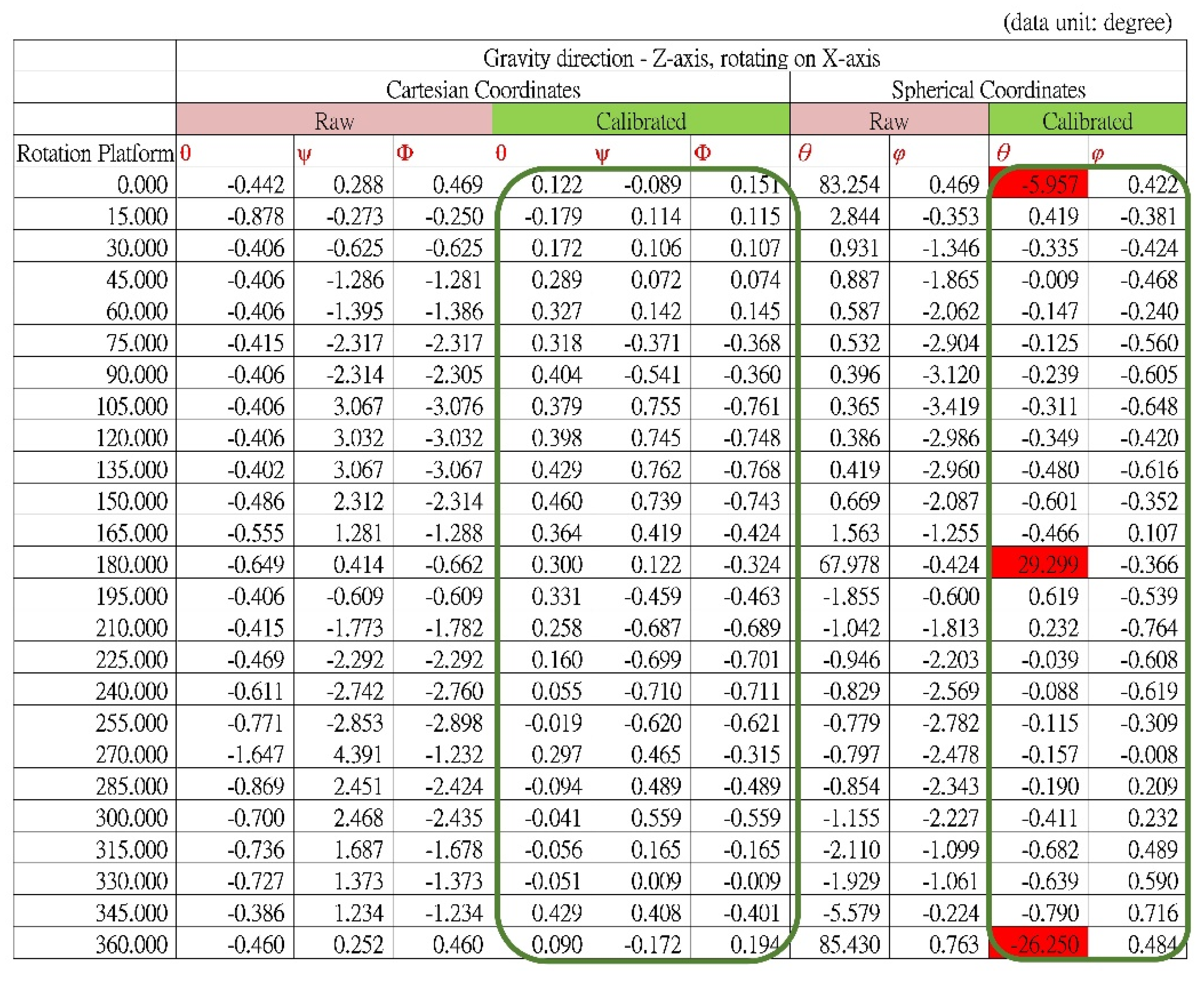
2.4. Calibration of the BASIC Module
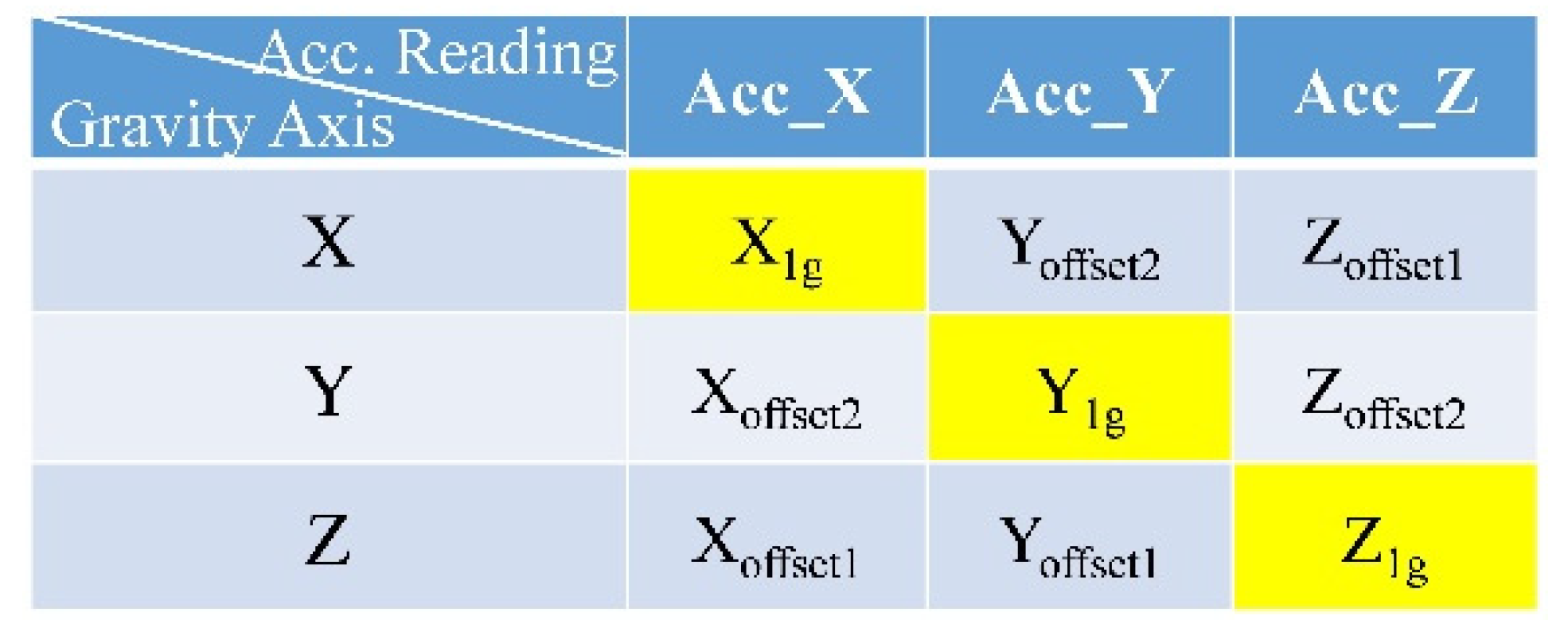
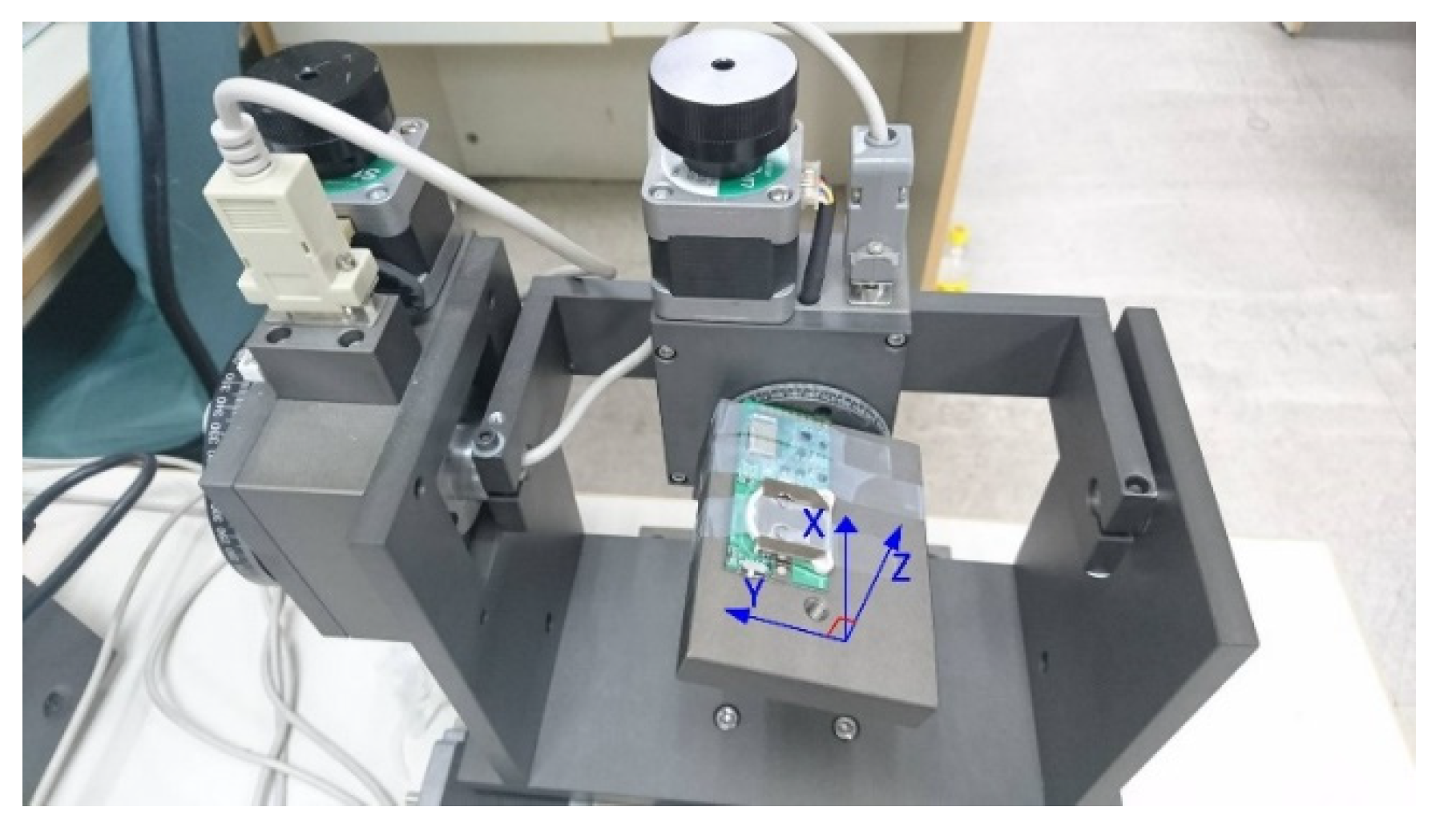
- The rotation platform was perfectly aligned with the horizontal plane, and the module was installed on the surface such that the edge with golden pads was in alignment with the platform’s edge, as shown in Figure 6a. Thus, the z-axis of the module (the orientation of the module shown in Figure 6b) could be aligned with the gravitational force direction. The terms Xoffset1, Yoffset1, and Z1g represent the acceleration data.
- The platform was rotated on the y-axis by 90° so that the x-axis of the module could be aligned with the gravitational force direction, as shown in Figure 6b. The terms X1g, Yoffset2, and Zoffset1 represent the acceleration data.
- From step 1, the platform was rotated on the x-axis by 90° so that the y-axis of the module can be aligned with the gravitational force direction, as shown in Figure 6c. The terms Xoffset2, Y1g, and Zoffset2 represent the acceleration data.
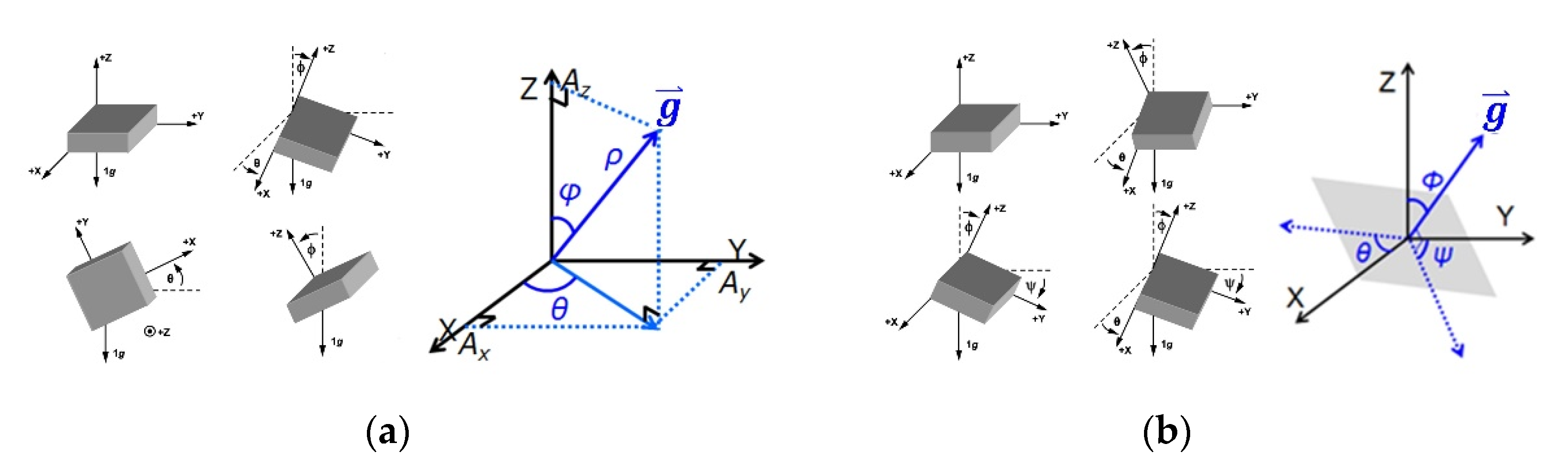
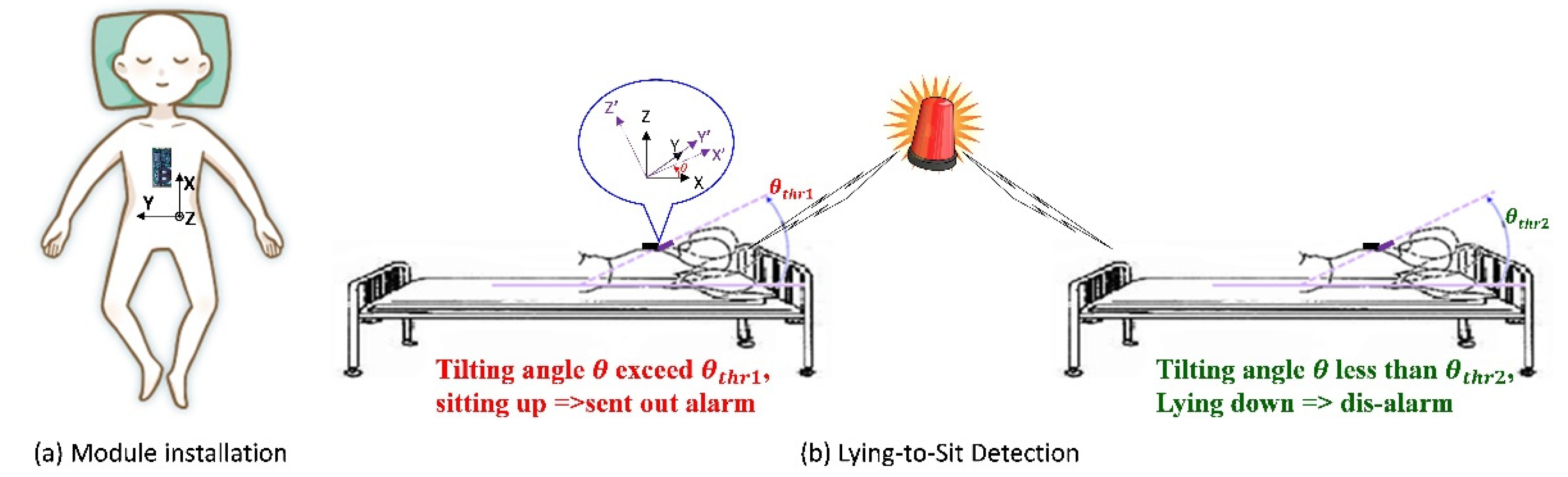
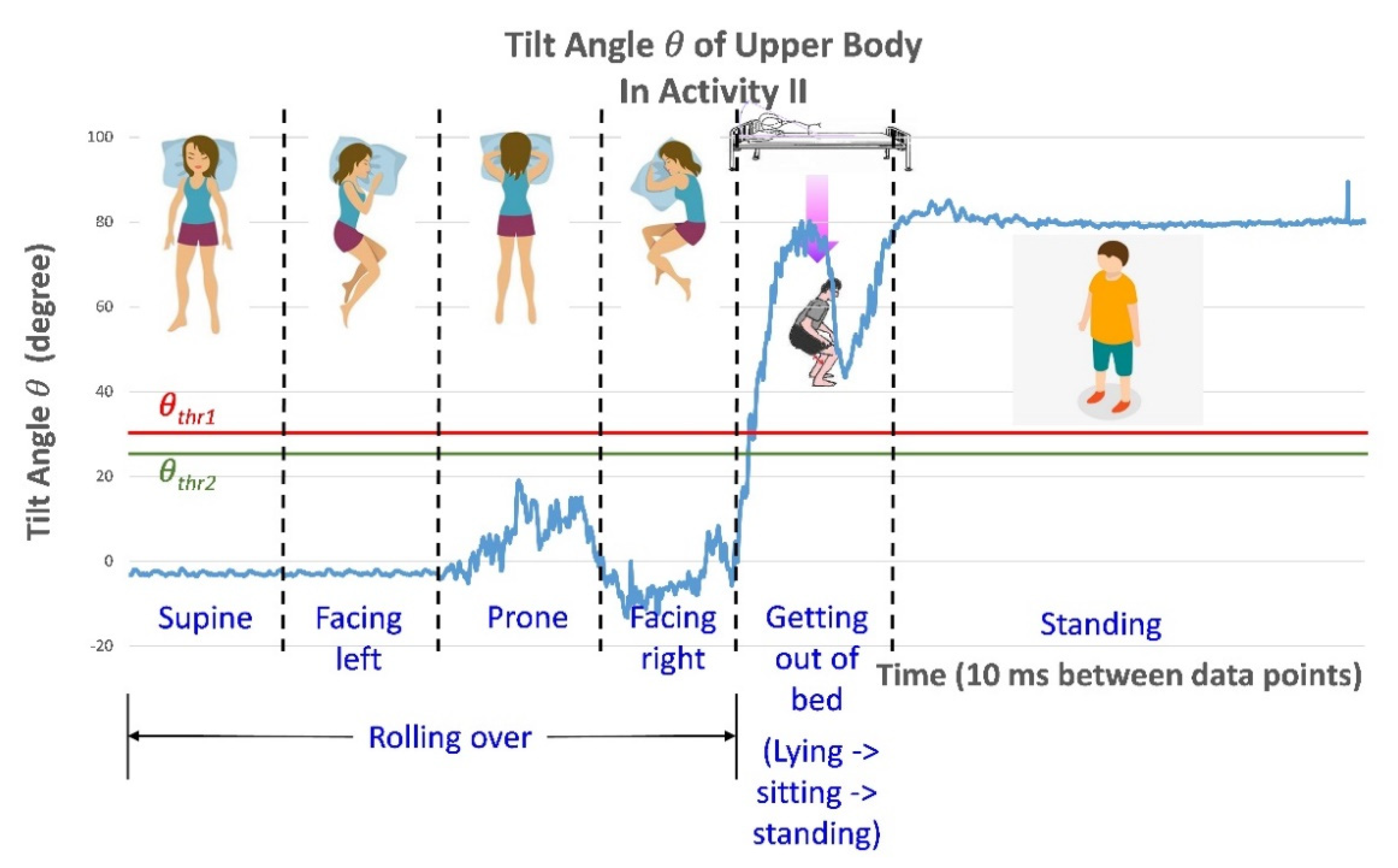
2.5. Posture Change Detection Methodology
3. Results
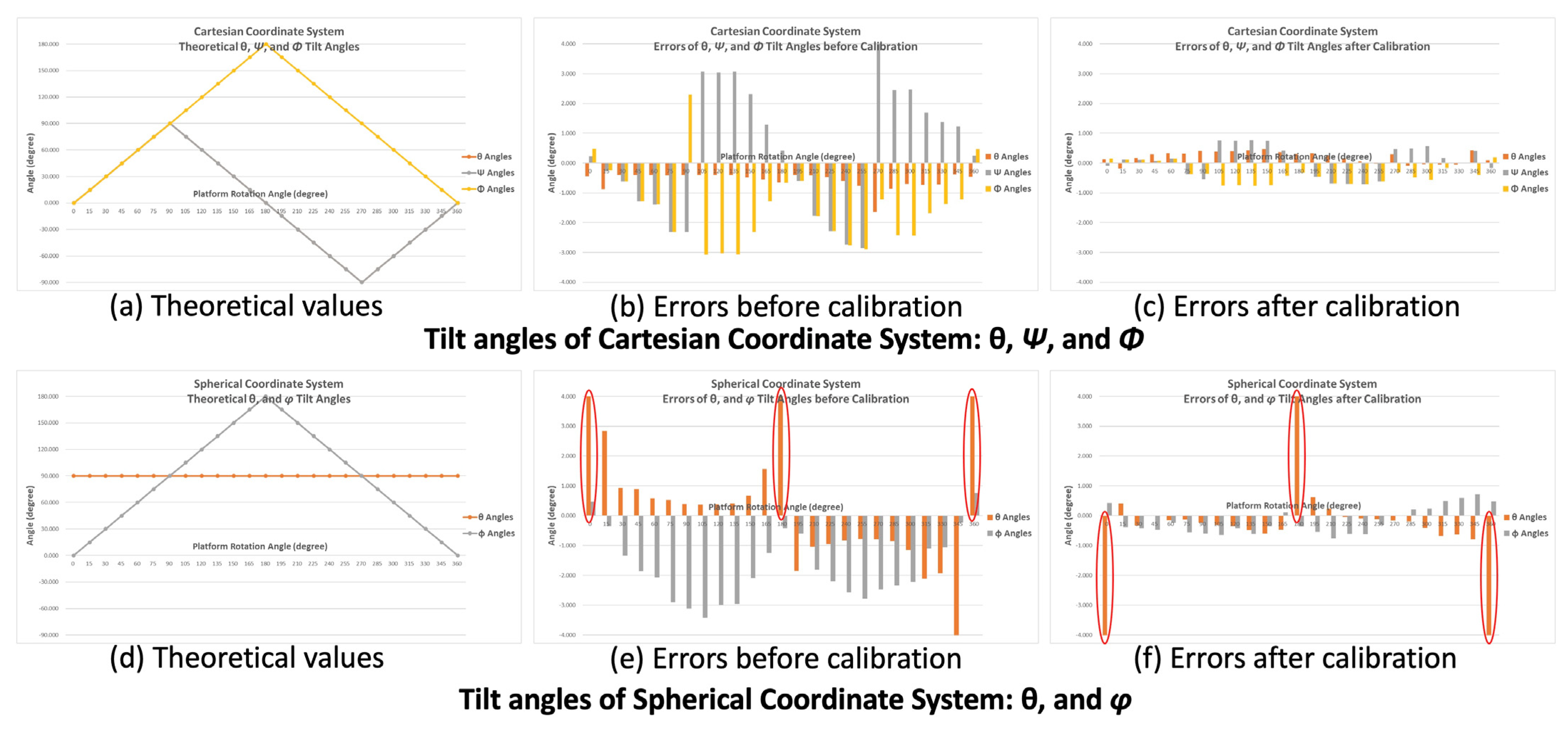
3.1. Subsection Tilt Angle Verification of the BASIC Module
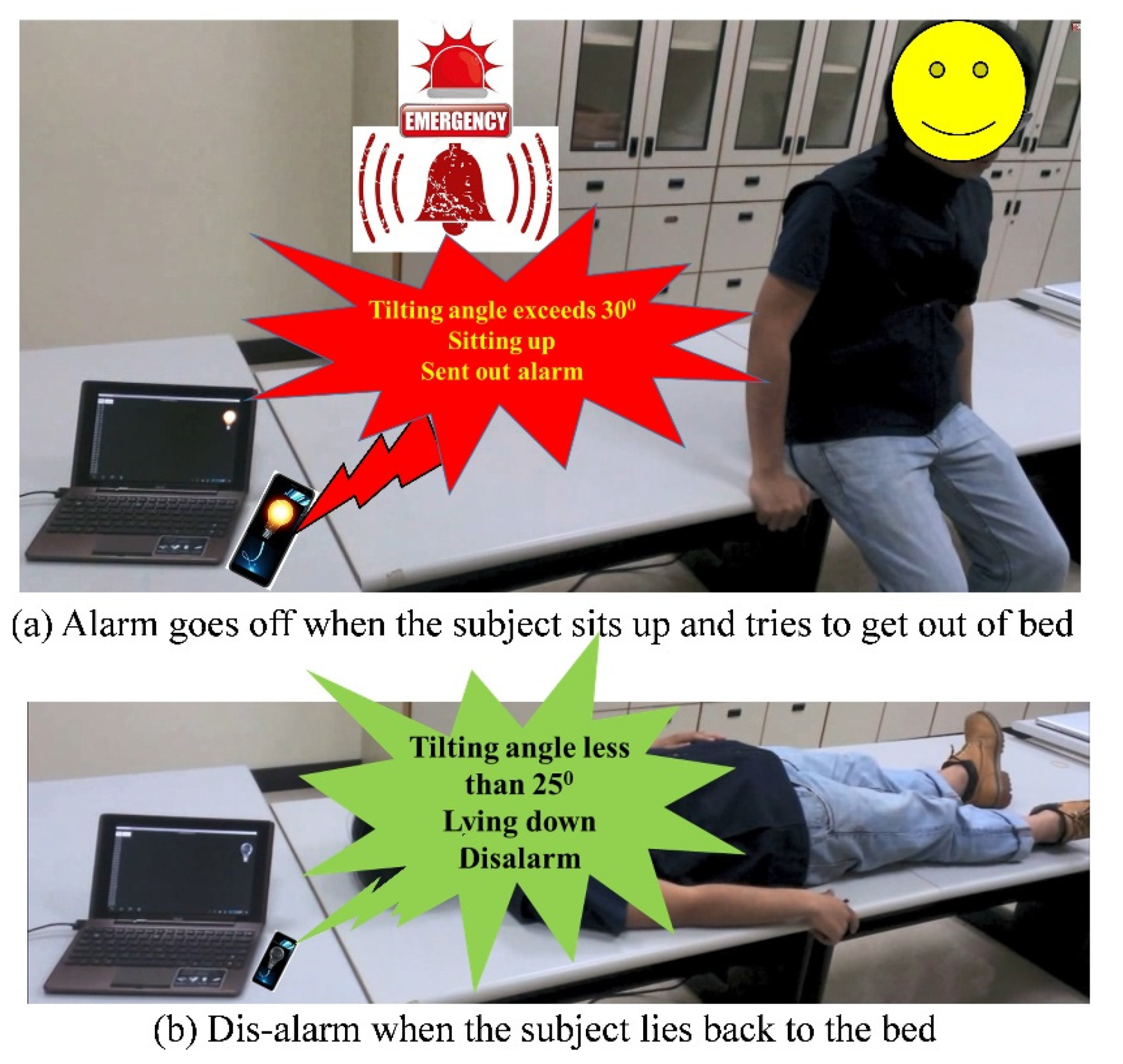
3.2. Development and Implementation for Bed Fall Prevention Application
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Department of Health and Human Services. National Healthcare Disparities Report 2014; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2005.
- Caudill, T.S.; Lofgren, R.; Jennings, C.D.; Karpf, M. Commentary: Health care reform and primary care: Training physicians for tomorrow’s challenges. Acad. Med. 2011, 86, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Hart, L.G.; Goodman, D.C. Geographic access to health care for rural Medicare beneficiaries. J. Rural Health 2006, 22, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Seshadri, D.R.; Li, R.T.; Voos, J.E.; Rowbottom, J.R.; Alfes, C.M.; Zorman, C.A.; Drummond, C.K. Wearable sensors for monitoring the physiological and biochemical profile of the athlete. npj Digit. Med. 2019, 2, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. Neuroeng. Rehabil. 2012, 9, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, R.C.; Lin, Y.; Wang, J.; Liu, G.; Timchalk, C.A. Nanotechnology-based electrochemical sensors for biomonitoring chemical exposures. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Couto, R.A.S.; Quinaz, M.B. Development of a Nafion/MWCNT-SPCE-based portable sensor for the voltammetric analysis of the anti-tuberculosis drug ethambutol. Sensors 2016, 16, 1015. [Google Scholar] [CrossRef] [Green Version]
- Bandodkar, A.J.; Wang, J. Non-invasive wearable electrochemical sensors: A review. Trends Biotechnol. 2014, 32, 363–371. [Google Scholar] [CrossRef]
- Lee, S.; Ha, G.; Wright, D.E.; Ma, Y.; Sen-Gupta, E.; Haubrich, N.R.; Branche, P.C.; Li, W.; Huppert, G.L.; Johnson, M.; et al. Highly flexible, wearable, and disposable cardiac biosensors for remote and ambulatory monitoring. npj Digit. Med. 2018, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Taelman, J.; Adriaensen, T.; van der Horst, C.; Linz, T.; Spaepen, A. Textile Integrated Contactless EMG Sensing for Stress Analysis. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC2007), France, Lyon, France, 23–26 August 2007; pp. 3966–3969. [Google Scholar]
- Park, J.L.; Fairweather, M.M.; Donaldson, D.I. Making the case for mobile cognition: EEG and sports performance. Neurosci. Biobehav. Rev. 2015, 52, 117–130. [Google Scholar] [CrossRef] [Green Version]
- Teng, X.F.; Zhang, Y.T.; Poon, C.C.Y.; Bonato, P. Wearable medical systems for p-Health. IEEE Rev. Biomed. Eng. 2008, 1, 62–74. [Google Scholar] [CrossRef]
- Bonato, P. Wearable sensors and systems. From enabling technology to clinical applications. IEEE Eng. Med. Biol. Mag. 2010, 29, 25–36. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, R.; Weinberg, H. Proceedings of the Five Motion Senses: MEMS Inertial Sensing to Transform Applications; White Papers; Analog Devices Inc.: Wilmington, MA, USA, 2010. [Google Scholar]
- World Health Organization Falls: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/falls (accessed on 16 July 2021).
- Santoyo-Ramón, J.A.; Casilari, E.; Cano-García, J.M. A Study of One-Class Classification Algorithms for Wearable Fall Sensors. Biosensors 2021, 11, 284. [Google Scholar] [CrossRef]
- Wang, X.; Ellul, J.; Azzopardi, G. Elderly Fall Detection Systems: A Literature Survey. Front. Robot. AI 2020, 7, 71–93. [Google Scholar] [CrossRef]
- Li, Q.; Stankovic, J.A.; Hanson, M.A.; Barth, A.T. Accurate, fast fall detection using gyroscopes and accelerometer-derived posture information. In Proceedings of the 6th International Workshop on Wearable and Implantable Body Sensor Network (BSN 2009), Berkeley, CA, USA, 3–5 June 2009; pp. 138–143. [Google Scholar]
- Khan, S.S.; Karg, M.E.; Kuli´c, D.; Hoey, J. Detecting falls with X-factor hidden markov models. Appl. Soft Comput. J. 2017, 55, 168–177. [Google Scholar] [CrossRef] [Green Version]
- Yang, K.; Ahn, C.R.; Vuran, M.C.; Aria, S.S. Semi-supervised near-miss fall detection for ironworkers with a wearable inertial measurement unit. Autom. Constr. 2016, 68, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.S.; Taati, B. Detecting unseen falls from wearable devices using channel-wise ensemble of autoencoders. Expert Syst. Appl. 2017, 87, 280–290. [Google Scholar] [CrossRef] [Green Version]
- Nho, Y.H.; Lim, J.G.; Kwon, D.S. Cluster-analysis-based user-adaptive fall detection using fusion of heart rate sensor and accelerometer in a wearable device. IEEE Access 2020, 8, 40389–40401. [Google Scholar] [CrossRef]
- Oliver, D.; Martin, F.; Seed, P. Preventing patient falls. Age Ageing 2002, 31, 75–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, D.A.; O’Connor, J.A.; Bonadies, J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J. Trauma Acute Care Surg. 2001, 50, 116–119. [Google Scholar] [CrossRef]
- Shorr, R.I.; Chandler, A.M.; Mion, L.C.; Waters, T.M.; Liu, M.; Daniels, M.J.; Kessler, L.A.; Miller, S.T. Effects of an intervention to increase bed alarm use to prevent falls in hospitalized patients: A cluster randomized trial. Ann. Intern. Med. 2012, 157, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Hubbartt, B.; Davis, S.G.; Kautz, D.D. Nurses’ experiences with bed exit alarms may lead to ambivalence about their effectiveness. Rehabil. Nurs. 2011, 36, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Cao, Z.; Xiao, Y.; Mao, J.; Yuan, J. Real-Time Detection of Fall from Bed Using a Single Depth Camera. IEEE Trans. Autom. Sci. Eng. 2019, 16, 1018–1032. [Google Scholar] [CrossRef]
- Bian, Z.P.; Hou, J.; Chau, L.P.; Magnenat-Thalmann, N. Fall detection based on body part tracking using a depth camera. IEEE J. Biomed. Health Inform. 2015, 19, 430–439. [Google Scholar] [CrossRef]
- Jähne-Raden, N.; Kulau, U.; Marschollek, M.; Wolf, K.H. INBED: A Highly Specialized System for Bed-Exit-Detection and Fall Prevention on a Geriatric Ward. Sensors 2019, 19, 1017. [Google Scholar] [CrossRef] [Green Version]
- Chou, W.C.; Lin, W.Y.; Lee, M.Y.; Lei, K.F. Design and assessment of a real-time accelerometer-based lying-to-sit sensing system for bed fall prevention. In Proceedings of the 2013 IEEE International Conference on Systems, Man, and Cybernetics, Manchester, UK, 13–16 October 2013; pp. 1471–1475. [Google Scholar]
- Lin, W.Y.; Chou, W.C.; Shiao, T.H.; Shiao, G.M.; Luo, C.S.; Lee, M.Y. Realization of a CORDIC-Based Plug-In Accelerometer Module for PSG System in Head Position Monitoring for OSAS Patients. J. Healthc. Eng. 2017, 2017, 4728187. [Google Scholar] [CrossRef] [Green Version]
- Riitta, M.; Iman, A.; Amir, M.R.; Aantaa, R.; Terävä, V.; Liljeberg, P.; Salanterä, S. The Internet of Things for basic nursing care—A scoping review. Int. J. Nurs. Stud. 2017, 69, 78–90. [Google Scholar]
- Preece, S.J.; Goulermas, J.Y.; Kenney, L.P.J.; Howard, D. A Comparison of Feature Extraction Methods for the Classification of Dynamic Activities from Accelerometer Data. IEEE Trans. Biomed. Eng. 2009, 56, 871–879. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Options | Descriptions |
|---|---|---|
| Orientation | X, −X, Y, −Y, Z, or −Z | Axis and direction of the accelerometer which is on the same direction of gravity force |
| Coordinates | Cartesian or Spherical | Which coordinate system of the tilting angles will be generated |
| Sensing Range | ±2 g, ±4 g, ±8 g, or ± 16 g | Acceleration sensing range of the accelerometer |
| Output Data Rate (ODR) | 1, 10, 25, 50 or 100 Hz | Output data rate of the module, i.e., accelerometer |
| Output Mode | Real-time, Burst, or Auto | The data packet output mode |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-Y.; Chen, C.-H.; Lee, M.-Y. Design and Implementation of a Wearable Accelerometer-Based Motion/Tilt Sensing Internet of Things Module and Its Application to Bed Fall Prevention. Biosensors 2021, 11, 428. https://doi.org/10.3390/bios11110428
Lin W-Y, Chen C-H, Lee M-Y. Design and Implementation of a Wearable Accelerometer-Based Motion/Tilt Sensing Internet of Things Module and Its Application to Bed Fall Prevention. Biosensors. 2021; 11(11):428. https://doi.org/10.3390/bios11110428
Chicago/Turabian StyleLin, Wen-Yen, Chien-Hung Chen, and Ming-Yih Lee. 2021. "Design and Implementation of a Wearable Accelerometer-Based Motion/Tilt Sensing Internet of Things Module and Its Application to Bed Fall Prevention" Biosensors 11, no. 11: 428. https://doi.org/10.3390/bios11110428