
Pressure Analysis in Rigid and Flexible Real Arteriovenous Fistula with Thickness Variation In Vitro
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Acquisition and Processing
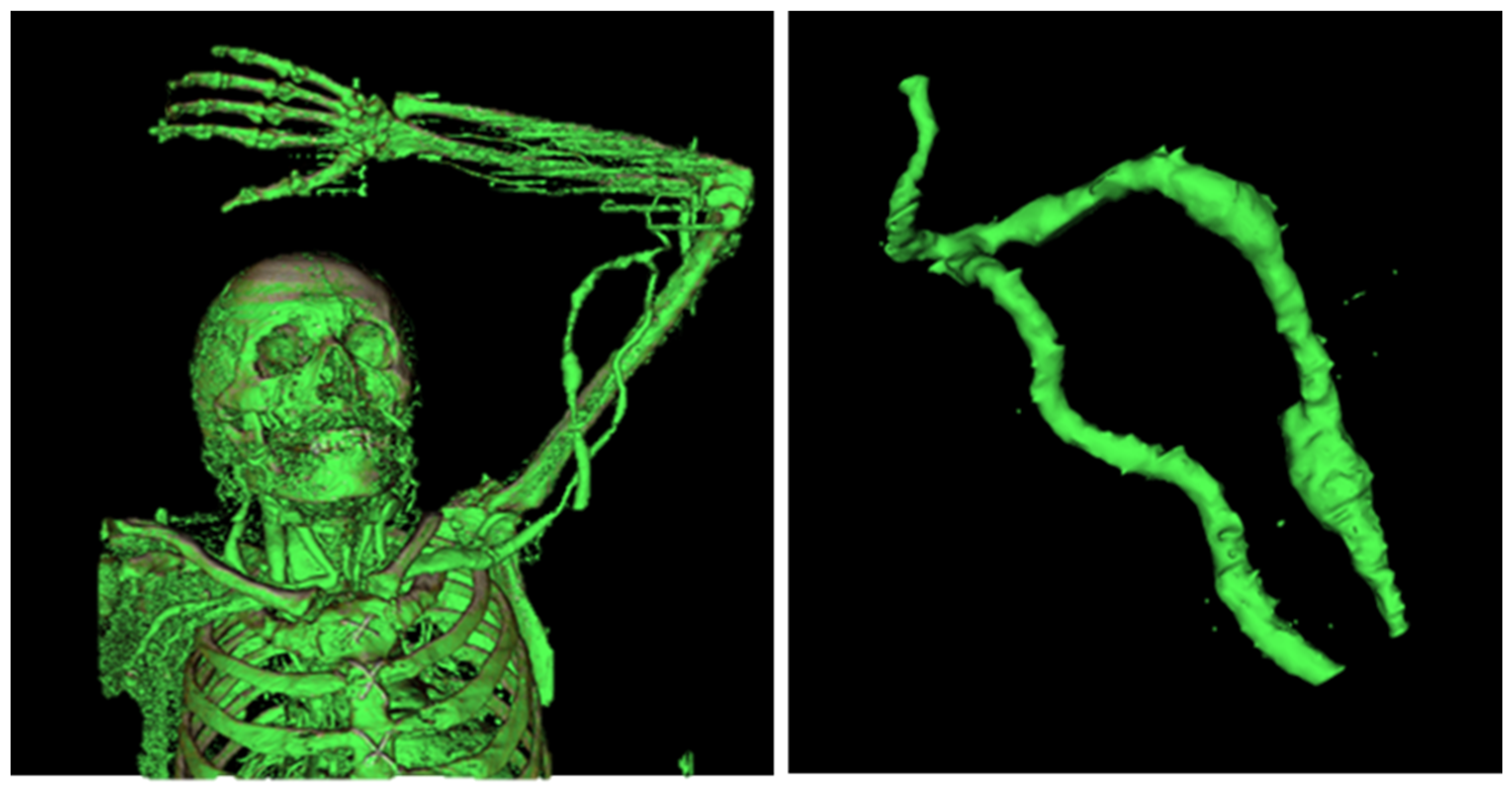
2.1.1. Data Acquisition—Computed Tomography
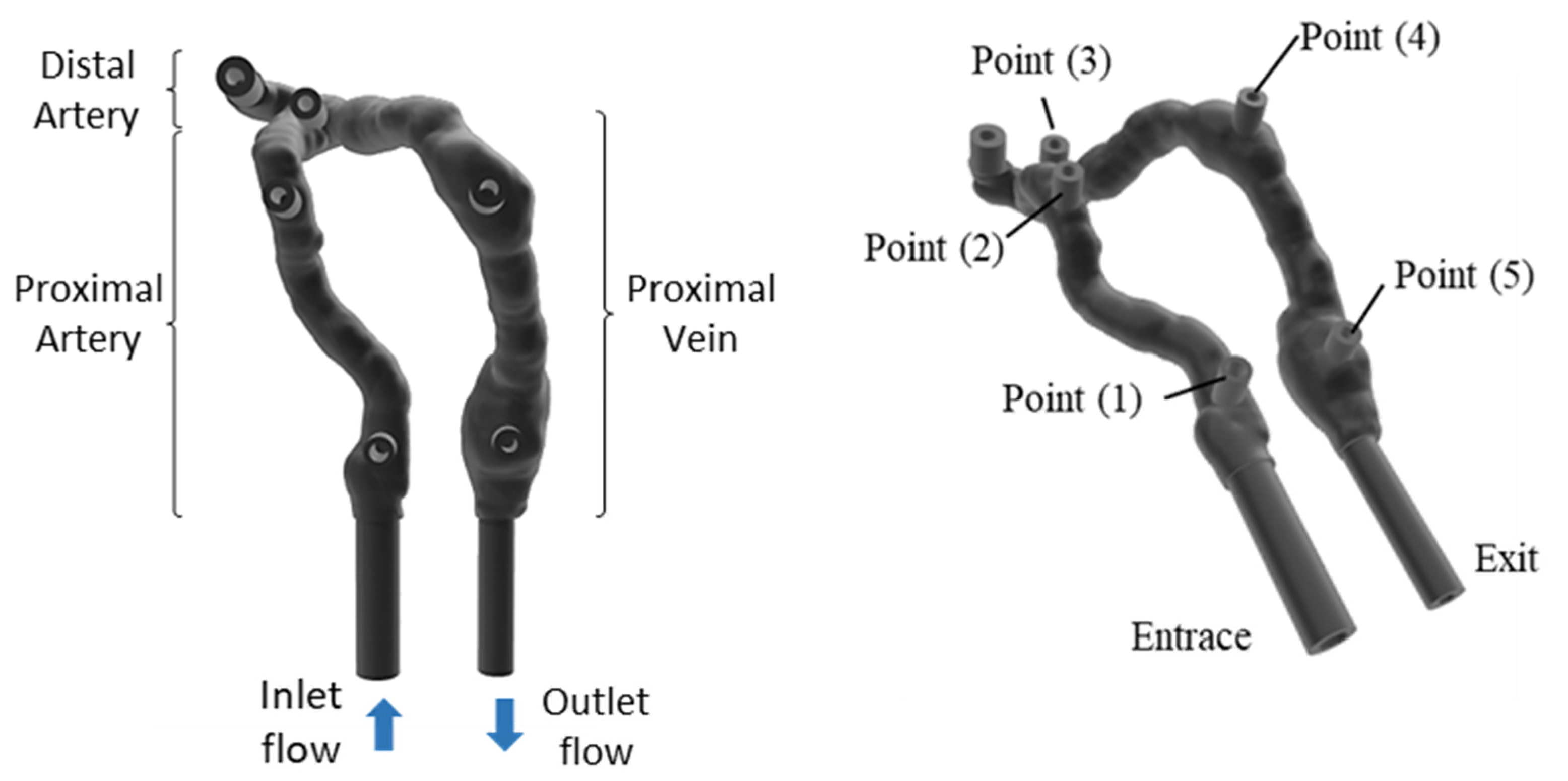
2.1.2. Data Processing
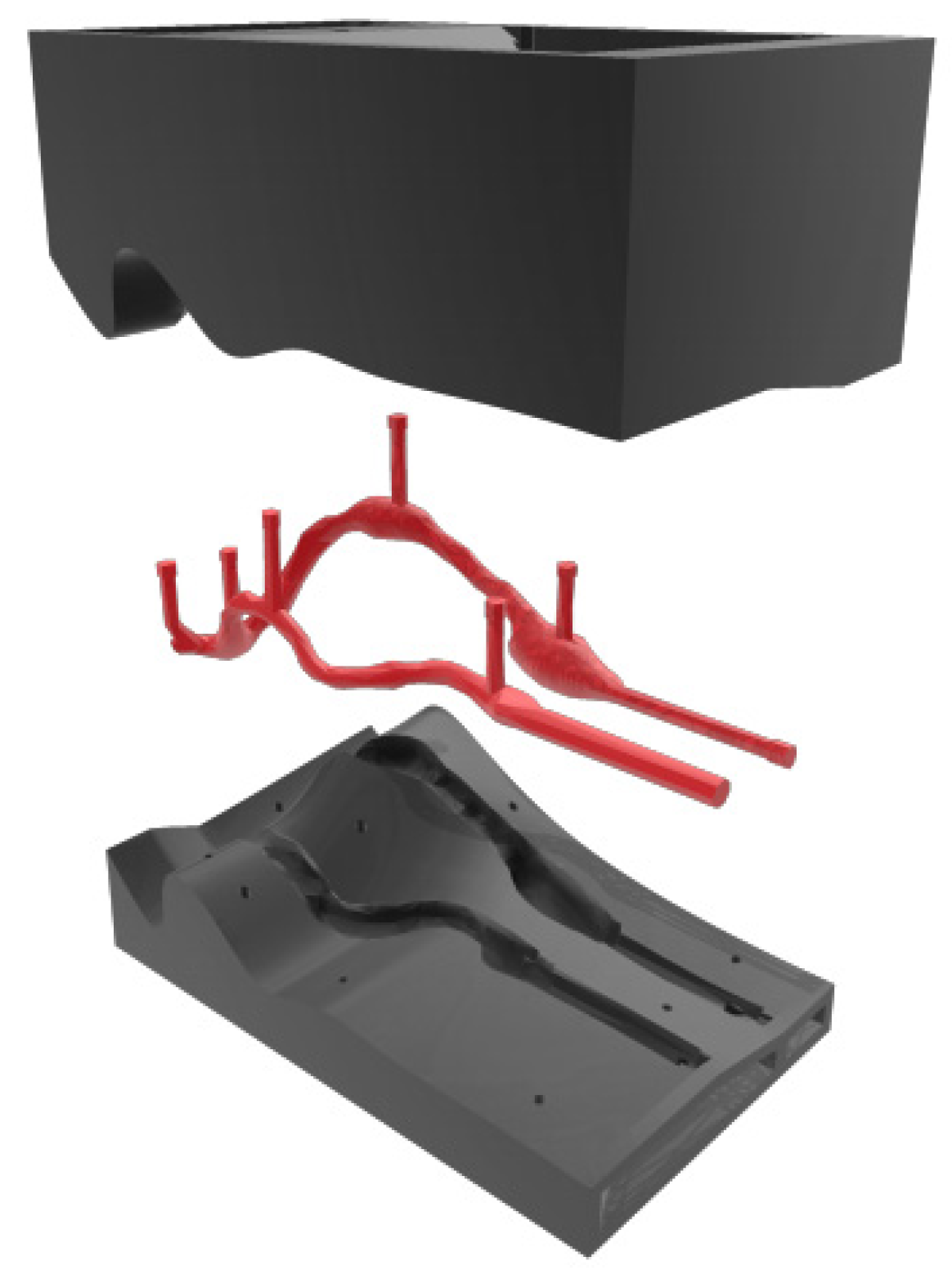
2.2. AVF Manufacturing
2.2.1. Flexible AVF
2.2.2. Rigid AVF
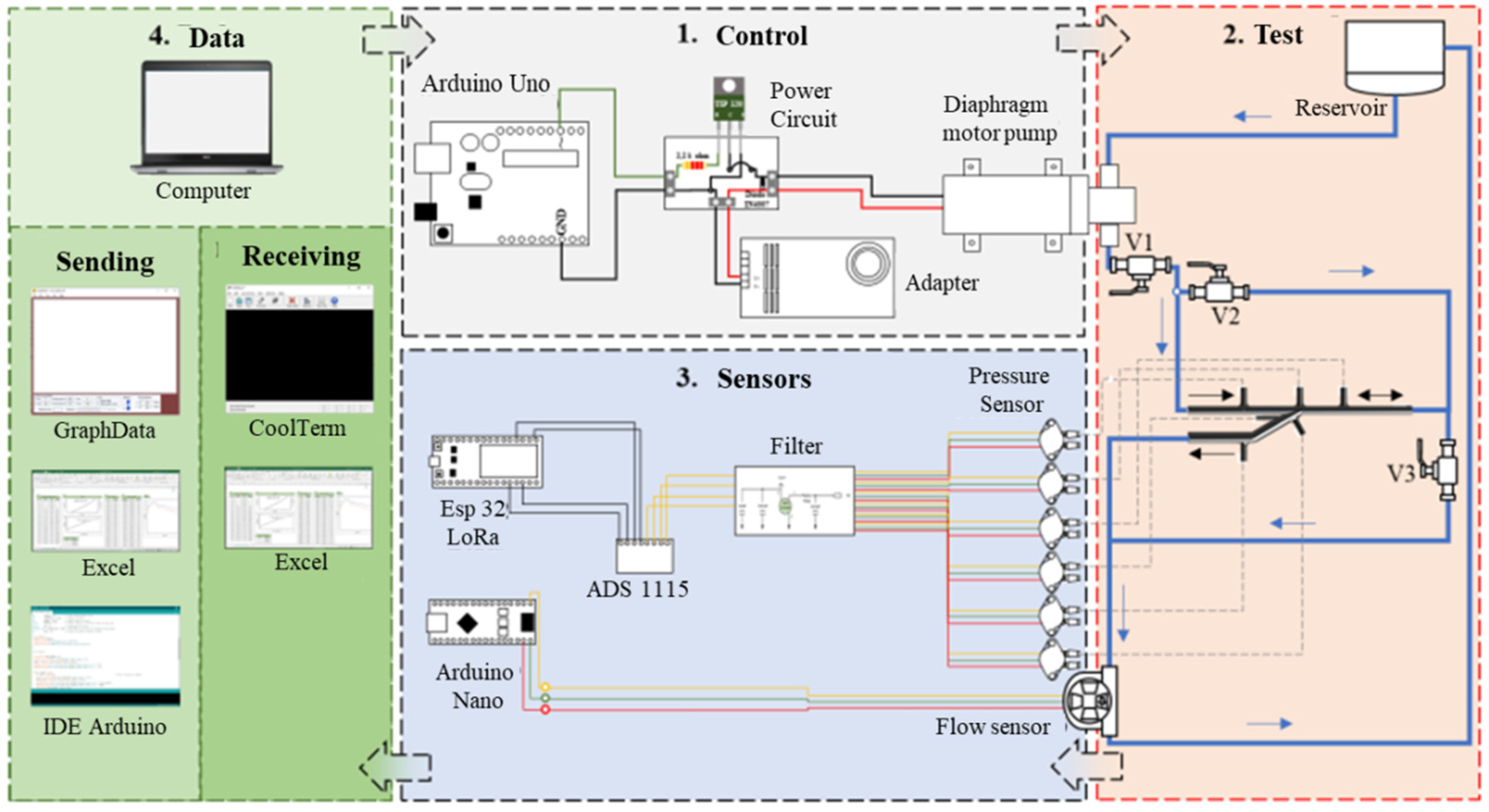
2.3. Experimental Analysis
2.4. Analysis Equations
3. Results
3.1. AVF Manufacturing—Results
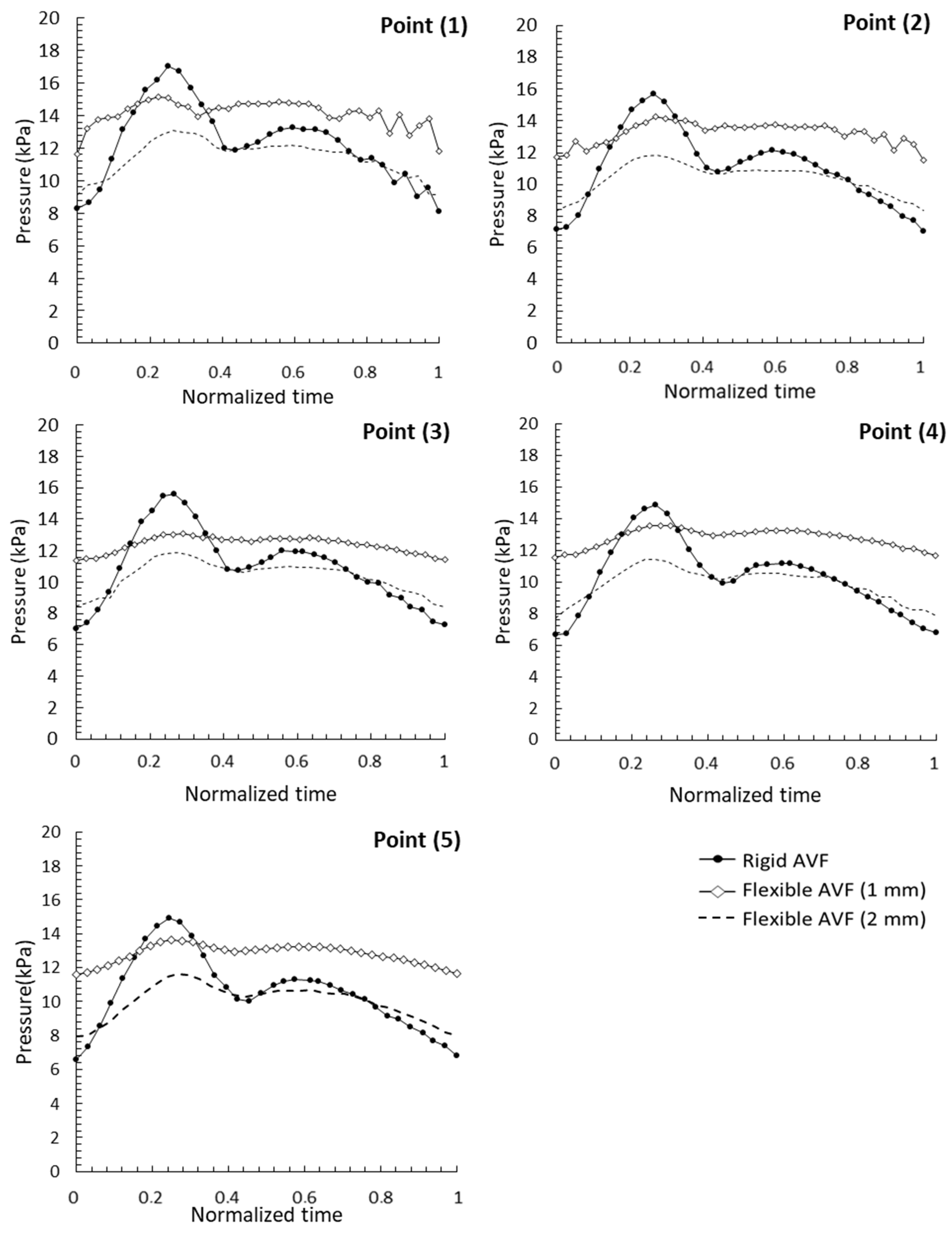
3.2. Pressure Analysis—Pulsatile Flow
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Villiers, A.M.; McBride, A.T.; Reddy, B.D.; Franz, T.; Spottiswoode, B.S. A validated patient-specific FSI model for vascular access in haemodialysis. Biomech. Model Mechanobiol. 2018, 17, 479–497. [Google Scholar] [CrossRef] [Green Version]
- Chandra, A.; Mix, D.; Varble, N. Hemodynamic study of arteriovenous fistulas for hemodialysis access. Vascular 2013, 21, 54–62. [Google Scholar] [CrossRef]
- Hu, H.; Patel, S.; Hanisch, J.J.; Santana, J.M.; Hashimoto, T.; Bai, H.; Kudze, T.; Foster, T.R.; Guo, J.; Yatsula, B.; et al. Future research directions to improve fistula maturation and reduce access failure. Semin. Vasc. 2016, 29, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Javadzadegan, A.; Lwin, N.M.; Wahab, M.A.A.; Simmons, A.; Barber, T. Analysis of Blood Flow Characteristics in a Model of a Mature Side-to-Side Arteriovenous Fistula. Artif. Organs 2017, 41, e251–e262. [Google Scholar] [CrossRef]
- Types of Arteriovenous Fistulas. Available online: https://www.ncbi.nlm.nih.gov/books/NBK493195/ (accessed on 19 July 2022).
- Rai, V.; Agrawal, D.K. Transcriptomic Analysis Identifies Differentially Expressed Genes Associated with Vascular Cuffing and Chronic Inflammation Mediating Early Thrombosis in Arteriovenous Fistula. Biomedicines 2022, 10, 433. [Google Scholar] [CrossRef]
- Malík, J. When Is Arteriovenous Fistula Dangerous for Hemodialysis Patients? Kidney Dial. 2022, 2, 82–84. [Google Scholar] [CrossRef]
- Manov, J.J.; Mohan, P.P.; Vazquez-Padron, R. Arteriovenous fistulas for hemodialysis: Brief review and current problems. J. Vasc. Access. 2022, 23, 839–846. [Google Scholar] [CrossRef]
- Alam, N.; Newport, D. Influence of Wall Compliance on the Flow Patterns in a Patient-Specific Brachio-Cephalic Arterio-Venous Fistula. Biomechanics 2022, 2, 158–173. [Google Scholar] [CrossRef]
- Browne, L.D.; Griffin, P.; Bashar, K.; Walsh, S.R.; Kavanagh, E.G.; Walsh, M.T. In Vivo Validation of the In Silico Predicted Pressure Drop Across an Arteriovenous Fistula. Ann. Biomed. Eng. 2015, 43, 1275–1286. [Google Scholar] [CrossRef]
- McGah, P.M.; Leotta, D.F.; Beach, K.W.; Riley, J.J.; Aliseda, A. Longitudinal Study of Remodeling in a Revised Peripheral Artery Bypass Graft Using 3D Ultrasound Imaging and Computational Hemodynamics. J. Biomech. Eng. 2011, 23, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Remuzzi, A.; Bozzetto, M. Biological and Physical Factors Involved in the Maturation of Arteriovenous Fistula for Hemodialysis. Cardio. Eng. Tech. 2017, 8, 273–279. [Google Scholar] [CrossRef]
- Botti, L.; Van Canneyt, K.; Kaminsky, R.; Claessens, T.; Planken, R.N.; Verdonck, P.; Remuzzi, A.; Antiga, L. Numerical Evaluation and Experimental Validation of Pressure Drops Across a Patient-Specific Model of Vascular Access for Hemodialysis. Cardio. Eng. Tech. 2013, 4, 485–499. [Google Scholar] [CrossRef]
- Dixon, B.S. Why don’t fistulas mature? Kidney Int. 2006, 8, 1413–1422. [Google Scholar] [CrossRef] [Green Version]
- Shiu, Y.T.; He, Y.; Tey, J.C.S.; Knysheva, M.; Anderson, B.; Kauser, K. Natural Vascular Scaffolding Treatment Promotes Outward Remodeling During Arteriovenous Fistula Development in Rats. Front. Bioeng. Biotechnol. 2021, 9, 622617. [Google Scholar] [CrossRef]
- Nath, K.A.; Kanakiriya, S.K.; Grande, J.P.; Anthony, J.C.; Zvonimir, S.K. Increased venous proinflammatory gene expression and intimal hyperplasia in an aorto-caval fistula model in the rat. Am. J. Pathol. 2003, 162, 2079–2090. [Google Scholar] [CrossRef] [Green Version]
- Hosseini, V.; Mallone, A.; Nasrollahi, F.; Ostrovidov, S.; Nasiri, R.; Mahmoodi, M.; Haghniaz, R.; Baidya, A.; Salek, M.M.; Darabi, M.A.; et al. Healthy and diseased in vitro models of vascular systems. Lab. Chip. 2021, 21, 641–659. [Google Scholar] [CrossRef]
- Santos, W.B.A. Análise do Escoamento Pulsátil em Fístula Arteriovenosa com Variação do Ângulo de Anastomose In Vitro e In Silico. Master’s Thesis, Federal University of Rio Grande do Norte, Natal, Brazil, 2021. [Google Scholar]
- He, Y.; Terry, C.M.; Nguyen, C.; Berceli, S.A.; Shiu, Y.T.E.; Cheung, A.K. Serial analysis of lumen geometry and hemodynamics in human arteriovenous fistula for hemodialysis using magnetic resonance imaging and computational fluid dynamics. J. Biomech. 2013, 46, 165–169. [Google Scholar] [CrossRef] [Green Version]
- Rajabi-Jagahrgh, E.; Krishnamoorthy, M.K.; RoyChaudhury, P.; Succop, P.; Wang, Y.; Choe, A.; Banerjee, R.K. Longitudinal assessment of hemodynamic endpoints in predicting arteriovenous fistula maturation. Semin. Dial. 2012, 26, 208–215. [Google Scholar] [CrossRef]
- Rajabi-Jagahrgh, E.; Krishnamoorthy, M.K.; Wang, Y.; Choe, A.; Roy-Chaudhury, P.; Banerjee, R.K. Influence of temporal variation in wall shear stress on intima-media thickening in arteriovenous fistulae. Semin. Dial. 2013, 26, 511–519. [Google Scholar] [CrossRef]
- Cunnane, C.V.; Cunnane, E.M.; Walsh, M.T. A Review of the Hemodynamic Factors Believed to Contribute to Vascular Access Dysfunction. Cardio. Eng. Tech. 2017, 8, 280–294. [Google Scholar] [CrossRef]
- Rangel, J.F.; Santos, W.B.A.; Pinheiro, L.H.; Costa, T.H.C.; Bessa, K.L.; Ortiz, J.P. Comparison of Pulsatile Pressure Flow through a Specific Patient’s Rigid and Deformable Arteriovenous Fistula: In Vitro Study. J. Appl. Fluid Mech. 2021, 14, 1593–1601. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
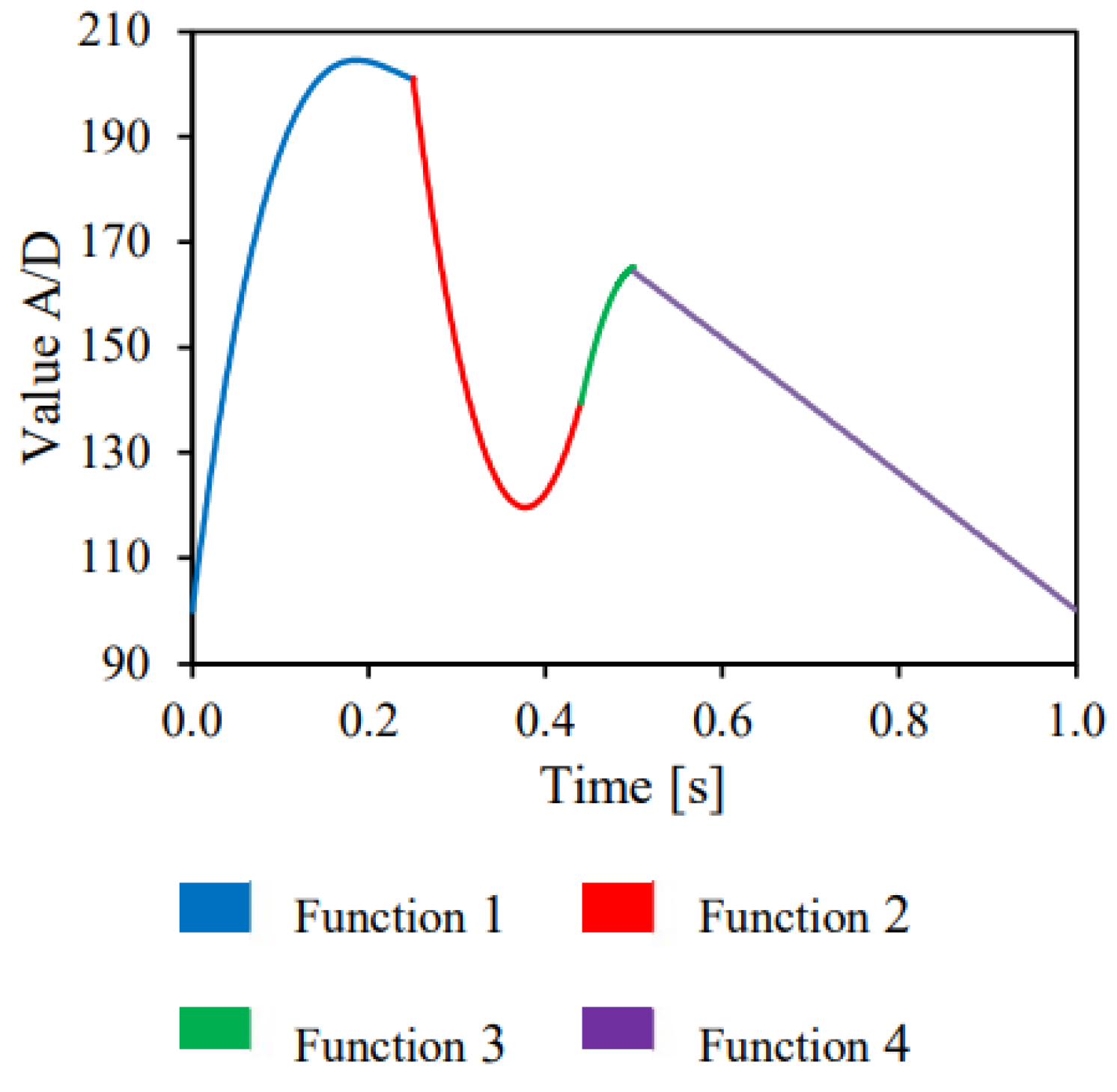
| Function 1 | y = 11.138x4 + 1607.1)x3 − 4774.4x2 + 1322.5x + 100 |
| Function 2 | y = 5060.4x2 − 3814.3x + 838.37 |
| Function 3 | y = −5833.3x2 + 5915x − 1333.9 |
| Function 4 | y = −4.1436x2 − 122.24x + 226.49 |
| Peak Pressure (kPa) | ||||||
|---|---|---|---|---|---|---|
| Point (1) | Point (2) | Point (3) | Point (4) | Point (5) | Exit | |
| AVF rigid | 17.02 | 15.72 | 15.59 | 14.87 | 14.90 | 7.17 |
| AVF flexible (1 mm) | 15.16 | 14.25 | 13.03 | 13.56 | 13.64 | 8.32 |
| AVF flexible (2 mm) | 13.11 | 11.87 | 11.88 | 11.42 | 11.63 | 5.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rangel, J.F.; de Almeida Santos, W.B.; de Carvalho Costa, T.H.; de Bessa, K.L.; Melo, J.D.D. Pressure Analysis in Rigid and Flexible Real Arteriovenous Fistula with Thickness Variation In Vitro. J. Funct. Biomater. 2023, 14, 310. https://doi.org/10.3390/jfb14060310
Rangel JF, de Almeida Santos WB, de Carvalho Costa TH, de Bessa KL, Melo JDD. Pressure Analysis in Rigid and Flexible Real Arteriovenous Fistula with Thickness Variation In Vitro. Journal of Functional Biomaterials. 2023; 14(6):310. https://doi.org/10.3390/jfb14060310
Chicago/Turabian StyleRangel, Jonhattan Ferreira, Willyam Brito de Almeida Santos, Thércio Henrique de Carvalho Costa, Kleiber Lima de Bessa, and José Daniel Diniz Melo. 2023. "Pressure Analysis in Rigid and Flexible Real Arteriovenous Fistula with Thickness Variation In Vitro" Journal of Functional Biomaterials 14, no. 6: 310. https://doi.org/10.3390/jfb14060310