

Employing Indirect Adenosine 2A Receptors (A2AR) to Enhance Osseointegration of Titanium Devices: A Pre-Clinical Study
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
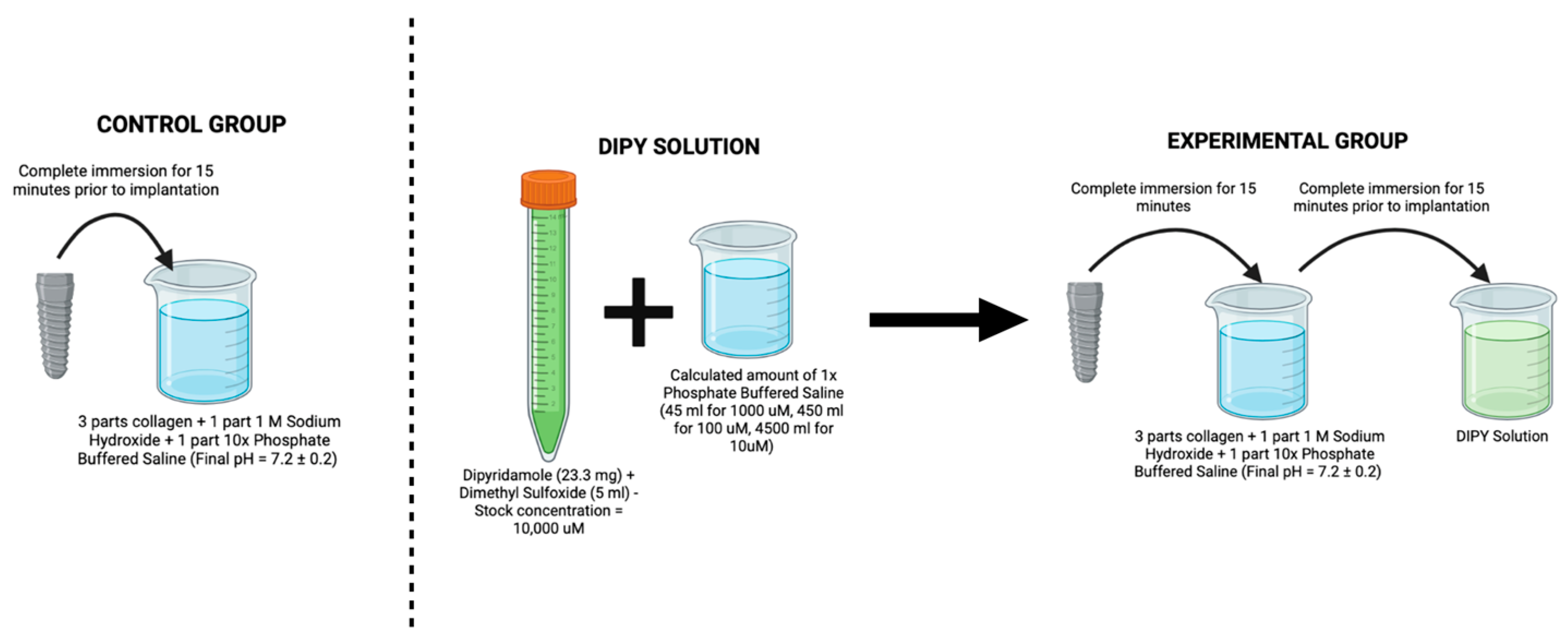
2.1. Surgical Model and Procedure
2.2. Sample Preparation and Histomorphometric Analysis
2.3. Statistical Analysis
3. Results
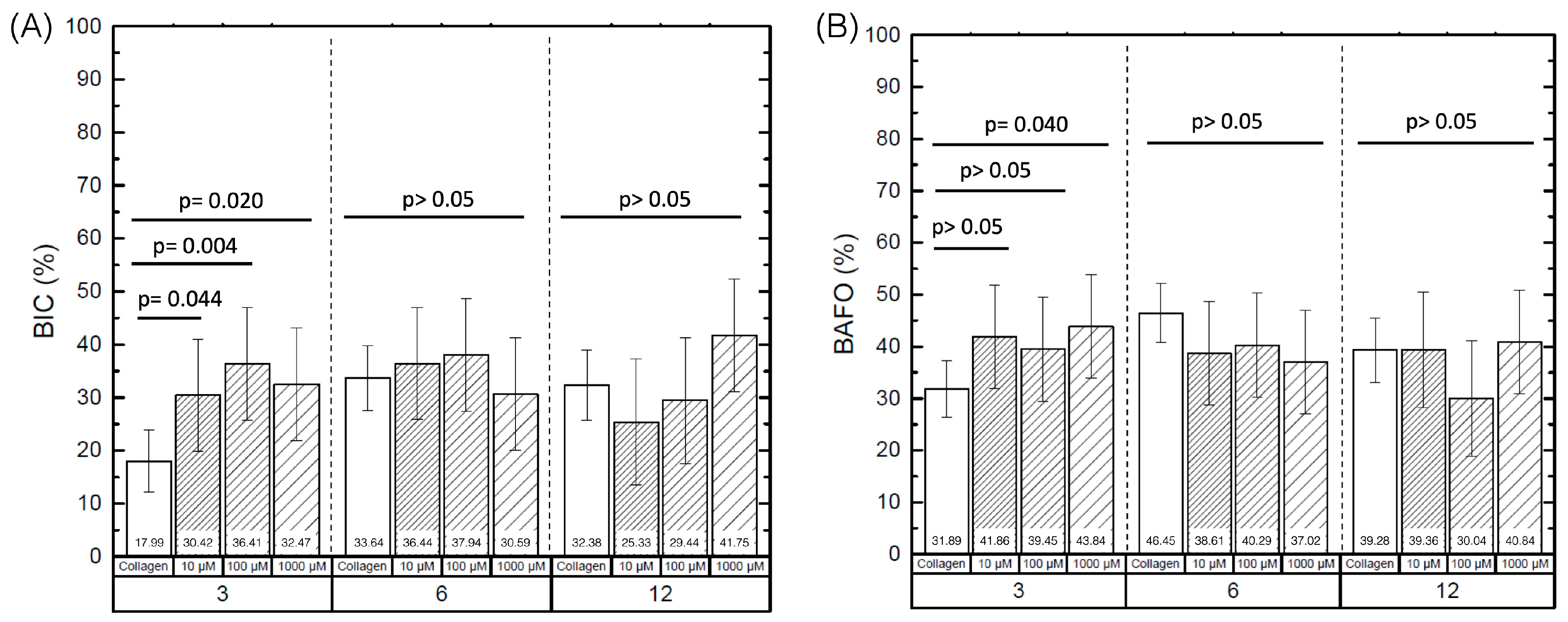
3.1. Histomorphometric Analysis
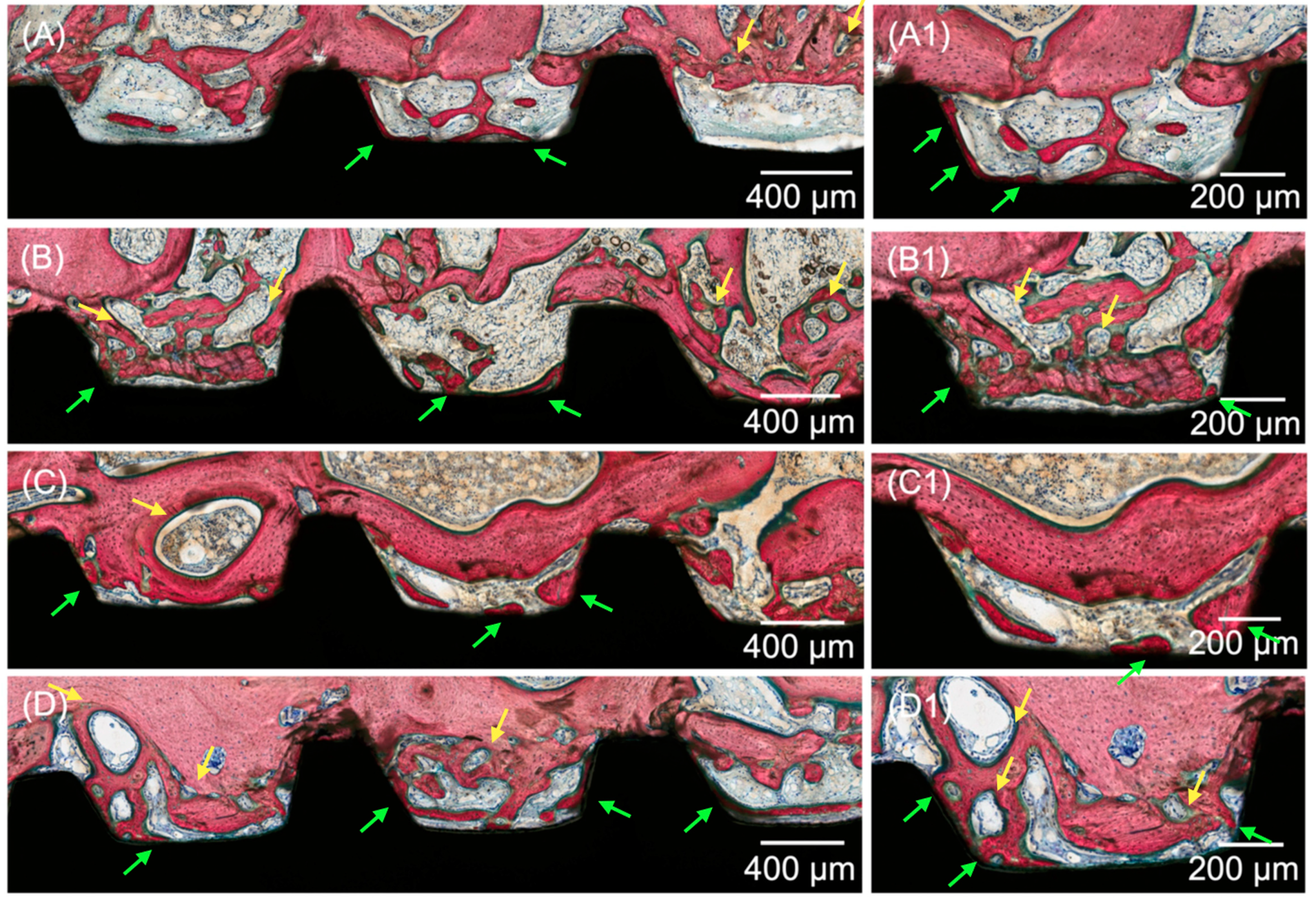
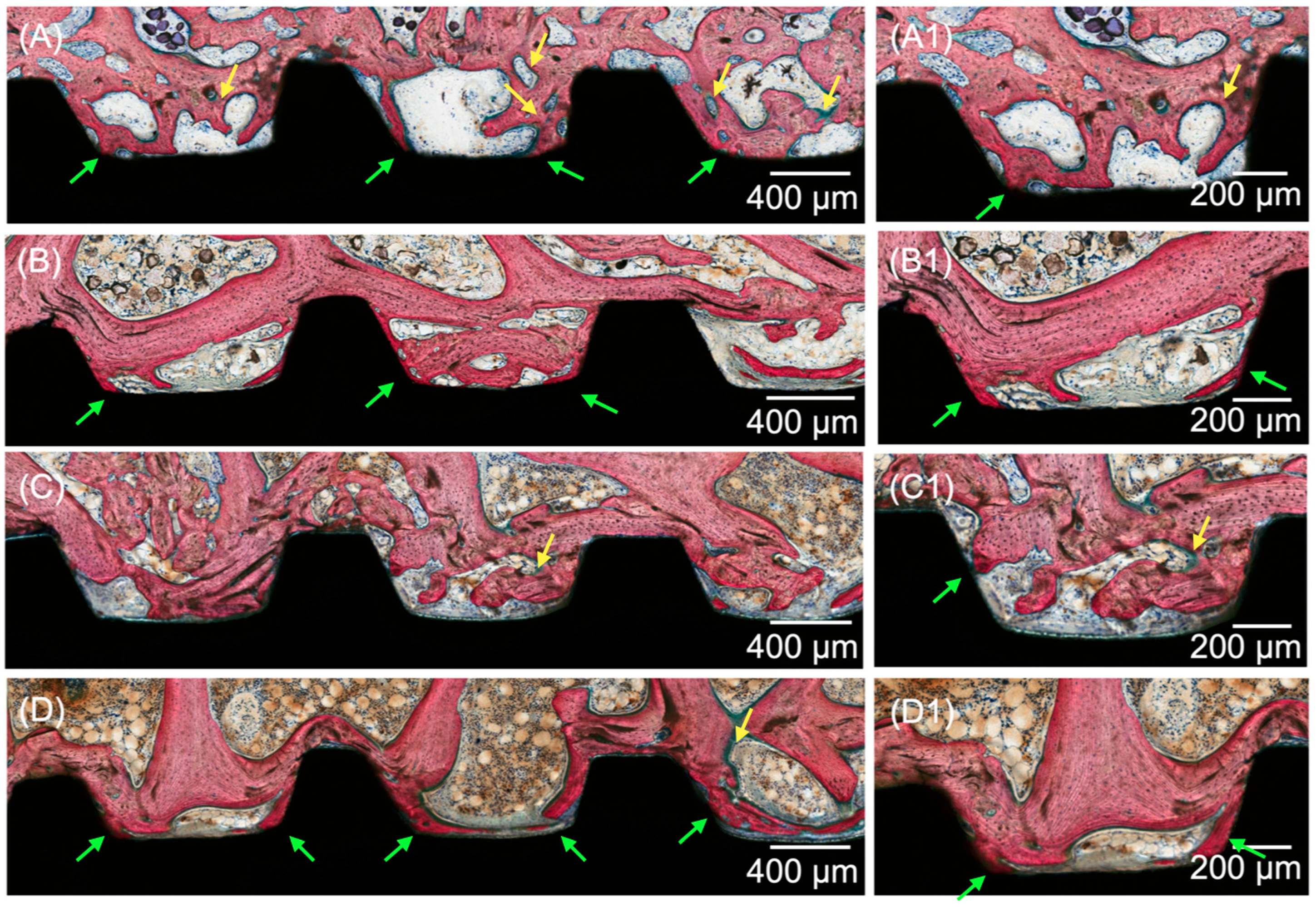
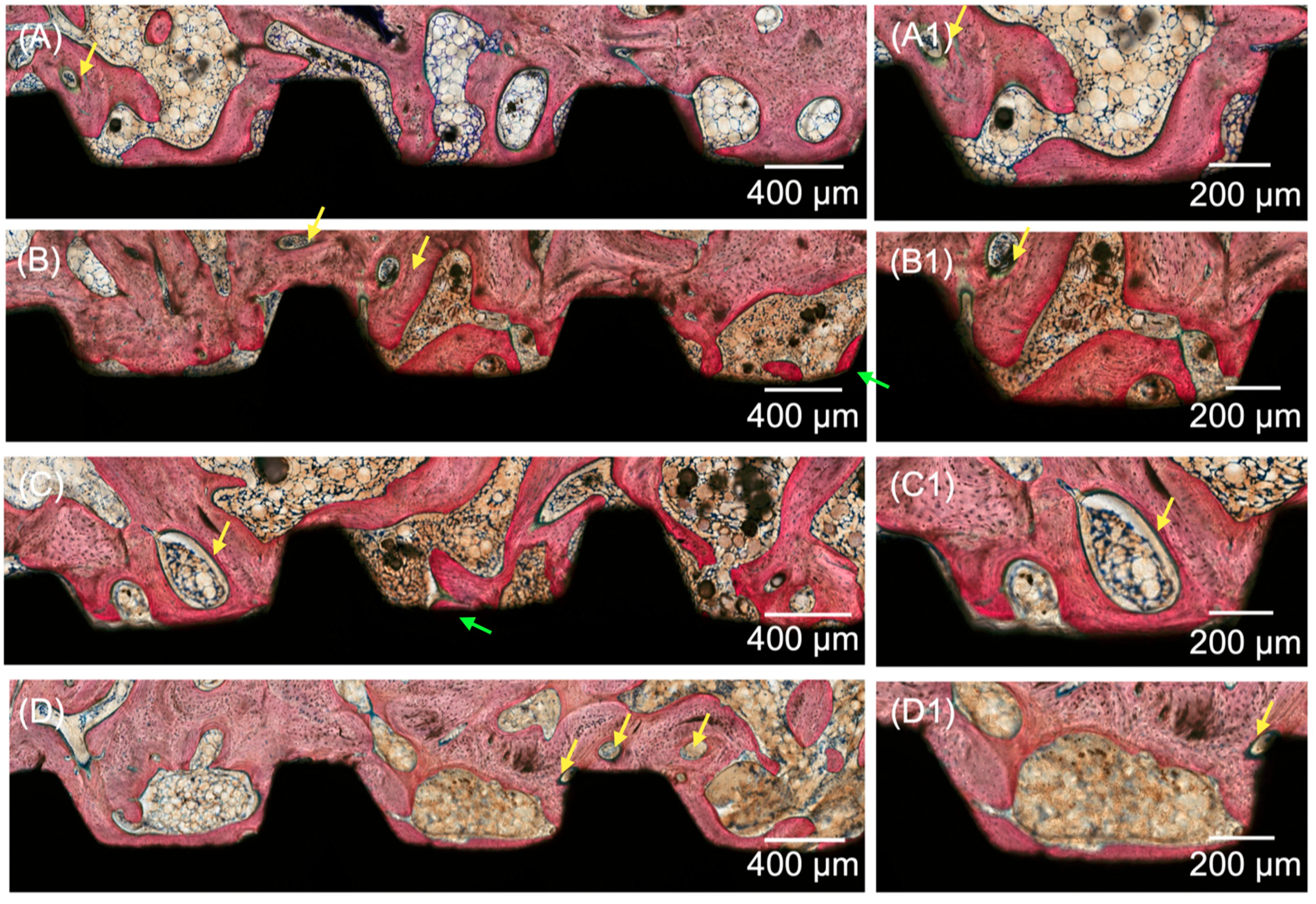
3.2. Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, X.; Chen, S.; Ji, W.; Shi, B. The risk factors of early implant failure: A retrospective study of 6113 implants. Clin. Implant. Dent. Relat. Res. 2021, 23, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Staedt, H.; Rossa, M.; Lehmann, K.M.; Al-Nawas, B.; Kammerer, P.W.; Heimes, D. Potential risk factors for early and late dental implant failure: A retrospective clinical study on 9080 implants. Int. J. Implant. Dent. 2020, 6, 81. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Bone Quality and Quantity and Dental Implant Failure: A Systematic Review and Meta-analysis. Int. J. Prosthodont. 2017, 30, 219–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goiato, M.C.; dos Santos, D.M.; Santiago, J.F., Jr.; Moreno, A.; Pellizzer, E.P. Longevity of dental implants in type IV bone: A systematic review. Int. J. Oral. Maxillofac. Surg. 2014, 43, 1108–1116. [Google Scholar] [CrossRef]
- Marquezan, M.; Osorio, A.; Sant’Anna, E.; Souza, M.M.; Maia, L. Does bone mineral density influence the primary stability of dental implants? A systematic review. Clin. Oral. Implant. Res. 2012, 23, 767–774. [Google Scholar] [CrossRef]
- Trisi, P.; De Benedittis, S.; Perfetti, G.; Berardi, D. Primary stability, insertion torque and bone density of cylindric implant ad modum Branemark: Is there a relationship? An in vitro study. Clin. Oral. Implant. Res. 2011, 22, 567–570. [Google Scholar] [CrossRef]
- Sartoretto, S.C.; Calasans-Maia, J.; Resende, R.; Camara, E.; Ghiraldini, B.; Barbosa Bezerra, F.J.; Granjeiro, J.M.; Calasans-Maia, M.D. The Influence of Nanostructured Hydroxyapatite Surface in the Early Stages of Osseointegration: A Multiparameter Animal Study in Low-Density Bone. Int. J. Nanomed. 2020, 15, 8803–8817. [Google Scholar] [CrossRef]
- Branemark, P.I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol. 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Bonfante, E.A.; Jimbo, R.; Witek, L.; Tovar, N.; Neiva, R.; Torroni, A.; Coelho, P.G. Biomaterial and biomechanical considerations to prevent risks in implant therapy. Periodontol. 2000 2019, 81, 139–151. [Google Scholar] [CrossRef]
- Berglundh, T.; Abrahamsson, I.; Lang, N.P.; Lindhe, J. De novo alveolar bone formation adjacent to endosseous implants. Clin. Oral. Implant. Res. 2003, 14, 251–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, P.G.; Suzuki, M.; Guimaraes, M.V.; Marin, C.; Granato, R.; Gil, J.N.; Miller, R.J. Early bone healing around different implant bulk designs and surgical techniques: A study in dogs. Clin. Implant. Dent. Relat. Res. 2010, 12, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Beutel, B.G.; Danna, N.R.; Granato, R.; Bonfante, E.A.; Marin, C.; Tovar, N.; Suzuki, M.; Coelho, P.G. Implant design and its effects on osseointegration over time within cortical and trabecular bone. J. Biomed. Mater. Res. B Appl. Biomater. 2016, 104, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Marin, C.; Teixeira, H.S.; Campos, F.E.; Gomes, J.B.; Guastaldi, F.; Anchieta, R.B.; Silveira, L.; Bonfante, E.A. Biomechanical evaluation of undersized drilling on implant biomechanical stability at early implantation times. J. Oral. Maxillofac. Surg. 2013, 71, e69–e75. [Google Scholar] [CrossRef] [PubMed]
- Giro, G.; Marin, C.; Granato, R.; Bonfante, E.A.; Suzuki, M.; Janal, M.N.; Coelho, P.G. Effect of drilling technique on the early integration of plateau root form endosteal implants: An experimental study in dogs. J. Oral. Maxillofac. Surg. 2011, 69, 2158–2163. [Google Scholar] [CrossRef]
- Lopez-Valverde, N.; Flores-Fraile, J.; Ramirez, J.M.; Sousa, B.M.; Herrero-Hernandez, S.; Lopez-Valverde, A. Bioactive Surfaces vs. Conventional Surfaces in Titanium Dental Implants: A Comparative Systematic Review. J. Clin. Med. 2020, 9, 2047. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Granato, R.; Marin, C.; Teixeira, H.S.; Suzuki, M.; Valverde, G.B.; Janal, M.N.; Lilin, T.; Bonfante, E.A. The effect of different implant macrogeometries and surface treatment in early biomechanical fixation: An experimental study in dogs. J. Mech. Behav. Biomed. Mater. 2011, 4, 1974–1981. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R. Osseointegration of metallic devices: Current trends based on implant hardware design. Arch. Biochem. Biophys. 2014, 561, 99–108. [Google Scholar] [CrossRef]
- Coelho, P.G.; Jimbo, R.; Tovar, N.; Bonfante, E.A. Osseointegration: Hierarchical designing encompassing the macrometer, micrometer, and nanometer length scales. Dent. Mater. 2015, 31, 37–52. [Google Scholar] [CrossRef]
- Ausiello, P.; Franciosa, P.; Martorelli, M.; Watts, D.C. Effects of thread features in osseo-integrated titanium implants using a statistics-based finite element method. Dent. Mater. 2012, 28, 919–927. [Google Scholar] [CrossRef]
- Benalcázar-Jalkh, E.B.; Nayak, V.V.; Gory, C.; Marquez-Guzman, A.; Bergamo, E.T.; Tovar, N.; Coelho, P.G.; Bonfante, E.A.; Witek, L. Impact of implant thread design on insertion torque and osseointegration: A preclinical model. Med. Oral Patol. Oral Y Cirugía Bucal. Ed. Ingl. 2023, 28, 7. [Google Scholar] [CrossRef] [PubMed]
- Abuhussein, H.; Pagni, G.; Rebaudi, A.; Wang, H.L. The effect of thread pattern upon implant osseointegration. Clin. Oral. Implant. Res. 2010, 21, 129–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.H.; Lim, Y.J.; Kim, M.J.; Kwon, H.B. The effect of various thread designs on the initial stability of taper implants. J. Adv. Prosthodont. 2009, 1, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Jimbo, R.; Giro, G.; Marin, C.; Granato, R.; Suzuki, M.; Tovar, N.; Lilin, T.; Janal, M.; Coelho, P.G. Simplified drilling technique does not decrease dental implant osseointegration: A preliminary report. J. Periodontol. 2013, 84, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Sarendranath, A.; Khan, R.; Tovar, N.; Marin, C.; Yoo, D.; Redisch, J.; Jimbo, R.; Coelho, P.G. Effect of low speed drilling on osseointegration using simplified drilling procedures. Br. J. Oral. Maxillofac. Surg. 2015, 53, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruiz, R.; Gold, J.; Somohano Marquez, T.; Romanos, G. Under-Drilling versus Hybrid Osseodensification Technique: Differences in Implant Primary Stability and Bone Density of the Implant Bed Walls. Materials 2020, 13, 390. [Google Scholar] [CrossRef] [Green Version]
- Lahens, B.; Neiva, R.; Tovar, N.; Alifarag, A.; Jimbo, R.; Bonfante, E.; Bowers, M.; Cuppini, M.; Freitas, H.; Witek, L.; et al. Biomechanical and Histologic Basis of Osseodensification Drilling For Endosteal Implant Placement in Low Density Bone. An Experimental Study in Sheep. J. Mech. Behav. Biomed. Mater. 2016, 63, 56–65. [Google Scholar] [CrossRef]
- Alhussaini, A.H.A. Effect of Platelet-Rich Fibrin and Bone Morphogenetic Protein on Dental Implant Stability. J. Craniofac. Surg. 2019, 30, 1492–1496. [Google Scholar] [CrossRef]
- Haimov, H.; Yosupov, N.; Pinchasov, G.; Juodzbalys, G. Bone Morphogenetic Protein Coating on Titanium Implant Surface: A Systematic Review. J. Oral. Maxillofac. Res. 2017, 8, e1. [Google Scholar] [CrossRef]
- Eawsakul, K.; Tancharoen, S.; Nasongkla, N. Combination of dip coating of BMP-2 and spray coating of PLGA on dental implants for osseointegration. J. Drug. Deliv. Sci. Technol. 2021, 61, 102296. [Google Scholar] [CrossRef]
- Guimaraes, M.B.; Bueno, R.S.; Blaya, M.B.; Shinkai, R.S.; Marques, L.M. Influence of the local application of sodium alendronate gel on osseointegration of titanium implants. Int. J. Oral. Maxillofac. Surg. 2015, 44, 1423–1429. [Google Scholar] [CrossRef] [PubMed]
- Alenezi, A.; Chrcanovic, B.; Wennerberg, A. Effects of Local Drug and Chemical Compound Delivery on Bone Regeneration Around Dental Implants in Animal Models: A Systematic Review and Meta-Analysis. Int. J. Oral. Maxillofac. Implant. 2018, 33, e1–e18. [Google Scholar] [CrossRef] [Green Version]
- Marin, C.; Jimbo, R.; Lorenzoni, F.C.; Witek, L.; Teixeira, H.; Bonfante, E.; Gil, J.; Granato, R.; Tovar, N.; Coelho, P.G. Bone-Forming Capabilities of a Newly Developed NanoHA Composite Alloplast Infused with Collagen: A Pilot Study in the Sheep Mandible. Int. J. Dent. 2013, 2013, 296391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osagie-Clouard, L.; Sanghani, A.; Coathup, M.; Briggs, T.; Bostrom, M.; Blunn, G. Parathyroid hormone 1–34 and skeletal anabolic action: The use of parathyroid hormone in bone formation. Bone Jt. Res. 2017, 6, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, D.; Tovar, N.; Jimbo, R.; Marin, C.; Anchieta, R.B.; Machado, L.S.; Montclare, J.; Guastaldi, F.P.; Janal, M.N.; Coelho, P.G. Increased osseointegration effect of bone morphogenetic protein 2 on dental implants: An in vivo study. J. Biomed. Mater. Res. A 2014, 102, 1921–1927. [Google Scholar] [CrossRef] [PubMed]
- Mediero, A.; Wilder, T.; Perez-Aso, M.; Cronstein, B.N. Direct or indirect stimulation of adenosine A2A receptors enhances bone regeneration as well as bone morphogenetic protein-2. FASEB J. 2015, 29, 1577–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albright, K.C.; Howard, V.J.; Howard, G. Selecting an Optimal Antiplatelet Agent for Secondary Stroke Prevention. Neurol. Clin. Pract. 2021, 11, e121–e128. [Google Scholar] [CrossRef]
- Harker, L.A.; Kadatz, R.A. Mechanism of action of dipyridamole. Thromb. Res. 1983, 29, 39–46. [Google Scholar] [CrossRef]
- Wang, M.M.; Flores, R.L.; Witek, L.; Torroni, A.; Ibrahim, A.; Wang, Z.; Liss, H.A.; Cronstein, B.N.; Lopez, C.D.; Maliha, S.G.; et al. Dipyridamole-loaded 3D-printed bioceramic scaffolds stimulate pediatric bone regeneration in vivo without disruption of craniofacial growth through facial maturity. Sci. Rep. 2019, 9, 18439. [Google Scholar] [CrossRef] [Green Version]
- Mediero, A.; Wilder, T.; Reddy, V.S.; Cheng, Q.; Tovar, N.; Coelho, P.G.; Witek, L.; Whatling, C.; Cronstein, B.N. Ticagrelor regulates osteoblast and osteoclast function and promotes bone formation in vivo via an adenosine-dependent mechanism. FASEB J. 2016, 30, 3887–3900. [Google Scholar] [CrossRef]
- Bekisz, J.M.; Flores, R.L.; Witek, L.; Lopez, C.D.; Runyan, C.M.; Torroni, A.; Cronstein, B.N.; Coelho, P.G. Dipyridamole enhances osteogenesis of three-dimensionally printed bioactive ceramic scaffolds in calvarial defects. J. Cranio-Maxillofac. Surg. 2018, 46, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Witek, L.; Alifarag, A.M.; Tovar, N.; Lopez, C.D.; Cronstein, B.N.; Rodriguez, E.D.; Coelho, P.G. Repair of Critical-Sized Long Bone Defects Using Dipyridamole-Augmented 3D-Printed Bioactive Ceramic Scaffolds. J. Orthop. Res. 2019, 37, 2499–2507. [Google Scholar] [CrossRef] [PubMed]
- Lopez, C.D.; Coelho, P.G.; Witek, L.; Torroni, A.; Greenberg, M.I.; Cuadrado, D.L.; Guarino, A.M.; Bekisz, J.M.; Cronstein, B.N.; Flores, R.L. Regeneration of a Pediatric Alveolar Cleft Model Using Three-Dimensionally Printed Bioceramic Scaffolds and Osteogenic Agents: Comparison of Dipyridamole and rhBMP-2. Plast. Reconstr. Surg. 2019, 144, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Maliha, S.G.; Lopez, C.D.; Coelho, P.G.; Witek, L.; Cox, M.; Meskin, A.; Rusi, S.; Torroni, A.; Cronstein, B.N.; Flores, R.L. Bone Tissue Engineering in the Growing Calvaria Using Dipyridamole-Coated, Three-Dimensionally-Printed Bioceramic Scaffolds: Construct Optimization and Effects on Cranial Suture Patency. Plast. Reconstr. Surg. 2020, 145, 337e–347e. [Google Scholar] [CrossRef]
- Lopez, C.D.; Diaz-Siso, J.R.; Witek, L.; Bekisz, J.M.; Gil, L.F.; Cronstein, B.N.; Flores, R.L.; Torroni, A.; Rodriguez, E.D.; Coelho, P.G. Dipyridamole Augments Three-Dimensionally Printed Bioactive Ceramic Scaffolds to Regenerate Craniofacial Bone. Plast. Reconstr. Surg. 2019, 143, 1408–1419. [Google Scholar] [CrossRef]
- Grossi, J.R.A.; Deliberador, T.M.; Giovanini, A.F.; Zielak, J.C.; Sebastiani, A.; Gonzaga, C.C.; Coelho, P.G.; Zetola, A.L.; Weiss, F.P.; Benalcazar Jalkh, E.B.; et al. Effects of local single dose administration of parathormone on the early stages of osseointegration: A pre-clinical study. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 1806–1813. [Google Scholar] [CrossRef]
- Grossi, J.R.; Parra, M.; Benalcazar-Jalkh, E.B.; Giovanini, A.F.; Zielak, J.C.; Sebstiani, A.M.; Gonzaga, C.C.; Coelho, P.G.; Witek, L.; Deliberador, T.M. Effects of a local single dose administration of growth hormone on the osseointegration of titanium implants. Med. Oral. Patol. Oral. Cir. Bucal. 2022, 27, e174–e180. [Google Scholar] [CrossRef]
- Ishack, S.; Mediero, A.; Wilder, T.; Ricci, J.L.; Cronstein, B.N. Bone regeneration in critical bone defects using three-dimensionally printed beta-tricalcium phosphate/hydroxyapatite scaffolds is enhanced by coating scaffolds with either dipyridamole or BMP-2. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 366–375. [Google Scholar] [CrossRef] [Green Version]
- Shen, C.; Wang, M.M.; Witek, L.; Tovar, N.; Cronstein, B.N.; Torroni, A.; Flores, R.L.; Coelho, P.G. Transforming the Degradation Rate of beta-tricalcium Phosphate Bone Replacement Using 3-Dimensional Printing. Ann. Plast. Surg. 2021, 87, e153–e162. [Google Scholar] [CrossRef]
- Taymouri, S.; Amirkhani, S.; Mirian, M. Fabrication and characterization of injectable thermosensitive hydrogel containing dipyridamole loaded polycaprolactone nanoparticles for bone tissue engineering. J. Drug. Deliv. Sci. Technol. 2021, 64, 102659. [Google Scholar] [CrossRef]
- Bergamo, E.T.P.; de Oliveira, P.; Jimbo, R.; Neiva, R.; Tovar, N.; Witek, L.; Gil, L.F.; Bonfante, E.A.; Coelho, P.G. Synergistic Effects of Implant Macrogeometry and Surface Physicochemical Modifications on Osseointegration: An In Vivo Experimental Study in Sheep. J. Long Term Eff. Med. Implant. 2019, 29, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Plecko, M.; Sievert, C.; Andermatt, D.; Frigg, R.; Kronen, P.; Klein, K.; Stubinger, S.; Nuss, K.; Burki, A.; Ferguson, S.; et al. Osseointegration and biocompatibility of different metal implants--a comparative experimental investigation in sheep. BMC Musculoskelet. Disord. 2012, 13, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubinger, S.; Biermeier, K.; Bachi, B.; Ferguson, S.J.; Sader, R.; von Rechenberg, B. Comparison of Er:YAG laser, piezoelectric, and drill osteotomy for dental implant site preparation: A biomechanical and histological analysis in sheep. Lasers Surg. Med. 2010, 42, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Stubinger, S.; Mosch, I.; Robotti, P.; Sidler, M.; Klein, K.; Ferguson, S.J.; von Rechenberg, B. Histological and biomechanical analysis of porous additive manufactured implants made by direct metal laser sintering: A pilot study in sheep. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1154–1163. [Google Scholar] [CrossRef]
- Muschler, G.F.; Raut, V.P.; Patterson, T.E.; Wenke, J.C.; Hollinger, J.O. The design and use of animal models for translational research in bone tissue engineering and regenerative medicine. Tissue Eng. Part B Rev. 2010, 16, 123–145. [Google Scholar] [CrossRef] [Green Version]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pacheco-Vergara, M.J.; Benalcázar-Jalkh, E.B.; Nayak, V.V.; Bergamo, E.T.P.; Cronstein, B.; Zétola, A.L.; Weiss, F.P.; Grossi, J.R.A.; Deliberador, T.M.; Coelho, P.G.; et al. Employing Indirect Adenosine 2A Receptors (A2AR) to Enhance Osseointegration of Titanium Devices: A Pre-Clinical Study. J. Funct. Biomater. 2023, 14, 308. https://doi.org/10.3390/jfb14060308
Pacheco-Vergara MJ, Benalcázar-Jalkh EB, Nayak VV, Bergamo ETP, Cronstein B, Zétola AL, Weiss FP, Grossi JRA, Deliberador TM, Coelho PG, et al. Employing Indirect Adenosine 2A Receptors (A2AR) to Enhance Osseointegration of Titanium Devices: A Pre-Clinical Study. Journal of Functional Biomaterials. 2023; 14(6):308. https://doi.org/10.3390/jfb14060308
Chicago/Turabian StylePacheco-Vergara, Maria Jesus, Ernesto Byron Benalcázar-Jalkh, Vasudev V. Nayak, Edmara T. P. Bergamo, Bruce Cronstein, André Luis Zétola, Fernando Pessoa Weiss, João Ricardo Almeida Grossi, Tatiana Miranda Deliberador, Paulo G. Coelho, and et al. 2023. "Employing Indirect Adenosine 2A Receptors (A2AR) to Enhance Osseointegration of Titanium Devices: A Pre-Clinical Study" Journal of Functional Biomaterials 14, no. 6: 308. https://doi.org/10.3390/jfb14060308