
Analysis of the Ability of Different Allografts to Act as Carrier Grafts for Local Drug Delivery
 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. Allografts
2.2. Graft Absorption Capacity Testing
2.3. Elution Kinetics
2.4. Fibrous Graft (Fiberfill®)
2.5. DBM and Cortical Granules
2.6. Cancellous Bone and Demineralized Cancellous Bone (Spongioflex®)
2.7. Exposure Times and Release
2.8. Gentamicin Quantification
2.9. Zone of Inhibition Test (ZOI)
2.10. Statistics
3. Results
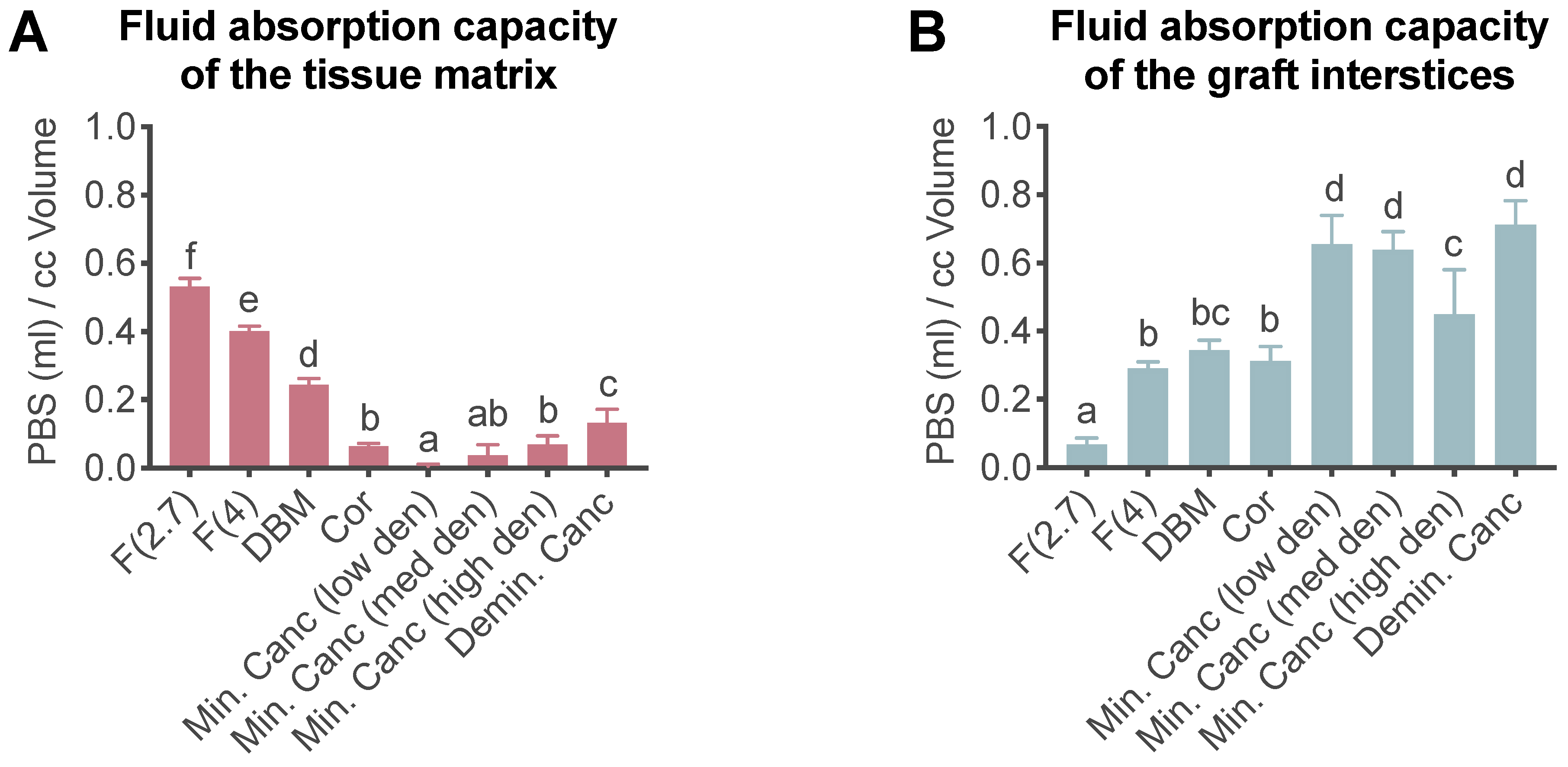
3.1. Liquid Absorption Capacity
3.2. Graft Elution and Antimicrobial Activity
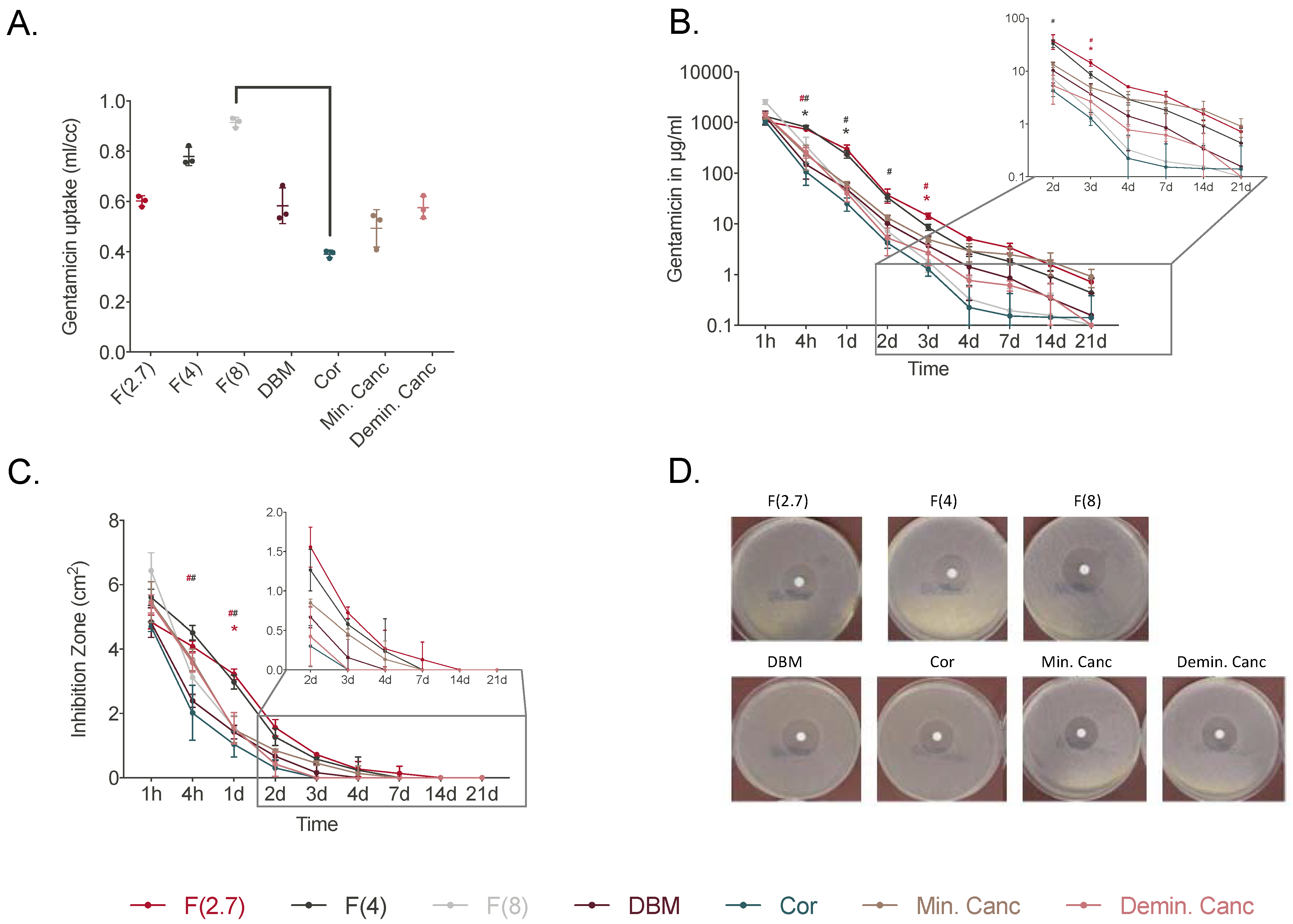
3.2.1. Rehydration Time: 30 min
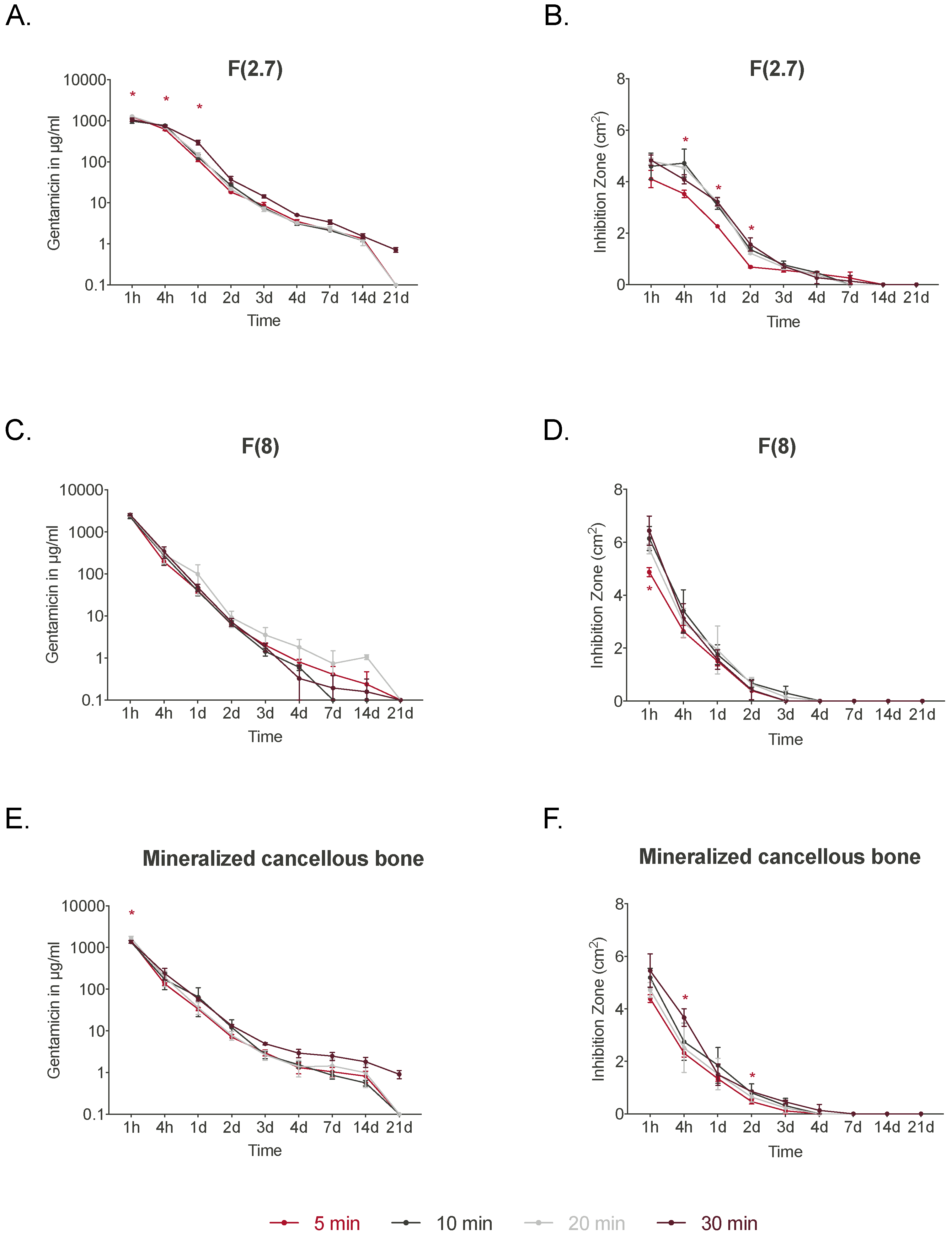
3.2.2. Varying Rehydration Times: 5 to 30 min
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moriarty, T.F.; Metsemakers, W.J.; Morgenstern, M.; Hofstee, M.I.; Vallejo Diaz, A.; Cassat, J.E.; Wildemann, B.; Depypere, M.; Schwarz, E.M.; Richards, R.G. Fracture-related infection. Nat. Rev. Dis. Prim. 2022, 8, 67. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.G.; O’Mahony, A.M.; Culligan, E.P.; O’Driscoll, C.M.; Ryan, K.B. Strategies to Mitigate and Treat Orthopaedic Device-Associated Infections. Antibiotics 2022, 11, 1822. [Google Scholar] [CrossRef] [PubMed]
- Pollard, T.C.; Newman, J.E.; Barlow, N.J.; Price, J.D.; Willett, K.M. Deep wound infection after proximal femoral fracture: Consequences and costs. J. Hosp. Infect. 2006, 63, 133–139. [Google Scholar] [CrossRef]
- Shapiro, L.M.; Graham, L.A.; Hawn, M.T.; Kamal, R.N. Quality Reporting Windows May Not Capture the Effects of Surgical Site Infections After Orthopaedic Surgery. J. Bone Jt. Surg. Am. Vol. 2022, 104, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.; Counsell, A.; Boulton, C.; Moran, C.G. Early infection after hip fracture surgery: Risk factors, costs and outcome. J. Bone Jt. Surg. Br. 2008, 90, 770–777. [Google Scholar] [CrossRef]
- Eckmann, C.; Kramer, A.; Assadian, O.; Flessa, S.; Huebner, C.; Michnacs, K.; Muehlendyck, C.; Podolski, K.M.; Wilke, M.; Heinlein, W.; et al. Clinical and economic burden of surgical site infections in inpatient care in Germany: A retrospective, cross-sectional analysis from 79 hospitals. PLoS ONE 2022, 17, e0275970. [Google Scholar] [CrossRef]
- Awad, S.S.; Palacio, C.H.; Subramanian, A.; Byers, P.A.; Abraham, P.; Lewis, D.A.; Young, E.J. Implementation of a methicillin-resistant Staphylococcus aureus (MRSA) prevention bundle results in decreased MRSA surgical site infections. Am. J. Surg. 2009, 198, 607–610. [Google Scholar] [CrossRef]
- Weigelt, J.A.; Lipsky, B.A.; Tabak, Y.P.; Derby, K.G.; Kim, M.; Gupta, V. Surgical site infections: Causative pathogens and associated outcomes. Am. J. Infect. Control 2010, 38, 112–120. [Google Scholar] [CrossRef]
- Frommelt, L. Use of antibiotics in bones: Prophylaxis and current treatment standards. Orthopade 2018, 47, 24–29. [Google Scholar] [CrossRef]
- Chan, Y.S.; Ueng, S.W.; Wang, C.J.; Lee, S.S.; Chen, C.Y.; Shin, C.H. Antibiotic-impregnated autogenic cancellous bone grafting is an effective and safe method for the management of small infected tibial defects: A comparison study. J. Trauma 2000, 48, 246–255. [Google Scholar] [CrossRef]
- Vardanian, A.J.; Chau, A.; Quinones-Baldrich, W.; Lawrence, P.F. Arterial allograft allows in-line reconstruction of prosthetic graft infection with low recurrence rate and mortality. Am. Surg. 2009, 75, 1000–1003. [Google Scholar] [CrossRef]
- Rupp, M.; Klute, L.; Baertl, S.; Walter, N.; Mannala, G.K.; Frank, L.; Pfeifer, C.; Alt, V.; Kerschbaum, M. The clinical use of bone graft substitutes in orthopedic surgery in Germany-A 10-years survey from 2008 to 2018 of 1,090,167 surgical interventions. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 110, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Balling, H.; Weckbach, A. Demineralized bone matrix versus autogenous bone graft for thoracolumbar anterior single-level interbody fusion. Acta Orthopædica Belg. 2020, 86, 2. [Google Scholar]
- Di Bella, C.; Dozza, B.; Frisoni, T.; Cevolani, L.; Donati, D. Injection of demineralized bone matrix with bone marrow concentrate improves healing in unicameral bone cyst. Clin. Orthop. Relat. Res. 2010, 468, 3047–3055. [Google Scholar] [CrossRef]
- Drosos, G.I.; Touzopoulos, P.; Ververidis, A.; Tilkeridis, K.; Kazakos, K. Use of demineralized bone matrix in the extremities. World J. Orthop. 2015, 6, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Kuhls, R.; Werner-Rustner, M.; Kuchler, I.; Soost, F. Human demineralised bone matrix as a bone substitute for reconstruction of cystic defects of the lower jaw. Cell. Tissue Bank. 2001, 2, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Winkler, H.; Kaudela, K.; Stoiber, A.; Menschik, F. Bone grafts impregnated with antibiotics as a tool for treating infected implants in orthopedic surgery—One stage revision results. Cell. Tissue Bank. 2006, 7, 319–323. [Google Scholar] [CrossRef]
- Winkler, H.; Stoiber, A.; Kaudela, K.; Winter, F.; Menschik, F. One stage uncemented revision of infected total hip replacement using cancellous allograft bone impregnated with antibiotics. J. Bone Jt. Surg. Br. 2008, 90, 1580–1584. [Google Scholar] [CrossRef]
- Coraca-Huber, D.C.; Steixner, S.J.M.; Najman, S.; Stojanovic, S.; Finze, R.; Rimashevskiy, D.; Saginova, D.; Barbeck, M.; Schnettler, R. Lyophilized Human Bone Allograft as an Antibiotic Carrier: An In Vitro and In Vivo Study. Antibiotics 2022, 11, 969. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Kelm, J. Enhancement of antibiotic elution from acrylic bone cement. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90, 467–475. [Google Scholar] [CrossRef]
- McConoughey, S.J.; Howlin, R.P.; Wiseman, J.; Stoodley, P.; Calhoun, J.H. Comparing PMMA and calcium sulfate as carriers for the local delivery of antibiotics to infected surgical sites. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 103, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Bormann, N.; Schwabe, P.; Smith, M.D.; Wildemann, B. Analysis of parameters influencing the release of antibiotics mixed with bone grafting material using a reliable mixing procedure. Bone 2014, 59, 162–172. [Google Scholar] [CrossRef]
- Ketonis, C.; Barr, S.; Shapiro, I.M.; Parvizi, J.; Adams, C.S.; Hickok, N.J. Antibacterial activity of bone allografts: Comparison of a new vancomycin-tethered allograft with allograft loaded with adsorbed vancomycin. Bone 2011, 48, 631–638. [Google Scholar] [CrossRef]
- Witsø, E.; Persen, L.; Benum, P.; Bergh, K. Cortical allograft as a vehicle for antibiotic delivery. Acta Orthop. 2005, 76, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Pruss, A.; Baumann, B.; Seibold, M.; Kao, M.; Tintelnot, K.; von Versen, R.; Radtke, H.; Dorner, T.; Pauli, G.; Gobel, U.B. Validation of the sterilization procedure of allogeneic avital bone transplants using peracetic acid-ethanol. Biologicals 2001, 29, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Diefenbeck, M.; Mückley, T.; Hofmann, G.O. Prophylaxis and treatment of implant-related infections by local application of antibiotics. Injury 2006, 37, S95–S104. [Google Scholar] [CrossRef]
- Winkler, H.; Haiden, P. Allograft Bone as Antibiotic Carrier. J. Bone Jt. Infect. 2017, 2, 52–62. [Google Scholar] [CrossRef]
- Sabbagh, F.; Kim, B.S. Microneedles for transdermal drug delivery using clay-based composites. Expert Opin. Drug. Deliv. 2022, 19, 1099–1113. [Google Scholar] [CrossRef]
- Van Vugt, T.A.G.; Arts, J.J.; Geurts, J.A.P. Antibiotic-Loaded Polymethylmethacrylate Beads and Spacers in Treatment of Orthopedic Infections and the Role of Biofilm Formation. Front. Microbiol. 2019, 10, 1626. [Google Scholar] [CrossRef]
- Buttaro, M.A.; Pusso, R.; Piccaluga, F. Vancomycin-supplemented impacted bone allografts in infected hip arthroplasty. Two-stage revision results. J. Bone Jt. Surg. Br. 2005, 87, 314–319. [Google Scholar] [CrossRef]
- Witsø, E.; Persen, L.; Løseth, K.; Bergh, K. Adsorption and release of antibiotics from morselized cancellous bone. In vitro studies of 8 antibiotics. Acta Orthop. Scand. 1999, 70, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Witso, E.; Persen, L.; Loseth, K.; Benum, P.; Bergh, K. Cancellous bone as an antibiotic carrier. Acta Orthop. Scand. 2000, 71, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Gruskin, E.; Doll, B.A.; Futrell, F.W.; Schmitz, J.P.; Hollinger, J.O. Demineralized bone matrix in bone repair: History and use. Adv. Drug Deliv. Rev. 2012, 64, 1063–1077. [Google Scholar] [CrossRef] [PubMed]
- Hou, H.; Li, B.; Zhang, Z.; Xue, C.; Yu, G.; Wang, J.; Bao, Y.; Bu, L.; Sun, J.; Peng, Z.; et al. Moisture absorption and retention properties, and activity in alleviating skin photodamage of collagen polypeptide from marine fish skin. Food Chem. 2012, 135, 1432–1439. [Google Scholar] [CrossRef]
- Thitiset, T.; Damrongsakkul, S.; Bunaprasert, T.; Leeanansaksiri, W.; Honsawek, S. Development of collagen/demineralized bone powder scaffolds and periosteum-derived cells for bone tissue engineering application. Int. J. Mol. Sci. 2013, 14, 2056–2071. [Google Scholar] [CrossRef]
- Sohling, N.; Leiblein, M.; Schaible, A.; Janko, M.; Schwable, J.; Seidl, C.; Brune, J.C.; Nau, C.; Marzi, I.; Henrich, D.; et al. First Human Leucocyte Antigen (HLA) Response and Safety Evaluation of Fibrous Demineralized Bone Matrix in a Critical Size Femoral Defect Model of the Sprague-Dawley Rat. Materials 2020, 13, 3120. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Brazel, C.S. On the importance and mechanisms of burst release in matrix-controlled drug delivery systems. J. Control. Release 2001, 73, 121–136. [Google Scholar] [CrossRef]
- Borcherding, K.; Marx, D.; Gatjen, L.; Bormann, N.; Wildemann, B.; Specht, U.; Salz, D.; Thiel, K.; Grunwald, I. Burst Release of Antibiotics Combined with Long-Term Release of Silver Targeting Implant-Associated Infections: Design, Characterization and in vitro Evaluation of Novel Implant Hybrid Surface. Materials 2019, 12, 3838. [Google Scholar] [CrossRef]
- Sorensen, T.S.; Sorensen, A.I. Bactericidal activity of gentamicin against S. aureus. In vitro study questions value of prolonged high concentrations. Acta Orthop. Scand. 1993, 64, 82–84. [Google Scholar] [CrossRef]
- Ueng, S.W.; Hsieh, P.H.; Shih, H.N.; Chan, Y.S.; Lee, M.S.; Chang, Y. Antibacterial activity of joint fluid in cemented total-knee arthroplasty: An in vivo comparative study of polymethylmethacrylate with and without antibiotic loading. Antimicrob. Agents Chemother. 2012, 56, 5541–5546. [Google Scholar] [CrossRef]
- Eidem, T.M.; Coughlan, A.; Towler, M.R.; Dunman, P.M.; Wren, A.W. Drug-eluting cements for hard tissue repair: A comparative study using vancomycin and RNPA1000 to inhibit growth of Staphylococcus aureus. J. Biomater. Appl. 2014, 28, 1235–1246. [Google Scholar] [CrossRef] [PubMed]
- Von Stechow, D.; Rauschmann, M. Effectiveness of combination use of antibiotic-loaded PerOssal® with spinal surgery in patients with spondylodiscitis. Eur. Surg. Res. 2009, 43, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Beuttel, E.; Bormann, N.; Pobloth, A.M.; Duda, G.N.; Wildemann, B. Impact of Gentamicin-Loaded Bone Graft on Defect Healing in a Sheep Model. Materials 2019, 12, 1116. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bormann, N.; Schmock, A.; Hanke, A.; Eras, V.; Ahmed, N.; Kissner, M.S.; Wildemann, B.; Brune, J.C. Analysis of the Ability of Different Allografts to Act as Carrier Grafts for Local Drug Delivery. J. Funct. Biomater. 2023, 14, 305. https://doi.org/10.3390/jfb14060305
Bormann N, Schmock A, Hanke A, Eras V, Ahmed N, Kissner MS, Wildemann B, Brune JC. Analysis of the Ability of Different Allografts to Act as Carrier Grafts for Local Drug Delivery. Journal of Functional Biomaterials. 2023; 14(6):305. https://doi.org/10.3390/jfb14060305
Chicago/Turabian StyleBormann, Nicole, Aysha Schmock, Anja Hanke, Volker Eras, Norus Ahmed, Maya S. Kissner, Britt Wildemann, and Jan C. Brune. 2023. "Analysis of the Ability of Different Allografts to Act as Carrier Grafts for Local Drug Delivery" Journal of Functional Biomaterials 14, no. 6: 305. https://doi.org/10.3390/jfb14060305