

Guided Bone Regeneration in a Periodontally Compromised Individual with Autogenous Tooth Bone Graft: A Radiomics Analysis
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
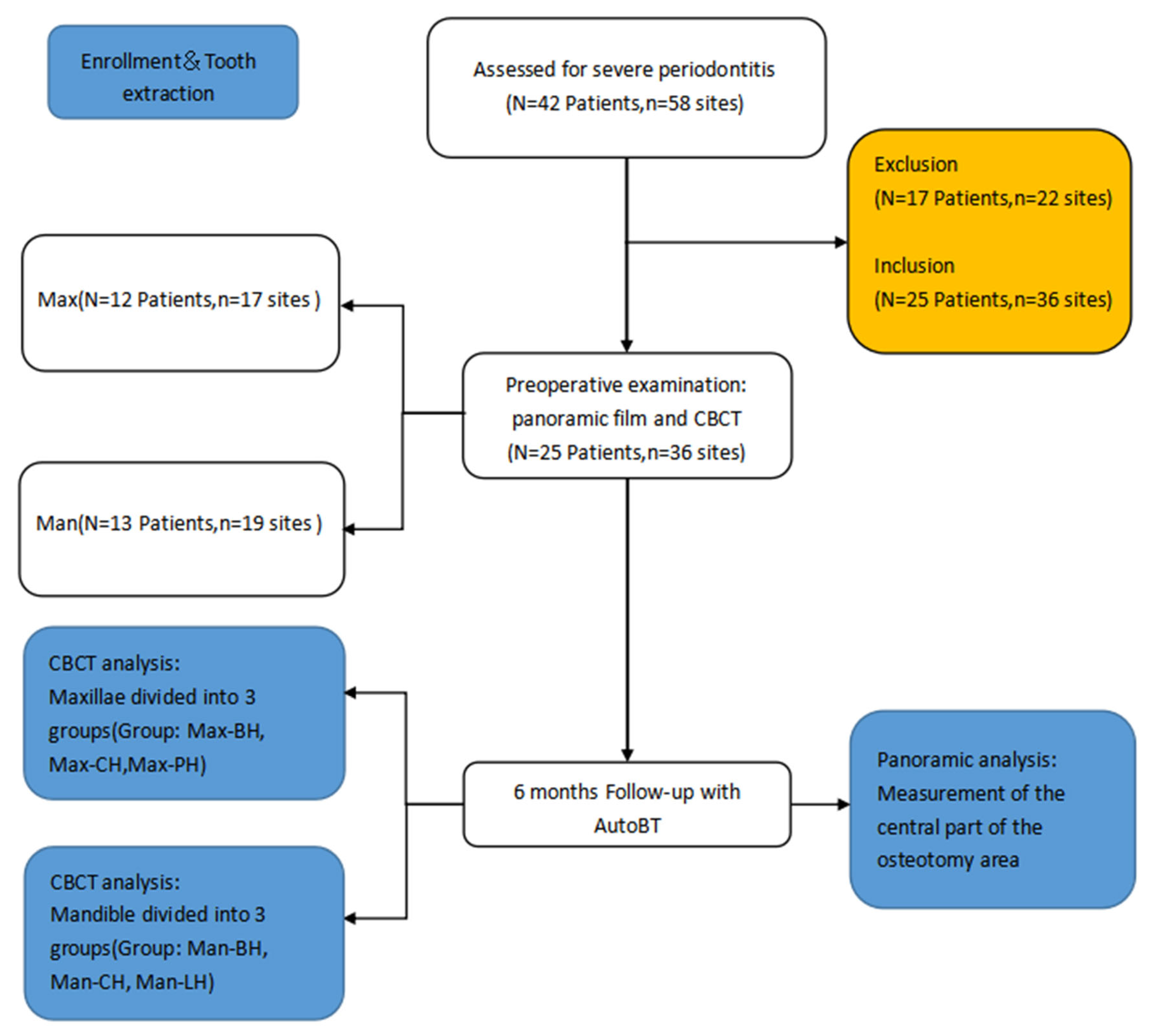
2.1. Ethics and Sample Selection
2.2. Patient Selection
- (a)
- Patient inclusion criteria:
- No history of underlying disease;
- Extraction cases of single premolar or molar with no significant chronic endodontic lesions;
- Patients who have achieved or maintained a healthy periodontal status after ultrasonic scaling;
- Healthy oral hygiene: no obvious supragingival calculus, no obvious redness or swelling of the gingiva, Debris Index ≤ 1, Plaque index ≤ 1 after oral hygiene instruction and good compliance;
- Severe periodontal disease as defined [10] by alveolar bone resorption exceeding two-thirds of the root length of the tooth in X-ray, tooth mobility 2–3, probing depth > 6 mm.
- (b)
- Patient exclusion criteria:
- Have severe systemic diseases and cannot undergo surgery;
- Have serious psychological or mental illness;
- Smoking more than 10 cigarettes per day;
- Pregnant and/or breastfeeding;
- Have an acute infection in the affected or adjacent teeth;
- Diagnosed with bone diseases, and have taken bisphosphonates for a long period;
- Patients with blood disorders, taking blood-thinning drugs.
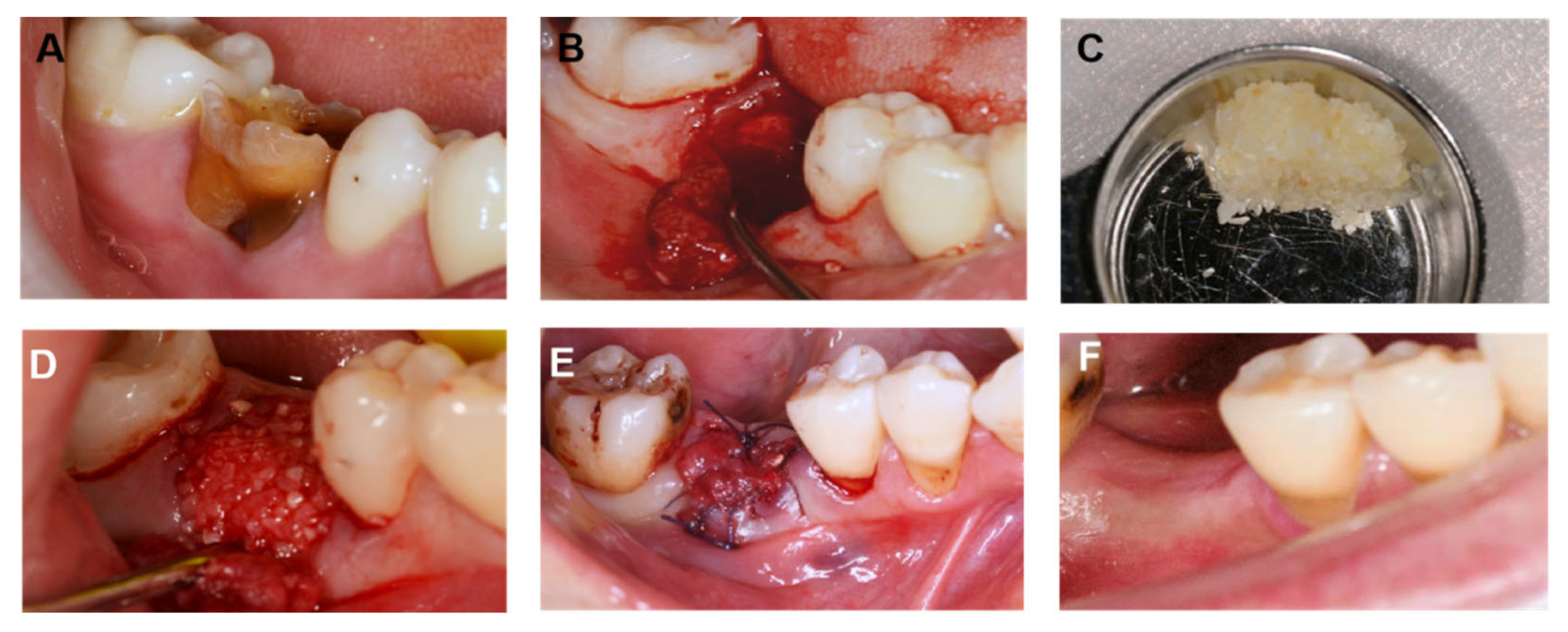
2.3. Material Preparation
- BonMaker® Automatic dental bone-graft-material preparation machine (Shenyang, China);
- BonMaker® Automatic dental bone-graft-material disinfection solution (Shenyang, China);
- Geistlich Bio-Gide® collagen membrane (Osteohealth, Zurich, Switzerland);
- TaiHe® Non-absorbent nylon suture (Chengdu, China)
AutoBT Preparation
2.4. Surgical Method
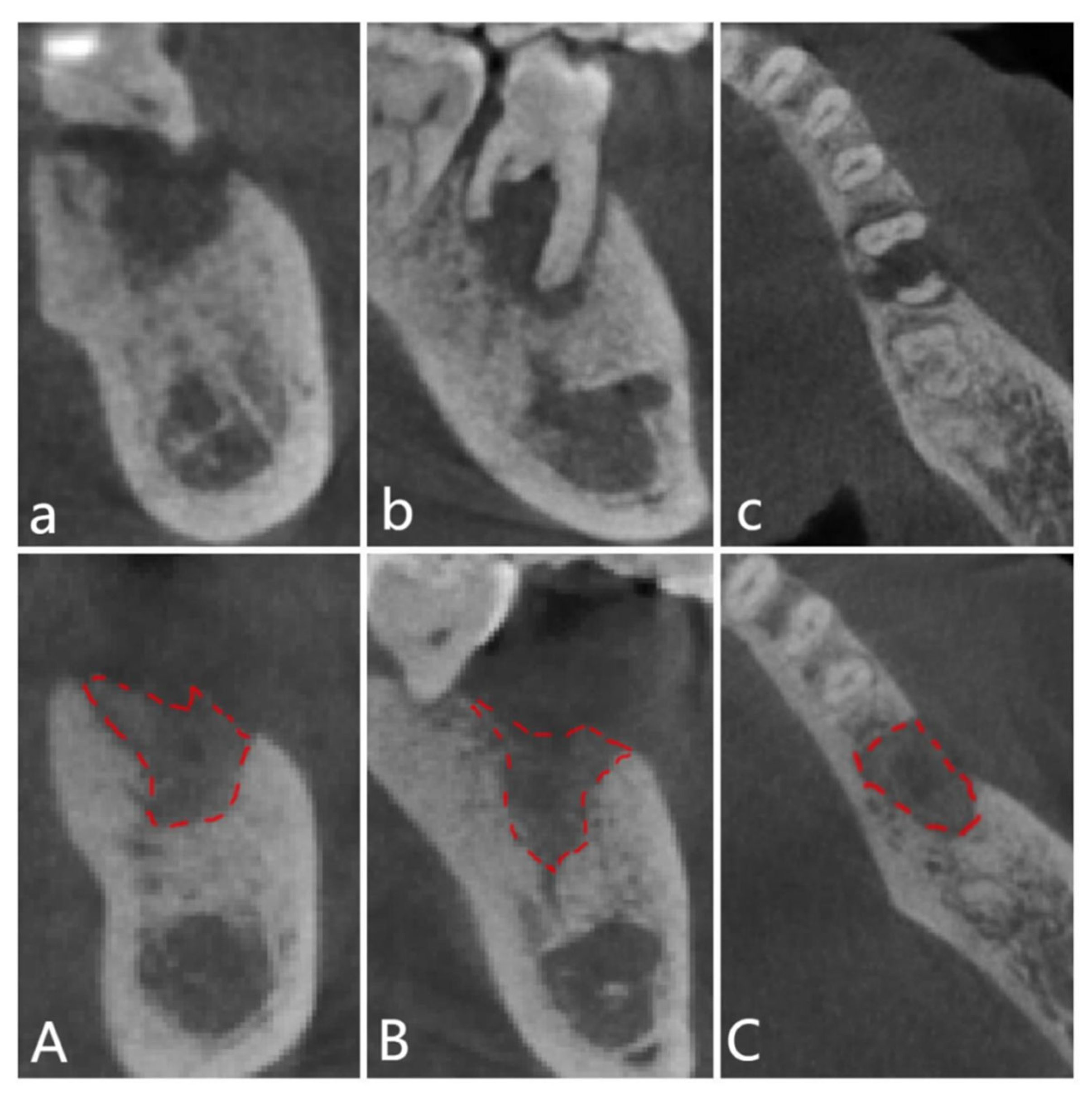
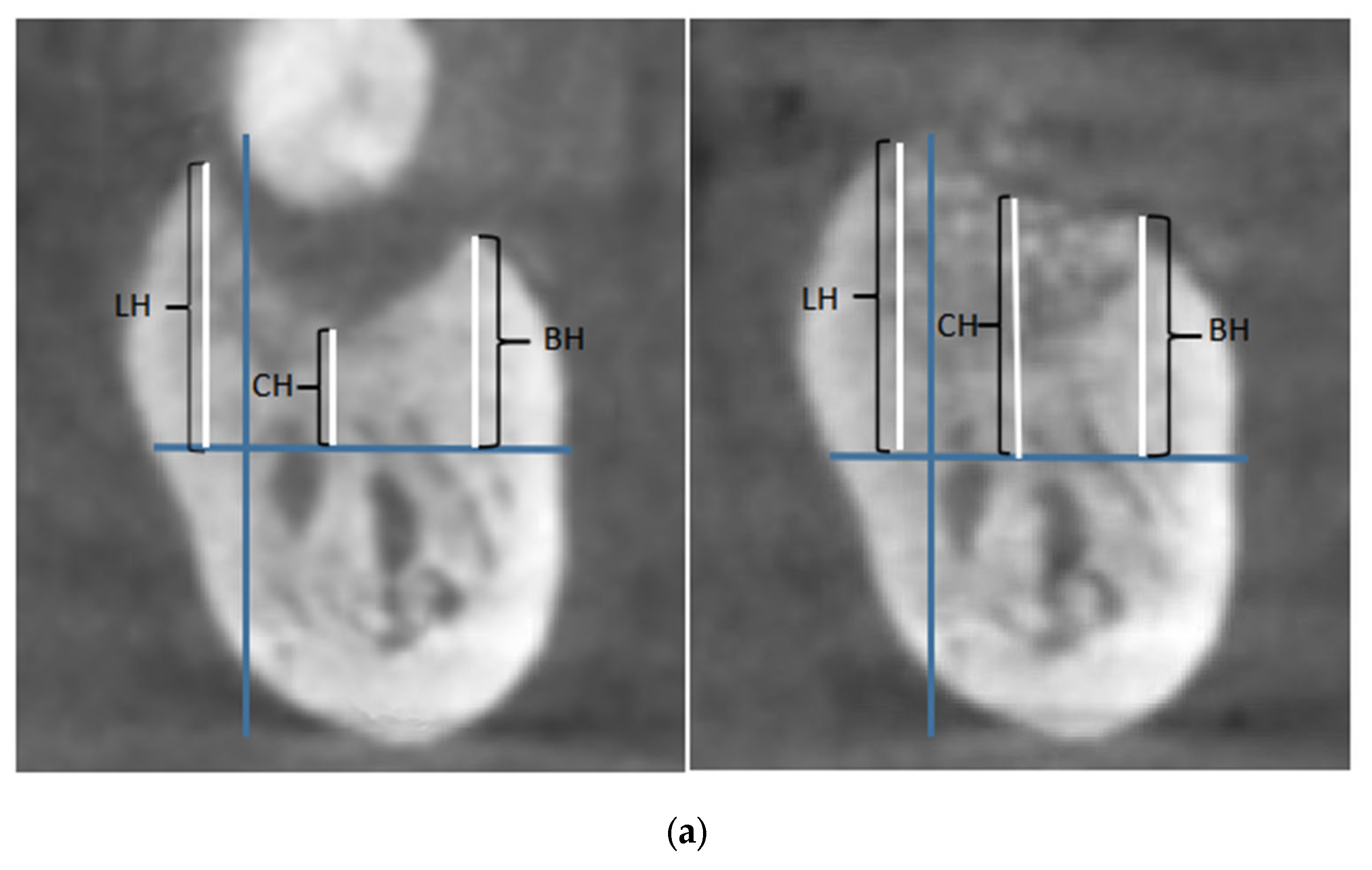
2.5. Observation Indicator
2.6. Statistical Analysis
3. Results
4. Case Report
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Primer 2017, 3, 17038. [Google Scholar] [CrossRef]
- Wong, L.B.; Yap, A.U.; Allen, P.F. Periodontal disease and quality of life: Umbrella review of systematic reviews. J. Periodontal Res. 2020, 56, 1–17. [Google Scholar] [CrossRef]
- Wu, H.; Qiu, W.; Zhu, X.; Li, X.; Xie, Z.; Carreras, I.; Dedeoglu, A.; Van Dyke, T.; Han, Y.W.; Karimbux, N.; et al. The Periodontal Pathogen Fusobacterium nucleatum Exacerbates Alzheimer’s Pathogenesis via Specific Pathways. Front. Aging Neurosci. 2022, 14, 912709. [Google Scholar] [CrossRef] [PubMed]
- Sansores-España, D.; Carrillo-Avila, A.; Melgar-Rodriguez, S.; Díaz-Zuñiga, J.; Martínez-Aguilar, V. Periodontitis and alzheimer’s disease. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, e43–e48. [Google Scholar] [CrossRef]
- Ide, M.; Harris, M.; Stevens, A.; Sussams, R.; Hopkins, V.; Culliford, D.; Fuller, J.; Ibbett, P.; Raybould, R.; Thomas, R.; et al. Periodontitis and Cognitive Decline in Alzheimer’s Disease. PLoS ONE 2016, 11, e0151081. [Google Scholar] [CrossRef] [Green Version]
- Cerajewska, T.L.; Davies, M.; West, N.X. Periodontitis: A potential risk factor for Alzheimer’s disease. Br. Dent. J. 2015, 218, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal disease and coronary heart disease incidence: A systematic review and meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079–2086. [Google Scholar] [CrossRef] [Green Version]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal Disease: A Risk Factor for Diabetes and Cardiovascular Disease. Int. J. Mol. Sci. 2019, 20, 1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martu, M.A.; Solomon, S.M.; Toma, V.; Maftei, G.A.; Iovan, A.; Gamen, A.; Hurjui, L.; Rezus, E.; Foia, L.; Forna, N.C. The importance of cytokines in periodontal disease and rheumatoid arthritis. Rev. Rom. J. Oral Rehabil. 2019, 11, 220–240. [Google Scholar]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161, Erratum in: J. Clin. Periodontol. 2019, 46, 787. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.L.; Wong, T.L.; Wong, M.C.; Lang, N.P. A systematic review of postextraction alveolar hard and Soft tissue dimensional changes in humans. Clin. Oral Implant. Res. 2012, 23 (Suppl. 5), 1–21. [Google Scholar] [CrossRef] [PubMed]
- Lekovic, V.; Kenney, E.B.; Weinlaender, M.; Han, T.; Klokkevold, P.; Nedic, M.; Orsini, M. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J. Periodontol. 1997, 68, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Gokdogan, O. Bone grafting in maxillofacial trauma. Curr. Opin. Otolaryngol. Head Neck Surg. 2022, 30, 260–264. [Google Scholar] [CrossRef]
- Arnal, H.M.; Angioni, C.D.; Gaultier, F.; Urbinelli, R.; Urban, I.A. Horizontal guided bone regeneration on knife-edge ridges: A retrospective case–control pilot study comparing two surgical techniques. Clin. Implant. Dent. Relat. Res. 2022, 24, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Farina, R.; Franzini, C.; Trombelli, L.; Simonelli, A. Minimal invasiveness in the transcrestal elevation of the maxillary sinus floor: A systematic review. Periodontology 2022, 2000. Epub ahead of print. [Google Scholar] [CrossRef]
- Pourdanesh, F.; Esmaeelinejad, M.; Aghdashi, F. Clinical outcomes of dental implants after use of tenting for bony augmentation: A systematic review. Br. J. Oral Maxillofac. Surg. 2017, 55, 999–1007. [Google Scholar] [CrossRef]
- Kim, Y.K.; Kim, S.G.; Yun, P.Y.; Yeo, I.S.; Jin, S.C.; Oh, J.S.; Kim, H.J.; Yu, S.K.; Lee, S.Y.; Kim, J.S.; et al. Auogenous teeth used for bone grafting: A comparison with traditional grafting materials. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, e39–e45. [Google Scholar] [CrossRef]
- Kim, Y.K.; Kim, S.G.; Byeon, J.H.; Lee, H.J.; Um, I.U.; Lim, S.C.; Kim, S.Y. Development of a novel bone grafting material using autogenous teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 496–503. [Google Scholar] [CrossRef]
- Boudiffa, M.; Wade-Gueye, N.M.; Guignandon, A.; Vanden-Bossche, A.; Sabido, O.; Aubin, J.E.; Jurdic, P.; Vico, L.; Lafage-Proust, M.H.; Malaval, L. Bone sialoprotein deficiency impairs osteoclastogenesis and mineral resorption in vitro. J. Bone Miner. Res. 2010, 25, 2669–2679. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Lee, J.; Um, I.-W.; Kim, K.-W.; Murata, M.; Akazawa, T.; Mitsugi, M. Tooth-derived bone graft material. J. Korean Assoc. Oral Maxillofac. Surg. 2013, 39, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Schultz, T.H.; Schultz, M. Intact growth factors are conserved in the extracellular matrix of ancient human bone and teeth: A storehouse for the study of human evolution in health and disease. Biol. Chem. 2005, 386, 767–776. [Google Scholar] [CrossRef]
- Rijal, G.; Shin, H.L. Human tooth-derived biomaterial as a graft substitute for hard tissue regeneration. Regen Med. 2017, 12, 263–273. [Google Scholar] [CrossRef]
- Nampo, T.; Watahiki, J.; Enomoto, A.; Taguchi, T.; Ono, M.; Nakano, H.; Yamamoto, G.; Irie, T.; Tachikawa, T.; Maki, K. A new method for alveolar bone repair using extracted teeth for the graf material. J. Periodontol. 2010, 81, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Urist, M.R.; Silverman, B.F.; Düring, K.; Dubuc, F.L.; Rosenberg, J.M. 24 The Bone Induction Principle. Clin. Orthop. Relat. Res. 1967, 53, 243–283. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Kim, S.G.; Oh, J.S.; Jin, S.C.; Son, J.S.; Kim, S.Y.; Lim, S.Y. Analysis of the inorganic component of autogenous tooth bone graft material. J. Nanosci. Nanotechnol. 2011, 11, 7442–7445. [Google Scholar] [CrossRef] [PubMed]
- Rosso, M.; Blasi, G.; Gherlone, E.; Rosso, R. Effect of Granulocyte-Macrophage Colony-Stimulating Factor on Prevention of Mucositis in Head and Neck Cancer Patients Treated with Chemo-Radiotherapy. J. Chemother. 1997, 9, 382–385. [Google Scholar] [CrossRef]
- Um, I.-W.; Kim, Y.-K.; Mitsugi, M. Demineralized dentin matrix scaffolds for alveolar bone engineering. J. Indian Prosthodont. Soc. 2017, 17, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, X.; Qi, Y.; Ma, X.; Qiao, S.; Cai, H.; Zhao, B.C.; Jiang, H.B.; Lee, E.S. Comparison of Autogenous Tooth Materials and Other Bone Grafts. Tissue Eng. Regen. Med. 2021, 18, 327–341. [Google Scholar] [CrossRef]
- Kim, Y.K.; Yun, P.Y.; Um, I.W.; Lee, H.J.; Yi, Y.J.; Bae, J.H.; Lee, J. Alveolar ridge preservation of an extraction socket using autogenous tooth bone graft material for implant site development: Prospective case series. J. Adv. Prosthodont. 2014, 6, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Jeong, K.I.; Kim, S.G.; Kim, Y.K.; Oh, J.S.; Jeong, M.A.; Park, J.J. Clinical study of graft materials using autogenous teeth in maxillary sinus augmentation. Implant Dent. 2011, 20, 471–475. [Google Scholar] [CrossRef]
- Wessing, B.; Lettner, S.; Zechner, W. Guided Bone Regeneration with Collagen Membranes and Particulate Graft Materials: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 87–100. [Google Scholar] [CrossRef] [PubMed]
- Juan, F.Y.; Al-Sabbagh, M. Use of Cone-Beam Computed Tomography in Early Detection of Implant Failure. Dent. Clin. N. Am. 2015, 59, 41–56. [Google Scholar]
- Si, J.; Zhu, Y.; Zhang, Z.; Ding, C.; Xia, L. Clinical evaluation of curved body layer film and cone beam CT for bone volume measurement in the implant area. J. Anhui Med. Univ. 2015, 50, 393–395. [Google Scholar]
- Wiltfang, J.; Schultze-Mosgau, S.; Nkenke, E.; Thorwarth, M.; Neukam, F.; Schlegel, K. Onlay augmentation versus sinuslift procedure in the treatment of the severely resorbed maxilla: A 5-year comparative longitudinal study. Int. J. Oral Maxillofac. Surg. 2005, 34, 885–889. [Google Scholar] [CrossRef]
- Naitoh, M.; Saburi, K.; Gotoh, K.; Kurita, K.; Ariji, E. Metal artifacts from posteriormandibular implants as seen in CBCT. Implant Dent. 2013, 22, 151–154. [Google Scholar] [CrossRef]
- Guo, W.; He, Y.; Zhang, X.; Lu, W.; Wang, C.; Yu, H.; Liu, Y.; Li, Y.; Zhou, Y.; Zhou, J.; et al. The use of dentin matrix scaffold and dental follicle cells for dentin regeneration. Biomaterials 2009, 30, 6708–6723. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Guo, W.; Yang, B.; Guo, L.; Sheng, L.; Chen, G.; Li, Y.; Zou, Q.; Xie, D.; An, X.; et al. Human treated dentin matrix as a natural scaffold for complete human dentin tissue regeneration. Biomaterials 2011, 32, 4525–4538. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Yeung, K.W.K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2017, 2, 224–247. [Google Scholar] [CrossRef]
- Gao, J.; Symons, A.; Bartold, P. Expression of Transforming Growth Factor-beta 1 (TGF-β1) in the Developing Periodontium of Rats. J. Dent. Res. 1998, 77, 1708–1716. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Wikesjö, U.M.E. Growth and differentiation factors for periodontal regeneration: A review on factors with clinical testing. J. Periodontal Res. 2012, 47, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.; Um, I.; Kim, Y.; Woo, J.; Lee, J. Autogenous demineralized dentin matrix from extracted tooth for the augmentation of alveolar bone defect: A prospective randomized clinical trial in comparison with anorganic bovine bone. Clin. Oral Implant. Res. 2016, 28, 809–815. [Google Scholar] [CrossRef]
- Camelo, M.; Nevins, M.L.; Schenk, R.K.; Simion, M.; Rasperini, G.; Lynch, S.E. Clinical, radiographic, and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int. J. Periodontics Restor. Dent. 1998, 18, 321–331. [Google Scholar]
- Gelețu, G.L.; Burlacu, A.; Murariu, A.; Andrian, S.; Golovcencu, L.; Baciu, E.-R.; Maftei, G.; Onica, N. Customized 3D-Printed Titanium Mesh Developed for an Aesthetic Zone to Regenerate a Complex Bone Defect Resulting after a Deficient Odontectomy: A Case Report. Medicina 2022, 58, 1192. [Google Scholar] [CrossRef]
- Gual-Vaqués, P.; Polis-Yanes, C.; Estrugo-Devesa, A.; Ayuso-Montero, R.; Marí-Roig, A.; López-López, J. Autogenous teeth used for bone grafting: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e112–e119. [Google Scholar] [CrossRef] [PubMed]
- Kozloysky, A.; Aboodi, G.; Moses, O.; Tal, H.; Artzi, Z.; Weinreb, M.; Nemcovsky, C.E. Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin. Oral. Implant. Res. 2009, 20, 1116–1123. [Google Scholar] [CrossRef]
- Lee, S.-H.; Lim, Y.-M.; Jeong, S.I.; An, S.-J.; Kang, S.-S.; Jeong, C.-M.; Huh, J.-B. The effect of bacterial cellulose membrane compared with collagen membrane on guided bone regeneration. J. Adv. Prosthodont. 2015, 7, 484–495. [Google Scholar] [CrossRef] [Green Version]
- Ottoni, J.M.P.; Oliveira, Z.F.L.; Mansini, R.; Cabral, A.M. Correlation between placement torque and survival of single-tooth implants. Int. J. Oral Maxillofac. Implant. 2005, 20, 769–776. [Google Scholar]
- Merli, M.; Migani, M.; Esposito, M. Vertical ridge augmentation with autogenous bone grafts: Resorbable barriers supported by ostheosynthesis plates versus titanium-reinforced barriers. A preliminary report of a blinded, randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2007, 22, 373–382. [Google Scholar]
- Minamizato, T.; Koga, T.; Takashi, I.; Nakatani, Y.; Umebayashi, M.; Sumita, Y.; Asahina, I. Clinical application of autogenous partially demineralized dentin matrix prepared immediately after extraction for alveolar bone regeneration in implant dentistry: A pilot study. Int. J. Oral Maxillofac. Surg. 2017, 47, 125–132. [Google Scholar] [CrossRef]
- Tecco, S.; Grusovin, M.G.; Sciara, S.; Bova, F.; Pantaleo, G.; Cappare, P. The association between three attitude-related indexes of oral hygiene and secondary implant failures: A retrospective longitudinal study. Int. J. Dent. Hyg. 2018, 16, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Kim, H.; Lee, D.; Park, C. Superimposition of a cone beam computed tomography (CBCT) scan and a photograph: A dental technique. J. Prosthet. Dent. 2021, 125, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Isman, O. Evaluation of jaw bone density and morphology in bruxers using panoramic radiography. J. Dent. Sci. 2020, 16, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M.; Fejérdy, P.; Dobó, N.C. Metal artefact on head and neck cone-beam CT images. Fogorv. Szle. 2008, 101, 171–178. [Google Scholar]
- Signorelli, L.; Patcas, R.; Peltomäki, T.; Schätzle, M. Radiation dose of cone-beam computed tomography compared to conventional radiographs in orthodontics. J. Orofac. Orthop. 2016, 77, 9–15. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Male | 11 |
| Female | 14 | |
| Age | Mean | 46 |
| Range | 28–60 | |
| Tooth position (N = 36) | First premolar | 3 |
| Second premolar | 5 | |
| First molar | 14 | |
| Second molar | 14 |
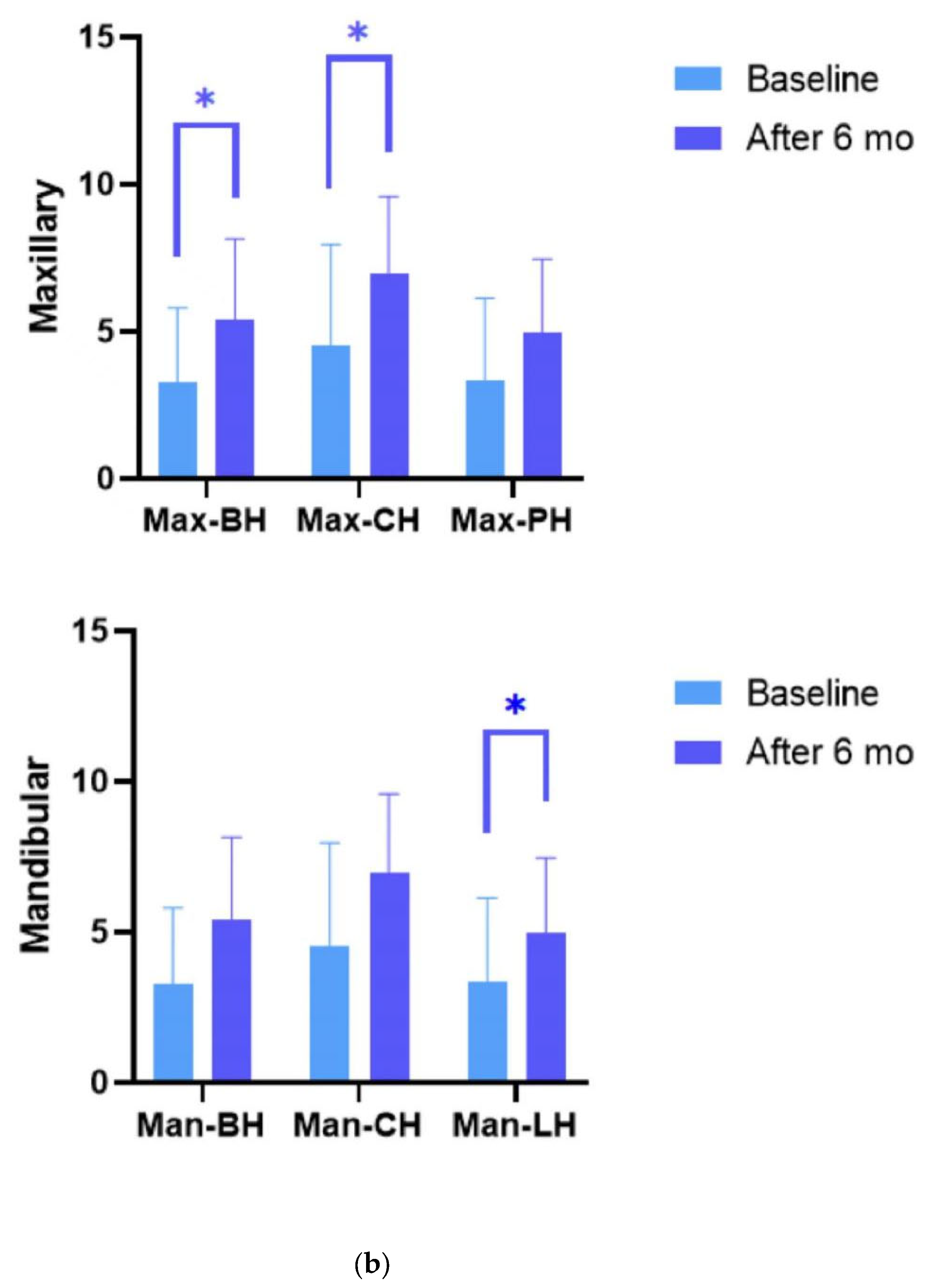
| Parameter | Baseline | After 6 Mo. | Change | p-Value |
|---|---|---|---|---|
| BH, mm | 3.25 ± 2.55 | 5.40 ± 2.74 | −2.15 ± 2.90 | 0.001 ** |
| CH, mm | 4.50 ± 3.46 | 6.95 ± 2.63 | −2.45 ± 2.36 | 0.001 ** |
| PH, mm | 3.33 ± 2.80 | 4.95 ± 2.51 | −1.62 ± 3.19 | 0.053 |
| Parameter | Baseline | After 6 Mo. | Change | p-Value |
|---|---|---|---|---|
| BH, mm | 11.86 ± 4.33 | 11.66 ± 2.59 | 0.19 ± 3.52 | 0.968 |
| CH, mm | 13.30 ± 2.665 | 14.01 ± 2.85 | −0.70 ± 2.71 | 0.272 |
| LH, mm | 8.81 ± 4.58 | 13.88 ± 2.91 | −5.07 ± 4.34 | <0.001 *** |
| Parameter | Baseline | After 6 Mo. | Change | p-Value |
|---|---|---|---|---|
| Bone height, mm | 6.63 ± 3.75 | 9.82 ± 3.72 | −3.19 ± 0.88 | <0.001 *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Jin, F.; Wang, R.; Shang, X.; Yang, P.; Zhu, Y.; Tsoi, J.K.H.; Chan, K.; Wang, S. Guided Bone Regeneration in a Periodontally Compromised Individual with Autogenous Tooth Bone Graft: A Radiomics Analysis. J. Funct. Biomater. 2023, 14, 220. https://doi.org/10.3390/jfb14040220
Li J, Jin F, Wang R, Shang X, Yang P, Zhu Y, Tsoi JKH, Chan K, Wang S. Guided Bone Regeneration in a Periodontally Compromised Individual with Autogenous Tooth Bone Graft: A Radiomics Analysis. Journal of Functional Biomaterials. 2023; 14(4):220. https://doi.org/10.3390/jfb14040220
Chicago/Turabian StyleLi, Jingyu, Feifan Jin, Renfei Wang, Xiaodan Shang, Peiran Yang, Yuchi Zhu, James K. H. Tsoi, Ki Chan, and Shuhua Wang. 2023. "Guided Bone Regeneration in a Periodontally Compromised Individual with Autogenous Tooth Bone Graft: A Radiomics Analysis" Journal of Functional Biomaterials 14, no. 4: 220. https://doi.org/10.3390/jfb14040220