

Calcium Phosphate Cements Combined with Blood as a Promising Tool for the Treatment of Bone Marrow Lesions
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Calcium Phosphate Cements and Their Blood Composites
2.2. Methods
2.2.1. Laser Granulometry
2.2.2. High Frequency Impedance
2.2.3. SEM Characterization
2.2.4. Injectability, Cohesion, and Decalcification Studies
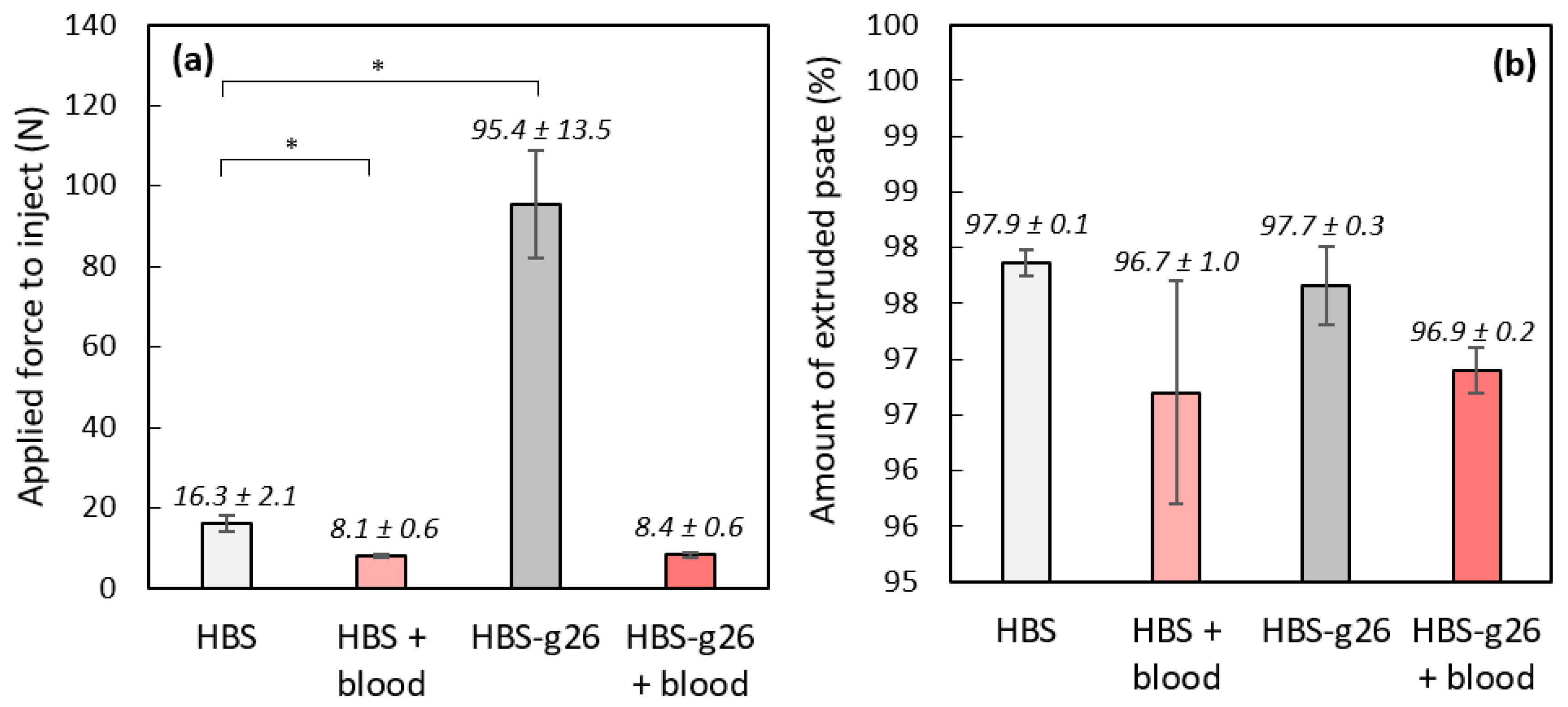
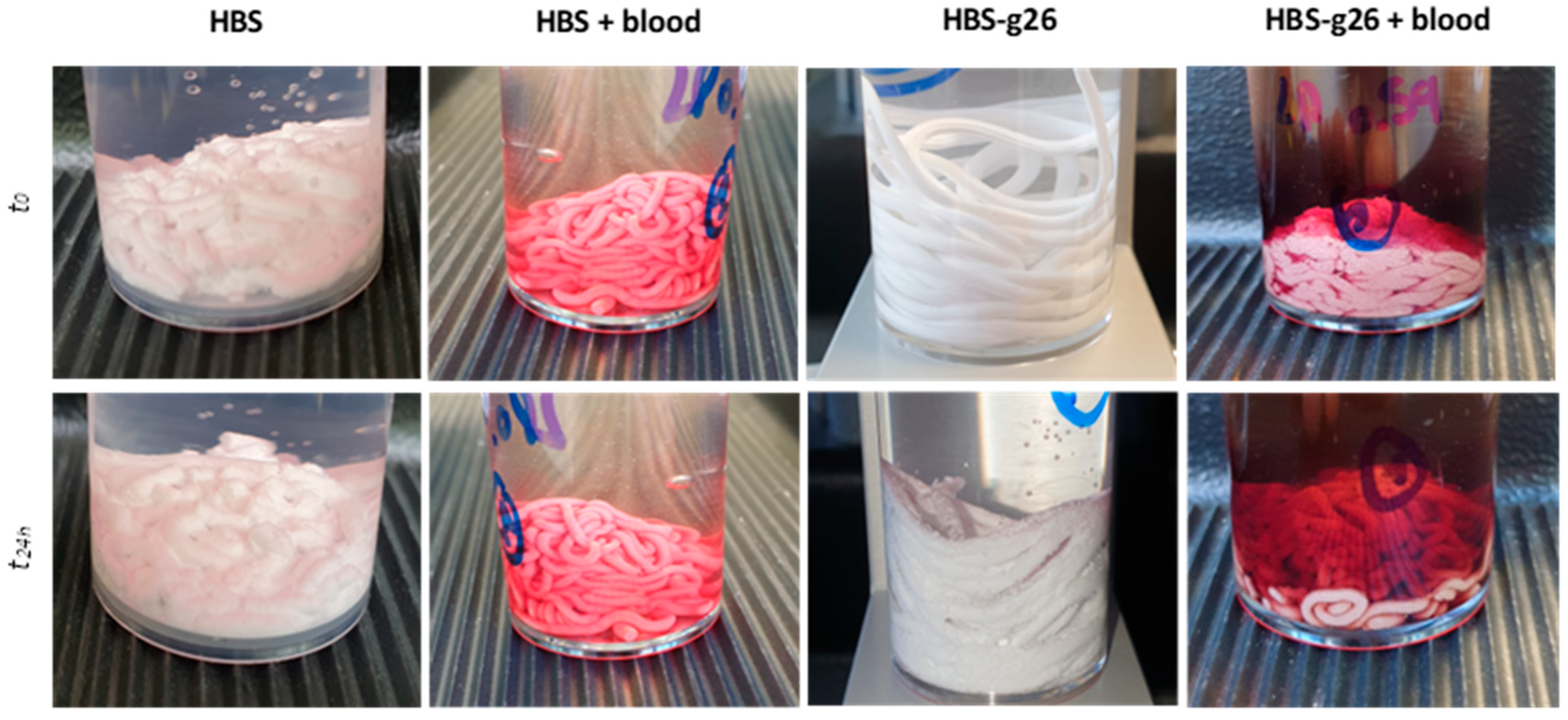
- Injectabilities were assessed using a texture analyzer (LLOYD Ametek LS5, AMETEK STC, Elancourt, France) equipped with a 5 kN sensor (5KN0634, LLOYD Ametek, AMETEK STC, Elancourt, France). The test consists in measuring the required force to extrude a cement paste from a syringe. In practice, after mixing the solid and liquid phases together in a mortar for 1 min, the cement paste was transferred into a 1.6 mm section syringe (5 mL, TERUMO, Shibuya City, Tokyo, Japan). The syringe was then placed on the texture analyzer and the experiments were started 15 min after the beginning of the mixing, as recommended by the manufacturer for the use of HBS. The displacement speed applied to the syringe plunger was set at 1 mm·s−1 and the force necessary for extrusion was recorded until full injection of the paste or until a maximal value of 100 N was reached. A picture of the device setup is given in the Supplementary Materials section. The extruded paste was directly collected in a 0.9 wt% sodium chloride solution placed below the syringe outlet. At the end of the extrusion, this solution was placed in an oven at 27 °C, and the cohesion of the paste right after injection and 24 h later was visually controlled. Each measurement was run in triplicate and the results are given as mean ± standard deviation (SD). The syringe was weighed empty and once filled with the cement sample. The syringe was weighed again at the end of the extrusion process, thus allowing us to determine the percentage of extruded paste for each assay.
- Once hardened for 72 h in a 0.9 wt% NaCl solution at 37 °C, the molded cylindrical samples of CPC combined with blood (6 mm in diameter and 12 mm in height) were decalcified by immersion in 30 mL of a 10 wt% aqueous solution of ethylenediaminetetraacetic acid (EDTA, Merck KGaA, Darmstadt, Germany) at room temperature for 3 weeks, with a renewal of the EDTA solution every 5 days. Then, the samples were successively submerged in a 4 wt% formaldehyde solution (5 mL, 2 days), 70% ethanol (10 mL, 1 day), 90% ethanol (10 mL, 1 day), and pure ethanol (10 mL, 8 days). The samples were then rinsed in a water/acetone mixture by increasing the acetone content progressively to end-up with a final rinsing with pure acetone.
2.3. In Vivo Implantation of CPC and Blood Composite CPC
2.3.1. In Vivo Implantation of CPC in Vendeen Sheep Model
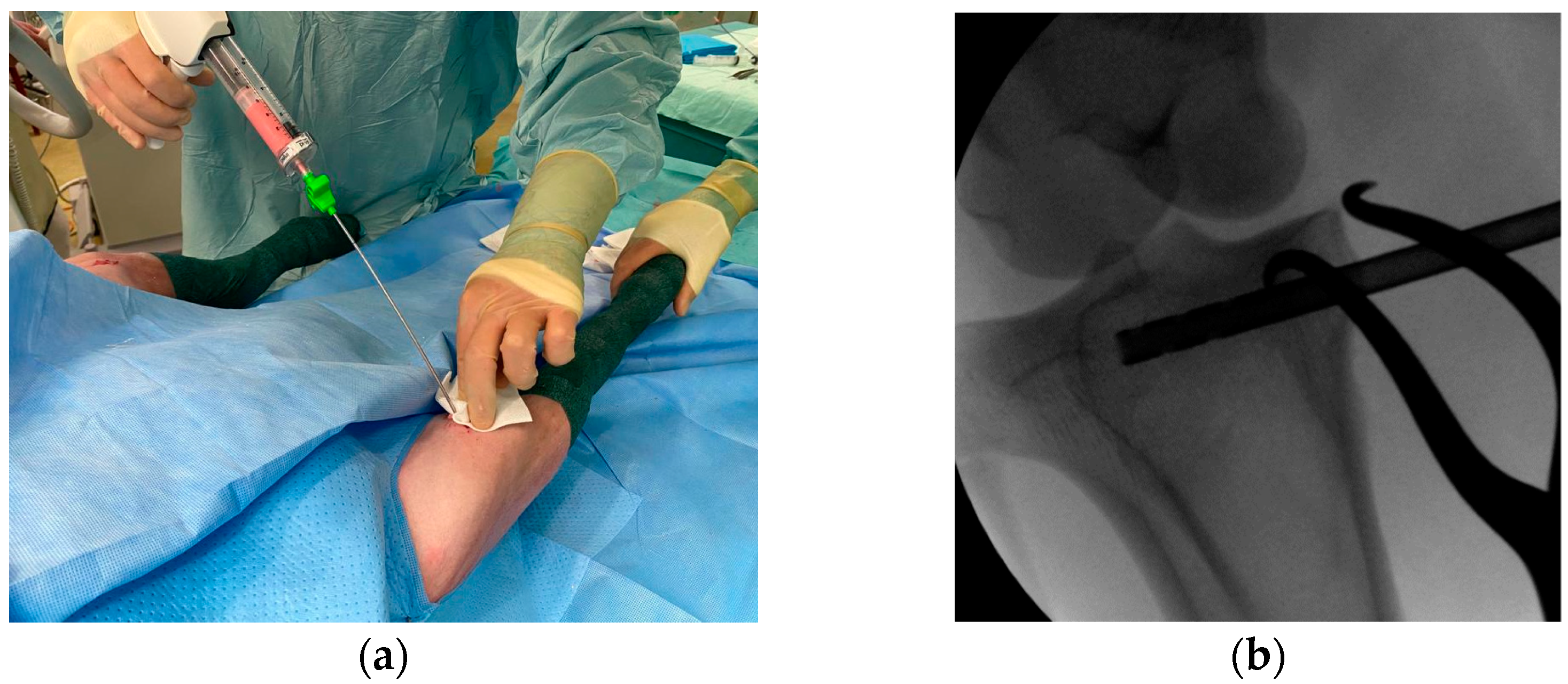
2.3.2. Human Blood CPC Composite
2.4. Data Acquisition and Analyses
2.4.1. Microcomputer Tomography (µ-CT Analyses)
2.4.2. Scanning Electron Microscopy (SEM) Analyses
2.4.3. Histological Analyses
2.4.4. Statistical Analyses
3. Results & Discussions
3.1. Granulometry of the Studied Cement Powders
3.2. Setting Time Monitoring of the Studied Cements Using High Frequency Impedance
3.3. Injectability and Cohesion Assessment of the Studied Cements
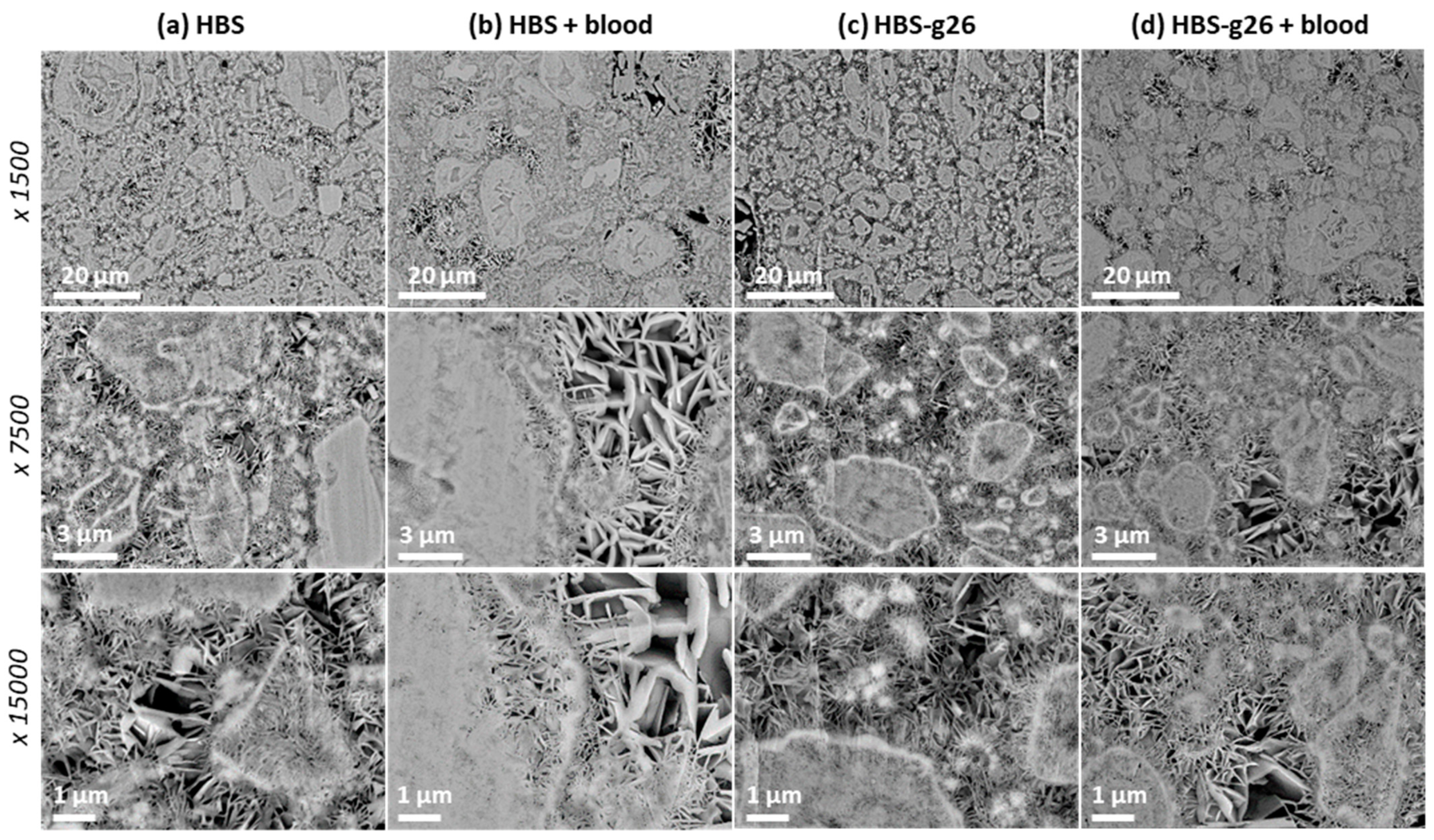
3.4. Analysis of the Microstructure of the Hardened Cements
3.5. In Vivo Implantation of CPCs and Their Blood Composites
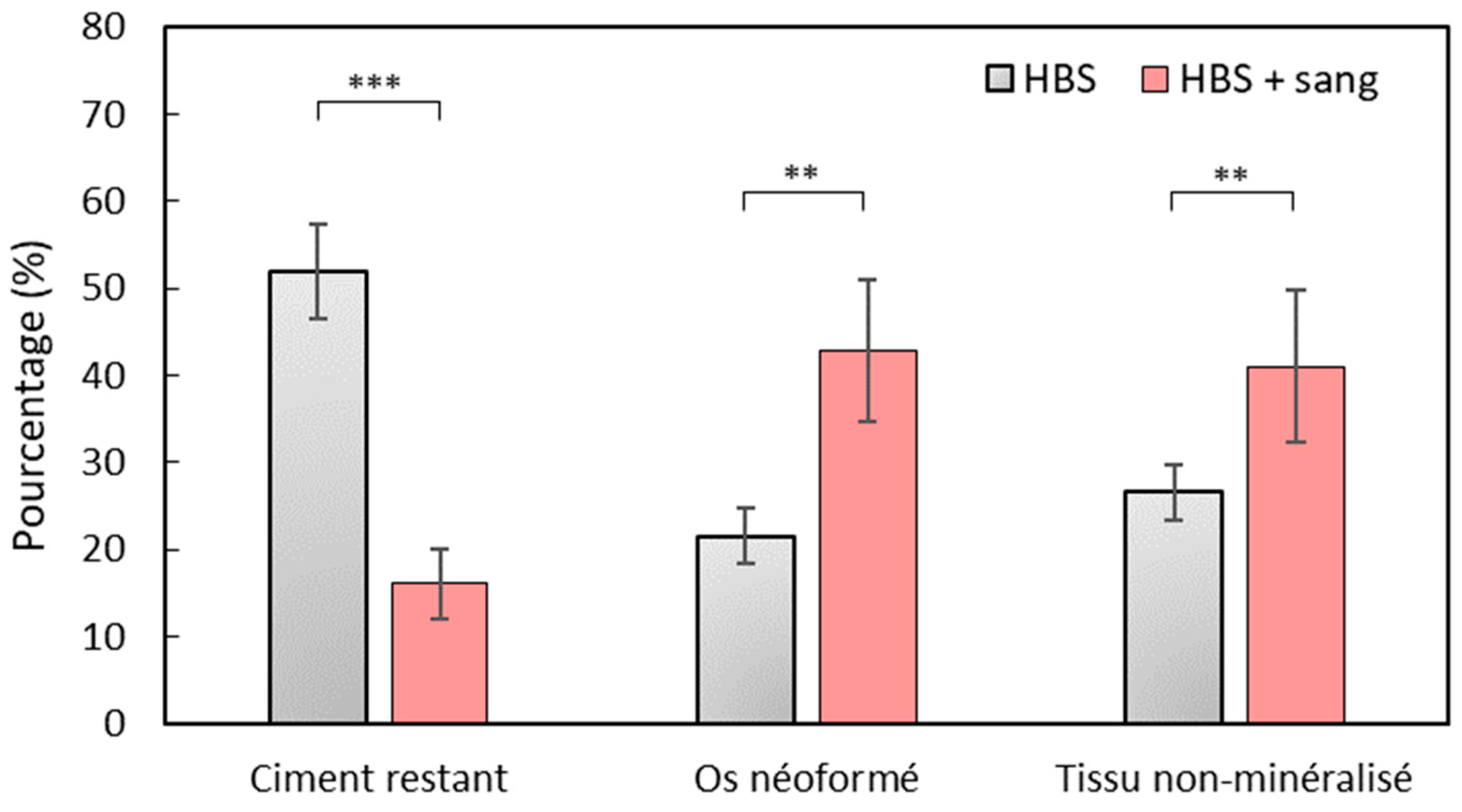
3.6. Microcomputed Tomography (µ-CT) Analysis
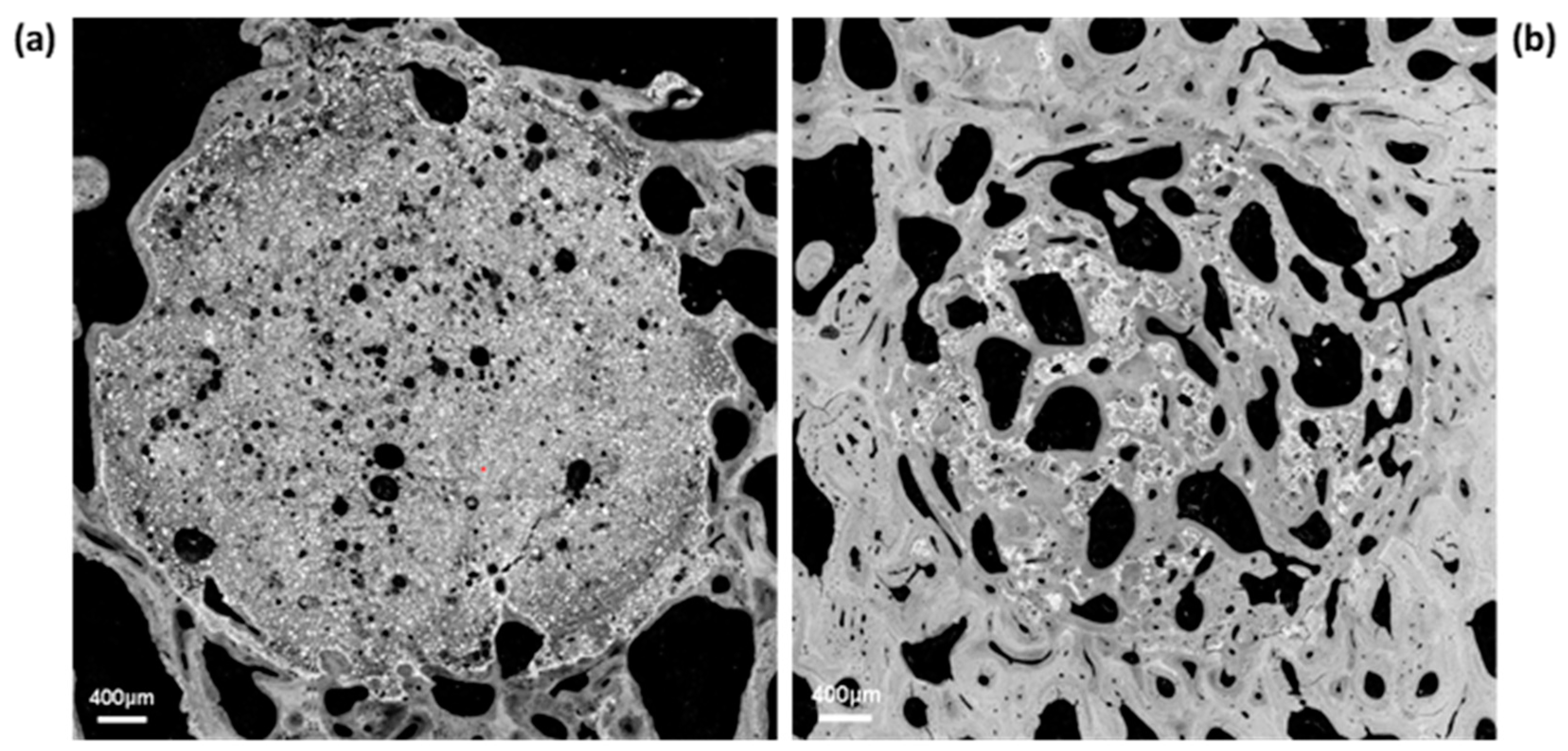
3.7. SEM Analyses
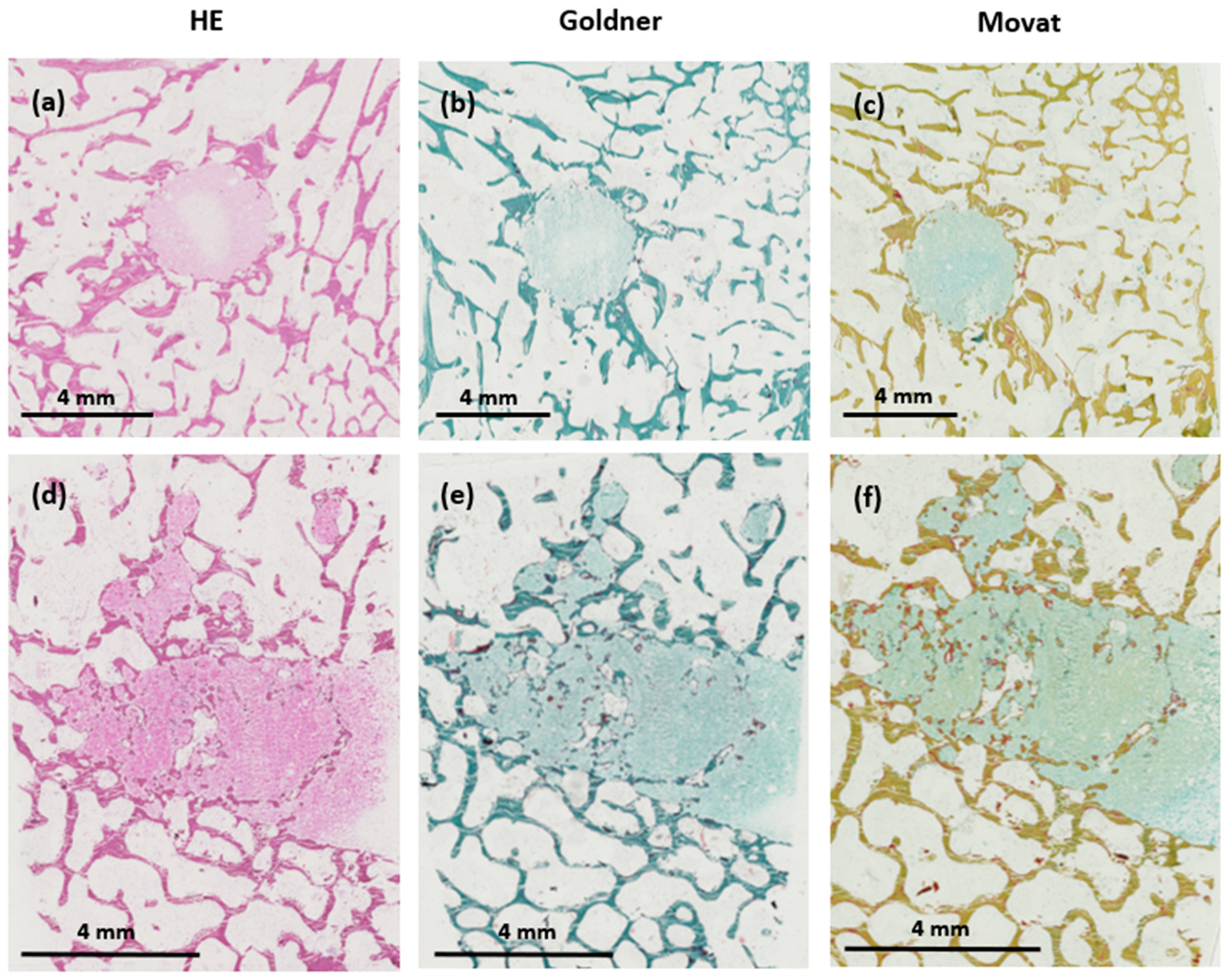
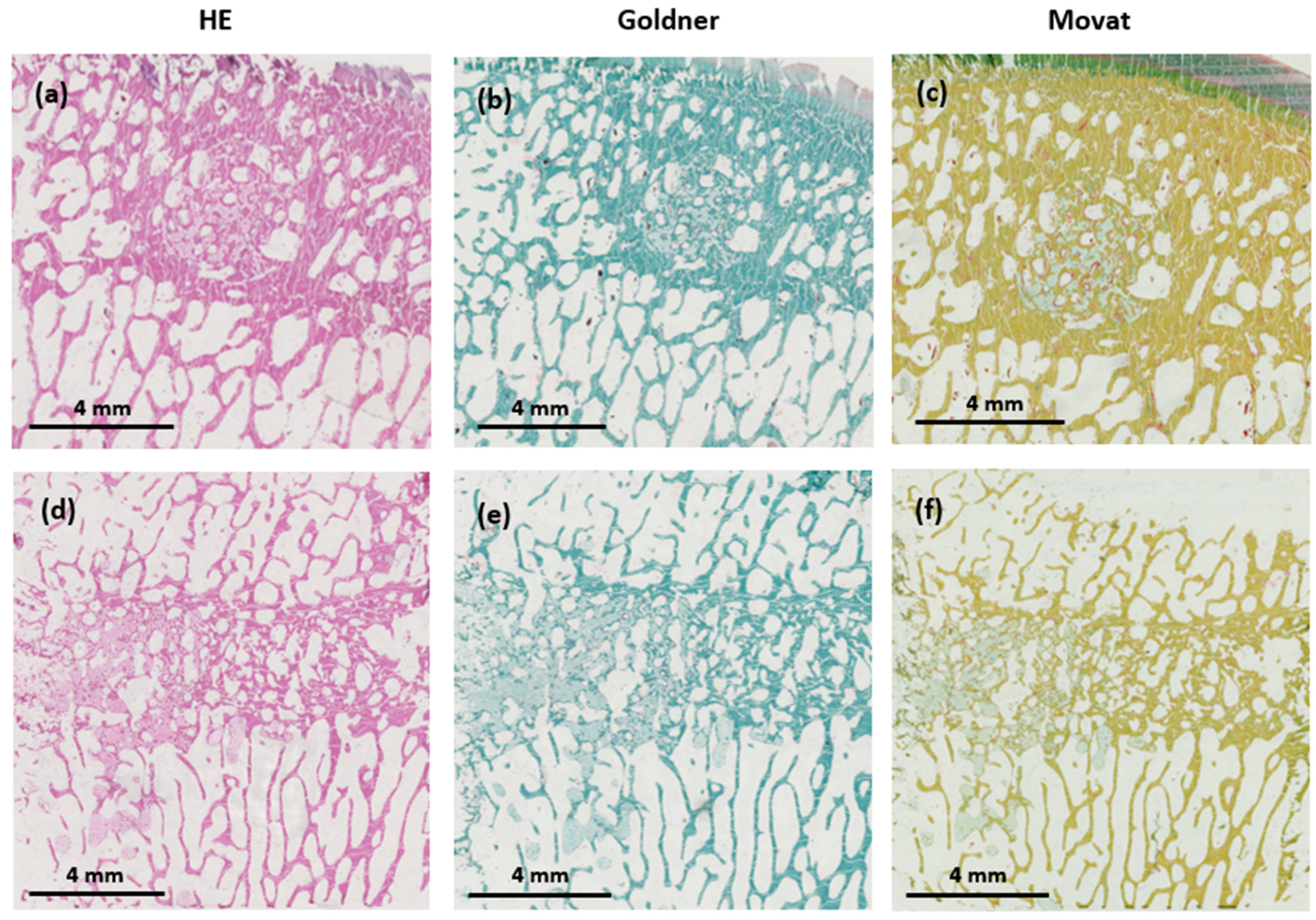
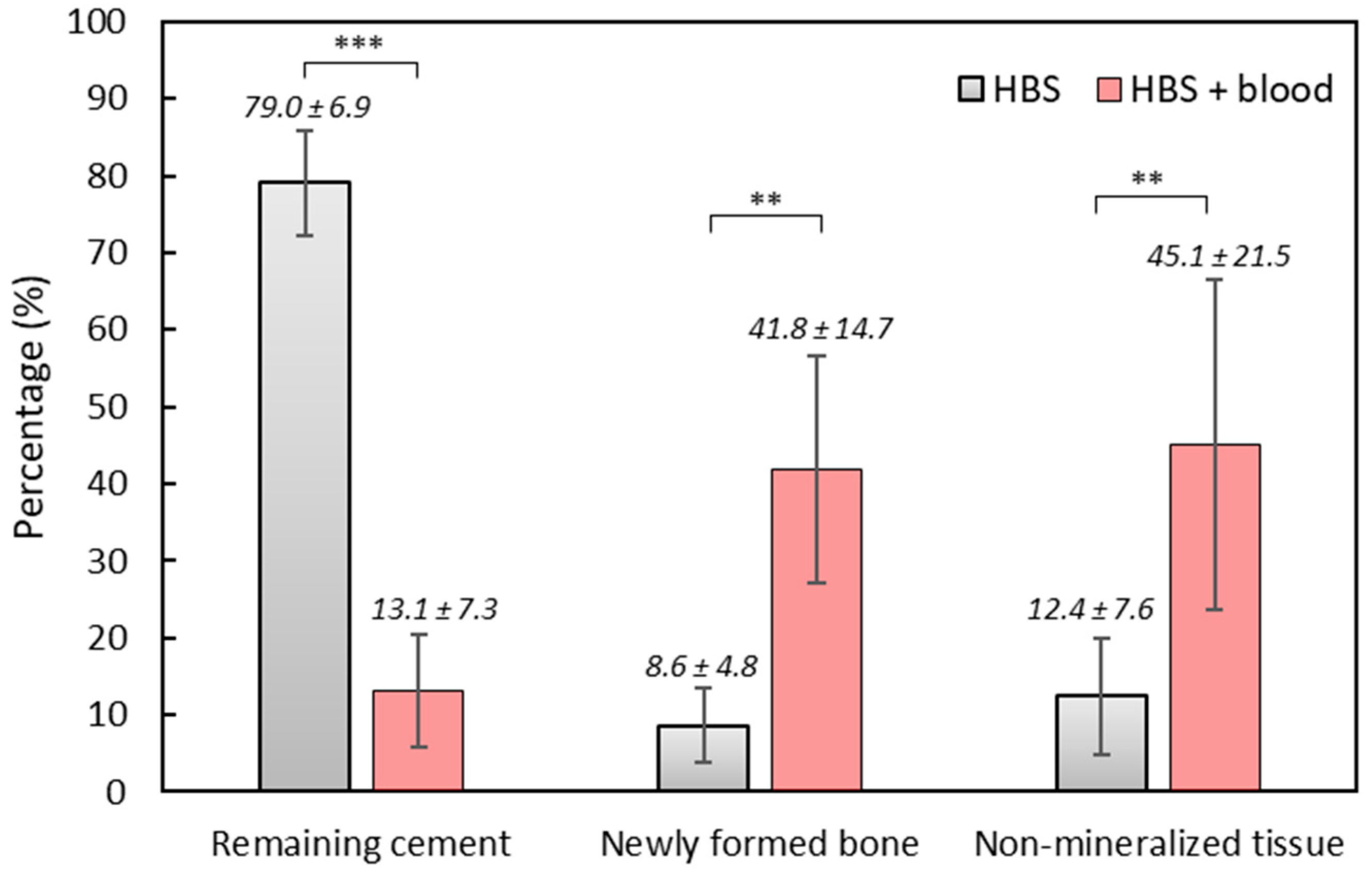
3.8. Light Microscopy Histological Analyses
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, W.E.; Chow, L.C. A New Calcium Phosphate Setting Cement. J. Dent. Res. 1983, 62, 672–679. [Google Scholar]
- LeGeros, R.; Chohayeb, A.; Shulman, A. Apatitic Calcium Phosphates: Possible Restorative Materials. J. Dent. Res. 1982, 61, 343. [Google Scholar]
- Lemaitre, A.M.J. Calcium phosphate Cements: Study of the β-Tricalcium Phosphate—Monocalcium Phosphate System. Biomaterials 1989, 10, 475–480. [Google Scholar]
- Bajammal, S.S.; Zlowodzki, M.; Lelwica, A.; Tornetta, P.; Einhorn, T.A.; Buckley, R.; Leighton, R.; Russell, T.A.; Larsson, S.; Bhandari, M. The Use of Calcium Phosphate Bone Cement in Fracture Treatment. A Meta-Analysis of Randomized Trials. J. Bone Jt. Surg. 2008, 90, 1186–1196. [Google Scholar] [CrossRef]
- Carey, L.; Xu, H.; Simonjr, C.; Takagi, S.; Chow, L. Premixed Rapid-Setting Calcium Phosphate Composites for Bone Repair. Biomaterials 2005, 26, 5002–5014. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.; Bauer, T.W. Use of Injectable Calcium Phosphate Cement for Fracture Fixation: A Review. Clin. Orthop. Relat. Res. 2002, 395, 23–32. [Google Scholar] [CrossRef]
- Larsson, S.; Hannink, G. Injectable Bone-Graft Substitutes: Current Products, Their Characteristics and Indications, and New Developments. Injury 2011, 42, 30–34. [Google Scholar] [CrossRef]
- Liu, H.; Li, H.; Cheng, W.; Yang, Y.; Zhu, M.; Zhou, C. Novel Injectable Calcium Phosphate/Chitosan Composites for Bone Substitute Materials. Acta Biomater. 2006, 2, 557–565. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, W.; Schnitzler, V.; Tancret, F.; Bouler, J.-M. Calcium Phosphate Cements for Bone Substitution: Chemistry, Handling and Mechanical Properties. Acta Biomater. 2014, 10, 1035–1049. [Google Scholar] [CrossRef]
- Alkhraisat, M.H.; Rueda, C.; Mariño, F.T.; Torres, J.; Jerez, L.B.; Gbureck, U.; Cabarcos, E.L. The Effect of Hyaluronic Acid on Brushite Cement Cohesion. Acta Biomater. 2009, 5, 3150–3156. [Google Scholar] [CrossRef]
- Lopez-Heredia, M.A.; Pattipeilohy, J.; Hsu, S.; Grykien, M.; van der Weijden, B.; Leeuwenburgh, S.C.G.; Salmon, P.; Wolke, J.G.C.; Jansen, J.A. Bulk Physicochemical, Interconnectivity, and Mechanical Properties of Calcium Phosphate Cements-Fibrin Glue Composites for Bone Substitute Applications. J. Biomed. Mater. Res. A 2013, 101, 478–490. [Google Scholar] [CrossRef]
- Ko, C.-L.; Chen, W.-C.; Chen, J.-C.; Wang, Y.-H.; Shih, C.-J.; Tyan, Y.-C.; Hung, C.-C.; Wang, J.-C. Properties of Osteoconductive Biomaterials: Calcium Phosphate Cement with Different Ratios of Platelet-Rich Plasma as Identifiers. Mater. Sci. Eng. C 2013, 33, 3537–3544. [Google Scholar] [CrossRef]
- Mellier, C.; Lefèvre, F.-X.; Fayon, F.; Montouillout, V.; Despas, C.; Le Ferrec, M.; Boukhechba, F.; Walcarius, A.; Janvier, P.; Dutilleul, M.; et al. A Straightforward Approach to Enhance the Textural, Mechanical and Biological Properties of Injectable Calcium Phosphate Apatitic Cements (CPCs): CPC/Blood Composites, a Comprehensive Study. Acta Biomater. 2017, 62, 328–339. [Google Scholar] [CrossRef]
- Bujoli, B.; Scimeca, J.-C.; Verron, E. Fibrin as a Multipurpose Physiological Platform for Bone Tissue Engineering and Targeted Delivery of Bioactive Compounds. Pharmaceutics 2019, 11, 556. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, H.; Pascal-Moussellard, H.; Lesoeur, J.; Schnitzler, V.; Fellah, B.H.; Wagner, N.M.S.; Mellier, C.; Bouler, J.-M.; Bujoli, B.; Gauthier, O. Injection of Calcium Phosphate Apatitic Cement/Blood Composites in Intervertebral Fusion Cages: A Simple and Efficient Alternative to Autograft Leading to Enhanced Spine Fusion. Spine 2020, 45, 1288–1295. [Google Scholar] [CrossRef]
- Key Features of Dragonfly. Available online: https://www.Theobjects.Com/Dragonfly/Features.html (accessed on 23 February 2023).
- Verron, E.; Gauthier, O.; Janvier, P.; Pilet, P.; Lesoeur, J.; Bujoli, B.; Guicheux, J.; Bouler, J.-M. In Vivo Bone Augmentation in an Osteoporotic Environment Using Bisphosphonate-Loaded Calcium Deficient Apatite. Biomaterials 2010, 31, 7776–7784. [Google Scholar] [CrossRef]
- ASTM Standard C266-20; Standard Test Method for Time of Setting of Hydraulic-Cement Paste by Gillmore Needles. ASTM International: West Conshohocken, PA, USA, 2021.
- Driessens, F.C.M.; Planell, J.A.; Boltong, M.G.; Khairoun, I.; Ginebra, M.P. Osteotransductive Bone Cements. Proc. Inst. Mech. Eng. Part H 1998, 212, 427–435. [Google Scholar] [CrossRef]
- Despas, C.; Schnitzler, V.; Janvier, P.; Fayon, F.; Massiot, D.; Bouler, J.-M.; Bujoli, B.; Walcarius, A. High-Frequency Impedance Measurement as a Relevant Tool for Monitoring the Apatitic Cement Setting Reaction. Acta Biomater. 2014, 10, 940–950. [Google Scholar] [CrossRef]
- Wilson, A.J.; Murphy, W.A.; Hardy, D.C.; Totty, W.G. Transient Osteoporosis: Transient Bone Marrow Edema? Radiology 1988, 167, 757–760. [Google Scholar] [CrossRef]
- Perry, T.A.; Parkes, M.J.; Hodgson, R.J.; Felson, D.T.; Arden, N.K.; O’Neill, T.W. Association between Bone Marrow Lesions & Synovitis and Symptoms in Symptomatic Knee Osteoarthritis. Osteoarthr. Cartil. 2020, 28, 316–323. [Google Scholar]
- Felson, D.T.; Parkes, M.J.; Marjanovic, E.J.; Callaghan, M.; Gait, A.; Cootes, T.; Lunt, M.; Oldham, J.; Hutchinson, C.E. Bone Marrow Lesions in Knee Osteoarthritis Change in 6–12 Weeks. Osteoarthr. Cartil. 2012, 20, 1514–1518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Compagnoni, R.; Lesman, J.; Ferrua, P.; Menon, A.; Minoli, C.; Gallazzi, M.; Domżalski, M.; Randelli, P. Validation of a New Topographic Classification of Bone Marrow Lesions in the Knee: The Six-Letter System. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Bonadio, M.B.; Ormond Filho, A.G.; Helito, C.P.; Stump, X.M.; Demange, M.K. Bone Marrow Lesion: Image, Clinical Presentation, and Treatment. Magn. Reson. Insights 2017, 10, 1178623X17703382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alliston, T.; Hernandez, C.J.; Findlay, D.M.; Felson, D.T.; Kennedy, O.D. Bone Marrow Lesions in Osteoarthritis: What Lies beneath. J. Orthop. Res. 2018, 36, 1818–1825. [Google Scholar] [CrossRef]
- Gobbi, A.; Karnatzikos, G.; Kumar, A. Long-Term Results after Microfracture Treatment for Full-Thickness Knee Chondral Lesions in Athletes. Knee Surg. Sport. Traumatol. Arthrosc. 2014, 22, 1986–1996. [Google Scholar] [CrossRef]
- Meier, C.; Kraenzlin, C.; Friederich, N.F.; Wischer, T.; Grize, L.; Meier, C.R.; Kraenzlin, M.E. Effect of Ibandronate on Spontaneous Osteonecrosis of the Knee: A Randomized, Double-Blind, Placebo-Controlled Trial. Osteoporos. Int. 2014, 25, 359–366. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Kramer, J.; Breitenseher, M.J.; Norden, C.; Vakil-Adli, A.; Hofmann, S.; Meizer, R.; Siedentop, H.; Landsiedl, F.; Aigner, N. Short-Term Outcome of Painful Bone Marrow Oedema of the Knee Following Oral Treatment with Iloprost or Tramadol: Results of an Exploratory Phase II Study of 41 Patients. Rheumatology 2007, 46, 1460–1465. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Sharkey, P. Subchondroplasty for Treating Bone Marrow Lesions. J. Knee Surg. 2015, 29, 555–563. [Google Scholar]
- Sánchez, M.; Delgado, D.; Pompei, O.; Pérez, J.C.; Sánchez, P.; Garate, A.; Bilbao, A.M.; Fiz, N.; Padilla, S. Treating Severe Knee Osteoarthritis with Combination of Intra-Osseous and Intra-Articular Infiltrations of Platelet-Rich Plasma: An Observational Study. Cartilage 2019, 10, 245–253. [Google Scholar] [CrossRef]
- Angadi, D.S.; Edwards, D.; Melton, J.T.K. Calcium Phosphate Injection of Symptomatic Bone Marrow Lesions of the Knee: What Is the Current Clinical Evidence? Knee Surg. Relat. Res. 2020, 32, 4. [Google Scholar] [CrossRef]
- Astur, D.C.; de Freitas, E.V.; Cabral, P.B.; Morais, C.C.; Pavei, B.S.; Kaleka, C.C.; Debieux, P.; Cohen, M. Evaluation and Management of Subchondral Calcium Phosphate Injection Technique to Treat Bone Marrow Lesion. Cartilage 2019, 10, 395–401. [Google Scholar] [CrossRef]
- Rebolledo, B.J.; Smith, K.M.; Dragoo, J.L. Hitting the Mark: Optimizing the Use of Calcium Phosphate Injections for the Treatment of Bone Marrow Lesions of the Proximal Tibia and Distal Femur. Arthrosc. Tech. 2018, 7, 1013–1018. [Google Scholar] [CrossRef] [Green Version]
- Hernigou, P.; Bouthors, C.; Bastard, C.; Flouzat Lachaniette, C.H.; Rouard, H.; Dubory, A. Subchondral Bone or Intra-Articular Injection of Bone Marrow Concentrate Mesenchymal Stem Cells in Bilateral Knee Osteoarthritis: What Better Postpone Knee Arthroplasty at Fifteen Years? A Randomized Study. Int. Orthop. (SICOT) 2021, 45, 391–399. [Google Scholar] [CrossRef]
- Maurel, B.; Le Corroller, T.; Bierry, G.; Buy, X.; Host, P.; Gangi, A. Treatment of Symptomatic Para-Articular Intraosseous Cysts by Percutaneous Injection of Bone Cement. Skelet. Radiol. 2013, 42, 43–48. [Google Scholar] [CrossRef]
- Bernhard, K.; Alan, N.G.; Kruse, D.; Stone, P.A. Surgical Treatment of Bone Marrow Lesion Associated with Recurrent Plantar Fasciitis: A Case Report Describing an Innovative Technique Using Subchondroplasty. J. Foot Ankle Surg. 2018, 57, 811–815. [Google Scholar] [CrossRef]
- Eriksen, E.F. Treatment of Bone Marrow Lesions (Bone Marrow Edema). BoneKey Rep. 2015, 4, 755. [Google Scholar] [CrossRef] [Green Version]
- Fokter, S.K.; Kuhta, M.; Hojnik, M.; Ledinek, Ž.; Kostanjšek, R. Tissue Integration of Calcium Phosphate Compound after Subchondroplasty: 4-Year Follow-Up in a 76-Year-Old Female Patient. Bioengineering 2023, 10, 208. [Google Scholar] [CrossRef]
- Eid, K.; Zelicof, S.; Perona, B.P.; Sledge, C.B.; Glowacki, J. Tissue Reactions to Particles of Bone-Substitute Materials in Intraosseous and Heterotopic Sites in Rats: Discrimination of Osteoinduction, Osteocompatibility, and Inflammation. J. Orthop. Res. 2001, 19, 962–969. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | HBS | HBS-g26 | QS |
|---|---|---|---|
| Mean size (µm) | 18.9 | 13.0 | 11.9 |
| Median (µm) | 45.3 | 53.9 | 52.1 |
| Mode (µm) | 18.7 | 5.21 | 4.58 |
| d10 (µm) | 1.65 | 0.87 | 0.88 |
| d50 (µm) | 9.86 | 5.92 | 6.17 |
| d90 (µm) | 35.3 | 31.1 | 47.7 |
| Minimal size (µm) | 0.11 | 0.11 | 0.11 |
| Maximal size (µm) | 272 | 272 | 111 |
| Studied Conditions | Dielectric Permittivity (ε′) | Dielectric Losses (ε″) | ||
|---|---|---|---|---|
| ti (min) | tf (min) | ti (min) | tf (min) | |
| HBS | 23 | 47 | 19 | 45 |
| HBS + human citrated blood | 620 | 740 | 610 | 790 |
| HBS + human heparinized blood | 450 | 583 | 450 | 670 |
| HBS + ovine citrated blood | 890 | 1050 | 860 | 1100 |
| HBS + ovine heparinized blood | 440 | 575 | 460 | 665 |
| HBS-g26 | <2 | 13 | <2 | 14 |
| HBS-g26 + human citrated blood | 30 | 82 | 32 | 100 |
| HBS-g26 + human heparinized blood | 12 | 79 | 8 | 96 |
| HBS-g26 + ovine citrated blood | 30 | 88 | 32 | 113 |
| HBS-g26 + ovine heparinized blood | 33 | 99 | 34 | 123 |
| Hardening Time at 37 °C (h) | HBS + Blood | Hardening Time at 37 °C (h) | HBS-g26 + Blood | ||
|---|---|---|---|---|---|
| Clotting | Pictures | Clotting | Pictures | ||
| 12 h | No |  | 18 h | In progress |  |
| 24 h | No |  | 24 h | Yes |  |
| 48 h | In progress |  | 32 h | Yes |  |
| 72 h | In progress |  | 40 h | Yes |  |
| 108 h | Yes |  | 56 h | Yes |  |
| 144 h | Yes |  | 72 h | Yes |  |
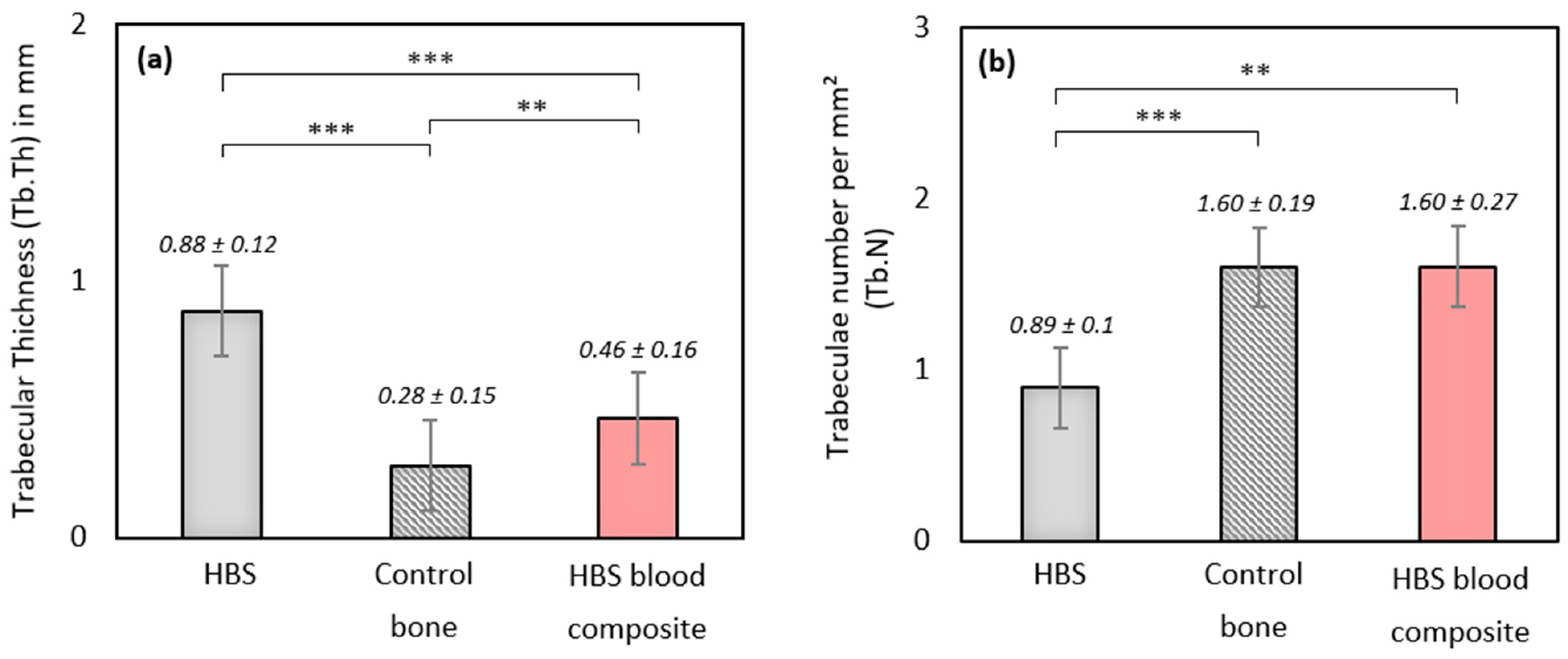
| Formulations | BV/TV (%) | Trabecular Thickness (Tb.Th, mm) | Trabeculae Number per mm² (Tb.N) | Trabecular Separation (Tb.Sp, mm) |
|---|---|---|---|---|
| HBS | 75.43 ± 7.91 | 0.88 ± 0.12 | 0.89 ± 0.10 | 0.51 ± 0.41 |
| HBS blood composite | 68.31 ± 11.98 | 0.46 ± 0.16 | 1.60 ± 0.27 | 0.34 ± 0.10 |
| Control bone | 45.26 ± 9.93 | 0.28 ± 0.15 | 1.60 ± 0.19 | 0.44 ± 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limelette, M.; De Fourmestraux, C.; Despas, C.; Lafragette, A.; Veziers, J.; Le Guennec, Y.; Touzot-Jourde, G.; Lefevre, F.-X.; Verron, E.; Bouler, J.-M.; et al. Calcium Phosphate Cements Combined with Blood as a Promising Tool for the Treatment of Bone Marrow Lesions. J. Funct. Biomater. 2023, 14, 204. https://doi.org/10.3390/jfb14040204
Limelette M, De Fourmestraux C, Despas C, Lafragette A, Veziers J, Le Guennec Y, Touzot-Jourde G, Lefevre F-X, Verron E, Bouler J-M, et al. Calcium Phosphate Cements Combined with Blood as a Promising Tool for the Treatment of Bone Marrow Lesions. Journal of Functional Biomaterials. 2023; 14(4):204. https://doi.org/10.3390/jfb14040204
Chicago/Turabian StyleLimelette, Maxence, Claire De Fourmestraux, Christelle Despas, Audrey Lafragette, Joelle Veziers, Yohan Le Guennec, Gwenola Touzot-Jourde, François-Xavier Lefevre, Elise Verron, Jean-Michel Bouler, and et al. 2023. "Calcium Phosphate Cements Combined with Blood as a Promising Tool for the Treatment of Bone Marrow Lesions" Journal of Functional Biomaterials 14, no. 4: 204. https://doi.org/10.3390/jfb14040204