
Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive—Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Polyurethane-Based Adhesive System (PUAS)
2.2. Fibrin- and Thrombin-Based Adhesive System (FTAS)
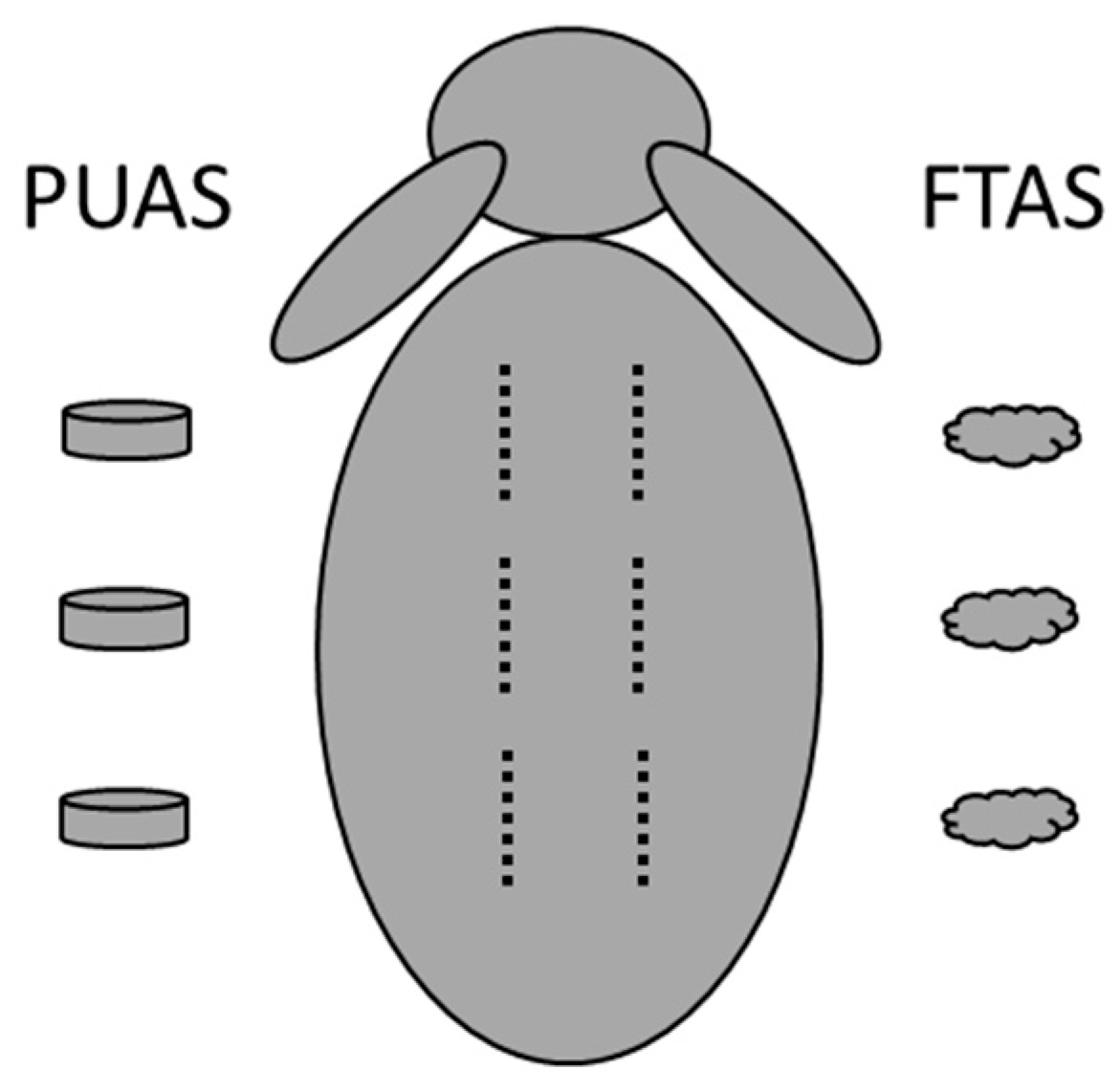
2.3. Preparation of Implants
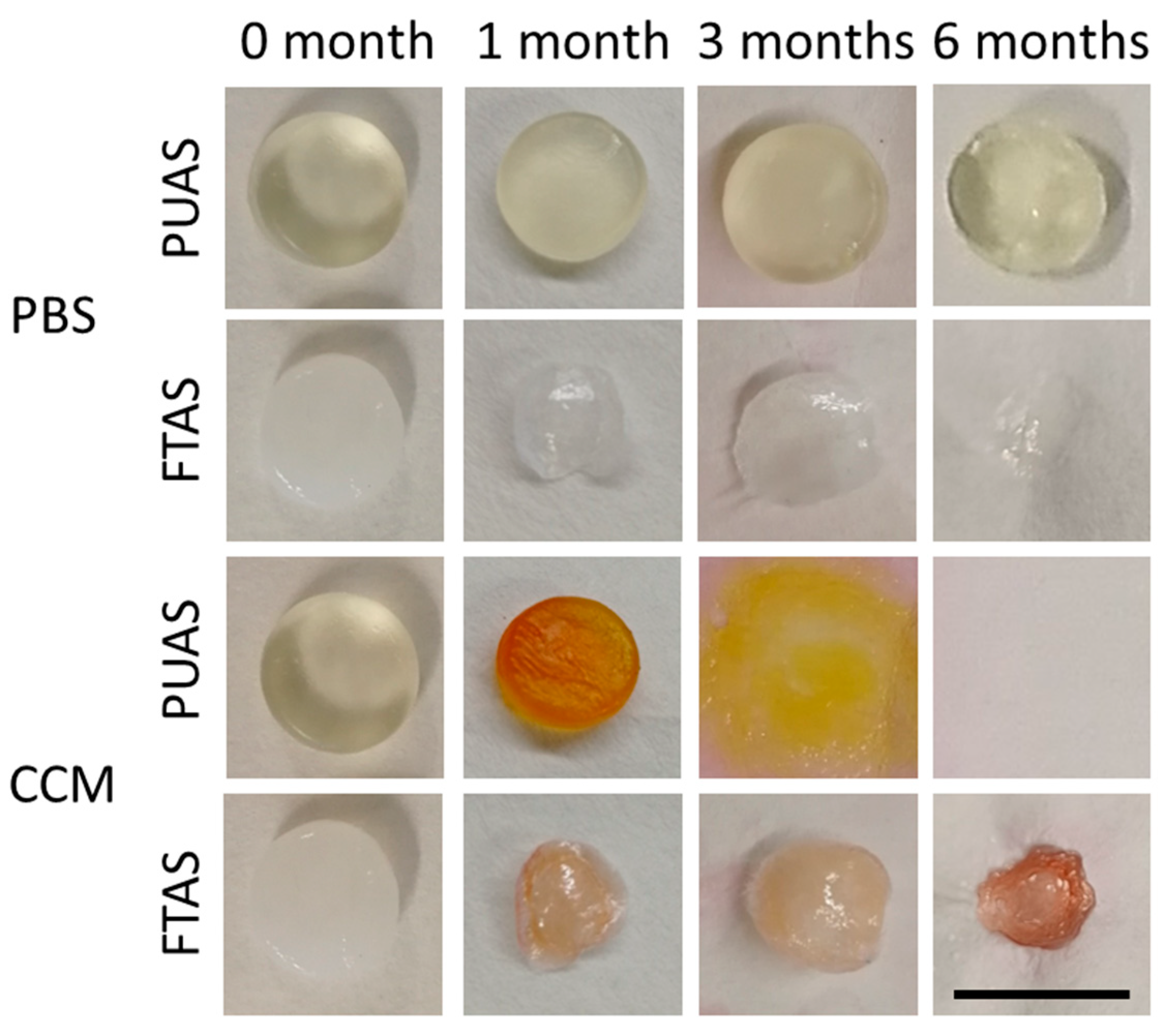
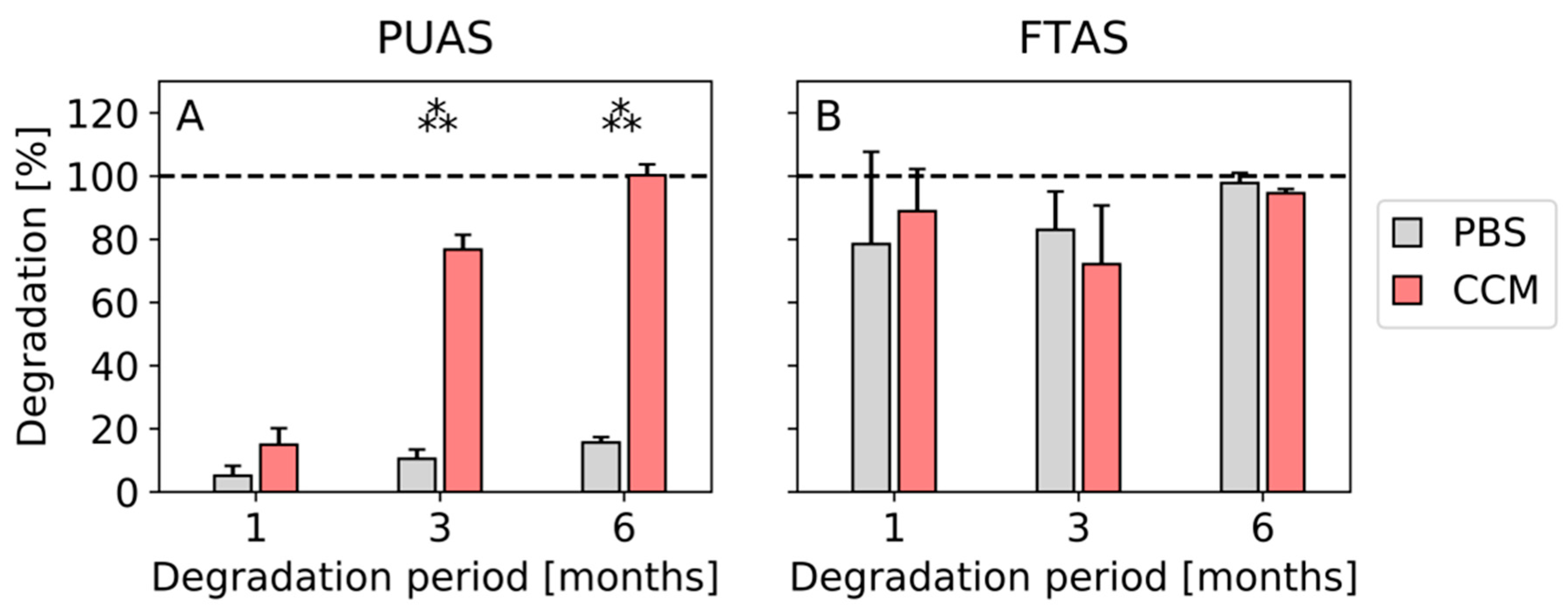
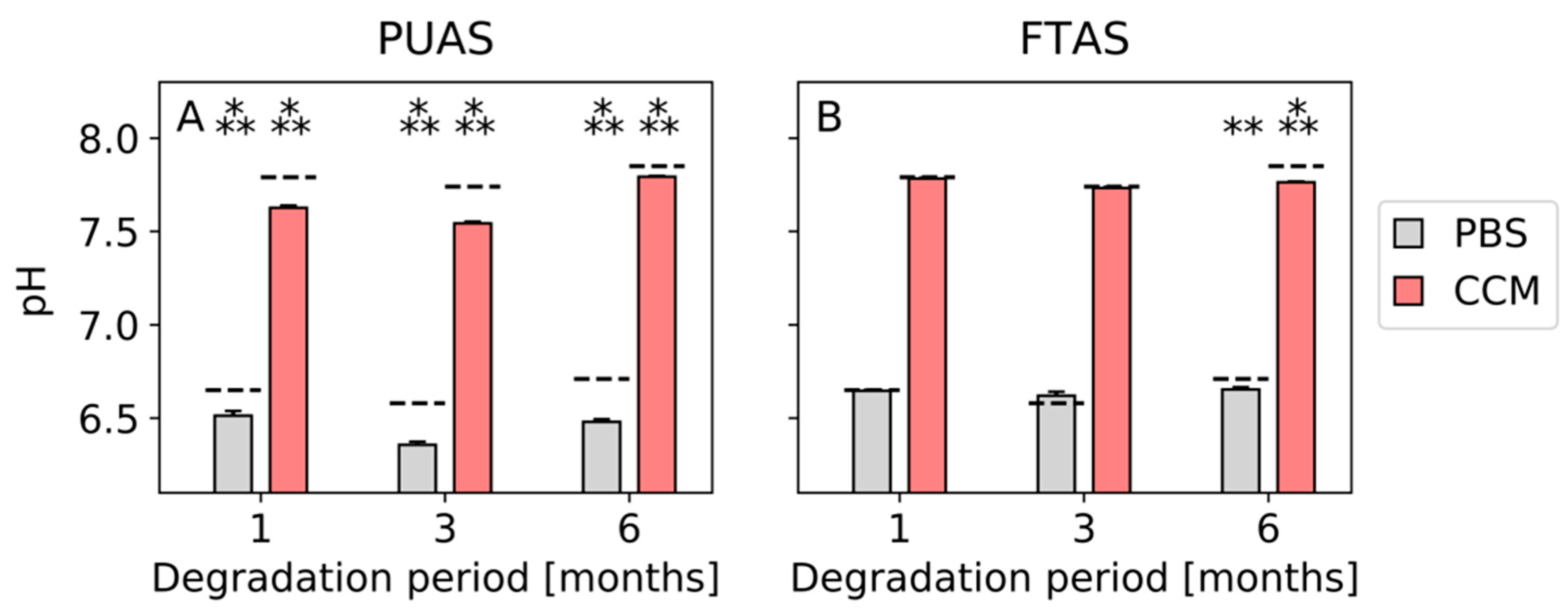
2.4. In Vitro Degradation
2.5. In Vivo Degradation
3. Statistics
4. Results
4.1. In Vitro Testing
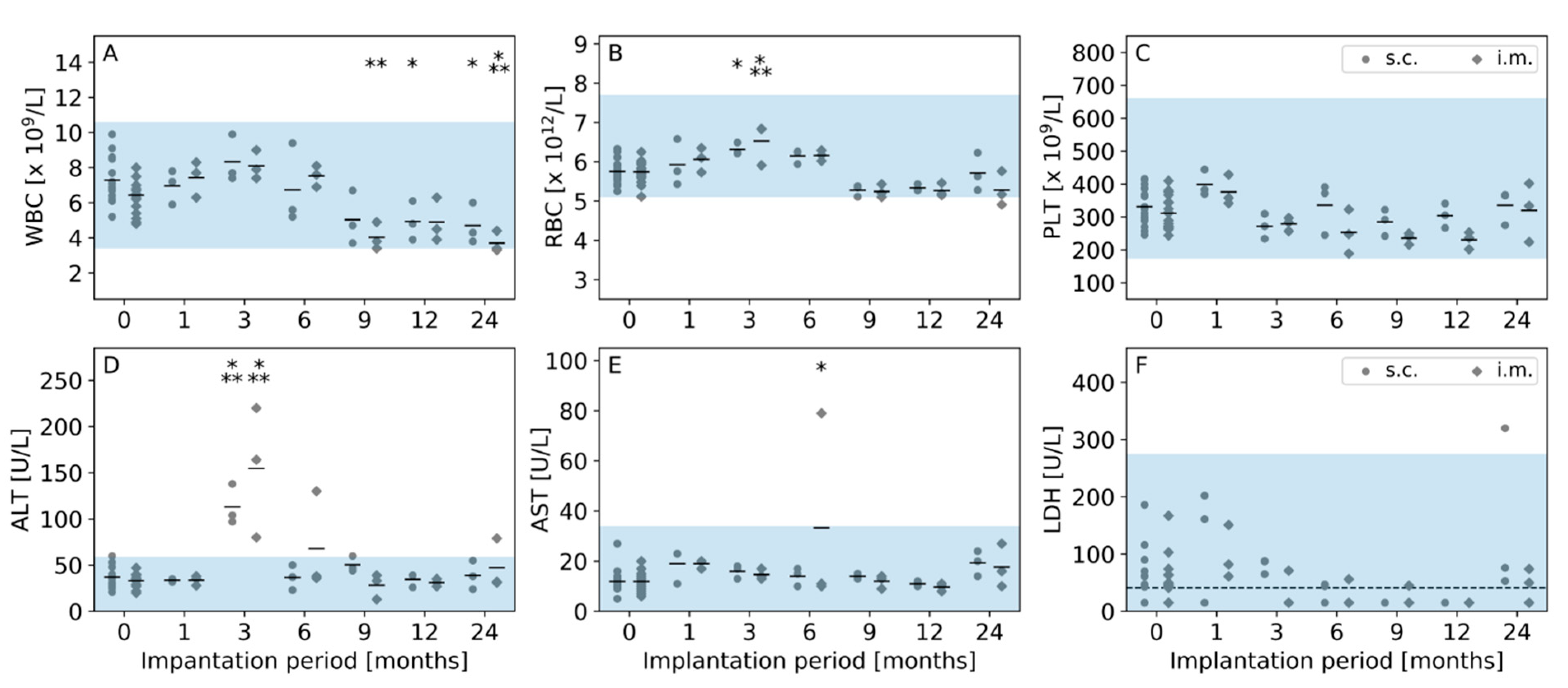
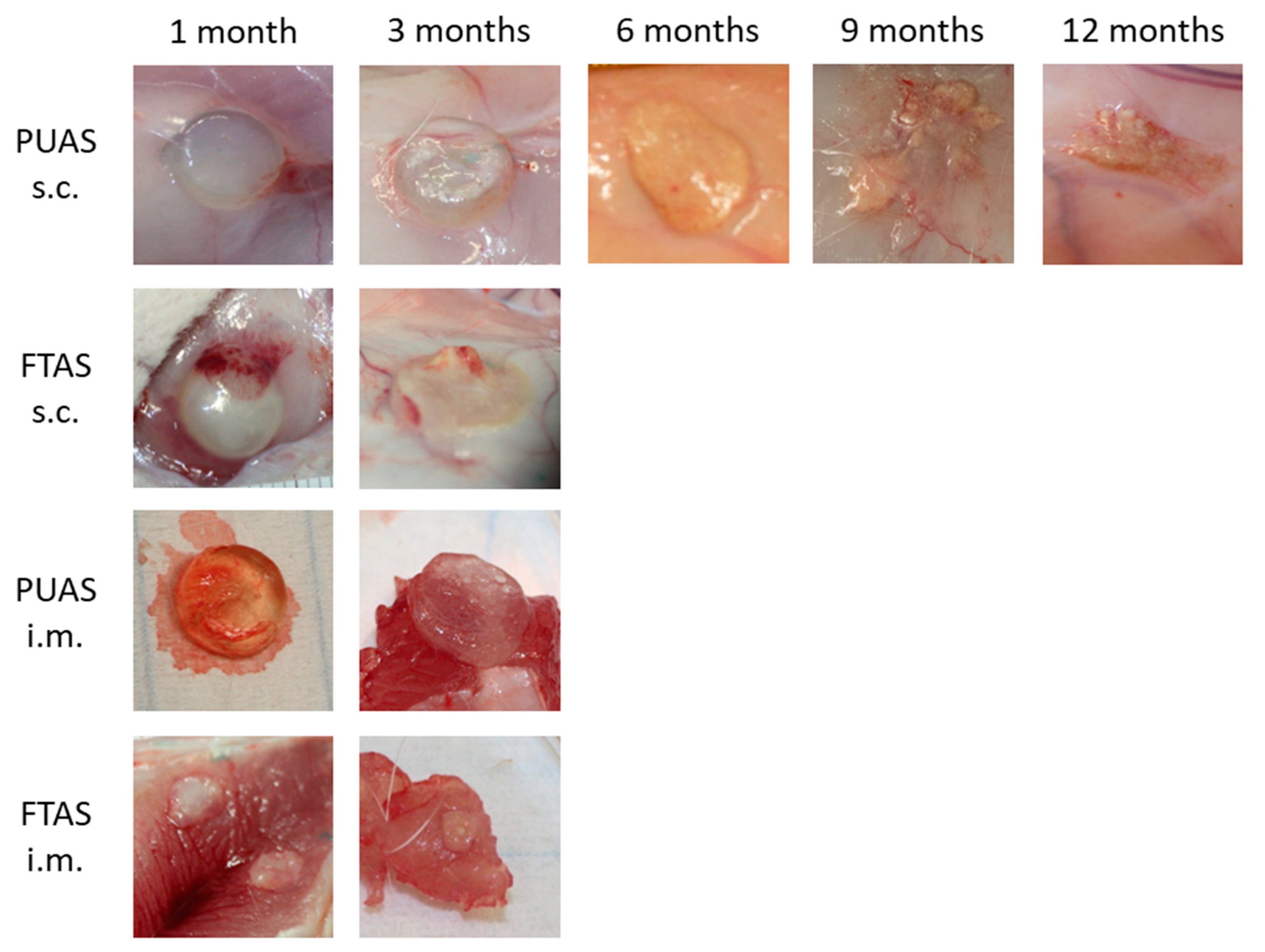
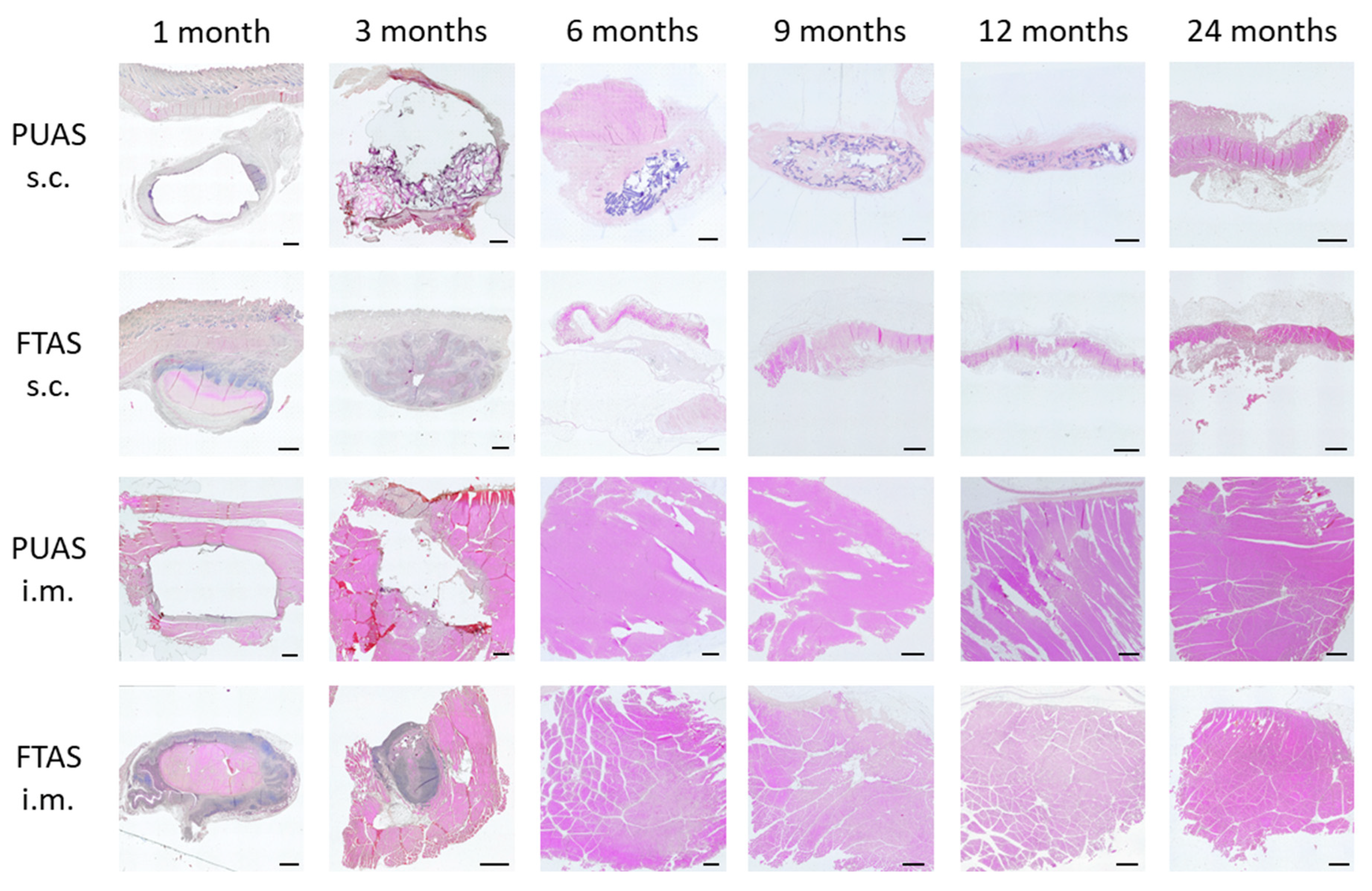
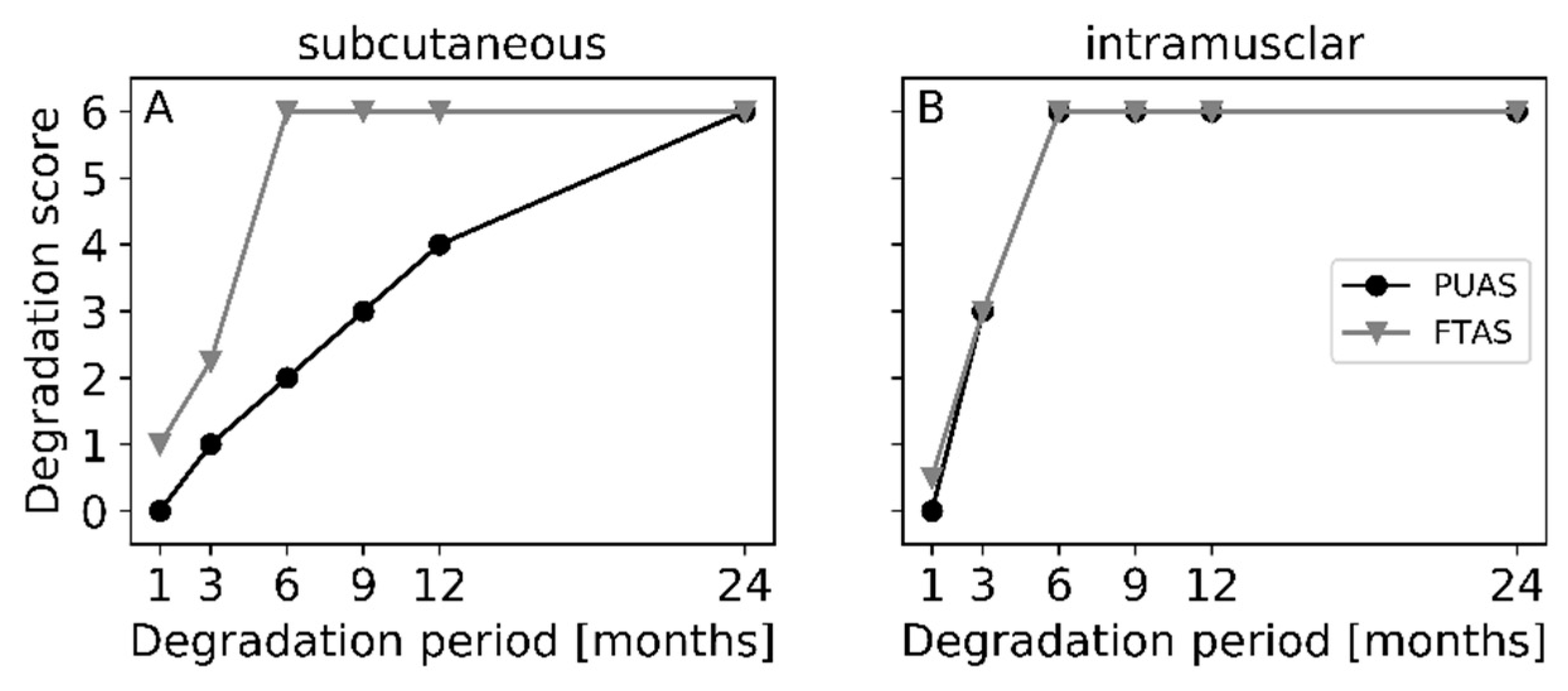
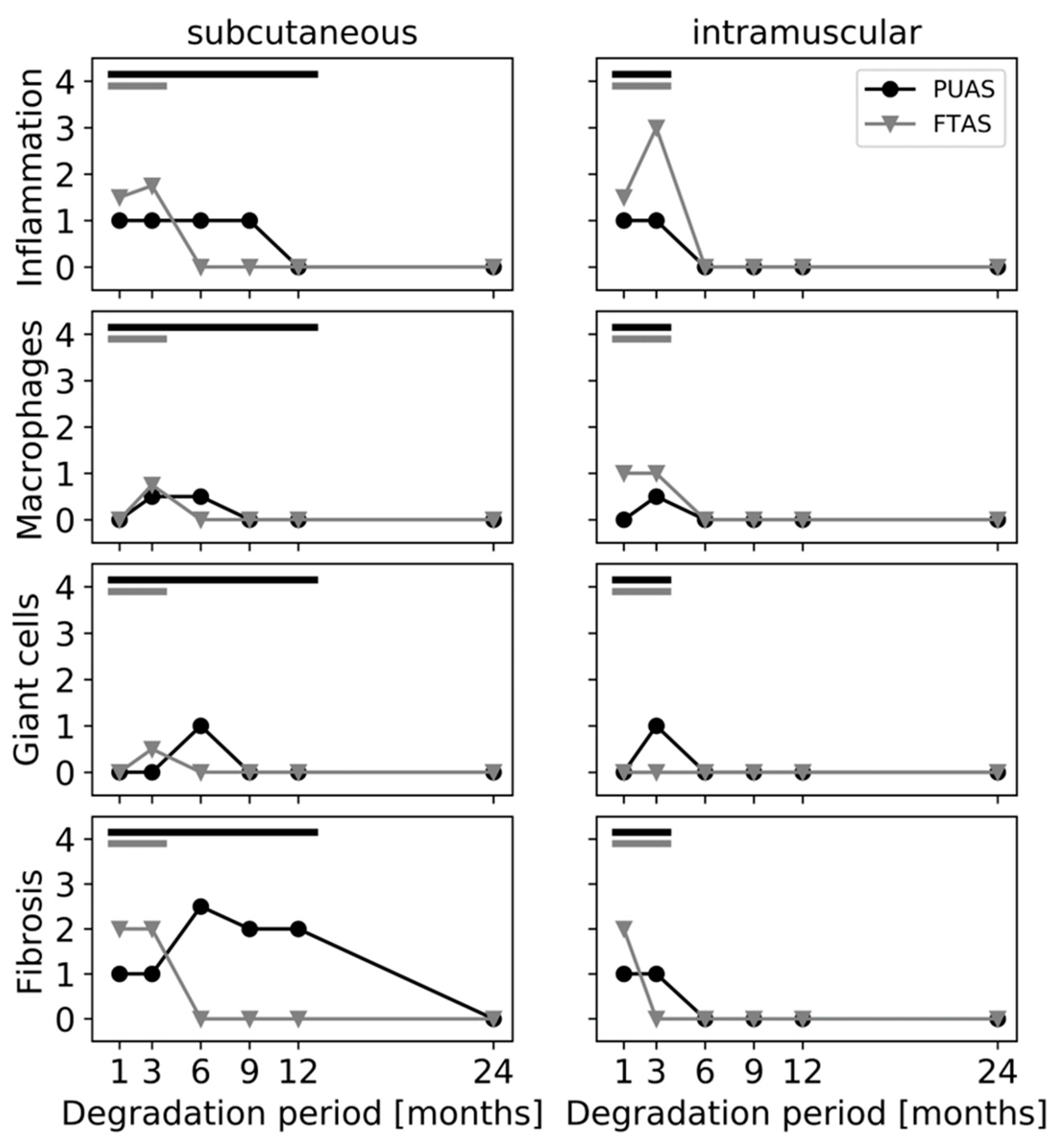
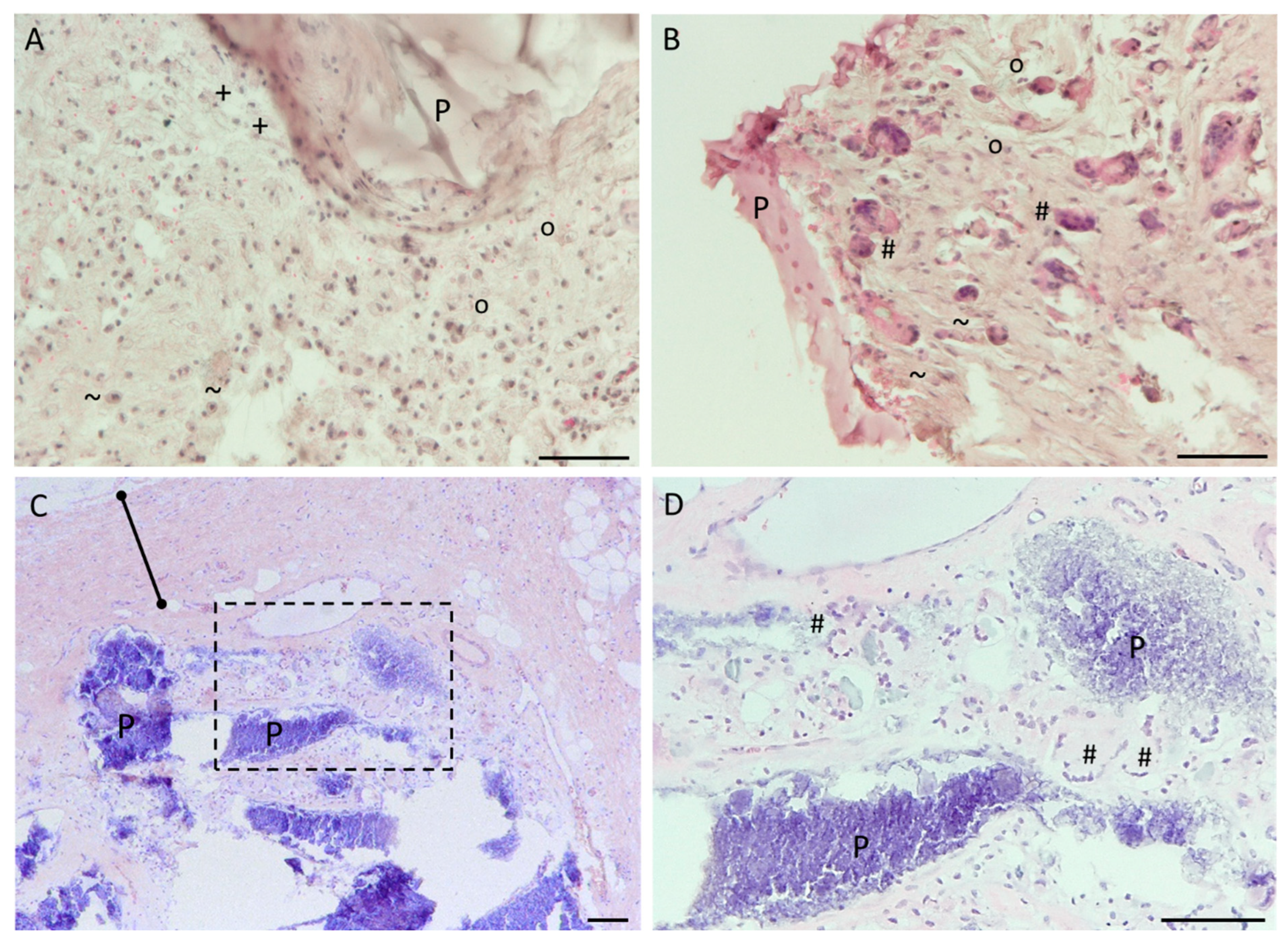
4.2. In Vivo Testing
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Scognamiglio, F.; Travan, A.; Rustighi, I.; Tarchi, P.; Palmisano, S.; Marsich, E.; Borgogna, M.; Donati, I.; de Manzini, N.; Paoletti, S. Adhesive and sealant interfaces for general surgery applications. J. Biomed. Mater. Res. B. Appl. Biomater. 2016, 104, 626–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhagat, V.; Becker, M.L. Degradable Adhesives for Surgery and Tissue Engineering. Biomacromolecules 2017, 18, 3009–3039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauto, A.; Mawad, D.; Foster, L.J.R. Adhesive biomaterials for tissue reconstruction. J. Chem. Technol. Biotechnol. 2008, 83, 464–472. [Google Scholar] [CrossRef]
- Sanders, L.; Nagatomi, J. Clinical applications of surgical adhesives and sealants. Crit. Rev. Biomed. Eng. 2014, 42, 271–292. [Google Scholar] [CrossRef]
- Taboada, G.M.; Yang, K.; Pereira, M.J.N.; Liu, S.S.; Hu, Y.; Karp, J.M.; Artzi, N.; Lee, Y. Overcoming the translational barriers of tissue adhesives. Nat. Rev. Mater. 2020, 5, 310–329. [Google Scholar] [CrossRef]
- Duarte, A.P.; Coelho, J.F.; Bordado, J.C.; Cidade, M.T.; Gil, M.H. Surgical adhesives: Systematic review of the main types and development forecast. Progress. Polym. Sci. 2012, 37, 1031–1050. [Google Scholar] [CrossRef]
- Schulten, L.; Spillner, J.; Kanzler, S.; Teubner, A.; Jockenhoevel, S.; Apel, C. A polyurethane-based surgical adhesive for sealing blood vessel anastomoses-A feasibility study in pigs. J. Biomed. Mater. Res. B. Appl. Biomater. 2022, 110, 1922–1931. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, M.; Brockhaus, J.; Kniha, K.; Merkord, F.; Peters, F.; Holzle, F.; Goloborodko, E.; Modabber, A. Mechanical strength and hydrostatic testing of VIVO adhesive in sutureless microsurgical anastomoses: An ex vivo study. Sci. Rep. 2021, 11, 13598. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, M.; Mohlhenrich, S.C.; Kniha, K.; Tolba, R.; Jockenhoevel, S.; Holzle, F.; Modabber, A. Microvascular anastomosis techniques using the medical adhesive VIVO and expandable micro-stents in a rat carotid artery model. Ann. Anat. 2021, 238, 151782. [Google Scholar] [CrossRef]
- Kalverkamp, S.; Mantas, A.; Spillner, J.; Hima, F.; Kanzler, S.S.; Stopinski, T.; Tolba, R.H.; Zayat, R. Efficacy of a Novel Medical Adhesive for Sealing Lung Parenchyma: An in vitro Study in Rabbit Lungs. Eur. Surg. Res. 2021, 62, 255–261. [Google Scholar] [CrossRef]
- Tanaka, H.; Fukushima, K.; Srinivasan, P.K.; Pawlowsky, K.; Koegel, B.; Hata, K.; Ku, Y.; Uemoto, S.; Tolba, R.H. Efficacy of the Novel Medical Adhesive, MAR-VIVO-107, in an Acute Porcine Liver Resection Model. Surg. Innov. 2017, 24, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K.; Tanaka, H.; Srinivasan, P.K.; Pawlowsky, K.; Kogel, B.; Uemoto, S.; Ku, Y.; Tolba, R.H. Hemostatic Efficacy and Safety of the Novel Medical Adhesive, MAR VIVO-107, in a Rabbit Liver Resection Model. Eur. Surg. Res. 2018, 59, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, P.K.; Sperber, V.; Afify, M.; Tanaka, H.; Fukushima, K.; Kogel, B.; Gremse, F.; Tolba, R. Novel synthetic adhesive as an effective alternative to Fibrin based adhesives. World J. Hepatol. 2017, 9, 1030–1039. [Google Scholar] [CrossRef]
- Hagemeister, K.; Ernst, L.; Srinivasan, P.K.; Tanaka, H.; Fukushima, K.; Tolba, R. Severity assessment in pigs after partial liver resection: Evaluation of a score sheet. Lab. Anim. 2020, 54, 251–260. [Google Scholar] [CrossRef]
- Heise, D.; Mirlas, Y.; Helmedag, M.; Eickhoff, R.; Kroh, A.; Lambertz, A.; Klink, C.D.; Neumann, U.P.; Klinge, U.; Tolba, R. Two Polyurethane Adhesives for PVDF Fixation Show Superior Biocompatibility in a Rat Model. J. Invest. Surg. 2022, 35, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Patel, R.M.; Wenham, A.; Smith, J.R. Biomedical applications of polyurethane materials and coatings. Trans. IMF 2018, 96, 121–129. [Google Scholar] [CrossRef] [Green Version]
- van Minnen, B.; Stegenga, B.; van Leeuwen, M.B.; van Kooten, T.G.; Bos, R.R. A long-term in vitro biocompatibility study of a biodegradable polyurethane and its degradation products. J. Biomed. Mater. Res. A 2006, 76, 377–385. [Google Scholar] [CrossRef]
- Wendels, S.; Averous, L. Biobased polyurethanes for biomedical applications. Bioact. Mater. 2021, 6, 1083–1106. [Google Scholar] [CrossRef]
- McBane, J.E.; Sharifpoor, S.; Cai, K.; Labow, R.S.; Santerre, J.P. Biodegradation and in vivo biocompatibility of a degradable, polar/hydrophobic/ionic polyurethane for tissue engineering applications. Biomaterials 2011, 32, 6034–6044. [Google Scholar] [CrossRef]
- Heckroth, H.; Eggert, C.; Hofmann, J.; Lorenz, K. Isocyanate-Functional Prepolymer for Biologically Degradable Adhesives. Patent WO2013092504A1, 27 June 2013. [Google Scholar]
- Baxter. TISSEEL Package Insert; Baxter Healthcare Corporation: Deerfield, IL, USA, 2019. [Google Scholar]
- Cauich-Rodríguez, J.V.; Chan-Chan, L.H.; Hernandez-Sánchez, F.; Cervantes-Uc, J.M. Advances in Biomaterials Science and Biomedical Applications, 1st ed.; Pignatello, R., Ed.; Chapter 3 Degradation of Polyurethanes for Cardiovascular Applications; IntechOpen: London, UK, 2013. [Google Scholar]
- Baxter. TISSEEL Thrombin Solution Safety Data Sheet; Baxter Healthcare Corporation: Deerfield, IL, USA, 2020. [Google Scholar]
- Baxter. TISSEEL Sealer Protein Solution Safety Data Sheet; Baxter Healthcare Corporation: Deerfield, IL, USA, 2021. [Google Scholar]
- Broekema, F.I.; Van Leeuwen, M.B.; Van Minnen, B.; Bos, R.R. In vivo degradation of polyurethane foam with 55 wt % polyethylene glycol. J. Biomed. Mater. Res. A 2015, 103, 3666–3675. [Google Scholar] [CrossRef]
- New Zealand White Rabbit Data Sheet. Available online: https://www.criver.com/sites/default/files/resource-files/RM-NZW-rabbit-information-sheet.pdf (accessed on 3 June 2022).
- Bal-Ozturk, A.; Cecen, B.; Avci-Adali, M.; Topkaya, S.N.; Alarcin, E.; Yasayan, G.; Ethan, Y.C.; Bulkurcuoglu, B.; Akpek, A.; Avci, H.; et al. Tissue Adhesives: From Research to Clinical Translation. Nano Today 2021, 36, 101049. [Google Scholar] [CrossRef] [PubMed]
- Santerre, J.P.; Woodhouse, K.; Laroche, G.; Labow, R.S. Understanding the biodegradation of polyurethanes: From classical implants to tissue engineering materials. Biomaterials 2005, 26, 7457–7470. [Google Scholar] [CrossRef]
- Dezfuli, S.N.; Huan, Z.; Mol, J.M.C.; Leeflang, M.A.; Chang, J.; Zhou, J. Influence of HEPES buffer on the local pH and formation of surface layer during in vitro degradation tests of magnesium in DMEM. Progress. Nat. Sci. Mater. Int. 2014, 24, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Frazao, L.P.; de Castro, J.V.; Neves, N.M. In Vivo Evaluation of the Biocompatibility of Biomaterial Device. Adv. Exp. Med. Biol. 2020, 1250, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.; Sreenivasan, K.; Mohanan, P.; Kumary, T.; Mohanty, M. Polyurethane Degradation in the Biological Milieu. Trends Biomater. Artif. Organs 2006, 19, 115–121. [Google Scholar]
- Klopfleisch, R.; Jung, F. The pathology of the foreign body reaction against biomaterials. J. Biomed. Mater. Res. A 2017, 105, 927–940. [Google Scholar] [CrossRef] [PubMed]
- Xia, Z.; Triffitt, J.T. A review on macrophage responses to biomaterials. Biomed. Mater. 2006, 1, R1–R9. [Google Scholar] [CrossRef]
- Sheikh, Z.; Brooks, P.J.; Barzilay, O.; Fine, N.; Glogauer, M. Macrophages, Foreign Body Giant Cells and Their Response to Implantable Biomaterials. Materials 2015, 8, 5671–5701. [Google Scholar] [CrossRef] [Green Version]
- Middleton, J.C.; Tipton, A.J. Synthetic biodegradable polymers as orthopedic devices. Biomaterials 2000, 21, 2335–2346. [Google Scholar] [CrossRef]
- Bhatia, S.; Shalaby, S.W.; Powers, D.L.; Lancaster, R.L.; Ferguson, R.L. The effect of site of implantation and animal age on properties of polydioxanone pins. J. Biomater. Sci. Polym. Ed. 1994, 6, 435–446. [Google Scholar] [CrossRef]
- Kim, K.; Jeong, C.G.; Hollister, S.J. Non-invasive monitoring of tissue scaffold degradation using ultrasound elasticity imaging. Acta Biomater. 2008, 4, 783–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Degradation Period (Months) | Number of Animals | |
|---|---|---|
| i.m. Location | s.c. Location | |
| 1 | 3 | 3 |
| 3 | 3 | 3 |
| 6 | 3 | 3 |
| 9 | 3 | 3 |
| 12 | 3 | 3 |
| 24 | 3 | 3 |
| Score | Observations during Microscopy |
|---|---|
| 0 | signs of degradation at the border of the material |
| 1 | degradation in one half of the material |
| 2 | degradation in the center of the material |
| 3 | fragmentation of the original implant structure |
| 4 | intracellular remnants of material |
| 5 | no visible material but signs of cellular activity indicative of degradation |
| 6 | no visible material and no signs of cellular activity indicative of degradation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bremer, L.; Hagemeister, K.; Moss, M.; Ernst, L.; Tolba, R.H.; Jockenhoevel, S.; Apel, C. Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive—Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing. J. Funct. Biomater. 2023, 14, 168. https://doi.org/10.3390/jfb14030168
Bremer L, Hagemeister K, Moss M, Ernst L, Tolba RH, Jockenhoevel S, Apel C. Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive—Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing. Journal of Functional Biomaterials. 2023; 14(3):168. https://doi.org/10.3390/jfb14030168
Chicago/Turabian StyleBremer, Lisanne, Kerstin Hagemeister, Michaela Moss, Lisa Ernst, René H. Tolba, Stefan Jockenhoevel, and Christian Apel. 2023. "Long-Term Degradation Assessment of a Polyurethane-Based Surgical Adhesive—Assessment and Critical Consideration of Preclinical In Vitro and In Vivo Testing" Journal of Functional Biomaterials 14, no. 3: 168. https://doi.org/10.3390/jfb14030168