
Reconstructive Peri-Implantitis Therapy by Using Bovine Bone Substitute with or without Hyaluronic Acid: A Randomized Clinical Controlled Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
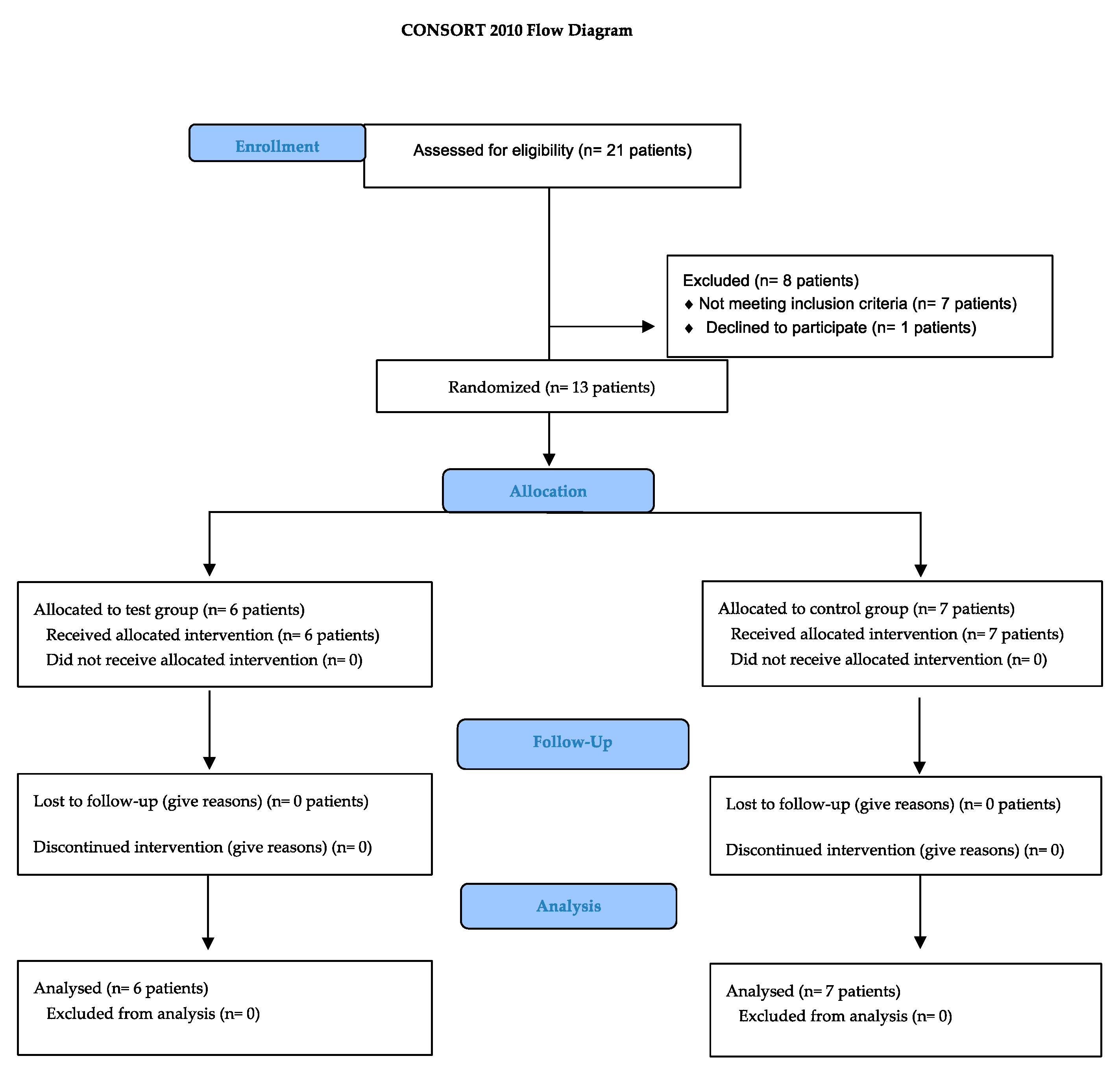
2.1. Study Design and Participants
- Minimum 18-year-old;
- Able to understand the information about the protocol of the study and to sign the inform consent before the treatment;
- Systematically healthy or with mild or moderate well-controlled systemic conditions or diseases including cardiovascular diseases (i.e., patients with hypertension and arrhythmia);
- No previous surgical peri-implantits treatment;
- Able to maintain adequate oral hygiene (O’Leary plaque index score <25%) [37];
- Presence of at least one implant (bone- or tissue- level) with peri-implantitis defined as: radiography bone loss >2 mm with BOP positive sign (+) at least one side around the implant and PPD >5 mm (mm); In the cases with absence of the previous radiogram, the peri-implantitis was defined in accordance to 2017 World Workshop Consensus (BOP +, PPD ≥6 mm and MB loss ≥3 mm) [3].
- Patients who did not receive antibiotic therapy within last 2 months;
- Non-smokers or light smokers (<10 cigarettes/day).
2.2. Study Protocol
2.2.1. Pre-Surgical Treatment (T0)
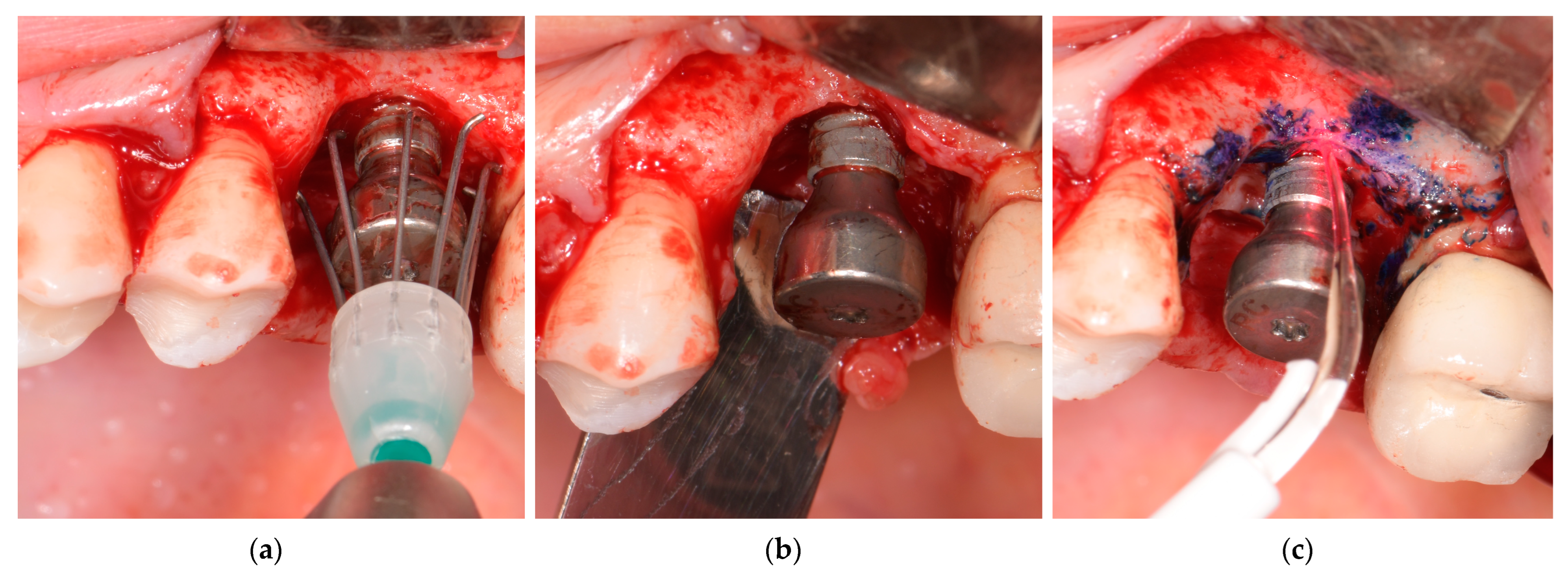
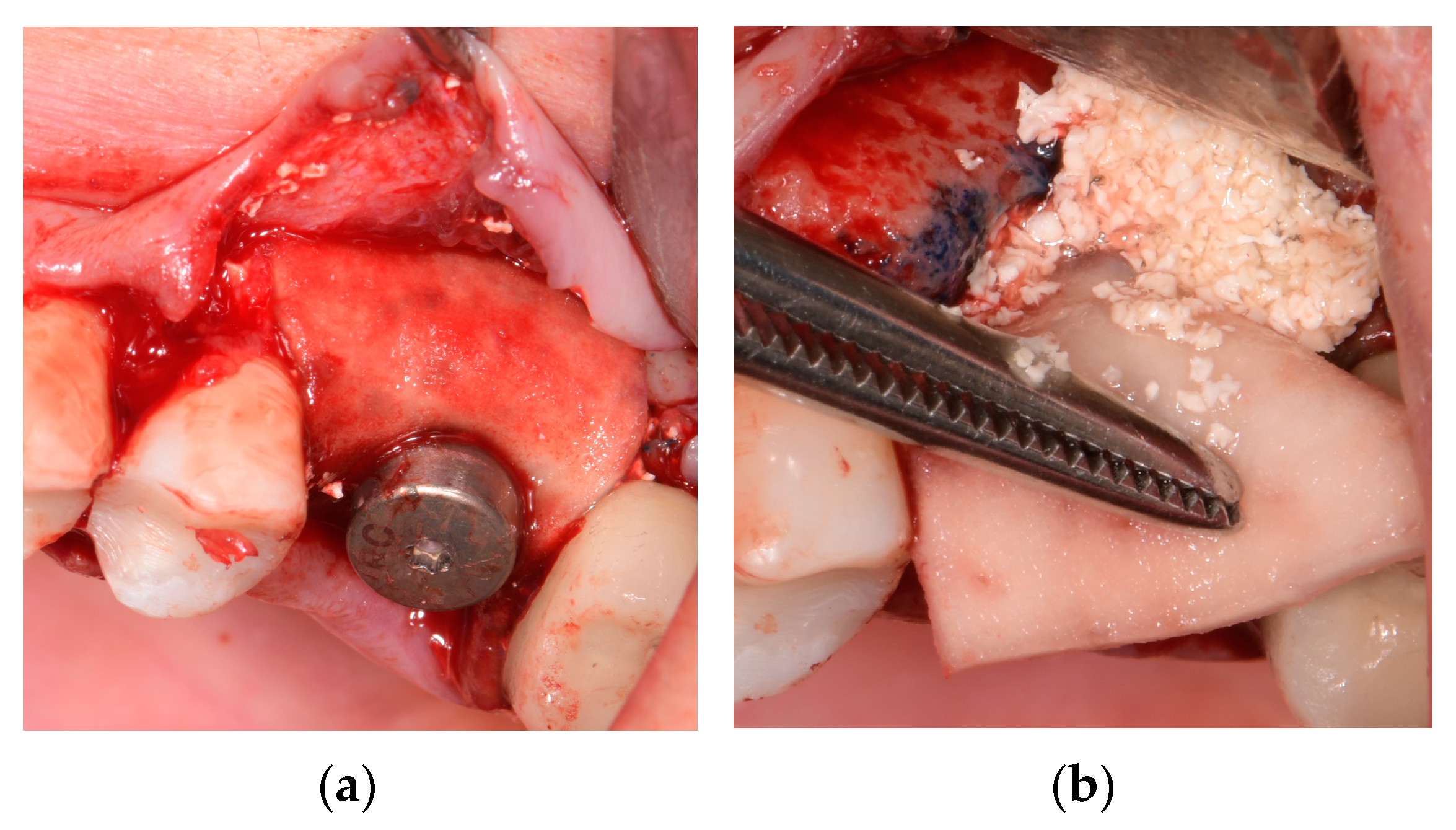
2.2.2. Surgical Regenerative Approaches (T1) with Patients’ Randomization
2.2.3. Postoperative Instruction, Re-Calls, and Prosthetic Rehabilitation
2.3. Data Collection and Intra-Examiner Calibration
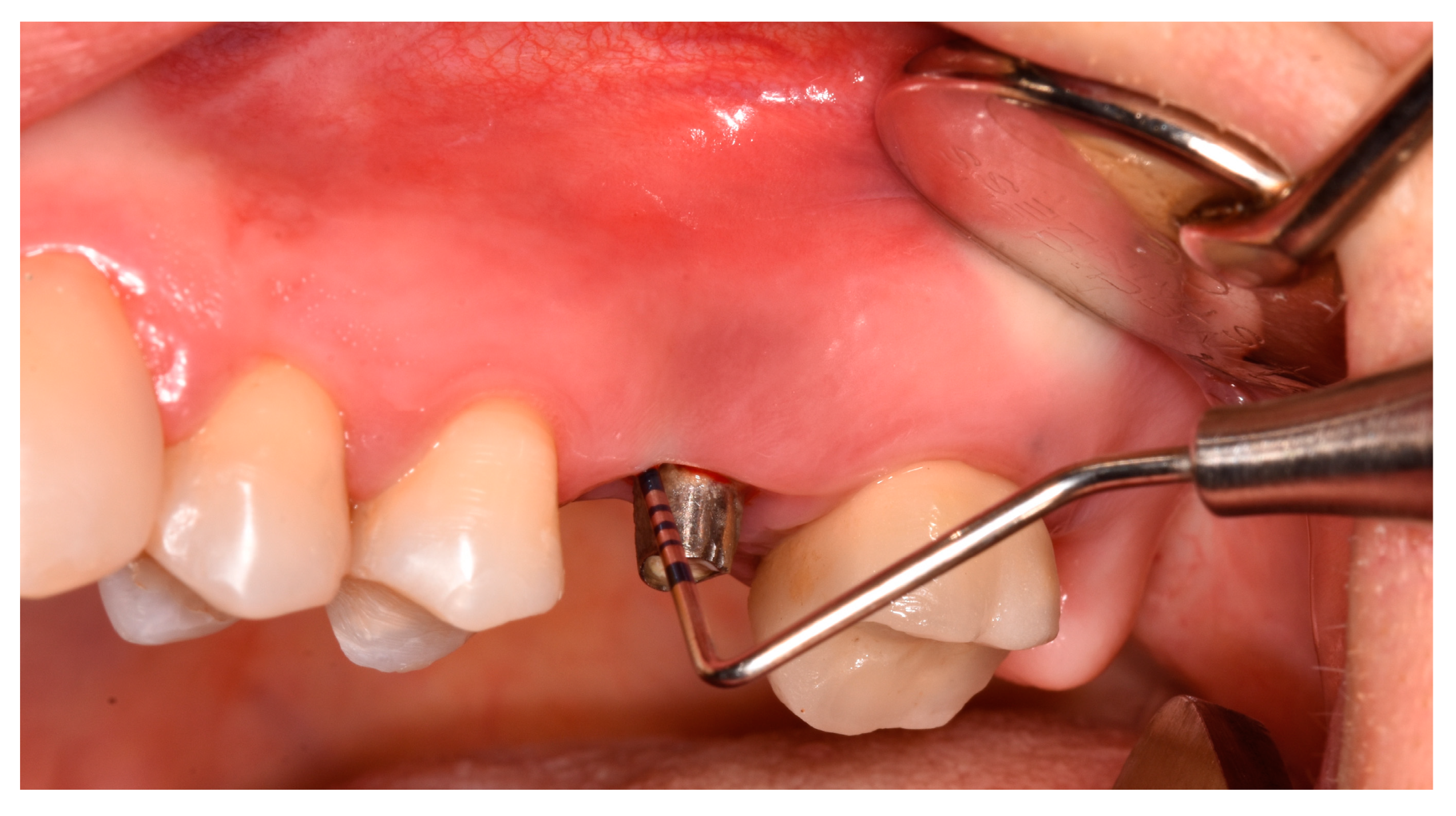
2.3.1. Clinical Examination
- Peri-implant probing depth (PPD) and clinical attachment level (CAL) were measured at the six sites (bucco-mesial, bucco-medial, bucco-distal, oro-mesial, oro-medial, and oro-distal) and recorded in millimeters (mm). PPD was determined as a distance from the mucosal margin (MM) to the depth of the probable peri-implant pocket, while CAL was obtained as distance from implant shoulder to the bottom of peri-implant pocket;
- Suppuration (SUP) on probing assessed dichotomously (+/−) after the probing;
- Keratinized mucosa width (KMW) was measured at the middle of the inserted implant as the distance between the free MM to a mucogingival junction (MGJ).
- Mucosal thickness (MT) was assessed at middle aspect of the examined implant, 3 mm from the top of the MM, by using endodontic needle (K-file, ISO 25) perpendicularly, under the local anesthesia (LA).
- Peri-implant osseous defects were estimated during the surgical procedure, following granulation tissue removal and implant surface mechanical decontamination. The defect morphology was classified into categories previously described by Schwarz et al. [18];
- Healing index (HI) was estimated within one month postoperatively, scored from 1 to 5 according to Landry et al. [39];
- Periodontitis history presence was assessed as dichotomously (yes/no);
- Visual analogue scale (VAS) had obtained patient morbidity and discomfort during surgical intervention and within four weeks postoperatively, scored 1 to 10. Cut-off points for both pain and difficulty were ≤3.4 (none or mild), 3.5–7.4 (moderate), and ≥7.5 (severe).
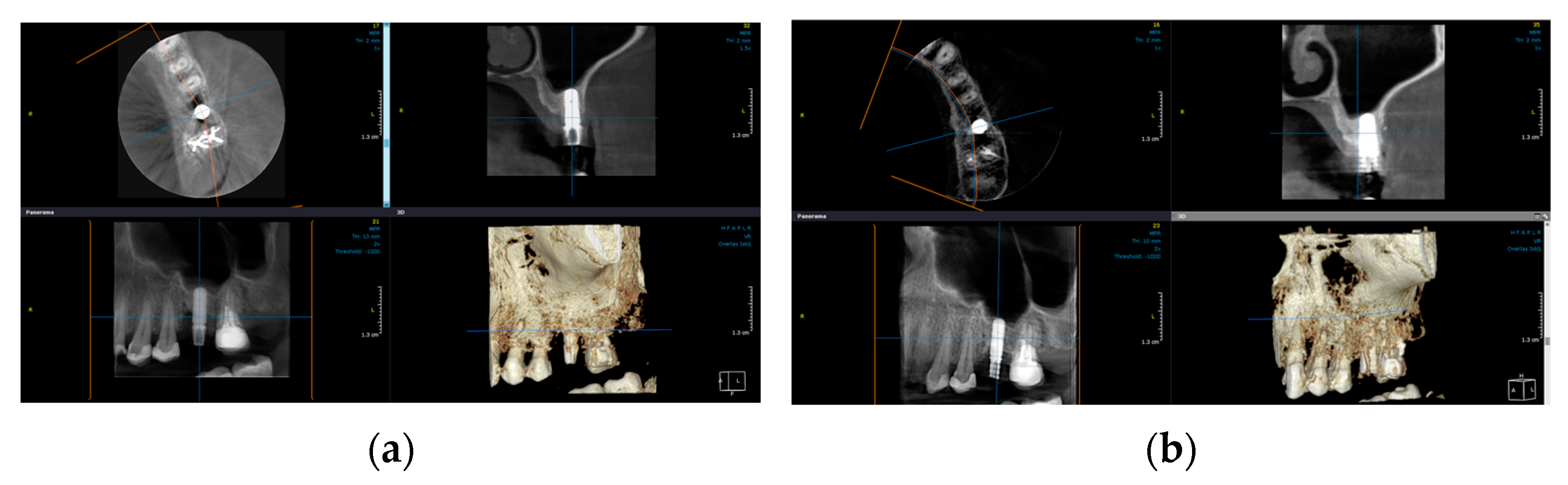
2.3.2. Radiographic Examination
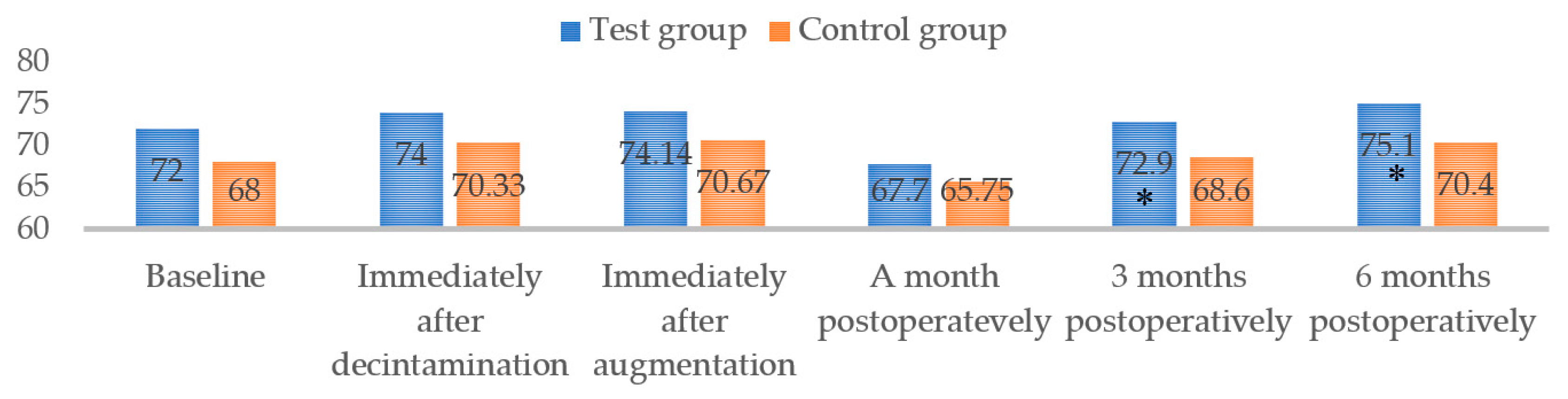
2.3.3. Implant Stability (ISQ) Examination
2.3.4. Success of Augmentation Therapy
2.4. Statistical Analysis
3. Results
3.1. Demographic Data and Implants-Based Characteristics
3.2. Clinical Outcomes Assessment
3.3. Radiographic Outcomes Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral. Implant. Res. 2009, 20 (Suppl. S4), 172–184. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Dahlin, C.; Jemt, T.; Sennerby, L.; Turri, A.; Wennerberg, A. Is marginal bone loss around oral implants the result of a provoked foreign body reaction? Clin. Implant. Dent. Relat. Res. 2014, 16, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Chapple, I.L. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39 (Suppl. S12), 202–206. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Rakašević, D.; Lazić, Z.; Rakonjac, B.; Soldatović, I.; Janković, S.; Magić, M.; Aleksić, Z. Efficiency of photodynamic therapy in the treatment of peri-implantitis—A three-month randomized controlled clinical trial. Srp. Arh. Celok. Lek. 2016, 144, 478–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarz, F.; Jepsen, S.; Obreja, K.; Galarraga-Vinueza, M.E.; Ramanauskaite, A. Surgical therapy of peri-implantitis. Periodontol. 2000 2022, 88, 145–181. [Google Scholar] [CrossRef]
- Roccuzzo, A.; De Ry, S.P.; Sculean, A.; Roccuzzo, M.; Salvi, G.E. Current Approaches for the Non-surgical Management of Peri-implant Diseases. Curr. Oral Health Rep. 2020, 7, 274–282. [Google Scholar] [CrossRef]
- Renvert, S.; Hirooka, H.; Polyzois, I.; Kelekis-Cholakis, A.; Wang, H.L. Diagnosis and non-surgical treatment of peri-implant diseases and maintenance care of patients with dental implants—Consensus report of working group 3. Int. Dent. J. 2019, 69 (Suppl. S2), 12–17. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Jepsen, S.; Herten, M.; Sager, M.; Rothamel, D.; Becker, J. Influence of different treatment approaches on non-submerged and submerged healing of ligature induced peri-implantitis lesions: An experimental study in dogs. J. Clin. Periodontol. 2006, 33, 584–595. [Google Scholar] [CrossRef]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Salvi, G.E.; Mombelli, A.; Loup, P.J.; Heitz, F.; Kruger, E.; Lang, N.P. Supportive peri-implant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin. Oral. Implant. Res. 2018, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ramanauskaite, A.; Daugela, P.; Faria de Almeida, R.; Saulacic, N. Surgical non-regenerative treatments for peri-implantitis: A systematic review. J. Oral. Maxillofac. Res. 2016, 7, e14. [Google Scholar] [CrossRef] [Green Version]
- de Waal, Y.C.; Raghoebar, G.M.; Meijer, H.J.; Winkel, E.G.; van Winkelhoff, A.J. Prognostic indicators for surgical peri-implantitis treatment. Clin. Oral. Implant. Res. 2016, 27, 1485–1491. [Google Scholar] [CrossRef]
- Lasserre, J.F.; Brecx, M.C.; Toma, S. Implantoplasty Versus Glycine Air Abrasion for the Surgical Treatment of Peri-implantitis: A Randomized Clinical Trial. Int. J. Oral. Maxillofac. Implant. 2020, 35, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Luengo, F.; Solonko, M.; Sanz-Esporrín, J.; Sanz-Sánchez, I.; Herrera, D.; Sanz, M. Clinical, microbiological, and biochemical impact of the surgical treatment of peri-implantitis-a prospective case series. J. Clin. Med. 2022, 11, 4699. [Google Scholar] [CrossRef]
- Roos-Jansaker, A.M.; Renvert, H.; Lindahl, C.; Renvert, S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: A prospective cohort study. J. Clin. Periodontol. 2007, 34, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Sahm, N.; Schwarz, K.; Becker, J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J. Clin. Periodontol. 2010, 37, 449–455. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Bieling, K.; Becker, J. Surgical regenerative treatment of peri-implantitis lesions using a nanocrystalline hydroxyapatite or a natural bone mineral in combination with a collagen membrane: A four-year clinical follow-up report. J. Clin. Periodontol. 2009, 36, 807–814. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bonino, F.; Bonino, L.; Dalmasso, P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: Comparative results of a prospective study on two different implant surfaces. J. Clin. Periodontol. 2011, 38, 738–745. [Google Scholar] [CrossRef] [Green Version]
- Monje, A.; Pons, R.; Roccuzzo, A.; Salvi, G.E.; Nart, J. Reconstructive therapy for the management of peri-implantitis via submerged guided bone regeneration: A prospective case series. Clin. Implant. Dent. Relat. Res. 2020, 22, 342–350. [Google Scholar] [CrossRef]
- Klein, M.O.; Kämmerer, P.W.; Götz, H.; Duschner, H.; Wagner, W. Long-term bony integration and resorption kinetics of a xenogeneic bone substitute after sinus floor augmentation: Histomorphometric analyses of human biopsy specimens. Int. J. Periodontics Restor. Dent. 2013, 33, e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Aghazadeh, A.; Rutger Persson, G.; Renvert, S. A single-centre randomized controlled clinical trial on the adjunct treatment of intra-bony defects with autogenous bone or a xenograft: Results after 12 months. J. Clin. Periodontol. 2012, 39, 666–673. [Google Scholar] [CrossRef]
- Ramos, U.D.; Suaid, F.A.; Wikesjö, U.M.E.; Susin, C.; Taba, M., Jr.; Novaes, A.B., Jr. Comparison between two antimicrobial protocols with or without guided bone regeneration in the treatment of peri-implantitis. A histomorphometric study in dogs. Clin. Oral. Implant. Res. 2017, 28, 1388–1395. [Google Scholar] [CrossRef]
- Derks, J.; Ortiz-Vigón, A.; Guerrero, A.; Donati, M.; Bressan, E.; Ghensi, P.; Schaller, D.; Tomasi, C.; Karlsson, K.; Abrahamsson, I.; et al. Reconstructive surgical therapy of peri-implantitis: A multicenter randomized controlled clinical trial. Clin. Oral. Implant. Res. 2022, 33, 921–944. [Google Scholar] [CrossRef]
- Teng, F.; Wei, L.; Yu, D.; Deng, L.; Zheng, Y.; Lin, H.; Liu, Y. Vertical bone augmentation with simultaneous implantation using deproteinized bovine bone block functionalized with a slow delivery of BMP-2. Clin. Oral. Implant. Res. 2020, 31, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Blatt, S.; Thiem, D.G.E.; Kyyak, S.; Pabst, A.; Al-Nawas, B.; Kämmerer, P.W. Possible implications for improved osteogenesis? The combination of platelet-rich fibrin with different bone substitute materials. Front. Bioeng. Biotechnol. 2021, 9, 640053. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Chiantella, G.C.; Windisch, P.; Gera, I.; Reich, E. Clinical evaluation of an enamel matrix protein derivative (Emdogain) combined with a bovine-derived xenograft (Bio-Oss) for the treatment of intrabony periodontal defects in humans. Int. J. Periodontics Restor. Dent. 2002, 22, 259–267. [Google Scholar]
- Pilloni, A.; Rojas, M.A.; Marini, L.; Russo, P.; Shirakata, Y.; Sculean, A.; Iacono, R. Healing of intrabony defects following regenerative surgery by means of single-flap approach in conjunction with either hyaluronic acid or an enamel matrix derivative: A 24-month randomized controlled clinical trial. Clin. Oral. Investig. 2021, 25, 5095–5107. [Google Scholar] [CrossRef]
- Fraser, J.R.; Laurent, T.C.; Laurent, U.B. Hyaluronan: Its nature, distribution, functions and turnover. J. Intern. Med. 1997, 242, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Eliezer, M.; Imber, J.C.; Sculean, A.; Pandis, N.; Teich, S. Hyaluronic acid as adjunctive to non-surgical and surgical periodontal therapy: A systematic review and meta-analysis. Clin. Oral. Investig. 2019, 23, 3423–3435. [Google Scholar] [CrossRef]
- Kyyak, S.; Pabst, A.; Heimes, D.; Kämmerer, P.W. The influence of hyaluronic acid biofunctionalization of a bovine bone substitute on osteoblast activity in vitro. Materials 2021, 14, 2885. [Google Scholar] [CrossRef] [PubMed]
- Shirakata, Y.; Imafuji, T.; Nakamura, T.; Kawakami, Y.; Shinohara, Y.; Noguchi, K.; Pilloni, A.; Sculean, A. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: A preclinical study in dogs. Quintessence Int. 2021, 308–316. [Google Scholar] [CrossRef]
- Asparuhova, M.B.; Chappuis, V.; Stähli, A.; Buser, D.; Sculean, A. Role of hyaluronan in regulating self-renewal and osteogenic differentiation of mesenchymal stromal cells and pre-osteoblasts. Clin. Oral. Investig. 2020, 24, 3923–3937. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, T.; Watanabe, C. Stimulation of osteoinduction in bone wound healing by high-molecular hyaluronic acid. Bone 1995, 16, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Fernández, E.; Magán-Fernández, A.; O’Valle, F.; Bravo, M.; Mesa, F. Hyaluronic acid reduces inflammation and crevicular fluid IL-1β concentrations in peri-implantitis: A randomized controlled clinical trial. J. Periodontal Implant. Sci. 2021, 51, 63–74. [Google Scholar] [CrossRef]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Mombelli, A.; van Oosten, M.A.; Schurch, E., Jr.; Land, N.P. The microbiota associated with successful or failing osseointegrated titanium implants. Oral. Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Landry, R.G.; Turnbull, R.S.; Howley, T. Effectiveness of benzydamyne HCl in the treatment of periodontal post-surgical patients. Res. Clin. Forums. 1988, 10, 105–118. [Google Scholar]
- Jepsen, S.; Schwarz, F.; Cordaro, L.; Derks, J.; Hämmerle, C.H.F.; Heitz-Mayfield, L.J.; Hernández-Alfaro, F.; Meijer, H.J.A.; Naenni, N.; Ortiz-Vigón, A.; et al. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol. 2019, 46 (Suppl. S21), 277–286. [Google Scholar] [CrossRef]
- Tomasi, C.; Regidor, E.; Ortiz-Vigón, A.; Derks, J. Efficacy of reconstructive surgical therapy at peri-implantitis-related bone defects. A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 340–356. [Google Scholar] [CrossRef] [Green Version]
- Roccuzzo, M.; Gaudioso, L.; Lungo, M.; Dalmasso, P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with 10% collagen. J. Clin. Periodontol. 2016, 43, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Terao, T. Hyaluronic acid-specific regulation of cytokines by human uterine fibroblasts. Am. J. Physiol. 1997, 273, C1151–C1159. [Google Scholar] [CrossRef] [PubMed]
- Božić, D.; Ćatović, I.; Badovinac, A.; Musić, L.; Par, M.; Sculean, A. Treatment of intrabony defects with a combination of hyaluronic acid and deproteinized porcine bone mineral. Materials 2021, 14, 6795. [Google Scholar] [CrossRef]
- Rakašević, D.; Gabrić, D. The effect of implant surface design and their decontamination methods in peri-implantitis treatment. In Current Concepts in Dental Implantology; Dragana, G., Marko, V., Eds.; IntechOpen: Rijeka, Croatia, 2021. [Google Scholar]
- Renvert, S.; Polyzois, I.; Maguire, R. Re-osseointegration on previously contaminated surfaces: A systematic review. Clin. Oral. Implant. Res. 2009, 20 (Suppl. S4), 216–227. [Google Scholar] [CrossRef] [PubMed]
- Marotti, J.; Tortamano, P.; Cai, S.; Ribeiro, M.S.; Franco, J.E.; de Campos, T.T. Decontamination of dental implant surfaces by means of photodynamic therapy. Lasers Med. Sci. 2013, 28, 303–309. [Google Scholar] [CrossRef] [Green Version]
- González, F.J.; Requena, E.; Miralles, L.; Sanz, J.L.; Barberá, J.; Enciso, J.J.; Larrazábal, C.; Gómez, M.D. Adjuvant Effect of Titanium Brushes in Peri-Implant Surgical Treatment: A Systematic Review. Dent. J. 2021, 9, 84. [Google Scholar] [CrossRef]
- de Tapia, B.; Valles, C.; Ribeiro-Amaral, T.; Mor, C.; Herrera, D.; Sanz, M.; Nart, J. The adjunctive effect of a titanium brush in implant surface decontamination at peri-implantitis surgical regenerative interventions: A randomized controlled clinical trial. J. Clin. Periodontol. 2019, 46, 586–596. [Google Scholar] [CrossRef]
- Haas, R.; Baron, M.; Dortbudak, O.; Watzek, G. Lethal photosensitization, autogenous bone, and e-PTFE membrane for the treatment of peri-implantitis: Preliminary results. Int. J. Oral. Maxillofac. Implant. 2000, 15, 374–382. [Google Scholar]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test Group | Control Group | Total | p-Value | ||
|---|---|---|---|---|---|
| Sex, n (%) | Female | 8(62) | 0.633 | ||
| History of treated periodontitis, n (%) | Yes | 3 (16) | 0.523 | ||
| Periodontitis | Grade II, Stage B | 5 (38) | 0.634 | ||
| Grade III, Stage B | 3 (24) | ||||
| Others | 5 (38) | ||||
| Smokers (<10 cigarettes), n (%) | 2 (33) | 2 (28) | 5 (38) | 0.326 | |
| Location, n (%) | Maxilla | 5 (71.4) | 9 (75) | 14 (74) | 0.999 |
| Mandible | 2 (28.6) | 3 (25) | 5 (26) | ||
| Implant system, n (%) | Straumann | 2 (29) | 7 (58) | 9 (47.4) | 0.425 |
| Bredent | 3 (44) | 2 (17) | 5 (26.3) | ||
| Other | 2 (29) | 5 (25) | 5 (26.3) | ||
| Type of restoration, n (%) | Cement-retained, single crown | 6 (86) | 6 (50) | 12 (63.2) | 0.173 |
| Screw-retained, single crown | 1 (14) | 6 (50) | 7 (31) | ||
| Peri-implant osseous defects, n (%) | Class 1 b | 4 (58) | 7 (58) | 11 (57) | 0.642 |
| Class 1 c | 1 (14) | 3 (25) | 4 (22) | ||
| Class 1 e | 1 (14) | 2 (17) | 3 (16) | ||
| Class 2 b | 1 (14) | 0 (0) | 1 (5) | ||
| Follow-Up Periods | Test Group | Control Group | p-Value | |
|---|---|---|---|---|
| PPD, SD ± mean | Baseline | 5.38 ± 1.06 | 5.10 ± 0.92 | 0.576 |
| 3 months | 2.56 ± 0.78 | 2.71 ± 0.38 | 0.573 | |
| 6 months | 2.34 ± 0.4 | 2.51 ± 0.39 | 0.360 | |
| Δ 6 m | 3.02 ± 0.94 | 2.6 ± 0.88 | 0.333 | |
| CAL, SD ± mean | Baseline | 4 ± 1.47 | 3.13 ± 1.49 | 0.179 |
| 3 months | 1.31 ± 0.62 | 1.83 ± 0.78 | 0.153 | |
| 6 months | 2.34 ± 0.1.67 | 2.5 ± 1.92 | 0.432 | |
| Δ 6 m | 1.64 ±1.09 | 1.21 ± 0.84 | 0.341 | |
| MT, SD ± mean | Baseline | 0.65 ± 0.16 | 0.90 ± 0.39 | 0.070 |
| 3 months | 1. 51± 0.37 | 1.45 ± 0.41 | 0.737 | |
| 6 months | 1.54 ± 0.59 | 1.56 ± 0.40 | 0.921 | |
| Δ 6 m | 0.9 ± 0.47 | 0. 6 ± 0.54 | 0.25 | |
| KMW, SD ± mean | Baseline | 2.36 ± 1.97 | 2.57 ± 2.02 | 0.578 |
| 3 months | 2.93 ±1.17 | 2.86 ± 1.92 | 0.318 | |
| 6 months | 3.26 ± 0.67 | 2.83 ± 2.01 | 0.131 | |
| Δ 6 m | 0.9 ± 1.9 | 0. 42 ± 0.96 | 0.47 | |
| mBlI score, n | Baseline | 2.55 ± 0.47 | 2.49 ± 0.61 | 0.724 |
| 3 months | 0.05 ± 0.12 | 0.06 ± 0.15 | 0.894 | |
| 6 months | 0 | 0.17 ± 0.39 | 0.266 | |
| Δ 6 m | 2.55 ± 0.47 | 2.32 ± 0.69 | 0.759 | |
| PI score, n | Baseline | 1.12 ± 0.74 | 1.22 ± 0.70 | 0.992 |
| 3 months | 0.1 ± 0.19 | 0.2 ± 0.21 | 0.345 | |
| 6 months | 0.07 ± 0.13 | 0.05 ± 0.1 | 0.996 | |
| Δ 6 m | 1.05 ± 0.69 | 1.17 ±0.7 | 0.767 |
| Test Group | Control Group | ||||||
|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | Δ BG | Baseline | 6 Months | Δ BG | ||
| V- MB level Mean ± SD | Mesial | 3.24 ± 1.44 | 0.22 ± 0.34 | 3.02 ± 1.01 * | 2.65 ± 1.36 | 0.68 ± 1.54 | 1.97 ± 0.43 * |
| Distal | 5.15 ± 2.38 | 0.77 ±1.56 | 4.38 ±1.6 * | 3.25 ±1 0.31 | 0.39 ± 0.42 | 2.89 ± 0.9 * | |
| Buccal | 3.76 ± 1.7 | 0.71 ± 0.5 | 3.05 ± 1.04 | 3.65 ± 1.32 | 0.2 ± 0.25 | 3.45 ± 1.11 | |
| Oral | 4.44 ± 2.1 | 0.29 ± 0.33 * | 4.15 ± 1.77 * | 2.41 ± 1.14 | 0.77 ± 1.4 * | 1.63 ± 0.4 * | |
| H- MB level Mean ± SD | Mesial | 3.81 ± 0.9 | 0.42 ± 0.92 | 3.39 ± 0.2 | 3.1 ± 0.9 | 0.16 ± 0.32 | 2.94 ± 0.7 |
| Distal | 3.51 ± 1.24 | 0.24 ± 1.1 | 3.27 ± 0.32 | 2.1 ± 1.12 | 0.17 ± 0.31 | 1.93 ± 0.75 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rakašević, D.; Šćepanović, M.; Mijailović, I.; Mišić, T.; Janjić, B.; Soldatović, I.; Marković, A. Reconstructive Peri-Implantitis Therapy by Using Bovine Bone Substitute with or without Hyaluronic Acid: A Randomized Clinical Controlled Pilot Study. J. Funct. Biomater. 2023, 14, 149. https://doi.org/10.3390/jfb14030149
Rakašević D, Šćepanović M, Mijailović I, Mišić T, Janjić B, Soldatović I, Marković A. Reconstructive Peri-Implantitis Therapy by Using Bovine Bone Substitute with or without Hyaluronic Acid: A Randomized Clinical Controlled Pilot Study. Journal of Functional Biomaterials. 2023; 14(3):149. https://doi.org/10.3390/jfb14030149
Chicago/Turabian StyleRakašević, Dragana, Miodrag Šćepanović, Iva Mijailović, Tijana Mišić, Bojan Janjić, Ivan Soldatović, and Aleksa Marković. 2023. "Reconstructive Peri-Implantitis Therapy by Using Bovine Bone Substitute with or without Hyaluronic Acid: A Randomized Clinical Controlled Pilot Study" Journal of Functional Biomaterials 14, no. 3: 149. https://doi.org/10.3390/jfb14030149