

The Reemergence of Monkeypox in Nigeria

1
Department of Microbiology, University of Lagos, Lagos, Nigeria
2
Department of Biochemistry, Federal University of Technology Akure (FUTA), Akure, Nigeria
*
Author to whom correspondence should be addressed.
Challenges 2023, 14(2), 22; https://doi.org/10.3390/challe14020022
Submission received: 12 March 2023
/
Revised: 18 April 2023
/
Accepted: 19 April 2023
/
Published: 20 April 2023
(This article belongs to the Special Issue Planetary Health: Building the Field and Growing the Movement (Including Manuscripts 2022 Planetary Health Annual Meeting and Festival))
Abstract
:The emergence and reemergence of infectious diseases caused by viruses continue to be a major public health concern globally, affecting both humans and animals. One such disease is monkeypox, a zoonotic infection caused by the monkeypox virus (MPXV) that has recurred in sub-Saharan Africa over several decades. Notably, the 2022 outbreak of monkeypox in Nigeria follows a deadly outbreak in 2017, which was preceded by the disease’s first recorded outbreak in 1978. Epidemiological investigations in 2017 showed no apparent link between human monkeypox cases and the outbreak that year, indicating the potential existence of multiple sources of the virus and limited human-to-human transmission. This underscores the presence of an alternative ecological niche in humans. Furthermore, in some communities in Nigeria, monkeys are regarded as sacred and not hunted or consumed, leading to their proliferation and increased likelihood of MPXV transmission. This mini-review focuses on the occurrence, epidemiological distribution, geographical distribution, endemicity, and possible solutions to reduce the spread of human monkeypox in Nigeria. The implications of this reemergence and the need for effective public health measures to prevent and control outbreaks of monkeypox are also discussed.
1. Introduction
Monkeypox is a zoonotic disease endemic to Central and West Africa [1], caused by the Monkeypox virus, a deadly virus of current public health concern. The Monkeypox virus, MPXV is a member of the Poxviridae family, with other members, such as variola virus (the virus responsible for smallpox disease), vaccinia virus (employed in the smallpox vaccine) [2], and the ectromelia, camelpox, and cowpox viruses [3].
Monkeypox, also referred to as Mpox, was first discovered in 1958 when there was an occurrence of a “pox-like” disease in two outbreaks in monkey colonies that had been set aside for research purposes. Although this “pox-like” disease was given the name “monkeypox,” the original generating source has remained unclear. Rodents found in Africa and non-human primates (i.e., monkeys) have been proposed as the reservoirs of the virus and the most probable primary cause of infections in humans [4].
The MPXV has linear double-stranded DNA, with a size ranging from 200 to 250 nm. The virus is also brick-shaped and enveloped, having the ability to invade host cells via the classical apoptotic mimicry mechanism [5]. Two clades have been described in the MPXV—the Central African/Congo Basin (CA) and West African (WA) clades. However, there have been recent reports showing that the clade should be renamed to Clade 1 (CA) and Clades 2 and 3 (WA), to avoid a bias nomenclature associated with geographic regions and nations [6].
After the discovery of human Monkeypox in 1970, several other human cases have been reported in many Central and Western African countries. Clinically, the symptoms of human Monkeypox are almost indistinguishable from the symptoms of smallpox but they appear milder and are rarely fatal. However, the enlargement of the lymph node occurring early at the onset of fever is a major distinguishing symptom between Monkeypox and smallpox. A rash sometimes appears, usually within the first three days after the onset of fever and lymphadenopathy, with the appearance of lesions simultaneously, and evolving at an equal speed. Another important peculiar characteristic specific to Monkeypox is that the pox distribution is mainly peripheral but, in severe cases, covers the whole body with an infection that can last up to 4 weeks until the lesion desquamates [7].
To date, there have been cases of human Monkeypox in 10 different African countries—the Democratic Republic of the Congo, Sierra Leone, Republic of the Congo, Cameroon, Gabon Central African Republic, Ivory Coast, Liberia, Nigeria, and South Sudan [8,9].
This article reviews the epidemiology, endemicity, and possible solutions to reduce the spread of human Monkeypox in Nigeria. Understanding the true state of human Monkeypox in Nigeria would be impactful in the efforts to limit the spread, direct decision making, and policy integration in public health, as well as contributing to the current pool of information available on human Monkeypox.
2. Methodology
2.1. Search Method
A literature search for the review was performed in “Science direct”, “Google scholar”, “PubMed”, “AJOL”, and “NATURE” journals using combinations of words as search terms, such as “Monkeypox in Nigeria”, “Human Monkeypox in Nigeria”, and “MPXV in Nigeria” to find articles published before 30 October 2022. Further, some published articles by the WHO and Nigeria Center for Disease Prevention and Control were included in the analysis.
2.2. Eligibility Criteria (Inclusion and Exclusion Criteria)
Identification of studies meeting the inclusion criteria was performed by the review authors, who screened the titles and abstracts of all retrieved articles. After the selected articles were read, a conclusive decision was made for each study.
The inclusion criteria include studies based on experimental data, studies discussing clinical manifestation and epidemiology of human Monkeypox, studies based on transmission and host reservoir of MPXV, and studies containing information on occurrence, pathogenesis, and symptoms of Monkeypox. Studies with old data that were not pertinent to the aim of the study were excluded. Studies not including Nigeria were excluded. Studies in Africa but not including Nigeria were excluded.
2.3. Data Extraction
Data were extracted from all selected articles independently by the reviewers based on the main research objectives: epidemiology, endemicity, and possible solutions to reduce the spread of human Monkeypox in Nigeria. All findings and statements regarding the outbreak in this study are based on published information, as listed in the references.
3. Results
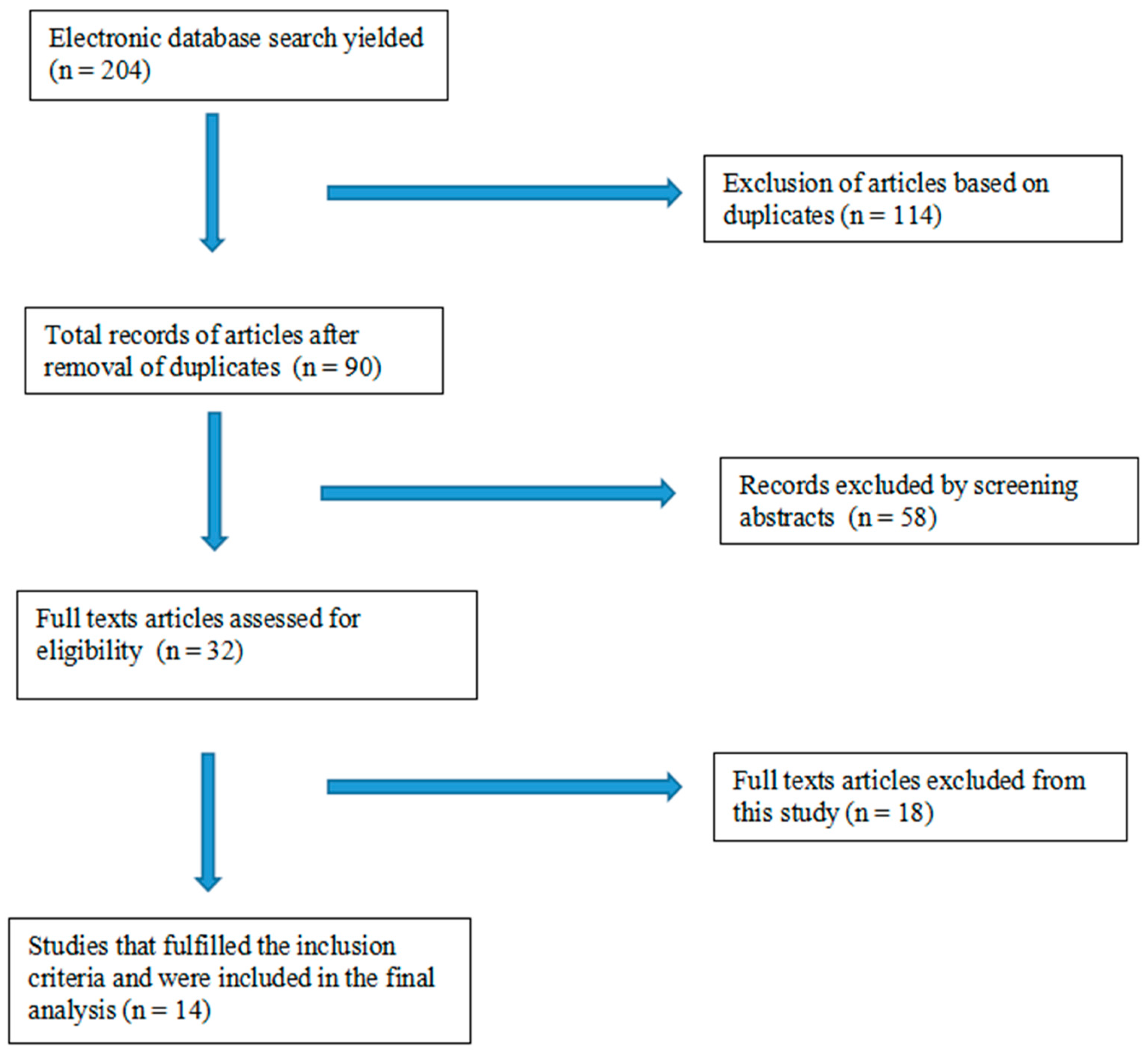
The database search identified a total of 204 articles, amongst which 11 articles were selected for this study. An additional six articles were added to the study through the reference list search. A total of 14 articles were analyzed for the review. The screening procedure for the included studies is shown in Figure 1.
3.1. Occurrence of Human Monkeypox in Nigeria
Prior to the recent outbreak of Monkeypox in Nigeria, the largest and most lethal outbreak was in 2017, which came after the Monkeypox outbreak of 1978 [10]. The Nigeria Centre for Disease Control (NCDC), on 22 September 2017, commenced an investigation on the Monkeypox outbreak following the identification of a child with a suspected case of Monkeypox [11]. This action showed the preparedness of the NCDC at this time for the outbreak. It activated an emergency operations center (EOC) on 9 October 2017, to implement plans against the outbreak [12]. The plan mainly focused on the research into the epidemiology of MPXV in regions with a high risk of the human–environmental–animal interface. Improved diagnosis and state-of-the-art sequencing were employed to assess various factors contributing to and enhancing the spread of monkeypox [10,13]. The data that were generated in 2017 suggested that the cases of human monkeypox and the 2017 outbreak were not linked epidemiologically. It was also noted that there was a possibility of the outbreak being connected to multiple sources with fewer human-to-human transmissions. This shows the existence of another ecological niche in humans where the expansion of the virus can occur aside from its natural reservoir. However, the specific source and role(s) played by the other abiotic factors in the Nigeria outbreak are not fully elucidated.
3.2. Declining Population Immunity in Nigeria
The significant epidemiological distribution of Monkeypox across West Africa and Nigeria provides an avenue for continuous spread across other regions and internationally. Whilst the stoppage of vaccination against smallpox stands as a huge pointer to the occurrences of Monkeypox in Nigeria because of a reduction in herd immunity, they could have risen from the increased human contact with other humans that have remained as endemic carriers of the MPXV [12,13]. Cases of protection against the MPXV as a result of vaccination against smallpox have been shown in studies on monkeys [14]. There is actually a concern that mass vaccination against smallpox might, in one way or another, curb the spread of the human Monkeypox virus. This concern is not baseless as there is a possibility that the absence of protection capability against MPXV in the younger age brackets that have not been vaccinated and the decreasing herd immunity among the older vaccinated age groups might be a risk factor in the increased susceptibility to the human Monkeypox infection [15]. This case is evident in Nigeria as the larger chunk of confirmed cases are found in the age group between 21 and 40 years, having a median age of 31 years (Table 1).
3.3. Geographic Distribution and Epidemiology of Human Monkeypox in Nigeria
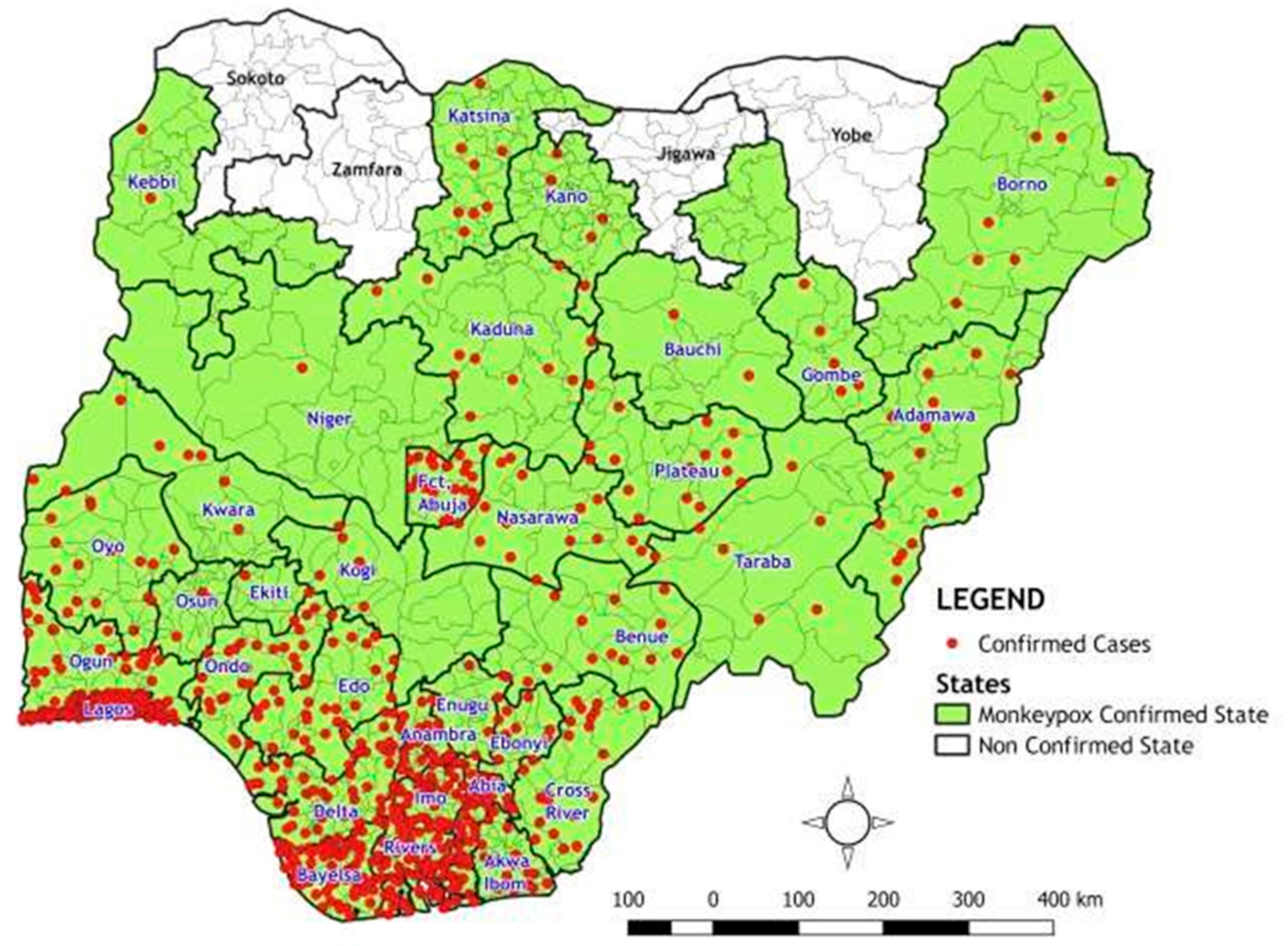
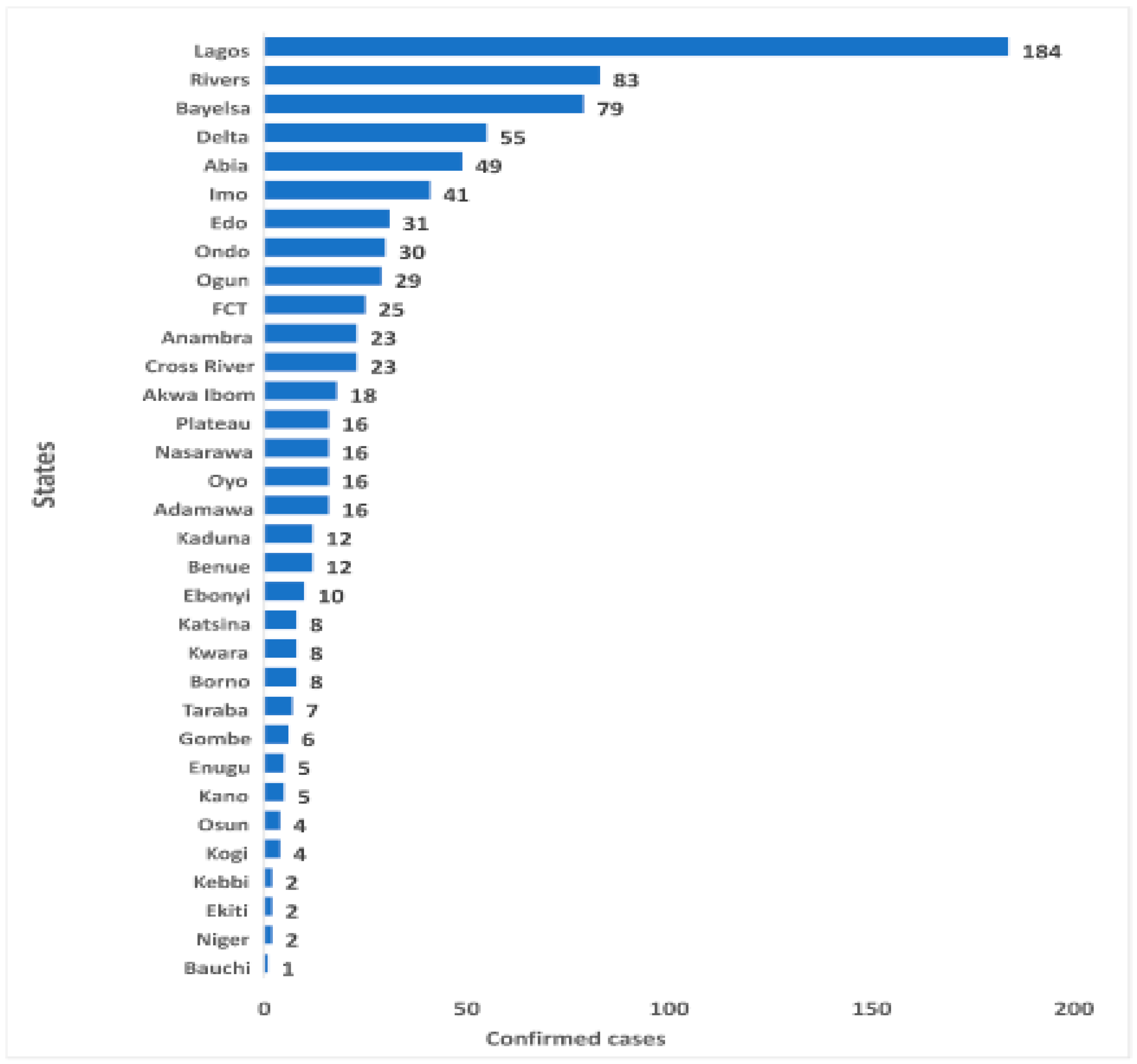
The World Health Organization (WHO) [8,9] describes Monkeypox as a zoonotic infection of viral origin occurring majorly in remote parts of Central and West Africa, along the tropical rainforest. This is the most probable case in Nigeria as many of the confirmed cases come from the state where the country’s dense forests and swamps are concentrated. The majority of Nigeria’s rainforest is situated in the Niger Delta and concentrated in the states of Rivers, Bayelsa, Edo, Cross River, Ondo, Ekiti, and Osun. Some of these states have, over the years, become the largest epicenter of confirmed cases in Nigeria (Figure 2 and Figure 3) and serve as a natural ecological niche of monkeypox [10]. Satellite imagery has shown that there is increasing development in the southern region of Nigeria, which is made at the cost of these forests [17]. The increase in the development of these areas also increases the chances of animal reservoirs, such as rodents, rabbits, and primates, having lost their natural habitat to have increased contact with humans [18].
It is also common to find monkeys allowed to roam freely in the compound and homes of people without being molested as the people in the community consider the animals sacred and never kill or eat them. “Awka na aso enwe”, meaning Awka forbids or does not eat monkeys, is a popular term used in the Capital City of Anambra state. This is also the tale in some parts of Enugu, Abia, and Ebonyi State. In Nigeria and most parts of Africa, bushmeat is a delicacy. This refers to any wild animal that is killed for consumption, including snakes, fruit bats, wild rats, antelopes, and porcupines. Hunters and dealers of ‘bush meat’ are key players in the process of any ‘spillover’ of the MPXV pathogen in Nigeria. Bayelsa, Delta, and River states are some states in Nigeria where the bushmeat business is prominent and thriving.
Previous studies have discovered a high serological prevalence of Orthopoxvirus (OPXV)-specific IgG in inhabitants of these forest locations, indicating constant continuous contact with Monkeypox virus and other Orthopoxviruses [19,20]. Additionally, the results published by the Nigeria CDC on the confirmed cases of monkeypox in Nigeria show that there is a higher prevalence of confirmed cases occurring among men in Nigeria (Figure 4). This is most likely due to the fact that men are more involved in activities in relation to wild animals, such as hunting and trading bushmeat, and, as such, are in contact with MPXV and other OPXVs.
Fresh cases of human Monkeypox are continuously being recorded in Nigeria, and as of 30 October 2022, 2061 suspected cases and 803 (40.3%) confirmed cases (550 male and 280 female) had been noted in 32 states and FCT since the reemergence of Monkeypox in 2017 [16], across various age groups. With 803 confirmed cases having been recorded in 32 states and FCT (Rivers, Bayelsa, Ondo, Gombe, Taraba, Kano, Niger, Cross River, Imo, Ogun, Ebonyi, Kogi, Kwara, Borno, Katsina, Adamawa, Akwa Ibom, Lagos, Delta, Bauchi, Abia, Oyo, Enugu, Ekiti, Nasarawa, Benue, Plateau, Edo, Anambra, Kaduna, Osun, Kebbi) and 15 deaths in 11 states (Lagos, Imo, Edo, FCT, Rivers, Cross River, Delta, Akwa Ibom, Taraba, Kogi, Ondo), there is an indication of endemicity of the MPXV in Nigeria.
3.4. Rise in Monkeypox Cases in Nigeria: Underlying Causes and Proposed Solution
The resurgence of Monkeypox in Nigeria has become a significant challenge for health authorities, policymakers, and local communities in Nigeria. This zoonotic disease, similar to smallpox, is transmitted through the exchange of bodily fluids with infected animals, such as rodents, monkeys, and squirrels. However, it can also be transmitted through close contact with an infected individual. One of the primary drivers behind the recent rise in Monkeypox cases in Nigeria is the growing contact between humans and wildlife, especially wildlife displaced due to deforestation, conflict, and poverty, particularly in North-Eastern Nigeria. This leads to increased population migration into forests, reliance on wild animals for food, and, therefore, a higher likelihood of human–animal contact and transmission of the virus. Moreover, excessive and unregulated contact with wild animals that serve as animal reservoirs of MPXV by residents of rainforest regions could be contributing factors to the reemergence of the disease. Additionally, inadequate surveillance and disease monitoring systems in the country could cause cases to go unnoticed or underreported, making it challenging to track and control the outbreak. Furthermore, increased urbanization and various activities such as traveling could also play a crucial role in the human-to-human transmission of MPXV. To combat the reemergence of Monkeypox in Nigeria, a comprehensive approach is necessary.
First, the One-Health approach, which emphasizes the interconnectedness of human, animal, and environmental health, could be a promising way to decrease the incidence of Monkeypox. This could involve coordinated efforts between human health, veterinary doctors, and environmental health professionals to address gaps in epidemiological data, identify specific animal reservoirs, and transmission patterns of the MPXV [21]. It is also essential to improve surveillance systems to effectively detect, monitor, and respond to outbreaks. This could be achieved by increasing funding for disease surveillance and strengthening collaboration between different arms of the government, NGOs, and community-based organizations [21].
Moreover, regulations should be put in place to limit the importation of rodents and non-human primates. Infected animals should be isolated from other animals that have been captured and placed into immediate quarantine. Raising public awareness about the disease and its prevention is also critical. This could be accomplished through campaigns, community engagement, and outreach programs aimed at educating high-risk groups, such as farmers, herdsmen, and other members of the public. Finally, the use of convalescent plasma from recovering patients has been shown to be effective in treating severe acute respiratory syndrome (SARS) and Ebola during previous epidemics that have caused global havoc [22,23]. This medical intervention dates back to the 1918 H1N1 influenza virus outbreak, where blood serum was administered to over 1700 patients. The use of convalescent plasma holds enormous promise for slowing the spread of infection and preventing the massive mortality that could result from a delay in the production of an effective medication or vaccine [23,24].
4. Conclusions
Monkeypox virus (MPXV) is a long-neglected zoonotic pathogen in Nigeria and, thus, further research is necessary to fully understand all the factors contributing to the reemergence of Monkeypox in Nigeria. This could facilitate the development of novel therapeutic compounds toward the protein target of the MPXV using computational methods and antiviral therapy to alleviate the disease’s impact. There is also a need for a surveillance study to be carried out in South-Eastern Nigeria to confirm the existence of a human reservoir for the virus.
Author Contributions
N.E. and O.A. conceptualized the present paper, whilst all authors were involved in data curation, formal analysis, and preparation of the initial draft of the manuscript. Investigations and Methodology were led by N.E. and T.A. Project administration was by N.E. Resources and software were led by T.A. and T.O. Supervision was conducted by N.E. and O.A., N.E. was responsible for review and editing of the final draft. All authors have read and agreed to the to the published version of the manuscript.
Funding
This review received no external funding and was self-sponsored by all the authors.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khodakevich, L.; Jezek, Z.; Messinger, D. Monkeypox virus: Ecology and public health significance. Bull. World Heal. Organ. 1988, 66, 747–752. [Google Scholar]
- Huygelen, C. Jenner’s cowpox vaccine in light of current vaccinology. Verh. K Acad. Geneeskd. Belg. 1996, 58, 479–536. [Google Scholar]
- Weinstein, R.A.; Nalca, A.; Rimoin, A.W.; Bavari, S.; Whitehouse, C.A. Reemergence of Monkeypox: Prevalence, Diagnostics, and Countermeasures. Clin. Infect. Dis. 2005, 41, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Update: Multistate outbreak of monkeypox—Illinois, Indiana, Kansas, Missouri, Ohio, and Wisconsin, 2003. MMWR Morb. Mortal Wkly. Rep. 2003, 52, 642–646. [Google Scholar]
- Swiss Institute of Bioinformatics (SIB). Orthopoxvirus. Available online: https://viralzone.expasy.org/149?outline=all_by_species (accessed on 7 April 2022).
- Happi, C.; Adetifa, I.; Mbala, P.; Njouom, R.; Nakoune, E.; Happi, A.; Ndodo, N.; Ayansola, O.; Mboowa, G.; Bedford, T.; et al. Urgent Need For a Non-Discriminatory and Non-Stigmatizing Nomenclature For Monkeypox Virus. Available online: https://virological.org/t/urgent-need-for-a-non-discriminatory-and-non-stigmatizing-nomenclature-for-monkeypox-virus/853 (accessed on 7 April 2022).
- Fenner, F.; Henderson, D.A.; Arita, I.; Jezek, Z.; Ladnyi, I.D. Human Monkeypox and Other Poxvirus Infections of Man. In Smallpox and its Eradication; World Health Organization: Geneva, Switzerland, 1988; pp. 1371–1409. [Google Scholar]
- World Health Organization. Emergencies. Disease Outbreaks. Available online: https://www.who.int/emergencies/situations/monkeypox-oubreak-2022 (accessed on 1 November 2022).
- WHO. Fact Sheet on Monkeypox. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 1 November 2022).
- Yinka-Ogunleye, A.; Aruna, O.; Dalhat, M.; Ogoina, D.; McCollum, A.; Disu, Y.; Mamadu, I.; Akinpelu, A.; Ahmad, A.; Burga, J.; et al. Outbreak of human monkeypox in Nigeria in 2017–18: A clinical and epidemiological report. Lancet Infect. Dis. 2019, 19, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Eteng, W.E.; Mandra, A.; Doty, J.; Yinka-Ogunleye, A.; Aruna, S.; Reynolds, M.G.; McCollum, A.M.; Davidson, W.; Wilkins, K.; Saleh, M.; et al. Notes from the field: Responding to an outbreak of monkeypox using the one health approach—Nigeria, 2017–2018. MMWR Morb. Mortal Wkly. Rep. 2018, 67, 1040–1041. [Google Scholar] [CrossRef] [PubMed]
- Nigeria Centre for Disease Control and Prevention. Situation Report: Update of Monkeypox Outbreak in Nigeria. Available online: https://ncdc.gov.ng/themes/common/files/sitreps/7ba9ce49faf09f5212c1dbb48b31184b.pdf (accessed on 1 November 2022).
- Faye, O.; Pratt, C.B.; Faye, M.; Fall, G.; Chitty, J.A.; Diagne, M.M.; Wiley, M.R.; Yinka-Ogunleye, A.F.; Aruna, S.; Etebu, E.N.; et al. Genomic characterisation of human monkeypox virus in Nigeria. Lancet Infect. Dis. 2018, 18, 246. [Google Scholar] [CrossRef] [PubMed]
- McConnell, S.; Hickman, R.L.; Wooding, W.L., Jr.; Huxsoll, D.L. Monkeypox: Experimental infection in chimpanzee (Pan satyrus) and immunization with vaccinia virus. Am. J. Vet. Res. 1968, 29, 1675–1680. [Google Scholar] [PubMed]
- Sklenovská, N.; Van Ranst, M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front. Public Heal. 2018, 6, 241. [Google Scholar] [CrossRef] [PubMed]
- Nigeria Centre for Disease Control and Prevention. An Update of a Monkeypox Outbreak in Nigeria. Available online: https://ncdc.gov.ng/diseases/sitreps/?cat=8&name=An%20Update%20of%20Monkeypox%20Outbreak%20in%20Nigeria (accessed on 1 November 2022).
- Izah, L.N.; Majid, Z.; Ariff, M.F.M.; Mohammed, H.I. Determining land use change pattern in southern Nigeria: A comparative study. IOP Conf. Ser. Earth Environ. Sci. 2018, 169, 012040. [Google Scholar] [CrossRef]
- Faust, C.L.; McCallum, H.I.; Bloomfield, L.S.P.; Gottdenker, N.L.; Gillespie, T.R.; Torney, C.J.; Dobson, A.P.; Plowright, R.K. Pathogen spillover during land conversion. Ecol Lett. 2018, 21, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Leendertz, S.A.J.; Stern, D.; Theophil, D.; Anoh, E.; Mossoun, A.; Schubert, G.; Wiersima, L.; Akoua-Koffi, C.; Couacy-Hymann, E.; Muyembe-Tamfum, J.-J.; et al. A cross-sectional serosurvey of antiorthopoxvirus antibodies in central and western Africa. Viruses 2017, 9, 278. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, M.G.; Carroll, D.S.; Olson, V.A.; Hughes, C.; Galley, J.; Likos, A.; Montgomery, J.M.; Suu-Ire, R.; Kwasi, M.O.; Root, J.J.; et al. A silent enzootic of an orthopoxvirus in Ghana, West Africa: Evidence for multi-species involvement n the absence of widespread human disease. Am. J. Trop. Med. Hyg. 2010, 82, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Akinsuyi, S.O.; Orababa, O.Q.; Juwon, O.M.; Oladunjoye, I.O.; Akande, E.T.; Ekpueke, M.M.; Emmanuel, H. One Health approach, a solution to reducing the menace of multidrug-resistant bacteria and zoonoses from domesticated animals in Nigeria–A review. Glob. Biosecurity 2021, 3, 1. [Google Scholar] [CrossRef]
- Babalola, A.B.; Adetobi, E.T.; Akinsuyi, O.S.; Adebisi, O.A.; Folajimi, E.O. Computational study of the therapeutic potential of novel heterocyclic derivatives against SARS-CoV-2. COVID 2021, 1, 757–774. [Google Scholar] [CrossRef]
- Ekpunobi, N.; Markjonathan, I.; Olanrewaju, O.; Olanihun, D. Idiosyncrasies of COVID-19; A Review. Iran. J. Med. Microbiol. 2020, 14, 290–296. [Google Scholar] [CrossRef]
- Maxmen, A. How blood from coronavirus survivors might save lives. Nature 2020, 580, 16–17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Categorization of articles identified for the study.

Figure 2.
States in Nigeria with confirmed and non-confirmed human Monkeypox cases from September 2017 to 30 October 2022 (32 states and FCT). Source: NCDC, 2022 [16].
Figure 2.
States in Nigeria with confirmed and non-confirmed human Monkeypox cases from September 2017 to 30 October 2022 (32 states and FCT). Source: NCDC, 2022 [16].

Figure 3.
Chart of confirmed human Monkeypox cases by state, September 2017–30 October 2022; source: NCDC, 2022 [16].
Figure 3.
Chart of confirmed human Monkeypox cases by state, September 2017–30 October 2022; source: NCDC, 2022 [16].

Figure 4.
Chart showing the sex distribution of Nigeria’s confirmed monkeypox cases from September 2017 to 30 October 2022. Source: NCDC, 2022 [16].
Figure 4.
Chart showing the sex distribution of Nigeria’s confirmed monkeypox cases from September 2017 to 30 October 2022. Source: NCDC, 2022 [16].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Age distribution of confirmed Monkeypox cases September 2017–30 October 2022.
| Age Group | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | Total |
|---|---|---|---|---|---|---|---|
| 0–10 Years | 7 | 5 | 1 | 0 | 1 | 98 | 112 |
| 11–20 Years | 12 | 4 | 1 | 0 | 4 | 96 | 117 |
| 21–30 Years | 34 | 13 | 13 | 4 | 10 | 147 | 221 |
| 31–40 Years | 26 | 17 | 22 | 4 | 13 | 171 | 253 |
| 41–50 Years | 9 | 10 | 9 | 0 | 5 | 68 | 101 |
| 51–60 Years | 0 | 0 | 1 | 0 | 1 | 24 | 26 |
| Total | 88 | 49 | 47 | 8 | 34 | 604 | 830 |
Source: NCDC, 2022 [16].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ekpunobi, N.; Akinsuyi, O.; Ariri, T.; Ogunmola, T. The Reemergence of Monkeypox in Nigeria. Challenges 2023, 14, 22. https://doi.org/10.3390/challe14020022
AMA Style
Ekpunobi N, Akinsuyi O, Ariri T, Ogunmola T. The Reemergence of Monkeypox in Nigeria. Challenges. 2023; 14(2):22. https://doi.org/10.3390/challe14020022
Chicago/Turabian StyleEkpunobi, Nzube, Oluwamayowa Akinsuyi, Theresa Ariri, and Temitope Ogunmola. 2023. "The Reemergence of Monkeypox in Nigeria" Challenges 14, no. 2: 22. https://doi.org/10.3390/challe14020022
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.