
Relationships of First-Trimester Body Mass Index and Weight Change with Persistent Organic Pollutant Concentrations in Pregnant Canadian Individuals
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data and Sample Collection
2.3. Statistical Analysis
3. Ethical Approval
4. Results
4.1. Characteristics of Study Participants
4.2. First-Trimester POP Levels
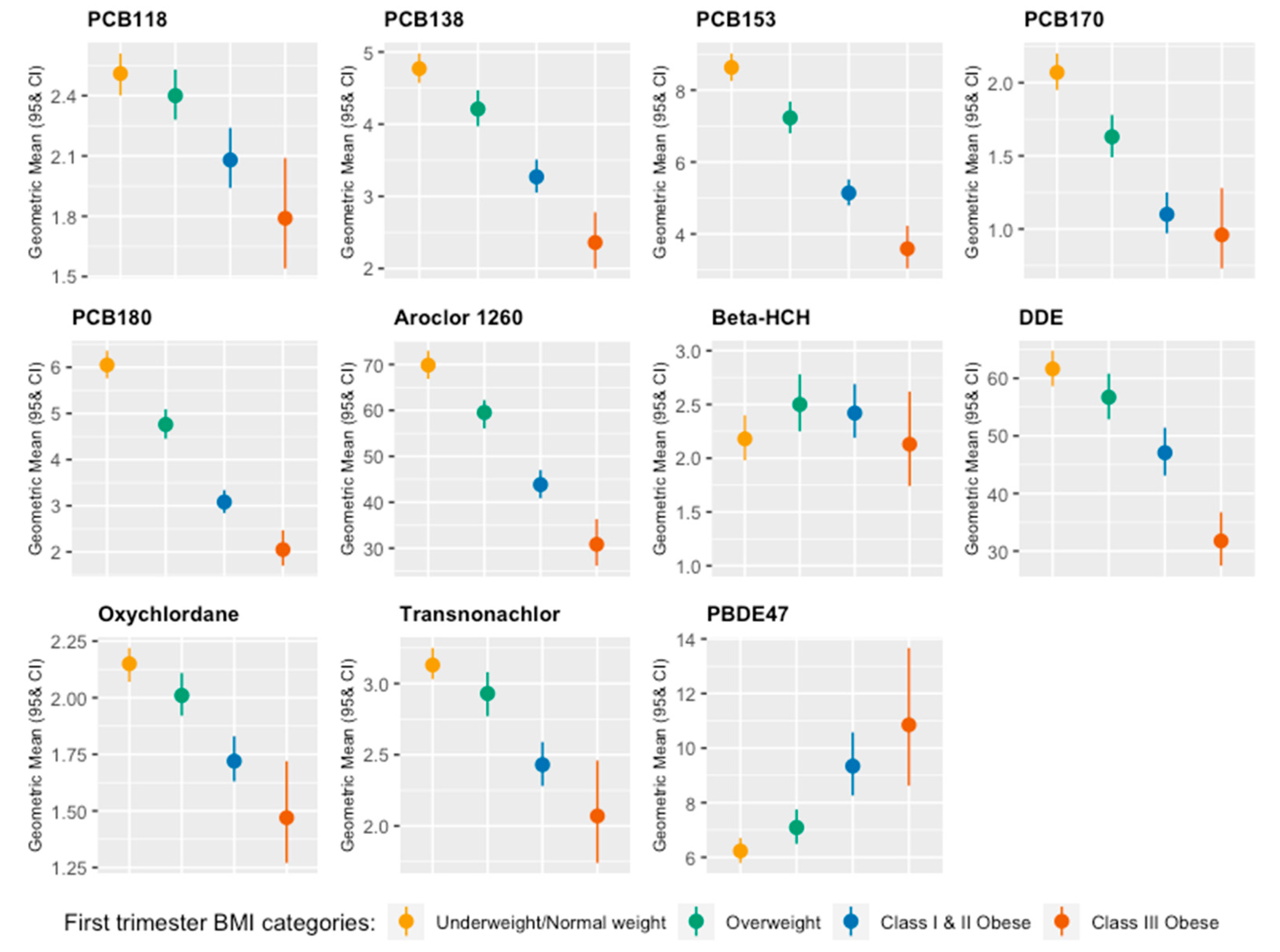
4.3. POP Levels and First-Trimester BMI
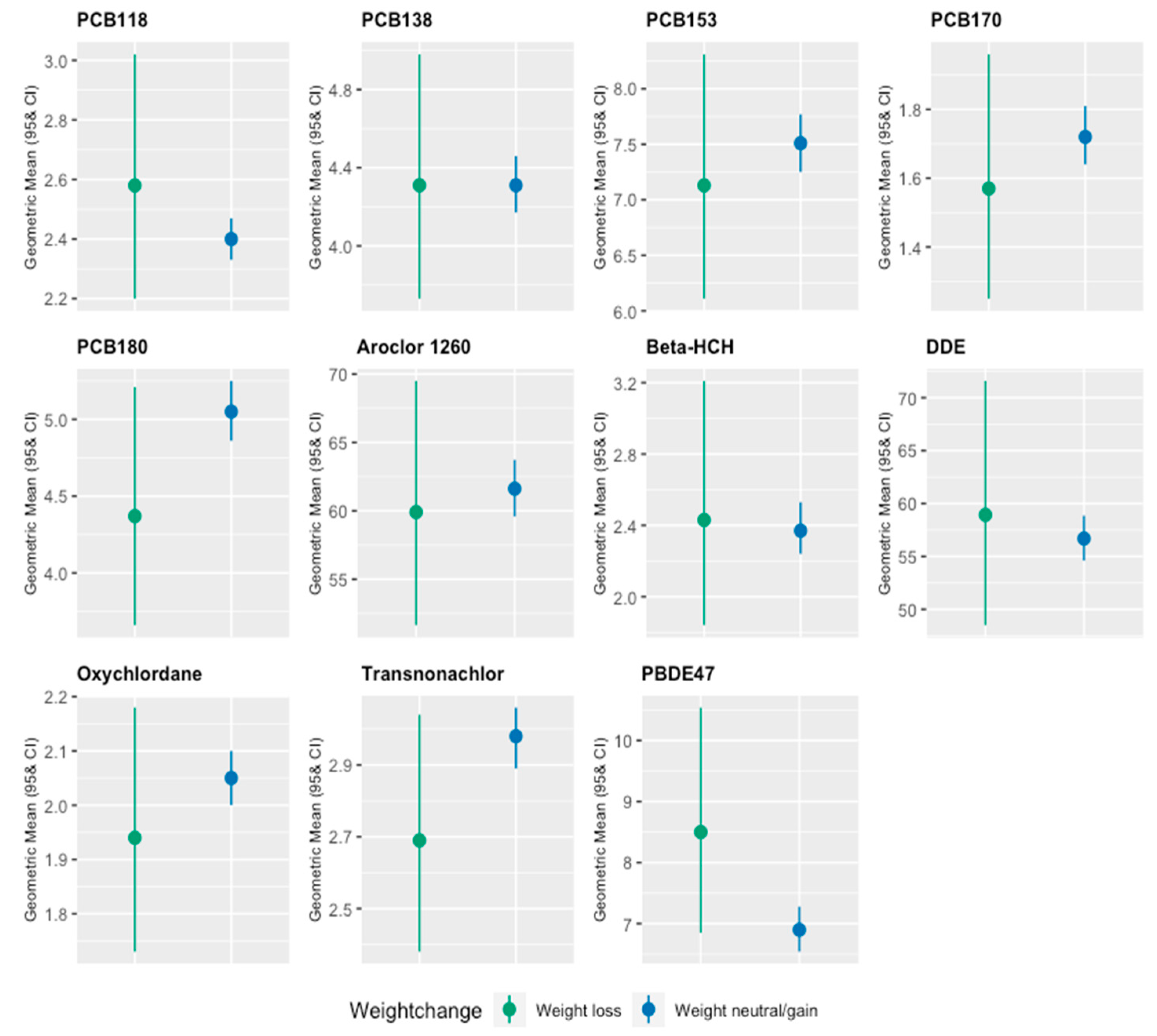
4.4. POP Levels and Early Pregnancy Weight Change
5. Discussion
5.1. Summary of Findings and Clinical Significance of the Findings
5.2. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Beta-HCH | Beta-Hexachlorocyclohexane |
| BMI | Body Mass Index |
| DDE | Dichlorodiphenyldichloroethylene |
| DDT | Dichlorodiphenyltrichloroethane |
| GWG | Gestational Weight Gain |
| LOD | Limit of Detection |
| MIREC | Maternal-Infant Research on Environmental Chemicals |
| PBB | Polybrominated biphenyl |
| PBDE | Polybrominated diphenyl ether |
| PCB | Polychlorinated biphenyl |
| POP | Persistent Organic Pollutant |
References
- Arendas, K.; Qiu, Q.; Gruslin, A. Obesity in pregnancy: Pre-conceptional to postpartum consequences. J. Obstet. Gynaecol. Can. 2008, 30, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Crane, J.M.G.; Murphy, P.; Burrage, L.; Hutchens, D. Maternal and perinatal outcomes of extreme obesity in pregnancy. J. Obstet. Gynaecol. Can. 2013, 35, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, S.C.; Pearce, J.; Ellis, S. Overweight, obesity and excessive weight gain in pregnancy as risk factors for adverse pregnancy outcomes: A narrative review. J. Hum. Nutr. Diet. 2022, 35, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Block, S.R.; Watkins, S.M.; Salemi, J.L.; Rutkowski, R.; Correia, J.A.; Kirby, R.S. Maternal pre-pregnancy body mass index and risk of selected birth defects: Evidence of a dose-response relationship. Paediatr. Perinat. Epidemiol. 2013, 27, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Neri, C.; Serafino, E.; Morlando, M.; Familiari, A. Microbiome and Gestational Diabetes: Interactions with Pregnancy Outcome and Long-Term Infant Health. J. Diabetes Res. 2021, 2021, 9994734. [Google Scholar] [CrossRef] [PubMed]
- LifeCycle Project-Maternal Obesity and Childhood Outcomes Study Group; Voerman, E.; Santos, S.; Inskip, H.; Amiano, P.; Barros, H.; Charles, M.A.; Chatzi, L.; Chrousos, G.P.; Corpeleijn, E.; et al. Association of Gestational Weight Gain With Adverse Maternal and Infant Outcomes. JAMA 2019, 321, 1702–1715. [Google Scholar] [CrossRef] [Green Version]
- Maxwell, C.; Gaudet, L.; Cassir, G.; Nowik, C.; McLeod, N.L.; Jacob, C.É.; Walker, M. Guideline No. 391-Pregnancy and Maternal Obesity Part 1: Pre-conception and Prenatal Care. J. Obstet. Gynaecol. Can. 2019, 41, 1623–1640. [Google Scholar] [CrossRef]
- Health Canada. Prenatal Nutrition Guidelines for Health Professionals, Background on Canada’s Food Guide. 2010. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/fn-an/alt_formats/pdf/nutrition/prenatal/ewba-mbsa-eng.pdf (accessed on 1 November 2022).
- Woolcott, C.; Dodds, L.; Ashley-Martin, J.; Piccinini-Vallis, H. Distribution of pregnancy-related weight measures. Can. Fam. Phys. 2016, 62, e400–e406. [Google Scholar]
- Lim, J.S.; Son, H.K.; Park, S.K.; Jacobs, D.R.; Lee, D.H. Inverse associations between long-term weight change and serum concentrations of persistent organic pollutants. Int. J. Obes. 2011, 35, 744–747. [Google Scholar] [CrossRef] [Green Version]
- Malarvannan, G.; Van Hoorenbeeck, K.; Deguchtenaere, A.; Verhulst, S.L.; Dirinck, E.; Van Gaal, L.; Jorens, P.G.; Covaci, A. Dynamics of persistent organic pollutants in obese adolescents during weight loss. Environ. Int. 2018, 110, 80–87. [Google Scholar] [CrossRef]
- Pestana, D.; Faria, G.; Sá, C.; Fernandes, V.C.; Teixeira, D.; Norberto, S.; Faria, A.; Meireles, M.; Marques, C.; Correia-Sá, L.; et al. Persistent organic pollutant levels in human visceral and subcutaneous adipose tissue in obese individuals—Depot differences and dysmetabolism implications. Environ. Res. 2014, 133, 170–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagen, P.; Walls, M.P. The Stockholm Convention on Persistent Organic Pollutants. Nat. Resour. Environ. 2005, 19, 49–52. [Google Scholar] [CrossRef]
- Ruzzin, J. Public health concern behind the exposure to persistent organic pollutants and the risk of metabolic diseases. BMC Public Health 2012, 12, 298. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization. Persistent Organic Pollutants: Impact on Child. Health. 2010. Available online: https://www.who.int/publications/i/item/persistent-organic-pollutants-impact-on-child-health (accessed on 1 November 2022).
- Adlard, B.; Davis, K.; Liang, C.L.; Curren, M.S.; Rodríguez-Dozal, S.; Riojas-Rodríguez, H.; Hernández-Ávila, M.; Foster, W.; Needham, L.; Wong, L.Y.; et al. Persistent organic pollutants (POPs) and metals in primiparous women: A comparison from Canada and Mexico. Sci. Total Environ. 2014, 500–501, 302–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerregaard-Olesen, C.; Long, M.; Ghisari, M.; Bech, B.H.; Nohr, E.A.; Uldbjerg, N.; Henriksen, T.B.; Olsen, J.; Bonefeld-Jørgensen, E.C. Temporal trends of lipophilic persistent organic pollutants in serum from Danish nulliparous pregnant women 2011–2013. Environ. Sci. Pollut. Res. Int. 2017, 24, 16592–16603. [Google Scholar] [CrossRef]
- Helou, K.; Matta, J.; Harmouche-Karaki, M.; Sayegh, N.; Younes, H.; Mahfouz, Y.; Mahfouz, M.; Karake, S.; Finan, R.; Abi-Tayeh, G.; et al. Maternal and cord serum levels of polychlorinated biphenyls (PCBs) and organochlorine pesticides (OCPs) among Lebanese pregnant women and predictors of exposure. Chemosphere 2021, 266, 129211. [Google Scholar] [CrossRef] [PubMed]
- Vizcaino, E.; Grimalt, J.O.; Glomstad, B.; Fernández-Somoano, A.; Tardón, A. Gestational weight gain and exposure of newborns to persistent organic pollutants. Environ. Health Perspect. 2014, 122, 873–879. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.Y.; Jain, R.B.; Wolkin, A.F.; Rubin, C.H.; Needham, L.L. Serum concentrations of selected persistent organic pollutants in a sample of pregnant females and changes in their concentrations during gestation. Environ. Health Perspect. 2009, 117, 1244–1249. [Google Scholar] [CrossRef]
- Longnecker, M.P.; Klebanoff, M.A.; Zhou, H.; Brock, J.W. Association between maternal serum concentration of the DDT metabolite DDE and preterm and small-for-gestational-age babies at birth. Lancet 2001, 358, 110–114. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, M.J.; Dadvand, P.; Grellier, J.; Martinez, D.; Vrijheid, M. Environmental risk factors of pregnancy outcomes: A summary of recent meta-analyses of epidemiological studies. Environ. Health 2013, 12, 6. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Principles for Evaluating Health Risks in Children Associated with Exposure to Chemicals. 2006. Available online: https://apps.who.int/iris/handle/10665/43604 (accessed on 1 August 2022).
- Fisher, M.; Arbuckle, T.E.; Liang, C.L.; LeBlanc, A.; Gaudreau, E.; Foster, W.G.; Haines, D.; Davis, K.; Fraser, W.D. Concentrations of persistent organic pollutants in maternal and cord blood from the maternal-infant research on environmental chemicals (MIREC) cohort study. Environ. Health A Glob. Access Sci. Source 2016, 15, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Arbuckle, T.E.; Fraser, W.D.; Fisher, M.; Davis, K.; Liang, C.L.; Lupien, N.; Bastien, S.; Velez, M.P.; von Dadelszen, P.; Hemmings, D.G.; et al. Cohort profile: The maternal-infant research on environmental chemicals research platform. Paediatr. Perinat. Epidemiol. 2013, 27, 415–425. [Google Scholar] [CrossRef]
- Mehta, S.S.; Applebaum, K.M.; James-Todd, T.; Coleman-Phox, K.; Adler, N.; Laraia, B.; Epel, E.; Parry, E.; Wang, M.; Park, J.S.; et al. Associations between sociodemographic characteristics and exposures to PBDEs, OH-PBDEs, PCBs, and PFASs in a diverse, overweight population of pregnant women. J. Expo. Sci. Environ. Epidemiol. 2020, 30, 42–55. [Google Scholar] [CrossRef]
- Williamson, E.J.; Aitken, Z.; Lawrie, J.; Dharmage, S.C.; Burgess, J.A.; Forbes, A.B. Introduction to causal diagrams for confounder selection. Respirology 2014, 19, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Helsel, D.R. Chapter 13: Multivariate Methods for Censored Data. In Statistics for Censored Environmental Data Using Minitab and R; John Wiley & Sons: Hoboken, NJ, USA, 2011; pp. 268–296. [Google Scholar]
- Government of Canada. Third Report on Human Biomonitoring of Environmental Chemicals in Canada. 2015. Available online: https://www.canada.ca/content/dam/hc-sc/migration/hc-sc/ewh-semt/alt_formats/pdf/pubs/contaminants/chms-ecms-cycle3/chms-ecms-cycle3-eng.pdf (accessed on 1 November 2022).
- Centers for Disease Control and Prevention (CDC). Fourth National Report on Human Exposure to Environmental Chemicals. 2021. Available online: https://ecologycenter.org/wp-content/uploads/2021/04/FourthReport_UpdatedTables_Volume2_Mar2021-508.pdf (accessed on 1 November 2022).
- Vafeiadi, M.; Georgiou, V.; Chalkiadaki, G.; Rantakokko, P.; Kiviranta, H.; Karachaliou, M.; Fthenou, E.; Venihaki, M.; Sarri, K.; Vassilaki, M.; et al. Association of Prenatal Exposure to Persistent Organic Pollutants with Obesity and Cardiometabolic Traits in Early Childhood: The Rhea Mother-Child Cohort (Crete, Greece). Environ. Health Perspect. 2015, 123, 1015–1021. [Google Scholar] [CrossRef] [PubMed]
- Adetona, O.; Horton, K.; Sjodin, A.; Jones, R.; Hall, D.B.; Aguillar-Villalobos, M.; Cassidy, B.E.; Vena, J.E.; Needham, L.L.; Naeher, L.P. Concentrations of select persistent organic pollutants across pregnancy trimesters in maternal and in cord serum in Trujillo, Peru. Chemosphere 2013, 91, 1426–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, W.G.; Cheung, A.P.; Davis, K.; Graves, G.; Jarrell, J.; Leblanc, A.; Liang, C.L.; Leech, T.; Walker, M.; Weber, J.P.; et al. Circulating metals and persistent organic pollutant concentrations in Canadian and non-Canadian born primiparous women from five Canadian centres: Results of a pilot biomonitoring study. Sci. Total Environ. 2012, 435–436, 326–336. [Google Scholar] [CrossRef]
- Glynn, A.; Aune, M.; Darnerud, P.O.; Cnattingius, S.; Bjerselius, R.; Becker, W.; Lignell, S. Determinants of serum concentrations of organochlorine compounds in Swedish pregnant women: A cross-sectional study. Environ. Health 2007, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Dirinck, E.; Jorens, P.G.; Covaci, A.; Geens, T.; Roosens, L.; Neels, H.; Mertens, I.; Van Gaal, L. Obesity and persistent organic pollutants: Possible obesogenic effect of organochlorine pesticides and polychlorinated biphenyls. Obes. (Silver Spring) 2011, 19, 709–714. [Google Scholar] [CrossRef]
- Vuong, A.M.; Braun, J.M.; Sjödin, A.; Webster, G.M.; Yolton, K.; Lanphear, B.P.; Chen, A. Prenatal Polybrominated Diphenyl Ether Exposure and Body Mass Index in Children Up To 8 Years of Age. Environ. Health Perspect. 2016, 124, 1891–1897. [Google Scholar] [CrossRef] [Green Version]
- Jansen, A.; Lyche, J.L.; Polder, A.; Aaseth, J.; Skaug, M.A. Increased blood levels of persistent organic pollutants (POP) in obese individuals after weight loss—A review. J. Toxicol. Environ. Health Part B Crit. Rev. 2017, 20, 22–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaacks, L.M.; Boyd Barr, D.; Sundaram, R.; Grewal, J.; Zhang, C.; Buck Louis, G.M. Pre-Pregnancy Maternal Exposure to Persistent Organic Pollutants and Gestational Weight Gain: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2016, 13, 905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashley-Martin, J.; Dodds, L.; Arbuckle, T.E.; Morisset, A.S.; Fisher, M.; Bouchard, M.F.; Shapiro, G.D.; Ettinger, A.S.; Monnier, P.; Dallaire, R.; et al. Maternal and Neonatal Levels of Perfluoroalkyl Substances in Relation to Gestational Weight Gain. Int. J. Environ. Res. Public Health 2016, 13, 146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Headen, I.; Cohen, A.K.; Mujahid, M.; Abrams, B. The accuracy of self-reported pregnancy-related weight: A systematic review. Obes. Rev. 2017, 18, 350–369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | N | % |
|---|---|---|
| Maternal age | ||
| <25 | 139 | 7.01 |
| 25–29 | 459 | 23.15 |
| 30–34 | 709 | 35.75 |
| 35+ | 676 | 34.09 |
| Maternal education a | ||
| High school or less | 175 | 8.83 |
| Some college or college degree | 572 | 28.87 |
| Undergraduate degree or higher | 1234 | 62.29 |
| Marital status | ||
| Married or common law | 1889 | 95.26 |
| Other | 94 | 4.74 |
| Maternal race | ||
| Caucasian | 1661 | 83.76 |
| Not Caucasian | 322 | 16.24 |
| Place of birth | ||
| Canada | 1612 | 81.29 |
| Other | 371 | 18.71 |
| Income | ||
| <$50,000 | 347 | 17.5 |
| $50,001–$100,000 | 786 | 39.64 |
| >$100,000 | 757 | 38.17 |
| Missing | 93 | 4.69 |
| Smoking status b | ||
| Current | 237 | 11.96 |
| Former c | 542 | 27.36 |
| Never | 1202 | 60.68 |
| Pre-pregnancy BMI d | ||
| Underweight (<18.5 kg/m2) | 52 | 2.83 |
| Normal weight (18.5–<25.0 kg/m2) | 1106 | 60.21 |
| Overweight (25.0–<30.0 kg/m2) | 404 | 21.99 |
| Obese (≥30.0 kg/m2) | 275 | 14.97 |
| First-trimester BMI e | ||
| Underweight/Normal weight (<18.5–<25.0 kg/m2) | 1013 | 52.98 |
| Overweight (25.0–<30.0 kg/m2) | 530 | 27.72 |
| Class I & II obese (30.0–<40.0 kg/m2) | 311 | 16.27 |
| Class III obese (≥40.0 kg/m2) | 58 | 3.03 |
| Weight change category f | ||
| Weight loss | 72 | 3.93 |
| Weight neutral or gain | 1760 | 96.07 |
| Parity | ||
| 0 | 876 | 44.18 |
| 1 | 800 | 40.34 |
| 2 | 231 | 11.65 |
| 3+ | 76 | 3.83 |
| Fasting status | ||
| No | 1914 | 98.00 |
| Yes | 39 | 2.00 |
| Season of blood collection (first trimester) | ||
| Spring | 448 | 22.92 |
| Summer | 464 | 23.73 |
| Fall | 575 | 29.41 |
| Winter | 468 | 23.94 |
| Gestational age at first-trimester visit (mean ± SD; wks) | 11.56 (1.58) | |
| POP | LOD | % <LOD | Maximum Value | KM Median (95% CI) | GM (95% CI) |
|---|---|---|---|---|---|
| Polychlorinated biphenyl (PCB) | |||||
| PCB28 | 0.05 | 99.74 | 260.00 | NE | NE |
| PCB66 | 0.03 | 99.28 | 28.00 | NE | NE |
| PCB74 | 0.03 | 96.54 | 18.40 | NE | NE |
| PCB99 | 0.03 | 97.16 | 12.93 | NE | NE |
| PCB101 | 0.03 | 99.90 | 12.06 | NE | NE |
| PCB105 | 0.01 | 95.71 | 13.62 | NE | NE |
| PCB118 | 0.01 | 26.61 | 37.93 | 2.30 (2.23, 2.38) | 2.35 (2.29, 2.43) |
| PCB128 | 0.01 | 99.79 | 5.00 | NE | NE |
| PCB138 | 0.01 | 7.03 | 71.66 | 4.01 (3.92, 4.21) | 4.21 (4.08, 4.37) |
| PCB146 | 0.01 | 85.43 | 16.00 | NE | NE |
| PCB153 | 0.01 | 1.29 | 155.00 | 7.00 (6.72, 7.29) | 7.30 (7.06, 7.54) |
| PCB156 | 0.01 | 79.07 | 17.46 | NE | NE |
| PCB163 | 0.01 | 68.11 | 23.81 | NE | NE |
| PCB167 | 0.01 | 98.41 | 4.48 | NE | NE |
| PCB170 | 0.01 | 46.82 | 71.66 | 1.55 (1.29, 1.67) | 1.67 (1.58, 1.75) |
| PCB178 | 0.01 | 95.71 | 9.02 | NE | NE |
| PCB180 | 0.01 | 7.39 | 183.33 | 4.72 (4.52, 4.90) | 4.87 (4.70, 5.05) |
| PCB183 | 0.01 | 91.21 | 23.33 | NE | NE |
| PCB187 | 0.01 | 57.21 | 45.00 | NE | NE |
| PCB194 | 0.01 | 81.17 | 30.00 | NE | NE |
| PCB203 | 0.01 | 89.35 | 14.16 | NE | NE |
| PCB201 | 0.01 | 83.72 | 20.00 | NE | NE |
| PCB206 | 0.01 | 97.67 | 6.61 | NE | NE |
| Aroclor 1260 | 0.1 | 2.69 | 1183.33 | 57.45 (55.29, 59.65) | 60.00 (58.11, 61.95) |
| Organochlorines | |||||
| Beta-HCH | 0.01 | 31.88 | 1108.11 | 2.24 (2.16, 2.31) | 2.32 (2.19, 2.46) |
| Cis-nonachlor | 0.005 | 88.31 | 3.91 | NE | NE |
| DDE | 0.09 | 1.03 | 5306.12 | 48.33 (46.67, 50.00) | 56.01 (54.02, 58.07) |
| DDT | 0.05 | 96.28 | 175.44 | NE | NE |
| HCB | 0.04 | 69.54 | 101.66 | NE | NE |
| Mirex | 0.01 | 91.83 | 38.03 | NE | NE |
| Oxychlordane | 0.005 | 7.81 | 17.50 | 2.09 (2.00, 2.15) | 2.00 (1.95, 2.05) |
| Parlar26 | 0.005 | 97.47 | 3.64 | NE | NE |
| Parlar50 | 0.005 | 87.28 | 5.00 | NE | NE |
| Transnonachlor | 0.01 | 15.87 | 34.33 | 2.89 (2.69, 3.02) | 2.90 (2.82, 2.98) |
| Polybrominated diphenyl ethers (PBDE) & Hexabromobiphenyl (PBB) | |||||
| PBB153 | 0.02 | 99.48 | 13.61 | NE | NE |
| PBDE100 | 0.02 | 78.46 | 327.27 | NE | NE |
| PBDE153 | 0.02 | 55.60 | 527.27 | NE | NE |
| PBDE28 | 0.03 | 99.07 | 27.14 | NE | NE |
| PBDE33 | 0.03 | 99.90 | 6.28 | NE | NE |
| PBDE47 | 0.03 | 34.28 | 727.27 | 6.97 (6.55, 7.31) | 7.02 (6.68, 7.38) |
| PBDE99 | 0.02 | 80.85 | 169.09 | NE | NE |
| POP | Overweight | Class I & II Obese | Class III Obese | |||
|---|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| PCB118 | −0.058 (−0.127, 0.011) | −0.045 (−0.108, 0.018) | −0.199 (−0.282, −0.115) | −0.083 (−0.162, −0.003) | −0.371 (−0.548, −0.195) | −0.181 (−0.347, −0.014) |
| PCB138 | −0.124 (−0.196, −0.052) | −0.106 (−0.169, −0.044) | −0.381 (−0.469, −0.293) | −0.253 (−0.331, −0.174) | −0.716 (−0.900, −0.531) | −0.475 (−0.638, −0.311) |
| PCB153 | −0.176 (−0.251, −0.102) | −0.157 (−0.219, −0.095) | −0.518 (−0.608, −0.427) | −0.379 (−0.456, −0.303) | −0.881 (−1.068, −0.695) | −0.640 (−0.800, −0.481) |
| PCB170 | −0.241 (−0.340, −0.142) | −0.223 (−0.309, −0.137) | −0.721 (−0.852, −0.589) | −0.557 (−0.674, −0.439) | −1.137 (−1.452, −0.821) | −0.835 (−1.117, −0.553) |
| PCB180 | −0.241 (−0.323, −0.158) | −0.228 (−0.295, −0.161) | −0.683 (−0.783, −0.582) | −0.544 (−0.629, −0.459) | −1.114 (−1.328, −0.899) | −0.885 (−1.068, −0.702) |
| Aroclor 1260 | −0.160 (−0.233, −0.087) | −0.141 (−0.202, −0.079) | −0.468 (−0.557, −0.379) | −0.333 (−0.410, −0.256) | −0.825 (−1.009, −0.640) | −0.583 (−0.743, −0.423) |
| Beta-HCH | 0.065 (−0.070, 0.201) | 0.101 (−0.006, 0.209) | −0.026 (−0.187, 0.138) | 0.225 (−0.092, 0.359) | −0.221 (−0.565, 0.123) | 0.296 (−0.019, 0.574) |
| DDE | −0.083 (−0.168, 0.002) | −0.053 (−0.124, 0.018) | −0.269 (−0.372, −0.167) | −0.118 (−0.206, −0.030) | −0.672 (−0.884, −0.459) | −0.368 (−0.549, −0.187) |
| Oxychlordane | −0.064 (−0.122, −0.006) | −0.062 (−0.115, −0.010) | −0.219 (−0.289, −0.149) | −0.163 (−0.228, −0.097) | −0.373 (−0.519, −0.226) | −0.261 (−0.397, −0.125) |
| Transnonachlor | −0.064 (−0.126, −0.002) | −0.066 (−0.122, −0.010) | −0.258 (−0.334, −0.182) | −0.191 (−0.261, −0.122) | −0.403 (−0.561, −0.244) | −0.282 (−0.428, −0.136) |
| PBDE47 | 0.103 (−0.011, 0.217) | 0.086 (−0.029, 0.201) | 0.402 (0.266, 0.537) | 0.362 (0.222, 0.502) | 0.528 (0.254, 0.802) | 0.460 (0.177, 0.743) |
| Weight Loss | ||
|---|---|---|
| Unadjusted | Adjusted | |
| PCB118 | 0.075 (−0.080, 0.230) | 0.144 (−0.003, 0.291) |
| PCB138 | −0.002 (−0.168, 0.164) | 0.146 (0.0003, 0.292) |
| PCB153 | −0.052 (−0.226, 0.121) | 0.143 (−0.001, 0.288) |
| PCB170 | −0.152 (−0.391, 0.087) | 0.112 (−0.098, 0.323) |
| PCB180 | −0.148 (−0.343, 0.045) | 0.134 (−0.024, 0.293) |
| Aroclor 1260 | −0.028 (−0.198, 0.141) | 0.148 (0.004, 0.292) |
| Beta-HCH | −0.008 (−0.314, 0.297) | 0.019 (−0.226, 0.254) |
| DDE | 0.039 (−0.152, 0.229) | 0.123 (−0.038, 0.285) |
| Oxychlordane | −0.056 (−0.187, 0.074) | 0.031 (−0.091, 0.152) |
| Transnonachlor | −0.112 (−0.254, 0.029) | 0.015 (−0.115, 0.144) |
| PBDE47 | 0.172 (−0.083, 0.426) | −0.008 (−0.273, 0.258) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levesque, M.; Ouedraogo, M.; Fakhraei, R.; Dingwall Harvey, A.; Bratton, E.; Walker, M.; Dodds, L.; Gaudet, L. Relationships of First-Trimester Body Mass Index and Weight Change with Persistent Organic Pollutant Concentrations in Pregnant Canadian Individuals. Challenges 2023, 14, 13. https://doi.org/10.3390/challe14010013
Levesque M, Ouedraogo M, Fakhraei R, Dingwall Harvey A, Bratton E, Walker M, Dodds L, Gaudet L. Relationships of First-Trimester Body Mass Index and Weight Change with Persistent Organic Pollutant Concentrations in Pregnant Canadian Individuals. Challenges. 2023; 14(1):13. https://doi.org/10.3390/challe14010013
Chicago/Turabian StyleLevesque, Marianne, Mariame Ouedraogo, Romina Fakhraei, Alysha Dingwall Harvey, Elizabeth Bratton, Mark Walker, Linda Dodds, and Laura Gaudet. 2023. "Relationships of First-Trimester Body Mass Index and Weight Change with Persistent Organic Pollutant Concentrations in Pregnant Canadian Individuals" Challenges 14, no. 1: 13. https://doi.org/10.3390/challe14010013