Spiritual Needs of Patients with Chronic Diseases



{kind=link}
{kind=link}
Abstract
:1. Background
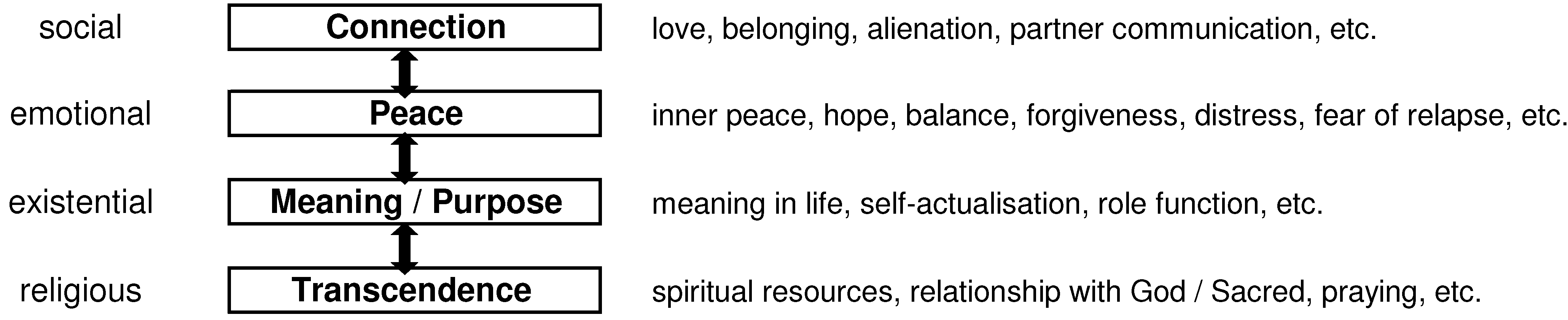
2. Needs of Patients with Chronic Diseases

3. Quantification of Spiritual Needs in Patients with Chronic Diseases
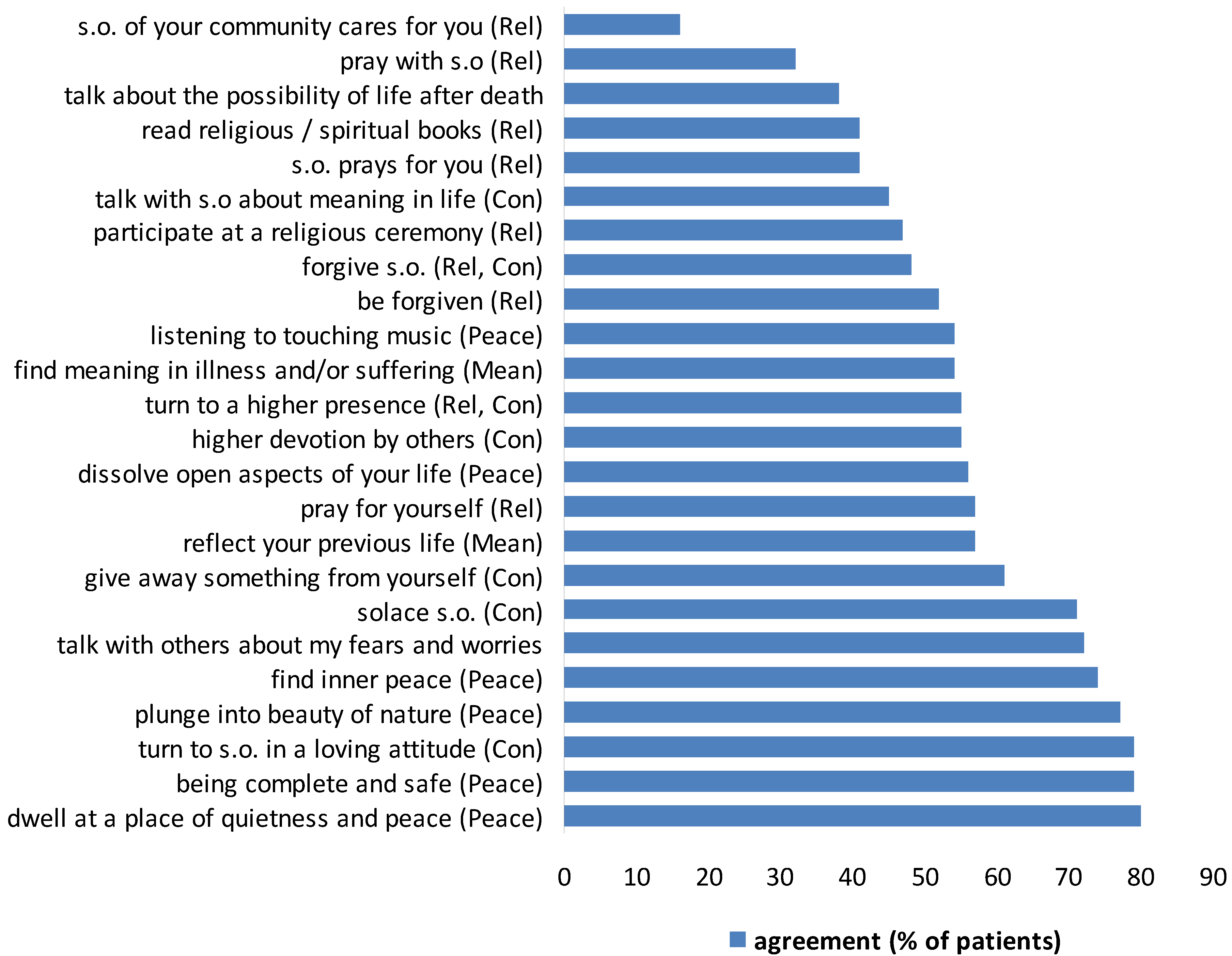
3.1. Findings

3.2. Interpretation
4. Addressing Spiritual Needs as an Approach in Health Care
5. Conclusions
Acknowledgements
References
- A. Büssing, J. Fischer, T. Ostermann, and P.F. Matthiesen. “Reliance on God´s help, depression and fatigue in female cancer patients.” Int. J. Psychiatry Med. 38 (2008): 357–372. [Google Scholar] [CrossRef] [PubMed]
- A. Büssing, A. Michalsen, H.J. Balzat, R.A. Grünther, T. Ostermann, E.A. Neugebauer, and P.F. Matthiessen. “Are spirituality and religiosity resources for patients with chronic pain conditions? ” Pain Med. 10 (2009): 327–339. [Google Scholar] [CrossRef] [PubMed]
- R. Hebert, B. Zdaniuk, R. Schulz, and M. Scheier. “Positive and negative religious coping and well-being in women with breast cancer.” J. Palliat. Med. 12 (2009): 537–545. [Google Scholar] [CrossRef] [PubMed]
- R.C. Nairn, and T.V. Merluzzi. “The role of religious coping in adjustment to cancer.” Psychooncology 12 (2003): 428–441. [Google Scholar] [CrossRef] [PubMed]
- A.C. Phelps, P.K. Maciejewski, M. Nilsson, T.A. Balboni, A.A. Wright, M.E. Paulk, E. Trice, D. Schrag, J.R. Peteet, S.D. Block, and H.G. Prigerson. “Religious coping and use of intensive life-prolonging care near death in patients with advanced cancer.” JAMA 301 (2009): 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- K. Ross, P.J. Handal, E.M. Clark, and J.S. Vander Wal. “The relationship between religion and religious coping: religious coping as a moderator between religion and adjustment.” J. Relig. Health 48 (2009): 454–467. [Google Scholar] [CrossRef] [PubMed]
- I.C. Thune-Boyle, J.A. Stygall, M.R. Keshtgar, and S.P. Newman. “Do religious/spiritual coping strategies affect illness adjustment in patients with cancer? A systematic review of the literature.” Soc. Sci. Med. 63 (2006): 151–164. [Google Scholar] [CrossRef] [PubMed]
- H.G. Koenig, D.A. King, and V.B. Carson. The Handbook of Religion and Health, 2n ed. New York, NY, USA: Oxford University Press, 2011. [Google Scholar]
- C.M. Puchalski. “Addressing the Spiritual Needs of Patients.” In Ethical Issues in Cancer Patient Care. Edited by P. Angelos. New York, NY, USA: Springer, 2009, pp. 79–91. [Google Scholar]
- D.P. Sulmasy. “A biopsychosocial-spiritual model for the care of patients at the end of life.” Gerontologist 42 (2002): 24–33. [Google Scholar] [CrossRef] [PubMed]
- T.A. Balboni, L.C. Vanderwerker, S.D. Block, M.E. Paulk, C.S. Lathan, J.R. Peteet, and H.G. Prigerson. “Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life.” J. Clin. Oncol. 25 (2007): 555–560. [Google Scholar] [CrossRef] [PubMed]
- S.A. Murray, M. Kendall, K. Boyd, A. Worth, and T.F. Benton. “Exploring the spiritual needs of people dying of lung cancer or heart failure: A prospective qualitative interview study of patients and their carers.” Palliat. Med. 18 (2004): 39–45. [Google Scholar] [CrossRef] [PubMed]
- S. Schmid-Buchi, R.J. Halfens, T. Dassen, and B. van den Borne. “A review of psychosocial needs of breast-cancer patients and their relatives.” J. Clin. Nurs. 17 (2008): 2895–2909. [Google Scholar] [CrossRef] [PubMed]
- N.E. Adler, and A.E.K. Page. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs. Washington, DC, USA: The National Academies Press, 2008. [Google Scholar]
- A.H. Maslov. “A Theory of Human Motivation.” Psychol. Rev. 50 (1943): 370–396. [Google Scholar] [CrossRef]
- M.J. Field, and C.K. Cassel. Approaching Death. Improving Care at the End of Life. Washington, DC, USA: National Academy Press, 1997. [Google Scholar]
- T. Koslander, A.B. da Silva, and A. Roxberg. “Existential and spiritual needs in mental health care: An ethical and holistic perspective.” J. Holist. Nurs. 27 (2009): 34–42. [Google Scholar] [CrossRef] [PubMed]
- L.G. Underwood, and J.A. Teresi. “The daily spiritual experience scale: Development, theoretical description, reliability, exploratory factor analysis, and preliminary construct validity using health-related data.” Ann. Behav. Med. 24 (2002): 22–33. [Google Scholar] [CrossRef] [PubMed]
- A. Büssing. ““Spiritualität”- Worüber reden wir? ” In Spiritualität, Krankheit und Heilung – Bedeutung und Ausdrucksformen der Spiritualität in der Medizin. Edited by A. Büssing, T. Ostermann, M. Glöckler and P.F. Matthiessen. Frankfurt, Germany: VAS - Verlag für Akademische Schriften, 2006, pp. 11–24. [Google Scholar]
- A. Büssing, A. Föller-Mancini, J. Gidley, and P. Heusser. “Aspects of Spirituality in Adolescents.” Int. J. Child. Spiritual. 15 (2010): 25–44. [Google Scholar] [CrossRef]
- A. Moadel, C. Morgan, A. Fatone, J. Grennan, J. Carter, G. Laruffa, A. Skummy, and J. Dutcher. “Seeking meaning and hope: Self-reported spiritual and existential needs among an ethnically-diverse cancer patient population.” Psychooncology 8 (1999): 378–385. [Google Scholar] [CrossRef] [PubMed]
- M. Raoul, and C. Rougeron. “Spiritual needs of end of life home care patients: A qualitative study with 13 patients.” J. Int. Bioethique 18 (2007): 63–83. [Google Scholar] [CrossRef] [PubMed]
- D.M. Hampton, D.E. Hollis, D.A. Lloyd, J. Taylor, and S.C. McMillan. “Spiritual needs of persons with advanced cancer.” Am. J. Hosp. Palliat. Care 24 (2007): 42–48. [Google Scholar] [CrossRef] [PubMed]
- J. Yong, J. Kim, S.S. Han, and C.M. Puchalski. “Development and validation of a scale assessing spiritual needs for Korean patients with cancer.” J. Palliat. Care 24 (2008): 240–246. [Google Scholar] [PubMed]
- A. Büssing, H.J. Balzat, and P. Heusser. “Spiritual needs of patients with chronic pain diseases and cancer - validation of the spiritual needs questionnaire.” Eur. J. Med. Res. 15 (2010): 266–273. [Google Scholar] [CrossRef] [PubMed]
- K. Galek, K.J. Flannelly, A. Vane, and R.M. Galek. “Assessing a patient´s spiritual needs. A comprehensive instrument.” Holist. Nurs. Pract. 19 (2005): 62–69. [Google Scholar] [CrossRef] [PubMed]
- A.L. Williams. “Perspectives on spirituality at the end of life: A meta-summary.” Palliat. Support Care 4 (2006): 407–417. [Google Scholar] [CrossRef] [PubMed]
- A. Höcker. “Spiritualität/Religiosität und Lebenssinn bei Krebspatienten.” Thesis at the Institue of Medical Psychology, University Hamburg Eppendorf, 2011. [Google Scholar]
- A. Büssing, A. Kopf, A. Janko, E.A.M. Neugebauer, and P. Heusser. “Psychosocial and spiritual needs of patients with chronic pain conditions.” In Presentation at the American Academy of Pain Medicine’s 27th Annual Meeting, Washington, DC, USA, 24–27 March 2011. in preparation.
- K.J. Flannelly, K. Galek, J. Bucchino, and A. Vane. “The relative prevalence of various spiritual needs.” Scott. J. Healthc. Chaplain. 9 (2006): 25–30. [Google Scholar]
- K.J. Flannelly, K. Galek, A. Vane, and R.M. Galek. “A test of the factor structure of the patients spiritual needs assessment scale.” Holist. Nurs. Pract. 20 (2006): 187–190. [Google Scholar] [CrossRef] [PubMed]
- A.L. Canada, P.E. Murphy, G. Fitchett, A.H. Peterman, and L.R. Schover. “A 3-factor model for the FACIT-Sp.” Psychooncology 17 (2008): 908–916. [Google Scholar] [CrossRef] [PubMed]
- E.H. Erikson. Dimensions of a new identity. New York, NY, USA: Norton, 1974. [Google Scholar]
- B. Bonevski, R. Sanson-Fisher, A. Girgis, L. Burton, P. Cook, and A. Boyes. “Evaluation of an instrument to assess the needs of patients with cancer. Supportive Care Review Group.” Cancer 88 (2000): 217–225. [Google Scholar] [CrossRef] [PubMed]
- A. Girgis, A. Boyes, R.W. Sanson-Fisher, and S. Burrows. “Perceived needs of women diagnosed with breast cancer: Rural versus urban location.” Aust. N Z J Public Health 24 (2000): 166–173. [Google Scholar] [CrossRef] [PubMed]
- K. Rainbird, J. Perkins, R. Sanson-Fisher, I. Rolfe, and P. Anseline. “The needs of patients with advanced, incurable cancer.” Br. J. Cancer 101 (2009): 759–764. [Google Scholar] [CrossRef] [PubMed]
- R. Sanson-Fisher, A. Girgism, A. Boyes, B. Bonevski, L. Burton, and P. Cook. “The unmet supportive care needs of patients with cancer. Supportive Care Review Group.” Cancer 88 (2000): 226–237. [Google Scholar] [CrossRef] [PubMed]
- H.R. Lin, and S.M. Bauer-Wu. “Psycho-spiritual well-being in patients with advanced cancer: An integrative review of the literature.” J. Adv. Nurs. 44 (2003): 69–80. [Google Scholar] [CrossRef] [PubMed]
- A.E. Molzahn, and L. Sheilds. “Why is it so hard to talk about spirituality? ” Can. Nurse. 104 (2008): 25–29. [Google Scholar] [PubMed]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Büssing, A.; Koenig, H.G. Spiritual Needs of Patients with Chronic Diseases. Religions 2010, 1, 18-27. https://doi.org/10.3390/rel1010018
Büssing A, Koenig HG. Spiritual Needs of Patients with Chronic Diseases. Religions. 2010; 1(1):18-27. https://doi.org/10.3390/rel1010018
Chicago/Turabian StyleBüssing, Arndt, and Harold G. Koenig. 2010. "Spiritual Needs of Patients with Chronic Diseases" Religions 1, no. 1: 18-27. https://doi.org/10.3390/rel1010018