A Systematic Review on the Association of Acquired Human Cytomegalovirus Infection with Hearing Loss

 ,
, 
Abstract
:1. Introduction
2. Experimental Section
2.1. Search Strategy
2.2. Research Questions and Selection Criteria
- Population: patients (adults or children) with a clinical diagnosis of progressive or sudden SNHL or tinnitus.
- Intervention: individuals with SNHL or tinnitus were classified according to the evidence of acquired CMV infection. Individuals were defined as cases if they presented SNHL or tinnitus and they had direct or indirect evidence of acquired CMV infection. Direct methods included nucleic acid amplification Polymerase Chain Reaction (PCR) and optimization variants) or in situ hybridization, and indirect methods (IgM and IgG antiviral antibodies and Complement fixation antibodies). Individuals were considered as controls if they did not show any evidence of hearing loss, regardless of previous exposure to CMV.
- Comparison: absolute and relative frequencies of human acquired CMV infection in case and control groups
- Outcome: audiological findings reported in individuals with acquired CMV infection.
- Study-design: case-controlled observational studies that ascertained a history of viral-infection with molecular-based diagnosis.
- Human uncontrolled case series.
- Animal studies.
- Published studies in a language other than English.
- Congenital CMV infection.
2.3. Data Extraction and Variables of Interest
2.4. Quality Assessment of Selected Studies
2.5. Data Synthesis and Meta-Analysis
3. Results
3.1. Study Selection
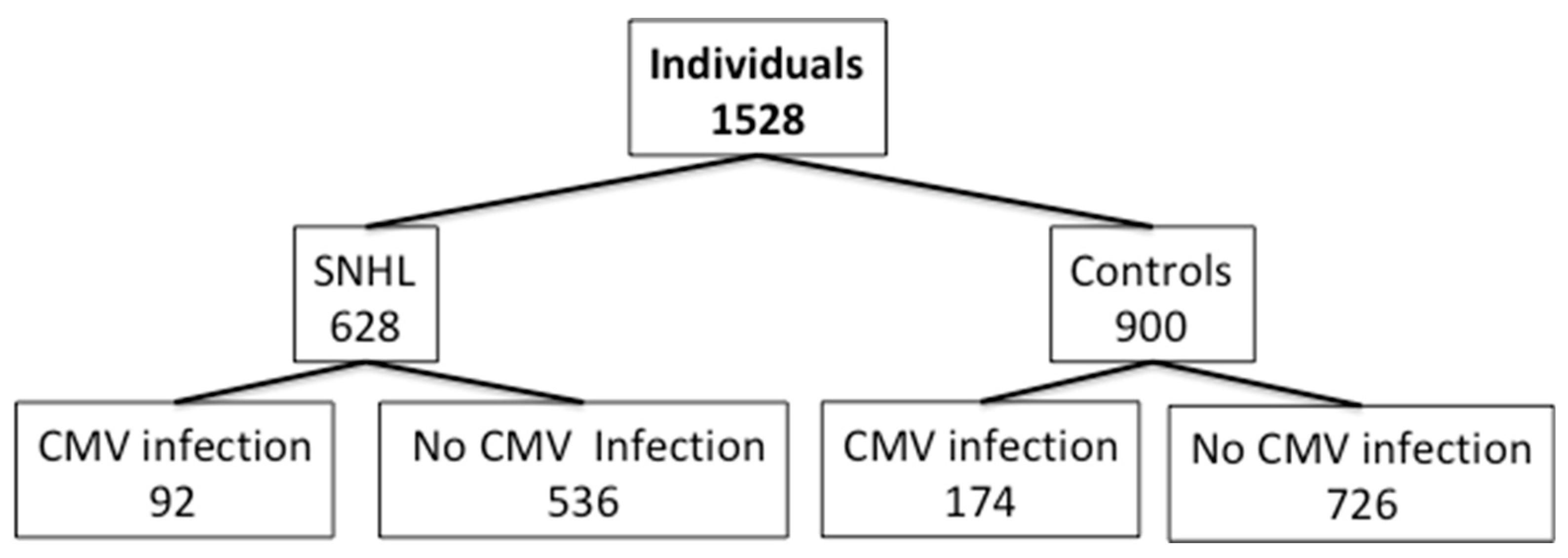
3.2. Sample Description and Audiological Findings
3.3. Methods for the Diagnosis of Human Acquired CMV Infection
3.4. Critical Appraisal
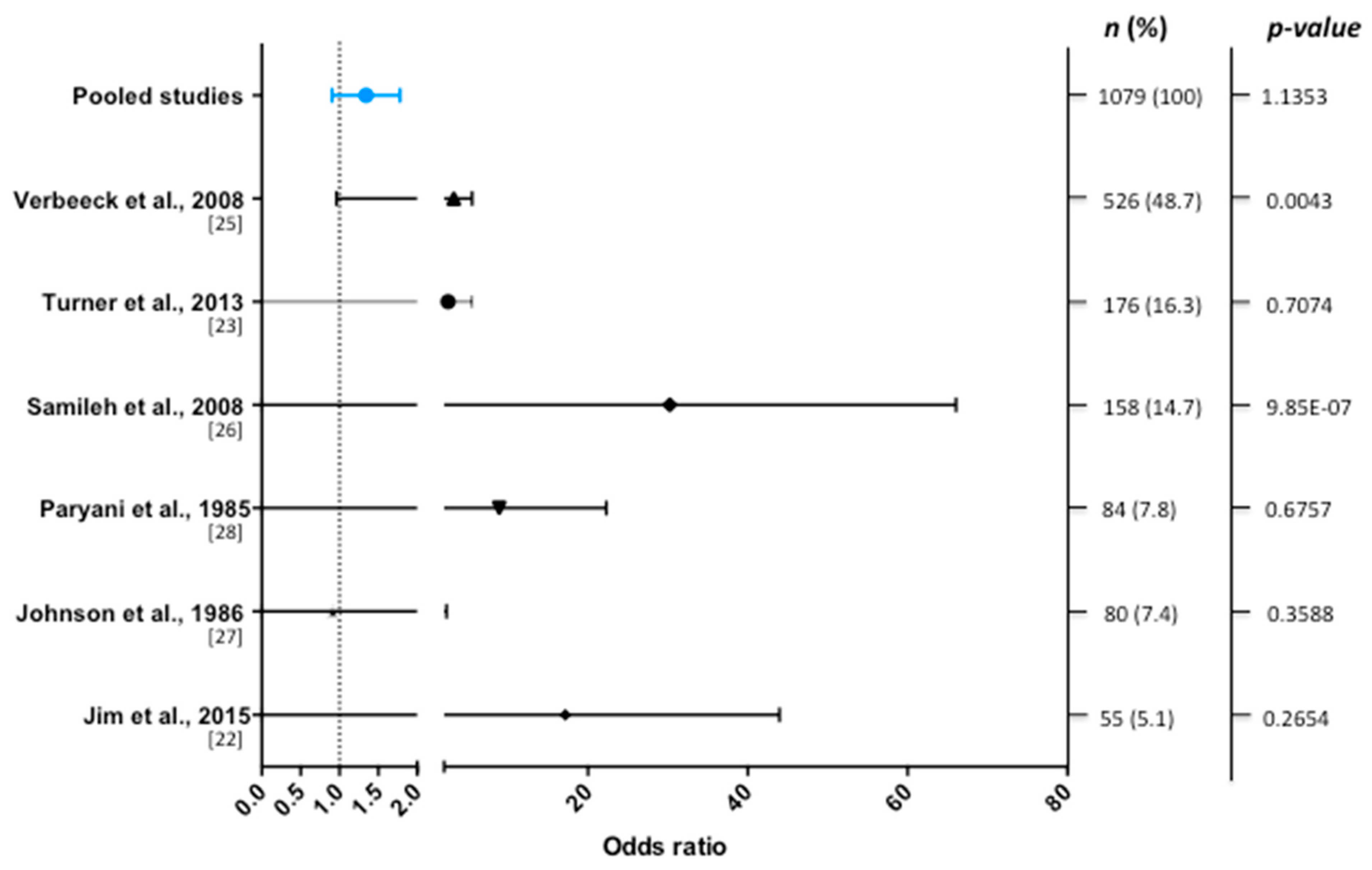
3.5. Data Synthesis and Meta-Analysis
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vancíková, Z.; Dvorák, P. Cytomegalovirus infection in immunocompetent and immunocompromised individuals—A review. Curr. Drug Targets Immune Endocr. Metab. Disord. 2001, 1, 179–187. [Google Scholar] [CrossRef]
- Dupont, L.; Reeves, M.B. Cytomegalovirus latency and reactivation: Recent insights into an age old problem. Rev. Med. Virol. 2016, 26, 75–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poole, E.; Walther, A.; Raven, K.; Benedict, C.A.; Mason, G.M.; Sinclair, J. The myeloid transcription factor GATA-2 regulates the viral UL144 gene during human cytomegalovirus latency in an isolate-specific manner. J. Virol. 2013, 87, 4261–4271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, E.N.; Stool, S. Cytomegalic Inclusion Disease of the Inner Ear. Laryngoscope 1968, 78, 1904–1915. [Google Scholar] [CrossRef]
- Bachor, E.; Sudhoff, H.; Litschel, R.; Karmody, C.S. The pathology of the temporal bones of a child with acquired cytomegalovirus infection: Studies by light microscopy, immunohistochemistry and polymerase-chain reaction. Int. J. Pediatric Otorhinolaryngol. 2000, 55, 215–224. [Google Scholar] [CrossRef]
- Schuknecht, H.F.; Suzuka, Y.; Zimmermann, C. Delayed endolymphatic hydrops and its relationship to Ménière’s disease. Ann. Otol. Rhinol. Laryngol. 1990, 99, 843–853. [Google Scholar] [CrossRef]
- McKenna, M.J.; Kristiansen, A.G.; Haines, J. Polymerase chain reaction amplification of a measles virus sequence from human temporal bone sections with active otosclerosis. Am. J. Otolaryngol. 1996, 17, 827–830. [Google Scholar]
- Kamei, T. Delayed Endolymphatic Hydrops as a Clinical Entity. Int. Tinnitus J. 2004, 10, 137–143. [Google Scholar]
- Lobo, D.; Tuñon, M.; Villarreal, I.; Brea, B.; Garcıa-Berrocal, J.R. Intratympanic gadolinium magnetic resonance imaging supports the role of endolymphatic hydrops in the pathogenesis of immune-mediated inner-ear disease. J. Laryngol. Otol. 2018, 132, 554–559. [Google Scholar] [CrossRef]
- Dean, N.J.; Pastras, C.; Brown, J.D.; Camp, A.J. Are viral-infections associated with Me´nière’s Disease? A systematic review and metaanalysis of molecular-markers of viral-infection in case-controlled observational studies of MD. PLoS ONE 2019, 14, e0225650. [Google Scholar]
- Cannon, M.J.; Schmid, D.S.; Hyde, T.B. Review of cytomegalovirus seroprevalence and demographic.characteristics associated with infection. Rev. Med. Virol. 2010, 20, 202–213. [Google Scholar] [CrossRef] [PubMed]
- Soetens, O.; Vauloup-Fellous, C.; Foulon, I.; Dubreuil, P.; De Saeger, B.; Grangeot-Keros, L.; Naessens, A. Evaluation of different cytomegalovirus (CMV) DNA PCR protocols for analysis of dried blood spots from consecutive cases of neonates with congenital CMV infections. J. Clin. Microbiol. 2008, 46, 943–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbi, M.; MacKay, W.G.; Binda, S.; van Loon, A.M. External quality assessment of cytomegalovirus DNA detection on dried blood spots. BMC Microbiol. 2008, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, C.; Walter, S.; Sharland, M.; Tookey, P.; Luck, S.; Peckham, C.; Griffiths, P. Use of stored dried blood spots for retrospective diagnosis of congenital CMV. J. Med. Virol. 2009, 81, 1394–1398. [Google Scholar] [CrossRef]
- Bale, J.F., Jr. Human cytomegalovirus infection and disorders of the nervous system. Arch. Neurol. 1984, 41, 310–320. [Google Scholar] [CrossRef]
- Bayer, W.L.; Tegtmeier, G.E. The blood donor: Detection and magnitude of cytomegalovirus carrier states and the prevalence of cytomegalovirus antibody. Yale J. Biol. Med. 1976, 49, 5–12. [Google Scholar]
- Sugiura, S.; Yoshikawa, T.; Nishiyama, Y.; Morishita, Y.; Sato, E.; Hattori, T.; Nakashima, T. Detection of human cytomegalovirus DNA in perilymph of patients with sensorineural hearing loss using real-time PCR. J. Med. Virol. 2003, 69, 72–75. [Google Scholar] [CrossRef]
- Di Nardo, W.; Cattani, P.; Lopizzo, T.; Cantore, I.; Marchese, M.R.; Marchetti, S.; Scorpecci, A.; Giannantonio, S.; Parrilla, C.; Cianfrone, F.; et al. Multiple viral genome search in endolabyrinthic fluids of profoundly deaf patients: Possible cytomegalovirus intracochlear reactivation. Audiol. Neurootol. 2009, 14, 290–295. [Google Scholar] [CrossRef]
- Teissier, N.; Delezoide, A.-L.; Mas, A.-E.; Khung-Savatovsky, S.; Bessières, B.; Nardelli, J.; Vauloup-Fellous, C.; Picone, O.; Houhou, N.; Oury, J.-F.; et al. Inner ear lesions in congenital cytomegalovirus infection of human fetuses. Acta Neuropathol. 2011, 122, 763–774. [Google Scholar] [CrossRef]
- Gross, M.; Wolf, D.G.; Elidan, J.; Eliashar, R. Enterovirus, cytomegalovirus, and Epstein-Barr virus infection screening in idiopathic sudden sensorineural hearing loss. Audiol. Neurotol. 2007, 12, 179–182. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.; Tetzlaff, J. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, 1–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jim, W.T.; Chiu, N.C.; Ho, C.S.; Shu, C.H.; Chang, J.H.; Hung, H.Y.; Kao, H.A.; Chang, H.Y.; Peng, C.C.; Yui, B.H.; et al. Outcome of Preterm Infants with Postnatal Cytomegalovirus Infection via Breast Milk: A Two-Year Prospective Follow-Up Study. Medicine 2015, 94, e1835. [Google Scholar] [CrossRef] [PubMed]
- Turner, K.M.; Lee, H.C.; Boppana, S.B.; Carlo, W.A.; Randolph, D.A. Incidence and impact of CMV infection in very low birth weight infants. Pediatrics 2014, 133, e609-15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikidis, D.; Nikolopoulos, T.P.; Kampessis, G.; Stamatiou, G.; Chrysovergis, A. Sudden sensorineural hearing loss: Subclinical viral and toxoplasmosis infections as aetiology and how they alter the clinical course. ORL J. Otorhinolaryngol. Relat. Spec. 2011, 73, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, J.; Van Kerschaver, E.; Wollants, E.; Beuselinck, K.; Stappaerts, L.; Van Ranst, M. Detection of perinatal cytomegalovirus infection and sensorineural hearing loss in belgian infants by measurement of automated auditory brainstem response. J. Clin. Microbiol. 2008, 46, 3564–3568. [Google Scholar] [CrossRef] [Green Version]
- Samileh, N.; Ahmad, S.; Mohammad, F.; Framarz, M.; Azardokht, T.; Jomeht, E. Role of cytomegalovirus in sensorineural hearing loss of children: A case-control study Tehran. Iran. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 203–208. [Google Scholar] [CrossRef]
- Johnson, S.J.; Hosford-Dunn, H.; Paryani, S.; Yeager, A.; Malachowski, N. Prevalence of sensorineural hearing loss in premature and sick term infants with perinatally acquired cytomegalovirus infection. Ear Hear. 1986, 7, 325–327. [Google Scholar] [CrossRef]
- Paryani, S.G.; Yeager, A.S.; Hosford-Dunn, H.; Johnson, S.J.; Malachowski, N.; Ariagno, R.L.; Stevenson, D.K. Sequelae of acquired cytomegalovirus infection in premature and sick term infants. J. Pediatr. 1985, 107, 451–456. [Google Scholar] [CrossRef]
- Paradowska, E.; Jabłońska, A.; Studzińska, M.; Suski, P.; Kasztelewicz, B.; Zawilińska, B.; Leśnikowski, Z.J. Distribution of cytomegalovirus gN variants and associated clinical sequelae in infants. J. Clin. Virol. 2013, 58, 271–275. [Google Scholar] [CrossRef]
- Wilson, W.R. The relationship of the herpesvirus family to sudden hearing loss: A prospective clinical study and literature review. Laryngoscope 1986, 96, 870–877. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Carraro, M.; Almishaal, A.; Hillas, E.; Firpo, M.; Park, A.; Harrison, R.V. Cytomegalovirus (CMV) Infection Causes Degeneration of Cochlear Vasculature and Hearing Loss in a Mouse Model. J. Assoc. Res. Otolaryngol. 2017, 18, 263–273. [Google Scholar] [CrossRef]
- Tsuprun, V.; Keskin, N.; Schleiss, M.R.; Schachern, P.; Cureoglu, S. Cytomegalovirus-induced pathology in human temporal bones with congenital and acquired infection. Am. J. Otolaryngol. 2019, 40, 102270. [Google Scholar] [CrossRef] [PubMed]
- Greco, A.; Gallo, A.; Fusconi, M.; Marinelli, C.; Macri, G.F.; de Vincentiis, M. Meniere’s disease might be an autoimmune condition? Autoimmun. Rev. 2012, 11, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Otake, H.; Tagaya, M.; Takahashi, Y.; Ito, Y.; Hama, A.; Nakashima, T. Progressive hearing loss following acquired cytomegalovirus infection in an immunocompromised child. Am. J. Otolaryngol. Head Neck Med. Surg. 2013, 34, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Vries, J.J.; Vesseur, A.; Rotteveel, L.J.; Korver, A.M.; Rusman, L.G.; Wessels, E.; Kroesa, A.C.M.; Mylanusb, E.A.; Oudesluys-Murphyd, A.M.; Frijns, J.H.M.; et al. Cytomegalovirus DNA detection in dried blood spots and perilymphatic fluids from pediatric and adult cochlear implant recipients with prelingual deafness. J. Clin. Virol. 2013, 56, 113–117. [Google Scholar] [CrossRef]
- Foulon, I.; Naessens, A.; Faron, G.; Foulon, W.; Jansen, A.C.; Gordts, F. Hearing thresholds in children with congenital CMV infection: A prospective study. Int. J. Pediatr. Otolaryngol. 2012, 76, 712–717. [Google Scholar] [CrossRef]
- Garcia Berrocal, J.R.; Ramírez-Camacho, R.; Portero, F.; Vargas, J.A. Role of viral and Mycoplasma pneumoniae infection in idiopathic sudden sensorineural hearing loss. Acta Oto-Laryngol. 2000, 120, 835–839. [Google Scholar] [CrossRef]
- Gkrania-Klotsas, E.; Langenberg, C.; Sharp, S.J.; Luben, R.; Khaw, K.-T.; Wareham, N.J. Seropositivity and higher immunoglobulin g antibody levels against cytomegalovirus are associated with mortality in the population-based European prospective investigation of cancer-norfolk cohort. Clin. Infect. Dis. 2013, 56, 1421–1427. [Google Scholar] [CrossRef]
- Meynard, J.L.; El Amrani, M.; Meyohas, M.C.; Fligny, I.; Gozlan, J.; Rozenbaum, W.; Frottier, J. Two cases of cytomegalovirus infection revealed by hearing loss in HIV- infected patients. Biomed. Pharmacother. 1997, 51, 461–463. [Google Scholar] [CrossRef]
- García-Berrocal, J.R.; Ramírez-Camacho, R.; González-García, J.A.; Verdaguer, J.M.; Trinidad, A. Does the serological study for viral infection in autoimmune inner ear disease make sense? ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 16–19. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Design | Population Studied (n) | Case Group Definition | Control Group Definition | Hearing results | Diagnosis of cytomegalovirus (CMV) infection | Relationship CMV- Sensorineural Hearing Loss (SNHL) | |||
|---|---|---|---|---|---|---|---|---|---|
| Pure Tone Audiometry | Neurophysiological Testing | Ascertainment Method | Determinant | ||||||
| Jim et al., 2015 [22] | Prospective case-control | Children <35 weeks (55) | Postnatal CMV infection through breast feeding (14) | Negative CMV infection (41) | Two infants with mild peripheral hearing impairment in both groups | No permanent delayed speech | Polymerase Chain Reaction (PCR) CMV isolation enzyme-linked immunosorbent assay (ELISA) | PCR-positive viral DNA in urine Culture positive urine (viruria) Antiviral IgM (serum) | None of the infants had CMV-related death or permanent SNHL |
| Turner et al., 2013 [23] | Retrospective case-control (from 1993 to 2008) | Infants with birth weights <1500 g (176) | Acquired CMV infection (16) | Negative CMV infection (160) | Suspected SNHL in 20% of infants with acquired CMV and 14% controls | Acquired CMV was not associated with neurologic sequelae | CMV isolation | Culture positive urine | Congenital CMV in infants is associated with high rates of neurologic injury and hearing loss comparing with acquired CMV infants |
| Kikidis et al., 2010 [24] | Prospective case-control | Adults patients with sudden SNHL (84) | CMV, herpes simplex virus, toxoplasma and Epstein-Barr infection (8) | Negative virus/toxoplasma infection (76) | Hearing level was 86.5 dB HL in the case group and 60.7 dB HL in the control group. | ELISA | Antiviral IgM (serum) | Recent subclinical viral or toxoplasmosis infections may be involved in the pathogenesis of sudden SNHL (in approx. 10% of cases), suggesting that sudden SNHL is not a single disease | |
| Verbeeck et al., 2008 [25] | Retrospective case-control (from 2002 to 2004) | Babies born between April 2002 and April 2004 (526) | 194 babies with indicative hearing impairment (22 positive CMV; 172 negative CMV) | 332 matched controls without hearing impairment (15 positive CMV; 317 negative CMV) | Hearing impairment at birth was confirmed by an audiological center in 136 out of the 526 tested babies while 390 tested babies proved to have normal hearing. | None of the children had developed delayed-onset hearing loss at the end of the study | PCR CMV isolation | PCR-positive viral DNA in urine Culture positive urine | Significantly more babies with confirmed hearing impairment were CMV positive after birth Babies with CMV viral loads above 4.5 log copies/mL urine seem to be 1.4 times more likely to have confirmed hearing impairment. |
| Samileh et al., 2008 [26] | Case-control study (from 2002–2003) | Children <14 years (158) | Children with SNHL (95) Acute infection (CMV-IgM) in 33/95, previous immunity (IgG) in 69/95 | Children without SNHL (63) Acute infection (CMV-IgM) in 2/57, previous immunity (CMV-IgG) in 54/57 | Severity of SNHL in cases included: 80% profound >95 db; 15% moderate; 5% mild. Unilateral SNHL 22% (20/95); bilateral SNHL 78% (75/95). | ELISA | Antiviral IgG and IgM (serum) | CMV is one of the most common infectious agents in SNHL children compared to the healthy children. Probably both congenital and acquired CMV can induce progressive hearing loss. | |
| Johnson et al., 1986 [27] | Prospective case-control | Infants (80) | Premature or sick term infants with perinatally acquired CMV (40) | Matched control subjects (40) | One case group subject had a bilateral SNHL> 4000 Hz. Four control subjects had SNHL, 3 requiring binaural hearing aids. | There were 12 transient conductive hearing losses due to serous or suppurative otitis media. Five of these losses were in the case group and seven were in the control group | CMV isolation | Culture positive Urine and/or saliva | Perinatally acquired CMV infection is not associated with significant SNHL in premature or full term infants through age 3. |
| Paryani et al., 1985 [28] | Prospective case-control | Infants (84) | Premature or sick term infants with perinatally acquired CMV (42) | Matched control subjects (42) | SNHL in 4 of 42 CMV infected patients (all mild-moderate) and in 2 of 42 controls (one severe) | All of the CMV infected patients had SNHL >4000 Hz, and hearing aids were not required. | CMV isolation | Culture positive urine and saliva | Acquired CMV infections are not associated with a significant increase in SNHL |
| Paradowska et al., 2013 [29] | Prospective case-control | Children (93) Adults (55) | Postnatal CMV infection + SNHL | CMV infected adults | Hearing loss in 10 children (11%) | Nested PCR (nPCR) | Viral DNA from peripheral blood, urine, and/or cerebrospinal fluid samples | No association was found | |
| Wilson, 1986 [30] | Prospective case-control | Adults and children (217) | SNHL | Healthy patients | Profound and mild, mid-frequency hearing losses | Complement fixation assay (CFA) | Antiviral IgG and IgM (serum) | No differences were found between the effects of herpes virus infection upon the degree of hearing loss in patients with or without herpes infection | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Gomez, E.; Perez-Carpena, P.; Flook, M.; Lopez-Escamez, J.A. A Systematic Review on the Association of Acquired Human Cytomegalovirus Infection with Hearing Loss. J. Clin. Med. 2020, 9, 4011. https://doi.org/10.3390/jcm9124011
Martinez-Gomez E, Perez-Carpena P, Flook M, Lopez-Escamez JA. A Systematic Review on the Association of Acquired Human Cytomegalovirus Infection with Hearing Loss. Journal of Clinical Medicine. 2020; 9(12):4011. https://doi.org/10.3390/jcm9124011
Chicago/Turabian StyleMartinez-Gomez, Estrella, Patricia Perez-Carpena, Marisa Flook, and José A. Lopez-Escamez. 2020. "A Systematic Review on the Association of Acquired Human Cytomegalovirus Infection with Hearing Loss" Journal of Clinical Medicine 9, no. 12: 4011. https://doi.org/10.3390/jcm9124011