

Efficacy and Safety of Co-Administered St. John’s Wort and Ginkgo biloba Extracts in Patients with Subjective Tinnitus: A Preliminary Prospective Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessments
2.3. Randomization
2.4. Intervention
2.5. Outcomes
2.6. Statistical Analyses
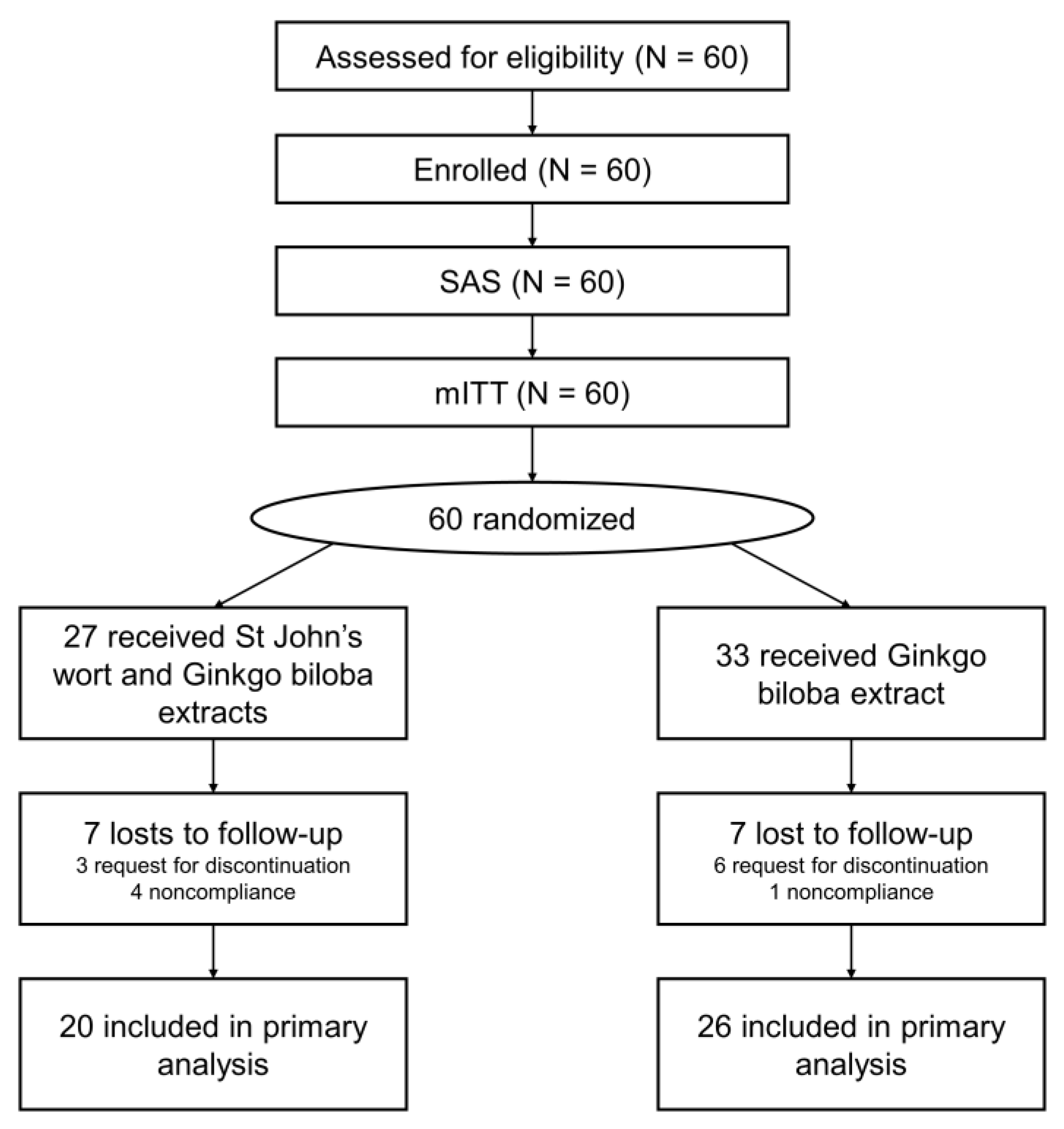
3. Results
3.1. Characteristics of the Groups before Drug Administration
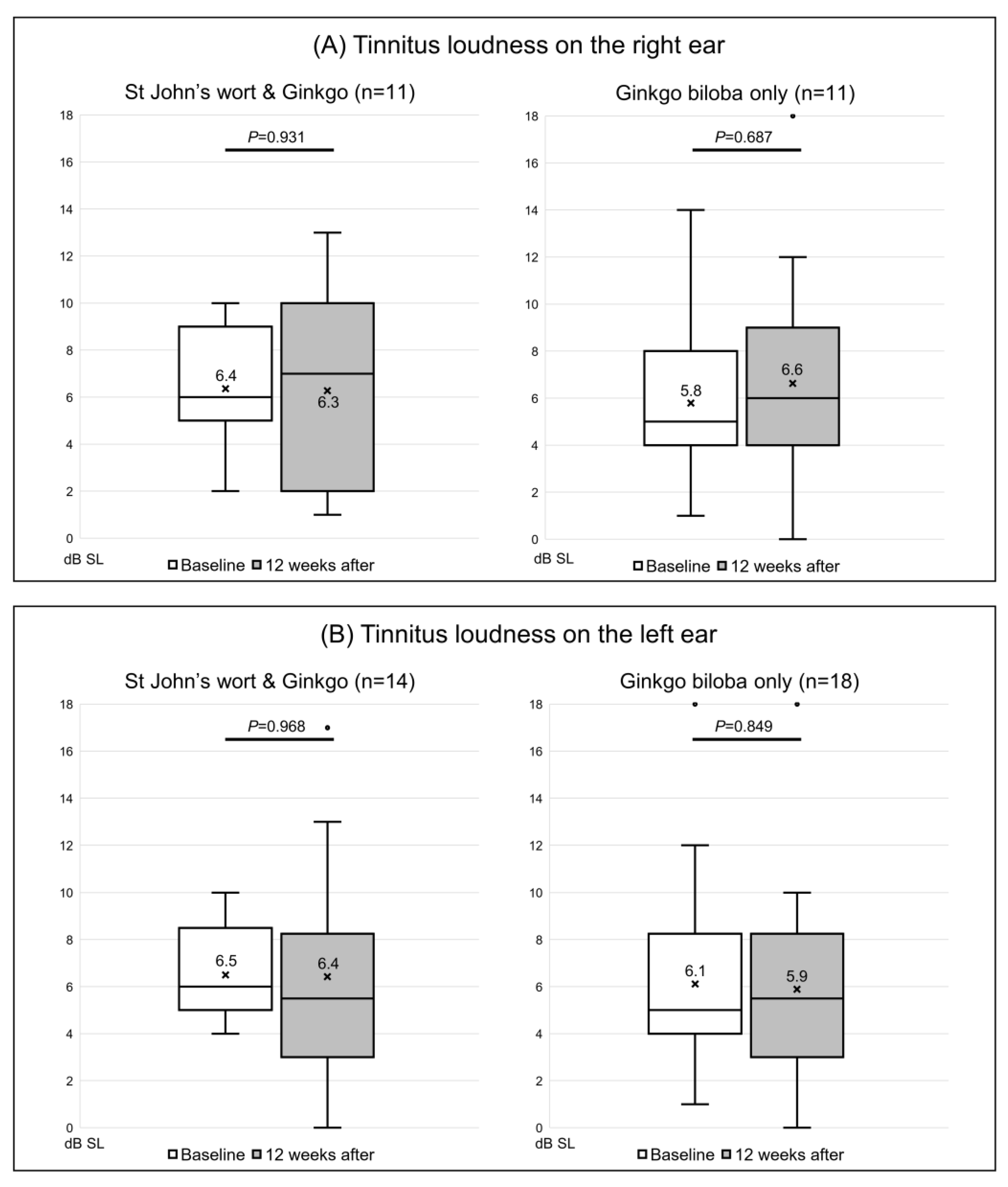
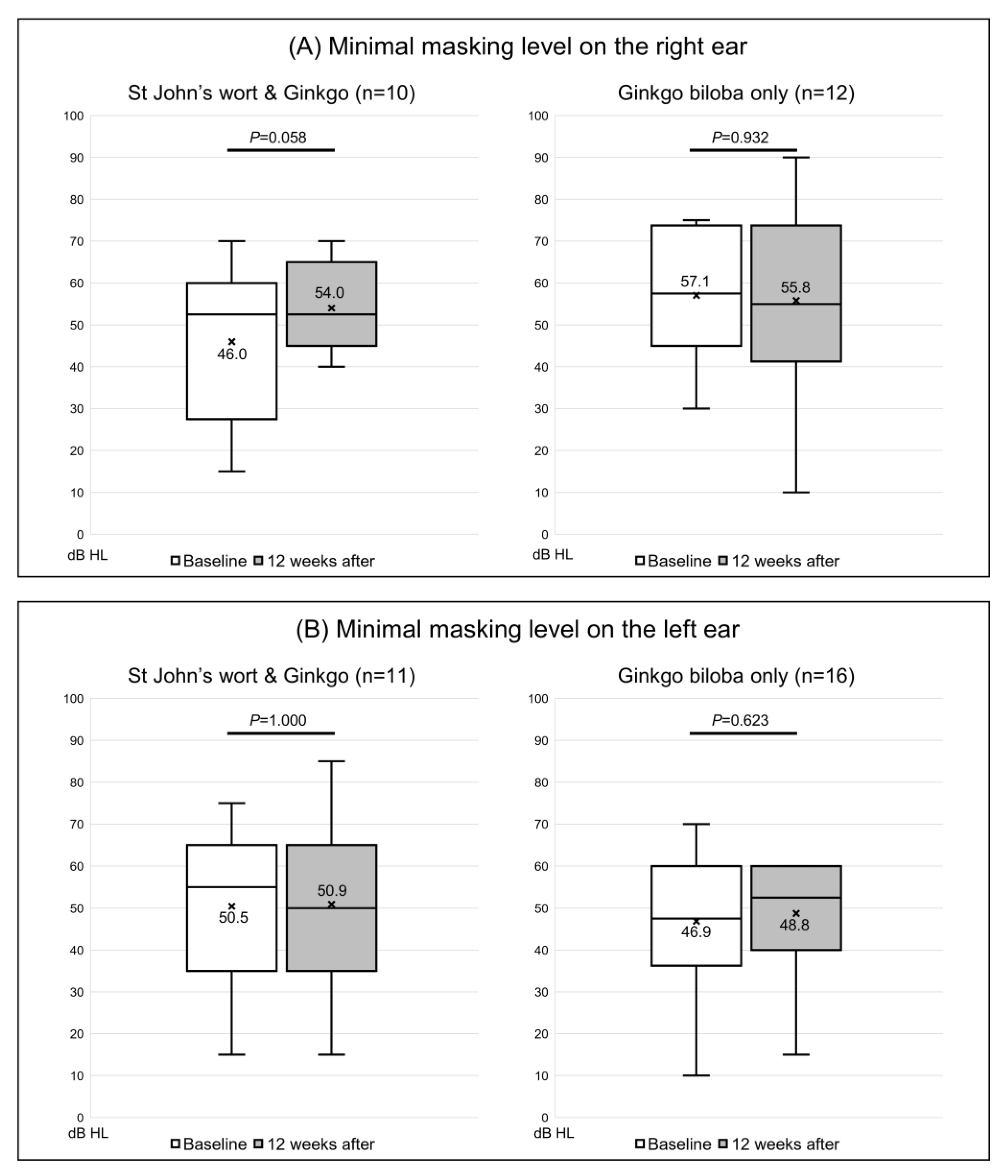
3.2. Changes in the Tinnitogram before and after Extract Administration
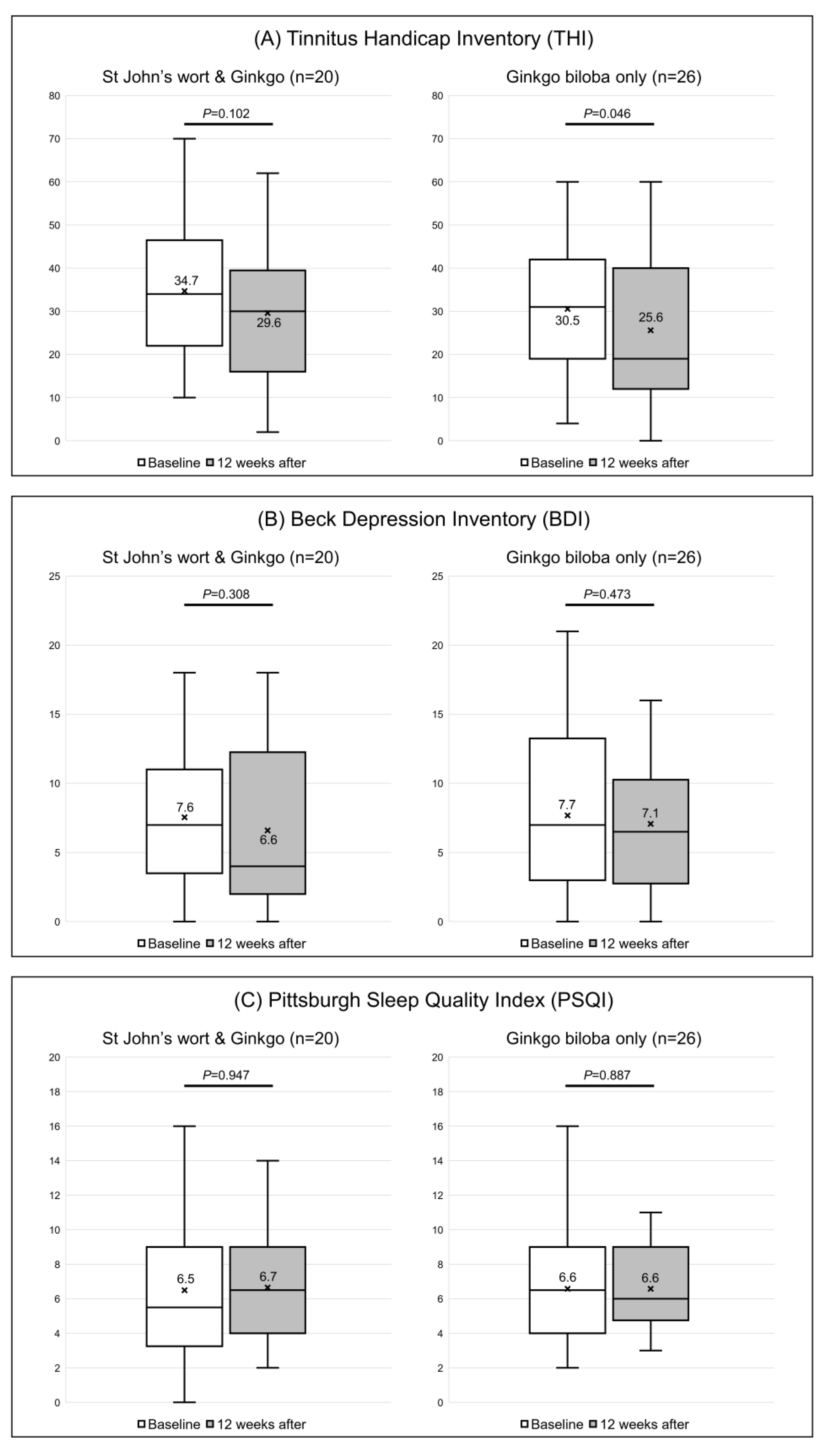
3.3. The Tinnitus Handicap Inventory (THI) Questionnaire Responses before and after Drug Administration
3.4. The Beck Depression Inventory (BDI) and the Pittsburgh Sleep Quality Index (PSQI)
3.5. Changes of the Quality of Life Using the Short Form-36 Health Survey (SF-36)
3.6. Multivariate Analysis of Factors Affecting the THI Score
3.7. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, H.J.; Lee, H.J.; An, S.Y.; Sim, S.; Park, B.; Kim, S.W.; Lee, J.S.; Hong, S.K.; Choi, H.G. Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS ONE 2015, 10, e0127578. [Google Scholar] [CrossRef] [PubMed]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, J.M.; Lin, H.W.; Bhattacharyya, N. Prevalence, Severity, Exposures, and Treatment Patterns of Tinnitus in the United States. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 959–965. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kim, Y.H. Relationship Between Diet and Tinnitus: Korea National Health and Nutrition Examination Survey. Clin. Exp. Otorhinolaryngol. 2018, 11, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Lee, S.H.; Koo, J.W.; Park, H.Y.; Lee, K.Y.; Choi, Y.S.; Oh, K.W.; Lee, A.; Yang, J.E.; Woo, S.Y.; et al. Prevalence and associated factors of tinnitus: Data from the Korean National Health and Nutrition Examination Survey 2009–2011. J. Epidemiol. 2014, 24, 417–426. [Google Scholar] [CrossRef]
- Coles, R.R. Epidemiology of tinnitus: (1) prevalence. J. Laryngol. Otol. Suppl. 1984, 9, 7–15. [Google Scholar] [CrossRef]
- Husain, F.T.; Gander, P.E.; Jansen, J.N.; Shen, S. Expectations for Tinnitus Treatment and Outcomes: A Survey Study of Audiologists and Patients. J. Am. Acad. Audiol. 2018, 29, 313–336. [Google Scholar] [CrossRef]
- Jastreboff, P.J. Tinnitus retraining therapy. Prog. Brain Res. 2007, 166, 415–423. [Google Scholar] [CrossRef]
- Jastreboff, P.J.; Hazell, J.W. A neurophysiological approach to tinnitus: Clinical implications. Br. J. Audiol. 1993, 27, 7–17. [Google Scholar] [CrossRef]
- Tunkel, D.E.; Bauer, C.A.; Sun, G.H.; Rosenfeld, R.M.; Chandrasekhar, S.S.; Cunningham, E.R., Jr.; Archer, S.M.; Blakley, B.W.; Carter, J.M.; Granieri, E.C.; et al. Clinical practice guideline: Tinnitus. Otolaryngol. Head Neck Surg. 2014, 151, S1–S40. [Google Scholar] [CrossRef]
- Ogawa, K.; Sato, H.; Takahashi, M.; Wada, T.; Naito, Y.; Kawase, T.; Murakami, S.; Hara, A.; Kanzaki, S. Clinical practice guidelines for diagnosis and treatment of chronic tinnitus in Japan. Auris Nasus Larynx 2020, 47, 1–6. [Google Scholar] [CrossRef]
- Chien, W.; Lin, F.R. Prevalence of hearing aid use among older adults in the United States. Arch. Intern. Med. 2012, 172, 292–293. [Google Scholar] [CrossRef]
- Moon, I.J.; Baek, S.Y.; Cho, Y.S. Hearing Aid Use and Associated Factors in South Korea. Medicine 2015, 94, e1580. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, D.; Lee, J.M.; Lee, S.K.; Kang, H.J.; Yeo, S.G. Review of Pharmacotherapy for Tinnitus. Healthcare 2021, 9, 779. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Bhattacharyya, N.; Lin, H.W. Relationships between tinnitus and the prevalence of anxiety and depression. Laryngoscope 2017, 127, 466–469. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef]
- Choi, J.; Lee, C.H.; Kim, S.Y. Association of Tinnitus with Depression in a Normal Hearing Population. Medicina 2021, 57, 114. [Google Scholar] [CrossRef]
- Sullivan, M.; Katon, W.; Russo, J.; Dobie, R.; Sakai, C. A randomized trial of nortriptyline for severe chronic tinnitus. Effects on depression, disability, and tinnitus symptoms. Arch. Intern. Med. 1993, 153, 2251–2259. [Google Scholar] [CrossRef]
- Mihail, R.C.; Crowley, J.M.; Walden, B.E.; Fishburne, J.; Reinwall, J.E.; Zajtchuk, J.T. The tricyclic trimipramine in the treatment of subjective tinnitus. Ann. Otol. Rhinol. Laryngol. 1988, 97, 120–123. [Google Scholar] [CrossRef]
- Zöger, S.; Svedlund, J.; Holgers, K.M. The effects of sertraline on severe tinnitus suffering--a randomized, double-blind, placebo-controlled study. J. Clin. Psychopharmacol. 2006, 26, 32–39. [Google Scholar] [CrossRef]
- Dib, G.C.; Kasse, C.A.; Alves de Andrade, T.; Gurgel Testa, J.R.; Cruz, O.L. Tinnitus treatment with Trazodone. Braz. J. Otorhinolaryngol. 2007, 73, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Baldo, P.; Doree, C.; Molin, P.; McFerran, D.; Cecco, S. Antidepressants for patients with tinnitus. Cochrane Database Syst. Rev. 2012, 2012, CD003853. [Google Scholar] [CrossRef] [PubMed]
- Holstein, N. Ginkgo special extract EGb 761 in tinnitus therapy. An overview of results of completed clinical trials. Fortschr. Med. Orig. 2001, 118, 157–164. [Google Scholar] [PubMed]
- von Boetticher, A. Ginkgo biloba extract in the treatment of tinnitus: A systematic review. Neuropsychiatr. Dis. Treat. 2011, 7, 441–447. [Google Scholar] [CrossRef]
- Rejali, D.; Sivakumar, A.; Balaji, N. Ginkgo biloba does not benefit patients with tinnitus: A randomized placebo-controlled double-blind trial and meta-analysis of randomized trials. Clin. Otolaryngol. Allied Sci. 2004, 29, 226–231. [Google Scholar] [CrossRef]
- Apaydin, E.A.; Maher, A.R.; Shanman, R.; Booth, M.S.; Miles, J.N.; Sorbero, M.E.; Hempel, S. A systematic review of St. John’s wort for major depressive disorder. Syst. Rev. 2016, 5, 148. [Google Scholar] [CrossRef]
- Linde, K.; Berner, M.M.; Kriston, L. St John’s wort for major depression. Cochrane Database Syst. Rev. 2008, 2008, CD000448. [Google Scholar] [CrossRef]
- Eatemadnia, A.; Ansari, S.; Abedi, P.; Najar, S. The effect of Hypericum perforatum on postmenopausal symptoms and depression: A randomized controlled trial. Complement Ther. Med. 2019, 45, 109–113. [Google Scholar] [CrossRef]
- Abdali, K.; Khajehei, M.; Tabatabaee, H.R. Effect of St John’s wort on severity, frequency, and duration of hot flashes in premenopausal, perimenopausal and postmenopausal women: A randomized, double-blind, placebo-controlled study. Menopause 2010, 17, 326–331. [Google Scholar] [CrossRef]
- Canenguez Benitez, J.S.; Hernandez, T.E.; Sundararajan, R.; Sarwar, S.; Arriaga, A.J.; Khan, A.T.; Matayoshi, A.; Quintanilla, H.A.; Kochhar, H.; Alam, M.; et al. Advantages and Disadvantages of Using St. John’s Wort as a Treatment for Depression. Cureus 2022, 14, e29468. [Google Scholar] [CrossRef]
- Zacharia, T.; Naik, P.V.; Sada, S.; Kuniyil, J.G.; Dwarakanath, V.M. Development and standardization of tinnitus handicap inventory in Kannada. Int. Tinnitus J. 2012, 17, 117–123. [Google Scholar] [CrossRef]
- Preljevic, V.T.; Østhus, T.B.; Sandvik, L.; Opjordsmoen, S.; Nordhus, I.H.; Os, I.; Dammen, T. Screening for anxiety and depression in dialysis patients: Comparison of the Hospital Anxiety and Depression Scale and the Beck Depression Inventory. J. Psychosom. Res. 2012, 73, 139–144. [Google Scholar] [CrossRef]
- Gu, H.; Kong, W.; Yin, H.; Zheng, Y. Prevalence of sleep impairment in patients with tinnitus: A systematic review and single-arm meta-analysis. Eur. Arch. Otorhinolaryngol. 2022, 279, 2211–2221. [Google Scholar] [CrossRef]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 health survey questionnaire: New outcome measure for primary care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef]
- Sieghart, W. Pharmacology of benzodiazepine receptors: An update. J. Psychiatry Neurosci. 1994, 19, 24–29. [Google Scholar] [CrossRef]
- Johnson, R.M.; Brummett, R.; Schleuning, A. Use of alprazolam for relief of tinnitus. A double-blind study. Arch. Otolaryngol. Head Neck Surg. 1993, 119, 842–845. [Google Scholar] [CrossRef]
- Jalali, M.M.; Kousha, A.; Naghavi, S.E.; Soleimani, R.; Banan, R. The effects of alprazolam on tinnitus: A cross-over randomized clinical trial. Med. Sci. Monit. 2009, 15, PI55–PI60. [Google Scholar]
- Jufas, N.E.; Wood, R. The use of benzodiazepines for tinnitus: Systematic review. J. Laryngol. Otol. 2015, 129, S14–S22. [Google Scholar] [CrossRef]
- Han, J.S.; Park, J.M.; Park, S.Y.; Vidal, J.L.; Ashaikh, H.K.; Kim, D.K.; Park, S.N. Typewriter tinnitus: An investigative comparison with middle ear myoclonic tinnitus and its long-term therapeutic response to carbamazepine. Auris Nasus Larynx 2020, 47, 580–586. [Google Scholar] [CrossRef]
- Piccirillo, J.F.; Finnell, J.; Vlahiotis, A.; Chole, R.A.; Spitznagel, E., Jr. Relief of idiopathic subjective tinnitus: Is gabapentin effective? Arch. Otolaryngol. Head Neck Surg. 2007, 133, 390–397. [Google Scholar] [CrossRef]
- Bauer, C.A.; Brozoski, T.J. Effect of gabapentin on the sensation and impact of tinnitus. Laryngoscope 2006, 116, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Farhadi, M.; Salem, M.M.; Asghari, A.; Daneshi, A.; Mirsalehi, M.; Mahmoudian, S. Impact of Acamprosate on Chronic Tinnitus: A Randomized-Controlled Trial. Ann. Otol. Rhinol. Laryngol. 2020, 129, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Kwon, O.D.; Kim, S.G.; Shin, I.H. Recognitional study about patients and caregivers’ understanding of clinical trial. J. Korean Cont. Soc. 2008, 12, 48–57. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| St John’s Wort & Ginkgo biloba (n = 20) | Ginkgo biloba (n = 26) | p-Value * | |
|---|---|---|---|
| Age | 50.3 (9.6) | 51.3 (8.9) | 0.724 |
| Gender | 0.275 ** | ||
| Female | 4 (20.0%) | 9 (34.6%) | |
| Male | 16 (80.0%) | 17 (65.4%) | |
| Height (cm) | 168.6 (7.9) | 165.6 (9.5) | 0.258 |
| Weight (kg) | 69.5 (11.9) | 67.2 (11.4) | 0.504 |
| Blood pressure (BP) | |||
| Systolic BP | 131.1 (13.0) | 126.9 (18.3) | 0.383 |
| Diastolic BP | 81.4 (9.8) | 81.5 (11.4) | 0.972 |
| Pulse (bpm) | 81.7 (9.0) | 77.7 (9.3) | 0.158 |
| Body temperature (°C) | 36.7 (0.3) | 36.6 (0.2) | 0.493 |
| Pure-tone thresholds (dB) *** | |||
| Right ear | 13.0 (5.7) | 15.6 (5.2) | 0.109 |
| Left ear | 15.1 (7.7) | 15.0 (6.0) | 0.953 |
| 36-Item Short Form Survey (SF-36) | |||
| Physical Functioning (PF) | 91.5 (11.0) | 85.8 (16.8) | 0.234 |
| Role-Physical (RP) | 75.0 (35.4) | 77.1 (32.9) | 0.847 |
| Bodily Pain (BP) | 78.0 (21.4) | 78.4 (23.6) | 0.954 |
| General Health (GH) | 49.7 (23.9) | 55.4 (21.1) | 0.403 |
| Vitality (VT) | 58.2 (18.0) | 52.0 (19.2) | 0.300 |
| Social Functioning (SF) | 74.5 (21.5) | 75.7 (18.6) | 0.851 |
| Role-Emotional (RE) | 88.2 (28.8) | 82.0 (34.1) | 0.539 |
| Mental Health (MH) | 72.0 (12.6) | 66.9 (14.9) | 0.258 |
| Beck Depression Inventory (BDI) | 7.6 (4.7) | 7.7 (5.9) | 0.930 |
| Pittsburgh Sleep Quality Index (PSQI) | 6.5 (4.0) | 6.6 (3.4) | 0.944 |
| Tinnitus Handicap Inventory (THI) | 34.7 (15.9) | 30.5 (16.7) | 0.396 |
| St John’s Wort & Ginkgo biloba (n = 20) | Baseline | 12 Weeks after | Difference from Baseline to 12 Weeks * | p-Value ** |
| Total score | 34.7 (15.9) | 29.6 (16.0) | 5.1 (14.7) | 0.102 |
| Functional domain | 13.5 (9.4) | 13.5 (7.3) | 0.0 (8.0) | 0.965 |
| Emotional domain | 10.8 (7.2) | 9.8 (6.7) | 1.0 (6.8) | 0.304 |
| Catastrophic domain | 6.8 (4.6) | 6.3 (4.7) | 0.5 (4.9) | 0.627 |
| Ginkgo biloba (n = 26) | Baseline | 12 Weeks after | Difference from Baseline to 12 Weeks * | p-Value ** |
| Total score | 30.5 (16.7) | 25.6 (17.1) | 4.9 (11.6) | 0.046 |
| Functional domain | 12.6 (7.8) | 11.0 (7.0) | 1.6 (5.9) | 0.166 |
| Emotional domain | 10.6 (7.2) | 9.5 (7.9) | 1.1 (5.2) | 0.290 |
| Catastrophic domain | 6.7 (4.5) | 5.2 (4.5) | 1.5 (3.7) | 0.056 |
| St John’s Wort & Ginkgo biloba (n = 20) | Baseline | 12 Weeks after | Difference from Baseline to 12 Weeks * | p-Value ** |
| Physical Functioning (PF) | 91.5 (11.0) | 89.7 (13.2) | 1.8 (8.7) | 0.589 |
| Role-Physical (RP) | 75.0 (35.4) | 79.4 (31.0) | –4.4 (15.9) | 0.257 |
| Bodily Pain (BP) | 78.0 (21.4) | 76.9 (23.9) | 1.1 (24.6) | 0.753 |
| General Health (GH) | 49.7 (23.9) | 55.0 (19.9) | –5.3 (14.7) | 0.240 |
| Vitality (VT) | 58.2 (18.0) | 61.5 (16.8) | –3.2 (18.1) | 0.664 |
| Social Functioning (SF) | 74.5 (21.5) | 83.9 (20.5) | –9.5 (15.7) | 0.047 |
| Role-Emotional (RE) | 88.2 (28.8) | 94.1 (24.3) | –5.9 (17.7) | 0.180 |
| Mental Health (MH) | 72.0 (12.6) | 71.1 (15.1) | 0.9 (10.4) | 0.607 |
| Ginkgo biloba (n = 26) | Baseline | 12 Weeks after | Difference from Baseline to 12 Weeks * | p-Value ** |
| Physical Functioning (PF) | 85.8 (16.8) | 83.8 (20.3) | 2.1 (9.0) | 0.395 |
| Role-Physical (RP) | 77.1 (32.9) | 72.9 (35.3) | 4.2 (26.2) | 0.431 |
| Bodily Pain (BP) | 78.4 (23.6) | 68.3 (22.6) | 10.2 (25.5) | 0.084 |
| General Health (GH) | 55.4 (21.1) | 51.7 (17.9) | 3.8 (12.7) | 0.178 |
| Vitality (VT) | 52.0 (19.2) | 55.6 (14.2) | –3.6 (16.0) | 0.294 |
| Social Functioning (SF) | 75.7 (18.6) | 70.5 (16.0) | 5.2 (18.2) | 0.253 |
| Role-Emotional (RE) | 82.0 (34.1) | 83.4 (31.1) | –1.5 (18.3) | 0.461 |
| Mental Health (MH) | 66.9 (14.9) | 64.5 (16.7) | 2.5 (14.9) | 0.625 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Ha, J.; Park, H.Y.; Choung, Y.-H.; Jang, J.H. Efficacy and Safety of Co-Administered St. John’s Wort and Ginkgo biloba Extracts in Patients with Subjective Tinnitus: A Preliminary Prospective Randomized Controlled Trial. J. Clin. Med. 2023, 12, 3261. https://doi.org/10.3390/jcm12093261
Kim H, Ha J, Park HY, Choung Y-H, Jang JH. Efficacy and Safety of Co-Administered St. John’s Wort and Ginkgo biloba Extracts in Patients with Subjective Tinnitus: A Preliminary Prospective Randomized Controlled Trial. Journal of Clinical Medicine. 2023; 12(9):3261. https://doi.org/10.3390/jcm12093261
Chicago/Turabian StyleKim, Hantai, Jungho Ha, Hun Yi Park, Yun-Hoon Choung, and Jeong Hun Jang. 2023. "Efficacy and Safety of Co-Administered St. John’s Wort and Ginkgo biloba Extracts in Patients with Subjective Tinnitus: A Preliminary Prospective Randomized Controlled Trial" Journal of Clinical Medicine 12, no. 9: 3261. https://doi.org/10.3390/jcm12093261