
Update on Shoulder Arthroplasties with Emphasis on Imaging
Abstract
:1. Introduction
2. Clinical
2.1. Anatomy and Biomechanics
2.2. Arthroplasty Indications
2.2.1. Degenerative
2.2.2. Trauma
2.2.3. Inflammatory Arthritis
2.2.4. Instability
2.2.5. Other
3. Preoperative Imaging
4. Post-Operative Imaging and Imaging of Complications
4.1. Imaging Techniques
4.2. General Complications
4.2.1. Loosening and Hardware Dissociation
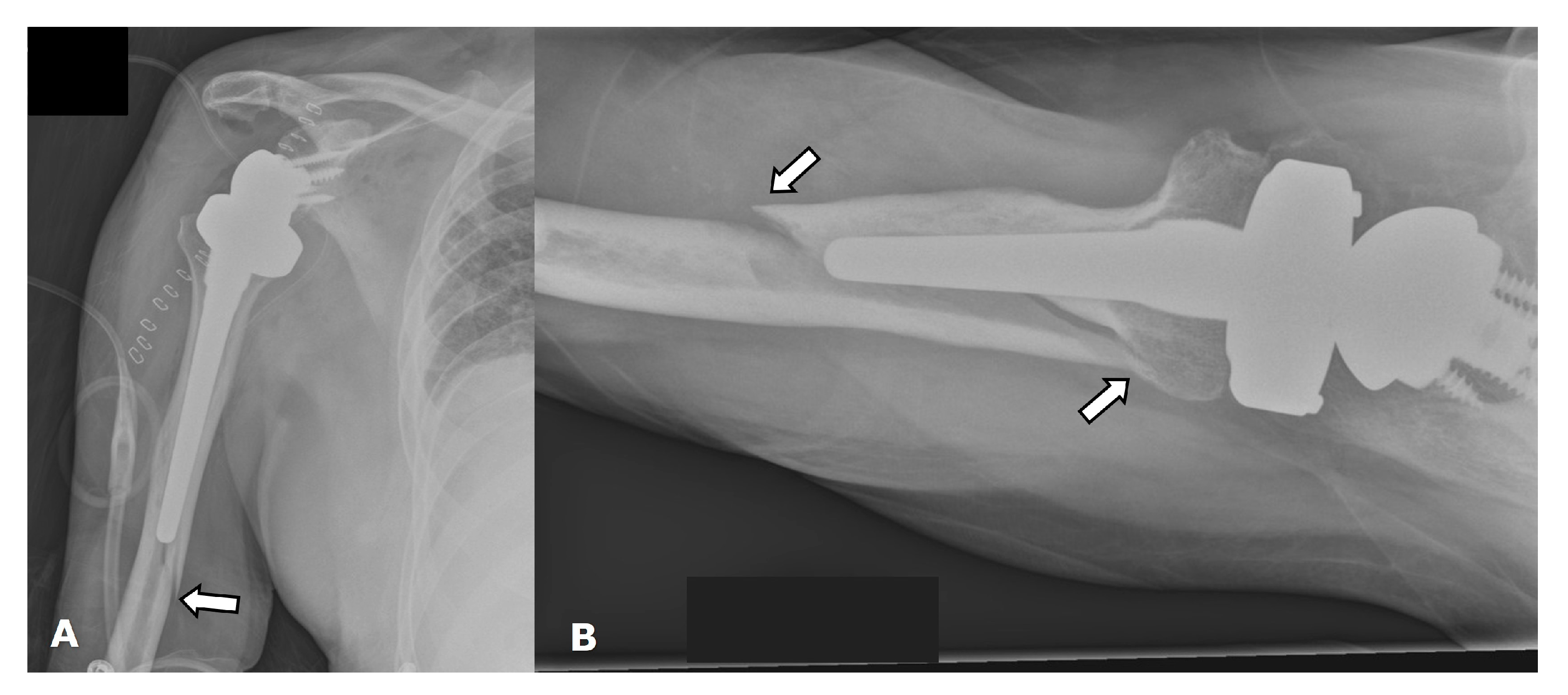
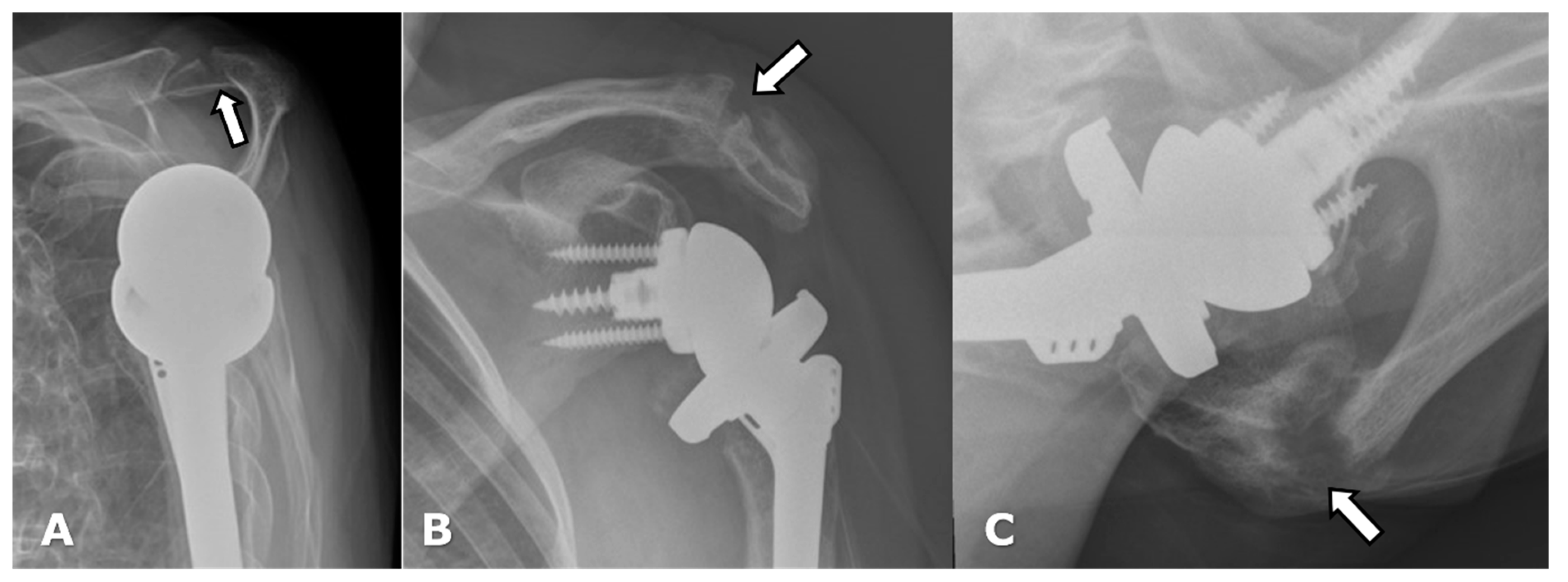
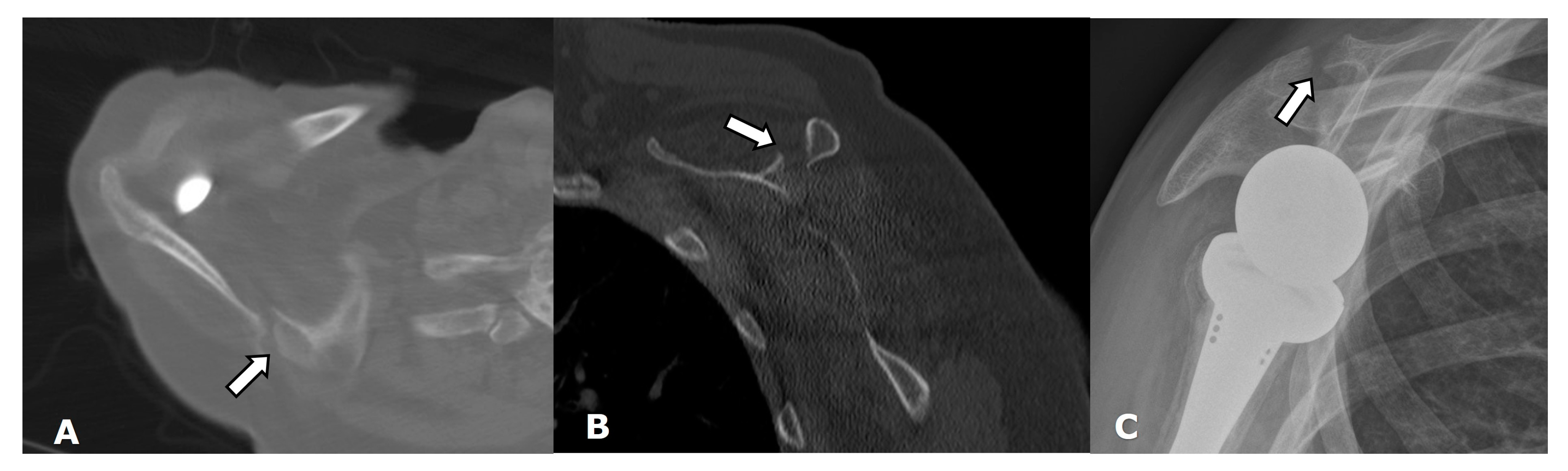
4.2.2. Stress Shielding and Fractures
4.2.3. Periprosthetic Joint Infection (PJI)
4.2.4. Rotator Cuff Tendon Tears
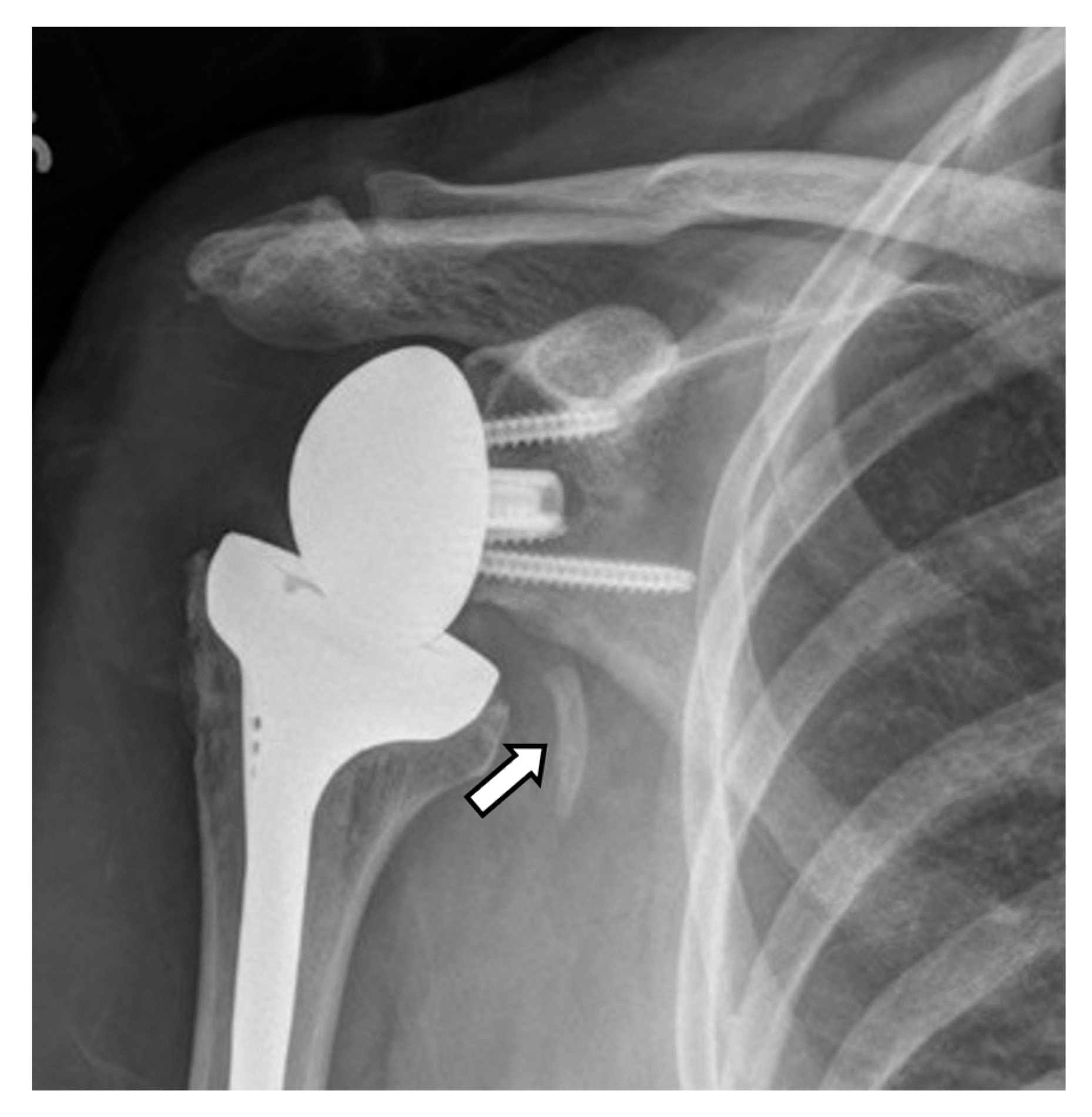
4.3. Unique Complications
5. Arthroplasty Types
5.1. Anatomic Arthroplasties
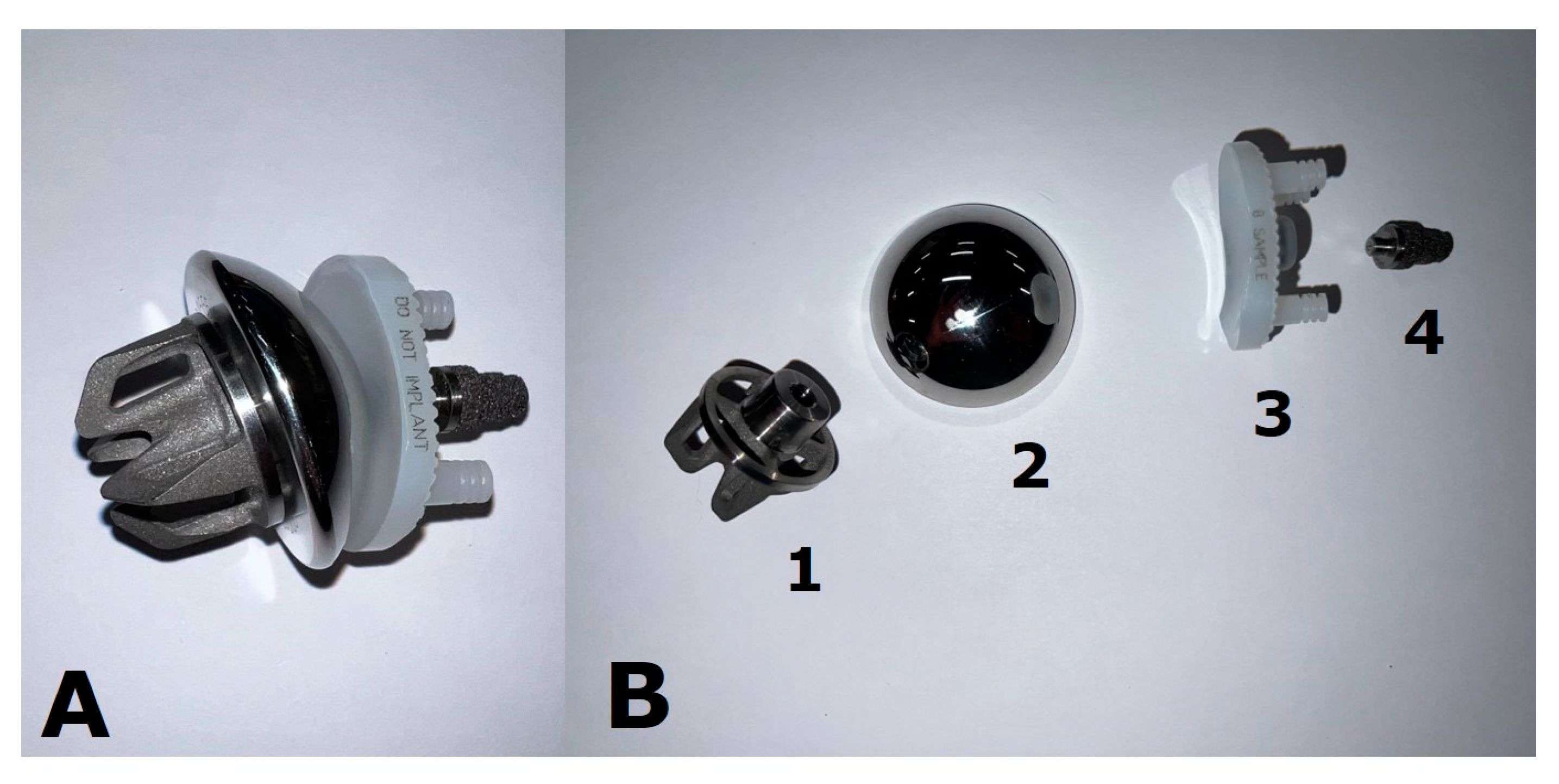
5.1.1. Humeral Head Resurfacing/Stemless Hemiarthroplasty (HHRA)
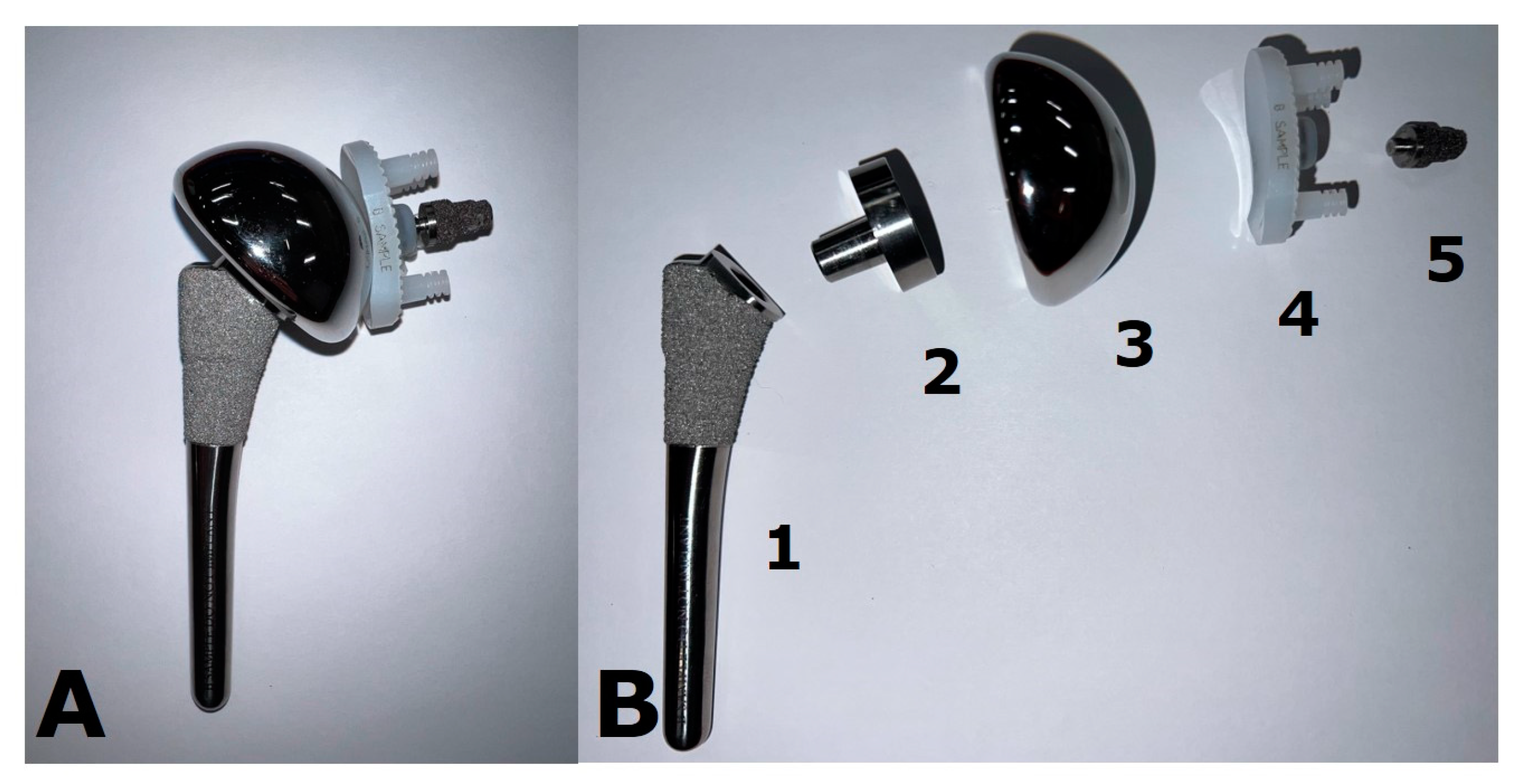
5.1.2. Hemiarthroplasty (HA)
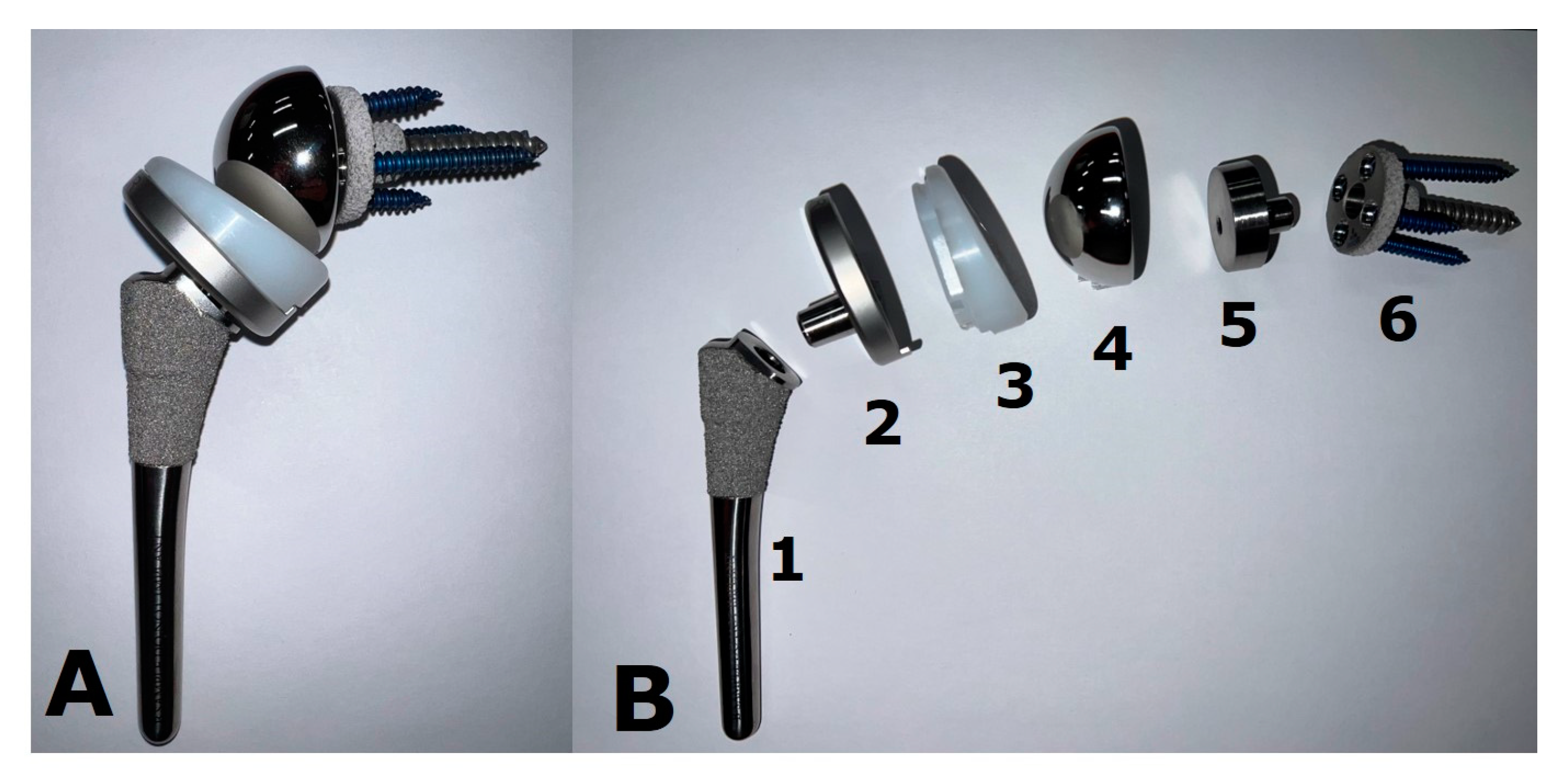
5.1.3. Anatomic Total Shoulder Arthroplasty (ATSA)
5.2. Reverse Arthroplasty
Reverse Total Shoulder Arthroplasty (RTSA)
5.3. Revision Shoulder Arthroplasty
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papalexis, N.; Ponti, F.; Rinaldi, R.; Peta, G.; Bruno, R.; Miceli, M.; Battaglia, M.; Marinelli, A.; Spinnato, P. Ultrasound-Guided Treatments for the Painful Shoulder. Curr. Med. Imaging 2021, 18, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.J.; Wong, T.T.; Kazam, J.K. Shoulder Arthroplasty, from Indications to Complications: What the Radiologist Needs to Know. Radiographics 2016, 36, 192–208. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, A.; Siebert, M.J.; Chhabra, A. How to Measure Glenoid Bone Stock and Version and Why It Is Important: A Practical Guide. Radiographics 2020, 40, 1671–1683. [Google Scholar] [CrossRef]
- Lee, D.H.; Choi, Y.S.; Potter, H.G.; Endo, Y.; Sivakumaran, T.; Lim, T.K.; Chun, T.J. Reverse total shoulder arthroplasty: An imaging overview. Skelet. Radiol. 2019, 49, 19–30. [Google Scholar] [CrossRef]
- Romero, B.A.; Horneff, J.G., 3rd. Soft Tissue Management in Shoulder Arthroplasty. Orthop. Clin. N. Am. 2022, 53, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Lo, L.; Koenig, S.; Leong, N.L.; Shiu, B.B.; Hasan, S.A.; Gilotra, M.N.; Wang, K.C. Glenoid bony morphology of osteoarthritis prior to shoulder arthroplasty: What the surgeon wants to know and why. Skelet. Radiol. 2020, 50, 881–894. [Google Scholar] [CrossRef]
- Bartolotta, R.J.; Ha, A.S. Current Imaging Concepts in Shoulder and Hip Arthroplasty. Radiol. Clin. N. Am. 2022, 60, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.N.; Bjørdal, J.; Wagle, T.M.; Karlberg, A.C.; Lien, O.A.; Eilertsen, L.; Mader, K.; Apold, H.; Larsen, L.B.; Madsen, J.E.; et al. Reverse Shoulder Arthroplasty Is Superior to Plate Fixation at 2 Years for Displaced Proximal Humeral Fractures in the Elderly: A Multicenter Randomized Controlled Trial. J. Bone Jt. Surg. Am. 2020, 102, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, E.; Ekholm, C.; Salomonsson, B.; Demir, Y.; Olerud, P.; Etzner, M.; Ihrman, R.; Nordqvist, A.; Scheer, J.; Westman, F. Reverse total shoulder arthroplasty provides better shoulder function than hemiarthroplasty for displaced 3- and 4-part proximal humeral fractures in patients aged 70 years or older: A multicenter randomized controlled trial. J. Shoulder Elb. Surg. 2020, 30, 994–1006. [Google Scholar] [CrossRef]
- Laas, N.; Engelsma, Y.; Hagemans, F.J.; Hoelen, M.A.; van Deurzen, D.F.; Burger, B.J. Reverse or Hemi Shoulder Arthroplasty in Proximal Humerus Fractures: A Single-Blinded Prospective Multicenter Randomized Clinical Trial. J. Orthop. Trauma 2021, 35, 252–258. [Google Scholar] [CrossRef]
- Cho, C.-H.; Kim, D.-H.; Song, K.-S. Reverse Shoulder Arthroplasty in Patients with Rheumatoid Arthritis: A Systematic Review. Clin. Orthop. Surg. 2017, 9, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.R.; Cannon, D.; Rodriguez, H.C.; Grewal, G.; Lewis, S.; Lapica, H.; Levy, J.C. Comparison of reverse shoulder arthroplasty and total shoulder arthroplasty for patients with inflammatory arthritis. J. Shoulder Elb. Surg. 2022, 32, 573–580. [Google Scholar] [CrossRef]
- Cerciello, S.; Corona, K.; Morris, B.J.; Paladini, P.; Porcellini, G.; Merolla, G. Shoulder arthroplasty to address the sequelae of anterior instability arthropathy and stabilization procedures: Systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2020, 140, 1891–1900. [Google Scholar] [CrossRef] [PubMed]
- Dekker, T.J.; Steele, J.R.; Vinson, E.V.; Garrigues, G.E. Current peri-operative imaging concepts surrounding shoulder arthroplasty. Skelet. Radiol. 2019, 48, 1485–1497. [Google Scholar] [CrossRef]
- Sperling, J.W. Pearls and Tips in Shoulder Arthroplasty. Clin. Orthop. Surg. 2019, 11, 258–264. [Google Scholar] [CrossRef]
- Konin, G.P. Imaging of Shoulder Arthroplasty. Semin. Musculoskelet. Radiol. 2015, 19, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Elsharkawi, M.; Cakir, B.; Reichel, H.; Kappe, T. Reliability of radiologic glenohumeral osteoarthritis classifications. J. Shoulder Elb. Surg. 2013, 22, 1063–1067. [Google Scholar] [CrossRef]
- Linke, P.M.; Zemke, K.; Ecker, N.U.; Neumann, J.; Werner, A.W. Standard radiological classification of glenohumeral osteoarthritis does not correlate with the complexity of the arthritic glenoid deformity. Arch. Orthop. Trauma Surg. 2021, 142, 1413–1420. [Google Scholar] [CrossRef]
- Ashir, A.; Lombardi, A.; Jerban, S.; Ma, Y.; Du, J.; Chang, E.Y. Magnetic resonance imaging of the shoulder. Pol. J. Radiol. 2020, 85, e420–e439. [Google Scholar] [CrossRef]
- Porcellini, G.; Micheloni, G.M.; Tarallo, L.; Paladini, P.; Merolla, G.; Catani, F. Custom-made reverse shoulder arthroplasty for severe glenoid bone loss: Review of the literature and our preliminary results. J. Orthop. Traumatol. 2021, 22, 2. [Google Scholar] [CrossRef]
- Schiffman, C.J.; Prabhakar, P.; Hsu, J.E.; Shaffer, M.L.; Miljacic, L.; Matsen, F.A. Assessing the Value to the Patient of New Technologies in Anatomic Total Shoulder Arthroplasty. J. Bone Jt. Surg. 2021, 103, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.C.; Ekelund, A.L.; Renfree, K.J.; Liu, P.T.; Chew, F.S. Radiologic Assessment of Reverse Shoulder Arthroplasty. Radiographics 2007, 27, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Gustas-French, C.; Petscavage-Thomas, J.; Bernard, S.A. Imaging of Shoulder Arthroplasties. Am. J. Roentgenol. 2018, 211, 485–495. [Google Scholar] [CrossRef]
- Walch, G.; Badet, R.; Boulahia, A.; Khoury, A. Morphologic study of the Glenoid in primary glenohumeral osteoarthritis. J. Arthroplast. 1999, 14, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Mori, D.; Abboud, J.A.; Namdari, S.; Williams, G.R. Glenoid bone loss in anatomic shoulder arthroplasty: Literature review and surgical technique. Orthop. Clin. N. Am. 2015, 46, 389–397. [Google Scholar] [CrossRef]
- Petscavage-Thomas, J. Preoperative planning and postoperative imaging in shoulder arthroplasty. Semin. Musculoskelet. Radiol. 2014, 18, 448–462. [Google Scholar] [CrossRef] [PubMed]
- Bercik, M.J.; Kruse, K., 2nd; Yalizis, M.; Gauci, M.-O.; Chaoui, J.; Walch, G. A modification to the Walch classification of the glenoid in primary glenohumeral osteoarthritis using three-dimensional imaging. J. Shoulder Elb. Surg. 2016, 25, 1601–1606. [Google Scholar] [CrossRef]
- Chen, K.C.; Chen, J.Y. All About Shoulder Arthroplasty: What Radiologists Should Know. Semin. Musculoskelet. Radiol. 2019, 23, 126–140. [Google Scholar] [CrossRef]
- Codsi, M.J.; Bennetts, C.; Gordiev, K.; Boeck, D.M.; Kwon, Y.; Brems, J.; Powell, K.; Iannotti, J.P. Normal glenoid vault anatomy and validation of a novel glenoid implant shape. J. Shoulder Elb. Surg. 2008, 17, 471–478. [Google Scholar] [CrossRef]
- Budge, M.D.; Lewis, G.S.; Schaefer, E.; Coquia, S.; Flemming, D.J.; Armstrong, A.D. Comparison of standard two-dimensional and three-dimensional corrected glenoid version measurements. J. Shoulder Elb. Surg. 2011, 20, 577–583. [Google Scholar] [CrossRef]
- Weatherby, P.J.; Efejuku, T.A.; Somerson, J.S. Complications After Anatomic Shoulder Arthroplasty: Revisiting Leading Causes of Failure. Orthop. Clin. N. Am. 2021, 52, 269–277. [Google Scholar] [CrossRef]
- Zhang, J.A.; Lam, P.H.; Beretov, J.; Murrell, G.A. A review of bone grafting techniques for glenoid reconstruction. Shoulder Elb. 2021, 14, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Favard, L.; Berhouet, J.; Walch, G.; Chaoui, J.; Lévigne, C. Superior glenoid inclination and glenoid bone loss: Definition, assessment, biomechanical consequences, and surgical options. Orthopade 2017, 46, 1015–1021. [Google Scholar] [CrossRef]
- Porcellini, G.; Tarallo, L.; Novi, M.; Spiezia, F.; Catani, F. Technology applications in shoulder replacement. J. Orthop. Traumatol. 2019, 20, 27. [Google Scholar] [CrossRef] [PubMed]
- Lilley, B.M.; Lachance, A.; Peebles, A.M.; Powell, S.N.; Romeo, A.A.; Denard, P.J.; Provencher, C.M.T. What is the deviation in 3D preoperative planning software? A systematic review of concordance between plan and actual implant in reverse total shoulder arthroplasty. J. Shoulder Elb. Surg. 2022, 31, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Kahn, T.; Chalmers, P.N. Proximal Humeral Bone Loss in Revision Shoulder Arthroplasty. Orthop. Clin. N. Am. 2019, 51, 87–95. [Google Scholar] [CrossRef]
- Roberts, C.C.; Metter, D.F.; Fox, M.G.; Appel, M.; Jawetz, S.T.; Morrison, W.B.; Nacey, N.; Said, N.; Stensby, J.D.; Subhas, N.; et al. ACR Appropriateness Criteria® Imaging After Shoulder Arthroplasty: 2021 Update. J. Am. Coll. Radiol. 2022, 19, S53–S66. [Google Scholar] [CrossRef]
- Gonzalez, J.-F.; Alami, G.B.; Baque, F.; Walch, G.; Boileau, P. Complications of unconstrained shoulder prostheses. J. Shoulder Elb. Surg. 2011, 20, 666–682. [Google Scholar] [CrossRef]
- Soliman, S.B.; Davis, J.J.; Muh, S.J.; Vohra, S.T.; Patel, A.; van Holsbeeck, M.T. Ultrasound evaluations and guided procedures of the painful joint arthroplasty. Skelet. Radiol. 2022, 51, 2105–2120. [Google Scholar] [CrossRef]
- Barreto, I.; Pepin, E.; Davis, I.; Dean, C.; Massini, T.; Rees, J.; Olguin, C.; Quails, N.; Correa, N.; Rill, L.; et al. Comparison of metal artifact reduction using single-energy CT and dual-energy CT with various metallic implants in cadavers. Eur. J. Radiol. 2020, 133, 109357. [Google Scholar] [CrossRef]
- Mohammadinejad, P.; Baffour, F.I.; Adkins, M.C.; Yu, L.; McCollough, C.H.; Fletcher, J.G.; Glazebrook, K.N. Benefits of iterative metal artifact reduction and dual-energy CT towards mitigating artifact in the setting of total shoulder prostheses. Skelet. Radiol. 2020, 50, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Koff, M.F.; Burge, A.J.; Potter, H.G. Clinical magnetic resonance imaging of arthroplasty at 1.5 T. J. Orthop. Res. 2020, 38, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Koch, K.M.; Lorbiecki, J.E.; Hinks, R.S.; King, K.F. A multispectral three-dimensional acquisition technique for imaging near metal implants. Magn. Reson. Med. 2009, 61, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Pauly, K.B.; Gold, G.E.; Pauly, J.M.; Hargreaves, B.A. SEMAC: Slice encoding for metal artifact correction in MRI. Magn. Reson. Med. 2009, 62, 66–76. [Google Scholar] [CrossRef]
- Nunes, J.; Andrade, R.B.; Azevedo, C.; Ferreira, N.V.; Oliveira, N.; Calvo, E.M.; Espregueira-Mendes, J.M.; Sevivas, N.M. Improved Clinical Outcomes After Lateralized Reverse Shoulder Arthroplasty: A Systematic Review. Clin. Orthop. Relat. Res. 2021, 480, 949–957. [Google Scholar] [CrossRef]
- Harrison, A.K.; Knudsen, M.; Braman, J.P. Hemiarthroplasty and Total Shoulder Arthroplasty Conversion to Reverse Total Shoulder Arthroplasty. Curr. Rev. Musculoskelet. Med. 2020, 13, 501–508. [Google Scholar] [CrossRef]
- Markes, A.R.; Cheung, E.; Ma, C.B. Failed Reverse Shoulder Arthroplasty and Recommendations for Revision. Curr. Rev. Musculoskelet. Med. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Fink, B.; Sevelda, F. Periprosthetic Joint Infection of Shoulder Arthroplasties: Diagnostic and Treatment Options. BioMed Res. Int. 2017, 2017, 4582756. [Google Scholar] [CrossRef]
- Funk, L.; Kadler, B.; Mehta, S. Propionibacterium acnes infection after shoulder surgery. Int. J. Shoulder Surg. 2015, 9, 139–144. [Google Scholar] [CrossRef]
- Paxton, E.S.; Green, A.; Krueger, V.S. Periprosthetic Infections of the Shoulder: Diagnosis and Management. J. Am. Acad. Orthop. Surg. 2019, 27, e935–e944. [Google Scholar] [CrossRef]
- Patel, M.S.; Singh, A.M.; Gregori, P.; Horneff, J.G.; Namdari, S.; Lazarus, M.D. Cutibacterium acnes: A threat to shoulder surgery or an orthopedic red herring? J. Shoulder Elb. Surg. 2020, 29, 1920–1927. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, G.E.; Zmistowski, B.; Cooper, A.M.; Green, A.; Hsu, J.; Ricchetti, E.; Namdari, S.; Frankle, M.; Gerber, C.; Tashjian, R.; et al. Proceedings from the 2018 International Consensus Meeting on Orthopedic Infections: The definition of periprosthetic shoulder infection. J. Shoulder Elb. Surg. 2019, 28, S8–S12. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, Y.; Kwon, Y.W. Total Shoulder Arthroplasty Utilizing the Subscapularis-Sparing Approach. Orthop. Clin. N. Am. 2020, 51, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Sardar, H.; Horner, N.S.; Al Mana, L.; Miller, B.S.; Khan, M.; Alolabi, B. Subscapularis-sparing approaches in shoulder arthroplasty: A systematic review. J. Orthop. 2021, 24, 165–172. [Google Scholar] [CrossRef]
- Miniaci, A.; Scarcella, M.J. Shoulder resurfacing for treatment of focal defects and diffuse osteoarthritis. Der Orthopäde 2021, 50, 112–118. [Google Scholar] [CrossRef]
- Hammond, G.; Tibone, J.E.; McGarry, M.H.; Jun, B.-J.; Lee, T.Q. Biomechanical Comparison of Anatomic Humeral Head Resurfacing and Hemiarthroplasty in Functional Glenohumeral Positions. J. Bone Jt. Surg. 2012, 94, 68–76. [Google Scholar] [CrossRef]
- Heuberer, P.R.; Brandl, G.; Pauzenberger, L.; Laky, B.; Kriegleder, B.; Anderl, W. Radiological changes do not influence clinical mid-term outcome in stemless humeral head replacements with hollow screw fixation: A prospective radiological and clinical evaluation. BMC Musculoskelet. Disord. 2018, 19, 28. [Google Scholar] [CrossRef]
- Sajadi, K.R.; Kwon, Y.W.; Zuckerman, J.D. Revision shoulder arthroplasty: An analysis of indications and outcomes. J. Shoulder Elb. Surg. 2010, 19, 308–313. [Google Scholar] [CrossRef]
- Papadonikolakis, A.; Neradilek, M.B.; Matsen, F.A., 3rd. Failure of the glenoid component in anatomic total shoulder arthroplasty: A systematic review of the English-language literature between 2006 and 2012. J. Bone Joint Surg. Am. 2013, 95, 2205–2212. [Google Scholar] [CrossRef]
- Paras, T.; Raines, B.; Kohut, K.; Sabzevari, S.; Chang, Y.-F.; Yeung, M.; Li, R.; Tublin, J.; Baradaran, A.; Lin, A. Clinical outcomes of reverse total shoulder arthroplasty for elective indications versus acute 3- and 4-part proximal humeral fractures: A systematic review and meta-analysis. J. Shoulder Elb. Surg. 2021, 31, e14–e21. [Google Scholar] [CrossRef]
- Coscia, A.C.; Matar, R.N.; Espinal, E.E.; Shah, N.S.; Grawe, B.M. Does preoperative diagnosis impact patient outcomes following reverse total shoulder arthroplasty? A systematic review. J. Shoulder Elb. Surg. 2021, 30, 1458–1470. [Google Scholar] [CrossRef] [PubMed]
- Burden, E.G.; Pennington, S.D.; Nyffeler, R.W. Reverse total shoulder arthroplasty. Bone Jt. J. 2021, 103, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Heifner, J.J.; Kumar, A.D.; Wagner, E.R. Glenohumeral osteoarthritis with intact rotator cuff treated with reverse shoulder arthroplasty: A systematic review. J. Shoulder Elb. Surg. 2021, 30, 2895–2903. [Google Scholar] [CrossRef] [PubMed]
- Lopiz, Y.; Alcobía-Díaz, B.; Galán-Olleros, M.; García-Fernández, C.; Picado, A.L.; Marco, F. Reverse shoulder arthroplasty versus nonoperative treatment for 3- or 4-part proximal humeral fractures in elderly patients: A prospective randomized controlled trial. J. Shoulder Elb. Surg. 2019, 28, 2259–2271. [Google Scholar] [CrossRef]
- Lau, S.C.; Large, R. Acromial fracture after reverse total shoulder arthroplasty: A systematic review. Shoulder Elb. 2019, 12, 375–389. [Google Scholar] [CrossRef] [PubMed]
- Nyffeler, R.W.; Altioklar, B.; Bissig, P. Causes of acromion and scapular spine fractures following reverse shoulder arthroplasty: A retrospective analysis and literature review. Int. Orthop. 2020, 44, 2673–2681. [Google Scholar] [CrossRef]
- Torrens, C.; Guirro, P.; Miquel, J.; Santana, F. Influence of glenosphere size on the development of scapular notching: A prospective randomized study. J. Shoulder Elb. Surg. 2016, 25, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Sirveaux, F.; Favard, L.; Oudet, D.; Huquet, D.; Walch, G.; Mole, D. Grammont inverted total shoulder arthroplasty in the treatment of glenohumeral osteoarthritis with massive rupture of the cuff. Results of a multicentre study of 80 shoulders. J. Bone Jt. Surg. 2004, 86, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Torrens, C.; Miquel, J.; Martínez, R.; Santana, F. Can small glenospheres with eccentricity reduce scapular notching as effectively as large glenospheres without eccentricity? A prospective randomized study. J. Shoulder Elb. Surg. 2019, 29, 217–224. [Google Scholar] [CrossRef]
- Van de Kleut, M.L.; Yuan, X.; Teeter, M.G.; Athwal, G.S. Bony increased-offset reverse shoulder arthroplasty vs. metal augments in reverse shoulder arthroplasty: A prospective, randomized clinical trial with 2-year follow-up. J. Shoulder Elb. Surg. 2022, 31, 591–600. [Google Scholar] [CrossRef]
- Favard, L. Revision of total shoulder arthroplasty. Orthop. Traumatol. Surg. Res. 2013, 99 (Suppl. S1), S12–S21. [Google Scholar] [CrossRef] [PubMed]
- Dines, J.S.; Fealy, S.; Strauss, E.J.; Allen, A.; Craig, E.V.; Warren, R.F.; Dines, D.M. Outcomes analysis of revision total shoulder replacement. J. Bone Jt. Surg. Am. 2006, 88, 1494–1500. [Google Scholar] [CrossRef]
- Erickson, B.J. Failed Reverse Total Shoulder Arthroplasty: What Are Our Bailouts? Curr. Rev. Musculoskelet. Med. 2021, 14, 291–296. [Google Scholar] [CrossRef] [PubMed]






























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Description |
|---|---|
| A1 | Mild central glenoid erosion with the humeral head centrally positioned. |
| A2 | Major central glenoid erosion with the humeral head centrally positioned; a line that connects the native anterior and posterior glenoid rims transects the humeral head. |
| B1 | No glenoid erosion; posteriorly subluxed humeral head with posterior joint space narrowing and osteophytes. |
| B2 | Biconcave glenoid due to posterior erosion and retroversion, with posteriorly subluxed humeral head. |
| B3 | Monoconcave glenoid with significant posterior glenoid wear with retroversion of at least 15 degrees or subluxation of 70% or both. |
| C | Retroverted glenoid with glenoid dysplasia. |
| D | Anteverted glenoid or anteriorly subluxed humeral head. |
| Grade | Finding |
|---|---|
| 1 | Lucency extends to scapular pillar |
| 2 | Lucency contacts the inferior glenoid screw |
| 3 | Lucency extends over the inferior glenoid screw |
| 4 | Lucency extends under the metaglene/baseplate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weaver, J.S.; Omar, I.M.; Chadwick, N.S.; Shechtel, J.L.; Elifritz, J.M.; Shultz, C.L.; Taljanovic, M.S. Update on Shoulder Arthroplasties with Emphasis on Imaging. J. Clin. Med. 2023, 12, 2946. https://doi.org/10.3390/jcm12082946
Weaver JS, Omar IM, Chadwick NS, Shechtel JL, Elifritz JM, Shultz CL, Taljanovic MS. Update on Shoulder Arthroplasties with Emphasis on Imaging. Journal of Clinical Medicine. 2023; 12(8):2946. https://doi.org/10.3390/jcm12082946
Chicago/Turabian StyleWeaver, Jennifer S., Imran M. Omar, Nicholson S. Chadwick, Joanna L. Shechtel, Jamie M. Elifritz, Christopher L. Shultz, and Mihra S. Taljanovic. 2023. "Update on Shoulder Arthroplasties with Emphasis on Imaging" Journal of Clinical Medicine 12, no. 8: 2946. https://doi.org/10.3390/jcm12082946