1. Introduction
Age is an imprinted parameter both from a medical and legal point of view [
1,
2]. There are many surgical and non-surgical procedures where precise estimation is very important [
3]. In addition to medical issues, there are a wide range of non-medical subjects, e.g., legal problems and qualifications in competitive sports, where a precise age estimation is mandatory [
4,
5]. Legal issues become more important due to migration, especially in countries where birth records can be lost [
6,
7].
In the past century, it has emerged that the most accurate biological indicator of bone age is skeletal maturity. Bone age reflects the biological age of the patient, including hormonal and socioeconomic factors that are modulators of the growth and maturation of the child [
8,
9,
10]. Therefore, this may be different from chronological age, especially in cases where factors that affect development are pushed to extremes, such as stress, malnutrition, or endocrine disorders [
11]. With the development of radiological techniques, it has emerged that methods used for bone scanning could also be used for age determination. Therefore, X-ray-based techniques have emerged, exclusively in upper- and middle-class Caucasian populations [
12,
13], which nowadays gain criticism for their applicability due to racial and social differences [
14,
15,
16,
17,
18]. With the advent of modern diagnostic techniques, there are attempts to use them in scanning for the estimation of the age of patients. Additionally, as a consequence, ultrasound, magnetic resonance (MR), and even computed tomography (CT) were employed [
19,
20,
21,
22,
23]. The MR approach is of great interest because it is radiation-free and provides a detailed representation of tissues, including growth plates and nuclei [
24,
25,
26]. The texture of such an image reflects the bone structure that is visualized in MR images. Textures represent complex patterns that are coded in the data and are built from points of different brightness and distribution. The distribution of the pixels and their characteristics can be analyzed by many textural features [
27,
28], such as phase frequency, coarseness, and regularity of randomness direction, to name a few [
1]. Careful analysis of the initial textural pattern provides standardized feature extraction, which goes beyond the recognizable abilities of the human eye [
29,
30,
31], allowing quantitative analysis of various medical images [
32,
33]. Changes in the growth zone and bone marrow composition reflect the maturation of the long bone as the site of dynamic morphological changes [
34,
35,
36,
37,
38].
Since a bone age assessment is of great importance, this topic has been addressed in order to support physicians with an automated analysis of the data, making this task less labor intensive. In the literature, there are many approaches to address this problem, when analyzing X-ray images of hands [
39,
40,
41,
42,
43,
44,
45], the chest [
40,
46], or whole-body images [
47,
48]. In the case of a fully automated deep learning approach, first the hand region was determined in the image using the U-Net network for semantic segmentation of the hand region, then the image registration was applied to allow for an easy determination of hand regions corresponding to each other between various images. Here, a deep learning approach for key point selection was also adopted. Finally, another network was used to solve the regression task and predict age. A similar pipeline was introduced in previous studies [
40,
44,
45], yet the authors underlined the importance of transfer learning when preparing regression models. There were also approaches that used one network for the evaluation of bone age, as presented in the research in which whole-body scans were analyzed using well-known deep architectures, such as VGGNet, GoogLeNet, and ResNet, to find the best solution [
47], or the hand X-ray image was analyzed with the attention-Xception network [
43]. In [
46] not only was the age determined from the chest radiograph images, but also, they analyzed the activation maps to find the most characteristic regions that influence the patient’s age. Instead of using regression models, generative adversarial networks (GANs) were exploited to decide bone age [
42]. It was also possible to estimate the age from the bone mineral density at Ward’s triangle and the trabecular volume measured in the iliac crest [
49,
50]. We should not resign from more traditional approaches based on histogram thresholding, which allowed a precise determination of the chondorous part of the growth plate [
51,
52,
53].
Most bone age assessment techniques implement X-ray-based imaging modalities that are invasive to some extent for patients. In this work, we would like to test whether other, non-invasive imaging techniques enable an accurate age estimation from acquired images that contain bone tissue. The aim of the present study was to explore whether the long bone textural analysis of the growth region on MRI images reflects changes in the age of the child and can possibly be applied for the determination of the bone age. To perform that examination, a dedicated database of MRI scans of adolescent hands was prepared. The descriptive region in the scan was marked manually, and then the textural features were extracted and the regression analysis was applied.
3. Results
Table 2 and
Table 3 collect the best results obtained after applying a two-layer neural network from the Matlab Regression Learner toolbox. The visualization of the results is depicted in
Figure 3 and
Figure 4. The results presented in
Table 2 and
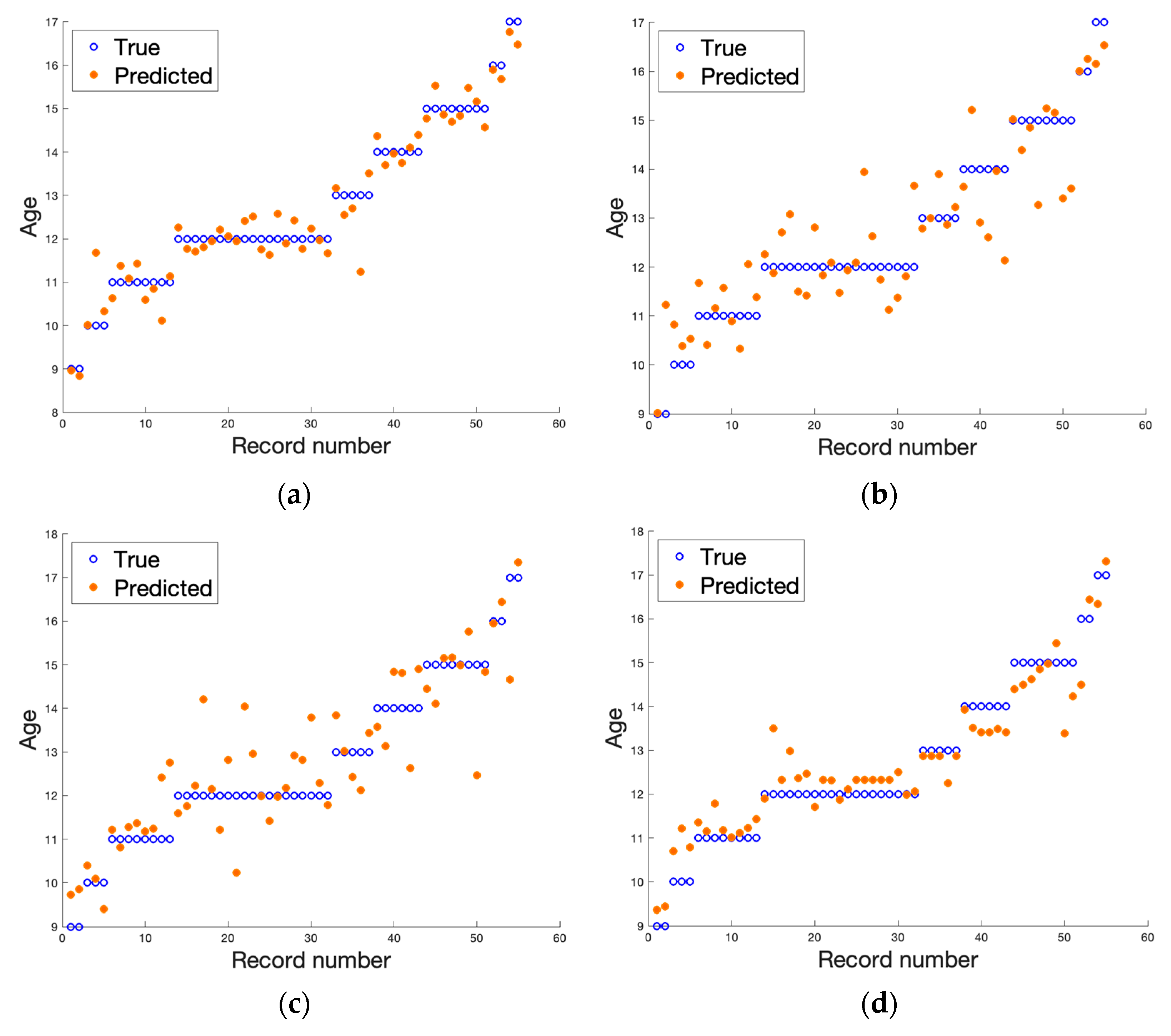
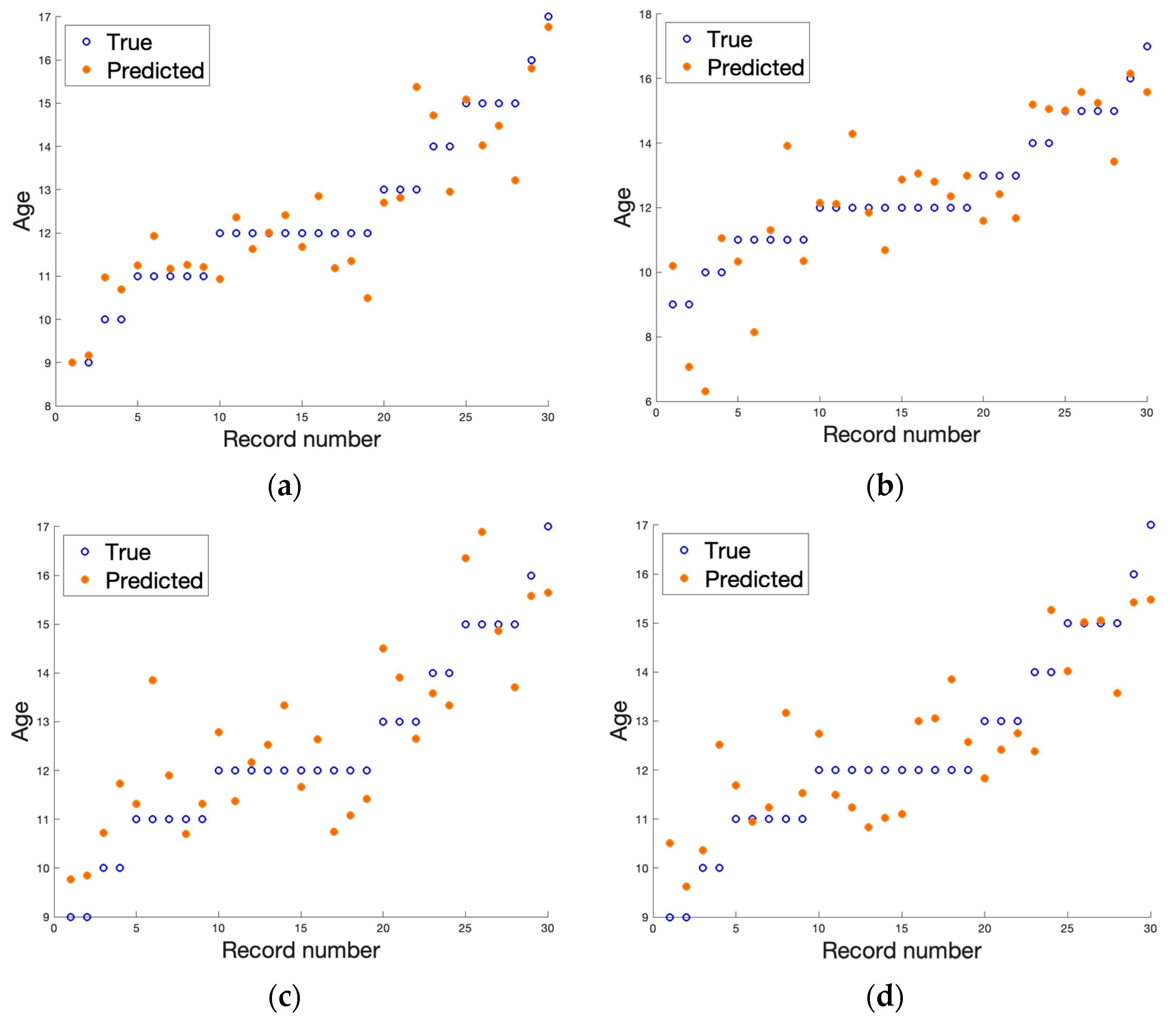
Table 3 are the average values of the regression errors obtained for each of the samples. The plots summarize the results of all the LOO trials. From the results presented, we can see that the regression analysis in all cases allowed the prediction of the age of a patient based on the textural features analysis of the MRI data. The gathered results suggest that, considering the bone region, we achieved more stable results with fewer errors. However, due to the limited amount of data, these discrepancies between the analyzed regions could be due to decreasing the number of samples from 55 (for the bone) to 30 (for the growth region). The dispersion coefficient is very high, yet significantly better results were obtained when a T1-weighted image using the original 12-bit DICOM data was considered. We achieved the best score, which was R2 equal to 0.94 for the original 12-bit representation (DICOM) when the bone region was evaluated. In this scenario, second place was taken by the T2-weighted image with a reduced number of bits to eight (R2 equals 0.87). When analyzing the results obtained for the growth region (see
Table 3), again, the T1-weighted image in 12-bit format returns the best outcomes, yet other results deteriorate significantly. This finding was also reflected in the other error metrics showing the smallest error in the case of DICOM T1-weighted datasets (see bold font in
Table 2 and
Table 3). The slight difference in the quality of age prediction by the chosen regressors was also noticeable in the plots presented in
Figure 3 and
Figure 4. Here, the predictions go through all observations in the case of analyzing textural features from bone DICOM T1-weighted images (see
Figure 3a) and are very close to this line when the growth region DICOM T1-weighted images are considered (see
Figure 4a). Since the true age was rounded to an integer value, the small discrepancies should not be surprising, as in reality, patients had a different number of months. As we noticed previously, the data reflected better when a shorter period was considered.
4. Discussion
Radiographic techniques are well-established methods that are used for the determination of bone age [
12,
13]. There are techniques that are based not only on the wrist estimation but also on other parts of the skeleton, including the clavicle [
65], elbow [
66], pelvis [
67,
68], humerus [
69], or calcaneus [
70,
71]. Dental studies become a focus as body parts are used for age estimation [
72,
73,
74].
Moreover, with the development of computer hardware, different techniques were proposed to obtain information from the image, allowing for the creation of efficient age evaluation systems, for example, Shorthand and BoneXpert to name a few [
75,
76]. There are many modern techniques that are based on shape extraction algorithms with comparative techniques, including those based on artificial intelligence [
77,
78,
79,
80]. However, many of these methods are still based on an X-ray analysis, where X-ray dose issues cannot be omitted.
Age determination based on a single radiograph is associated with low doses [
81]. However, a cumulative dose in cases where multiple X-rays must be performed might not be acceptable. Ultrasonography, however, which is free from radiation and easy to use, is known as an operator-dependent method, which is a serious drawback of this otherwise useful technique [
82].
MR was proposed as a method free of radiation exposure, but it is also repetitive, and in this regard, according to the results, it is stable.
Table 4 provided a comparison of the MAE metric for our solution and other approaches working on X-ray data. As we can see, it outperformed other methods markedly. A certain drawback of MRIs is the time needed for the exam, which forces cooperation with young patients. Regarding the success of the MR examination, parental assistance is very important [
24]. Child safety and comfort was assured in this study. That was very important as unintentional movement caused by inconvenient body alignment disturbs image creation. This is especially important in a proposed method where a small region of interest in the growth plate is used; therefore, a perfect image is key to the success of the proposed solution. Child cooperation is mandatory. However as described by Terada et al. [
23] and Dvorak et al [
22], short exam time was sufficient condition to ensure the creation of proper images. In our study, in contradiction to the protocol proposed by Dvorak et al. [
22], Hojreh et al. [
26], Stern et al. [
83], and Quasim et al. [
84], in addition to the T1-weighted spin echo and the gradient echo sequence (as applied in [
23,
24]), a T2-weighted spin echo was used. The choice of a T2-weighted sequence was dictated by the need to discriminate the number of watery progenitor cells because the amount of signals from these watery compounds was used as an indicator of the immaturity of the growth zone. The dependence of the growth zone composition on age with possible detection with the MR technique was described in experimental and clinical studies by Ecklund et al. [
85], who described the dependence of the signal of the growth region composition. This agrees with histological studies proposed by Ballock et al. [
86] and Breur et al. [
87], who precisely described the basis of the known fact that the pattern of ongoing calcification of the growth region reflects maturation with age, which is at the core of the signal changes that are analyzed in our study as one of the discriminators of long bone maturation. In a study by Yun et al. [
88], the dependence between the MR growth plate signal assessed in MR and skeletal maturation was not presented; however, the authors performed a study in the younger children group. One must remember that the proposed analysis of the growth plate is based on the narrow tissue element of progenitor cells, which is less than 3 mm and is a niche compared to the surrounding bone [
89,
90].
Despite the relatively low volume of the growth region in the composition of highly watery cells, it is highly detectable by high MR sequences, which in the image analysis, were reflected by a high correlation with histogram parameters (a sensitive indicator of brightness distribution but not necessarily structure) and supported by the presented regression analysis. This is logical because, in the zone of highly watery progenitor cells, the defined structure is very sparse, but the signal is strong. It can be observed that the younger the patient (with a wider growth region and more fluid), the brighter the signal. In older children, the amount of watery progenitor cells was reduced at the expense of the calcified bone rim, with a subsequent reduction in the influence of the bright area.
In a comparison of the T1-weighted and T2-weighted sequences, regression occurred more accurately for T1-weighted images than for T2-weighted signals, which is at least in part due to a high tissue contrast created between less hydrated trabeculae due to hydroxyapatite and therefore, low signal bone elements and high signal bone marrow [
37,
38]. The discriminative effect of the T2-weighted image due to the good differentiation between the unconverted bone marrow and the trabeculae can be partially spoiled by shift artifacts due to chemical composition, but also by the thickness of the trabeculae [
91,
92].
A slight influence on the results was observed regarding the type of encoding, the DICOM format was better with the T1-weighted sequence, which might be due to the overall contrast in the image where the T1-weighted sequence sensitive to water produces high signal differentiation in the image that is associated with a significant amount of blood morphotic elements in the immature marrow. This observation is consistent with clinical observations where sequences with a high TR time are used to differentiate lesions due to high visual contrast [
93]. It is also worth mentioning that comparing different MRI sequences is problematic; however, there are works showing that the registration of two series of MRI data is possible to some extent [
94].
Recently, new algorithms for automated bone marrow segmentation from MRI data have been developed [
95,
96]. We are going to implement such algorithms in our future research, especially when a large image database will be collected. The challenge will be to modify these algorithms in such a way as to select a specific ROI from the segmented, whole bone marrow. We know that radiomic features are prone to many problems. One of them is the low repeatability of texture features when multicenter studies are performed. On the other hand, such studies are essential to ensure the reliable validation of the developed machine learning models. It was shown in [
97] that normalization applied to muscle tissue images acquired by different MR scanners improved the reproducibility of the calculated selected texture features. We will further investigate the influence of various ROI normalization schemes’ texture feature repeatability and reproducibility. Another factor that affects the calculation of bone marrow radiomic features is the variation of signal intensity between different scanners [
98] as well as its dependence on signal blur phenomena. It is mostly caused by a chemical shift and magnetic susceptibility artifact, which belong to a class of tissue-specific artifacts. Other, less important might be also geometric artifacts that come from tissue tilt. Bone marrow analysis is always challenging and requires optimal image acquisition and compensation of acquisition artifacts.
There are some limitations to this study. First, the image acquisition was relatively long. However, the scanning time was successfully overcome by the cooperative and motivated children. Since it was a pilot study and we only wanted to verify the hypothesis that it is possible to determine the bone age with high accuracy from the MRI images, a small group of patients was examined. For further studies, it should be extended. Finally, the error in the segmentation of the growth plate must be considered, given the small area of interest and the averaging effect due to the influence of the surrounding tissues.

 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}



