
The Effect of Domiciliary Professional Oral Care on Root Caries Progression in Care-Dependent Older Adults: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.2. Search Strategy
2.3. Quality Assessment and Overall Risk of Bias
2.4. Data Extraction and Data Analysis
3. Results
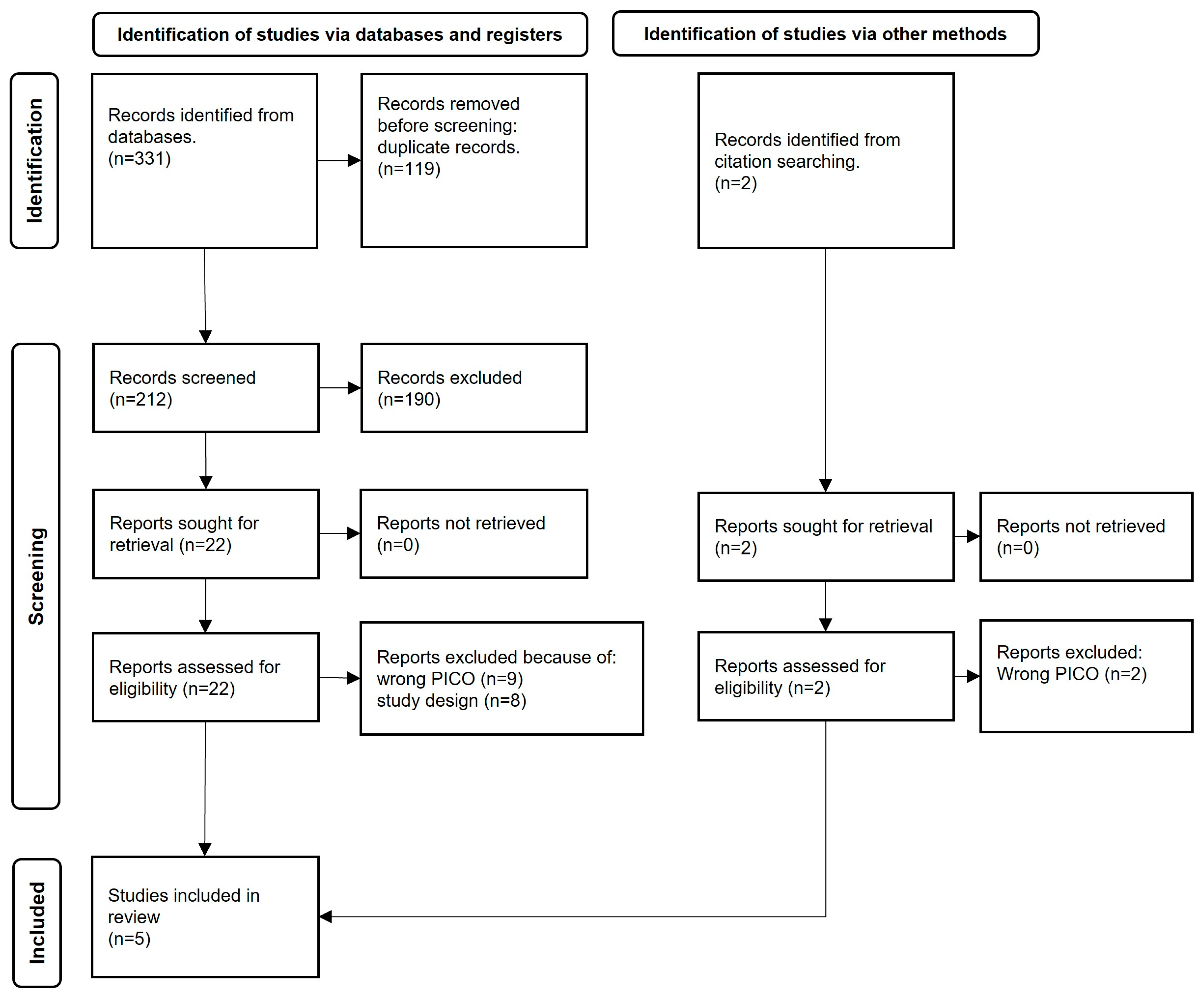
3.1. Search Results
3.2. Risk of Bias
3.3. Interventions
3.4. Analysis
Root Caries Index
3.5. Root Caries Development and Progression
4. Discussion
4.1. Active Participation of Dental Personnel
4.2. Training Nursing Staff
4.3. Awareness and Information among the Older Adults
5. Conclusions
6. Clinical Relevance
7. Supporting Information
8. Difference between Protocol and Review
Supplementary Materials
Author Contributions
Funding
Institutional review board statement
Informed consent statement
Data availability statement
Acknowledgments
Conflicts of Interest
References
- Silva, M.; Hopcraft, M.; Morgan, M. Dental caries in Victorian nursing homes. Aust. Dent. J. 2014, 59, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Rapp, L.; Maret, D.; Diemer, F.; Lacoste Ferré, M.H. Dental Caries in Geriatric Dentistry: An Update for Clinicians. Int. J. Oral Dent. Health 2019, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Leung, K.C.M.; Sardana, D.; Wong, M.C.M.; Lo, E.C.M. Risk predictors of dental root caries: A systematic review. J. Dent. 2019, 89, 103166. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.V.; Shugars, D.A.; Bader, J.D. Root caries risk indicators: A systematic review of risk models. Community Dent. Oral Epidemiol. 2010, 38, 383–397. [Google Scholar] [CrossRef]
- Kumar, S.; Tadakamadla, J.; Johnson, N.W. Effect of Toothbrushing Frequency on Incidence and Increment of Dental Caries: A Systematic Review and Meta-Analysis. J. Dent. Res. 2016, 95, 1230–1236. [Google Scholar] [CrossRef] [Green Version]
- Walsh, T.; Worthington, H.V.; Glenny, A.M.; Marinho, V.C.; Jeroncic, A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst. Rev. 2019, 3, CD007868. [Google Scholar] [CrossRef]
- Burrow, M.F.; Stacey, M.A. Management of Cavitated Root Caries Lesions: Minimum Intervention and Alternatives. Monogr. Oral Sci. 2017, 26, 106–114. [Google Scholar] [CrossRef]
- Bashir, N.Z. Update on the prevalence of untreated caries in the US adult population, 2017–2020. J. Am. Dent. Assoc. 2022, 153, 300–308. [Google Scholar] [CrossRef]
- Gavriilidou, N.N.; Belibasakis, G.N. Root caries: The intersection between periodontal disease and dental caries in the course of ageing. Br. Dent. J. 2019, 227, 1063–1067. [Google Scholar] [CrossRef]
- Pentapati, K.C.; Siddiq, H.; Yeturu, S.K. Global and regional estimates of the prevalence of root caries—Systematic review and meta-analysis. Saudi Dent. J. 2019, 31, 3–15. [Google Scholar] [CrossRef]
- The Swedish National Board o Health and Welfare. “Nationella Riktlinjer för Tandvård—Stöd för Styrning Och Ledning”. Socialstyrelsen. 2021. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/nationella-riktlinjer/2021-9-7549.pdf (accessed on 10 June 2022).
- Meyer-Lueckel, H.; Machiulskiene, V.; Giacaman, R.A. How to Intervene in the Root Caries Process? Systematic Review and Meta-Analyses. Caries Res. 2019, 53, 599–608. [Google Scholar] [CrossRef]
- Ekstrand, K.R.; Poulsen, J.E.; Hede, B.; Twetman, S.; Qvist, V.; Ellwood, R.P. A randomized clinical trial of the anti-caries efficacy of 5000 compared to 1450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013, 47, 391–398. [Google Scholar] [CrossRef]
- European Commission. One Hundred Words for Equality: A Glossary of Terms on Equality between Women and Men; Office for Official Publications of the European Communities: Luxembourg, 1998. [Google Scholar]
- Dixe, M.d.A.C.R.; Frontini, R.; Sousa, P.M.L.; Peralta, T.d.J.d.A.; Teixeira, L.F.d.C.; Querido, A.I.F. Dependent person in self-care: Analysis of care needs. Scand. J. Caring Sci. 2020, 34, 727–735. [Google Scholar] [CrossRef] [Green Version]
- Wårdh, I.; Jonsson, M.; Wikstrom, M. Attitudes to and knowledge about oral health care among nursing home personnel--an area in need of improvement. Gerodontology 2012, 29, e787–e792. [Google Scholar] [CrossRef]
- Sjögren, P.; Girestam, C.; Skott, P.; Marsson, N.; Nova, R.; Zimmerman, M.; Wårdh, I. Professional Domiciliary Oral Care for Elderly in Nursing Homes—A Randomized Controlled Pilot Trial. Health 2016, 8, 1112–1119. [Google Scholar] [CrossRef] [Green Version]
- Gronbeck-Linden, I.; Hagglin, C.; Petersson, A.; Linander, P.O.; Gahnberg, L. Discontinued dental attendance among elderly people in Sweden. J. Int. Soc. Prev. Community Dent. 2016, 6, 224–229. [Google Scholar] [CrossRef]
- Fereshtehnejad, S.M.; Garcia-Ptacek, S.; Religa, D.; Holmer, J.; Buhlin, K.; Eriksdotter, M.; Sandborgh-Englund, G. Dental care utilization in patients with different types of dementia: A longitudinal nationwide study of 58,037 individuals. Alzheimers Dement. 2018, 14, 10–19. [Google Scholar] [CrossRef]
- Li, R.; Lo, E.C.; Liu, B.Y.; Wong, M.C.; Chu, C.H. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J. Dent. 2016, 51, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Ástvaldsdóttir, Á.; Boström, A.M.; Davidson, T.; Gabre, P.; Gahnberg, L.; Sandborgh Englund, G.; Skott, P.; Ståhlnacke, K.; Tranaeus, S.; Wilhelmsson, H.; et al. Oral health and dental care of older persons-A systematic map of systematic reviews. Gerodontology 2018, 35, 290–304. [Google Scholar] [CrossRef]
- Chalmers, J.; Pearson, A. Oral hygiene care for residents with dementia: A literature review. J. Adv. Nurs. 2005, 52, 410–419. [Google Scholar] [CrossRef]
- Zhang, W.; McGrath, C.; Lo, E.C.; Li, J.Y. Silver diamine fluoride and education to prevent and arrest root caries among community-dwelling elders. Caries Res. 2013, 47, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Oral Health Surveys—Basic Methods; WHO: Geneva, Switzerland, 2013; p. 125. ISBN 978-92-4-154864-9. Available online: https://www.who.int/oral_health/publications/9789241548649/en/ (accessed on 8 May 2020).
- Katz, R.V. Assessing root caries in populations: The evolution of the root caries index. J. Public Health Dent. 1980, 40, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.; Burke, F.; Allen, P.F. Incidence, Prevalence and Global Distribution of Root Caries. Monogr. Oral Sci. 2017, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fejerskov, O.; Luan, W.M.; Nyvad, B.; Budtz-Jorgensen, E.; Holm-Pedersen, P. Active and inactive root surface caries lesions in a selected group of 60- to 80-year-old Danes. Caries Res. 1991, 25, 385–391. [Google Scholar] [CrossRef]
- Mourad Ouzzani, H.H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. Available online: https://www.rayyan.ai/ (accessed on 6 August 2021). [CrossRef] [Green Version]
- Swedish Agency for Health Technology Assessment and Assessment of Social Service (SBU). Utvärdering av Metoder i Hälso- Och Sjukvården Och Insatser i Socialtjänsten: En Metodbok. 2020. Available online: https://www.sbu.se/metodbok (accessed on 24 May 2022).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Wyatt, C.C. A 5-year follow-up of older adults residing in long-term care facilities: Utilisation of a comprehensive dental programme. Gerodontology 2009, 26, 282–290. [Google Scholar] [CrossRef]
- Wyatt, C.C.L.; MacEntee, M.I. Caries management for institutionalized elders using fluoride and chlorhexidine mouthrinses. Community Dent. Oral Epidemiol. 2004, 32, 322–328. [Google Scholar] [CrossRef]
- Niessen, L.C. Chlorhexidine varnish, sodium fluoride varnish, and silver diamine fluoride solution can prevent the development of new root caries in elders living in senior homes in Hong Kong. J. Evid. Based Dent. Pract. 2012, 12, 95–96. [Google Scholar] [CrossRef]
- López, R.M.; Uribe, M.R.; Rodríguez, B.O.; Casasempere, I.V. Comparison between amine fluoride and chlorhexidine with institutionalized elders: A pilot study. Gerodontology 2013, 30, 112–118. [Google Scholar] [CrossRef]
- Yi Mohammadi, J.J.; Franks, K.; Hines, S. Effectiveness of professional oral health care intervention on the oral health of residents with dementia in residential aged care facilities: A systematic review protocol. JBI Database System. Rev. Implement. Rep. 2015, 13, 110–122. [Google Scholar] [CrossRef]
- Nct. Effectiveness on SDF Solution and PVP-I Combined NaF Varnish in Preventing Root Caries in Elders. 2018. Available online: https://clinicaltrials.gov/show/NCT03654820 (accessed on 10 September 2021).
- Mojon, P.; Rentsch, A.; Budtz-Jørgensen, E.; Baehni, P.C. Effects of an oral health program on selected clinical parameters and salivary bacteria in a long-term care facility. Eur. J. Oral Sci. 1998, 106, 827–834. [Google Scholar] [CrossRef]
- Ritter, A.V. The Efficacy of Fluoride on Root Caries Progression May Be Dose-dependent. J. Evid. Based Dent. Pract. 2013, 13, 177–179. [Google Scholar] [CrossRef]
- Marchesan, J.T.; Byrd, K.M.; Moss, K.; Preisser, J.S.; Morelli, T.; Zandona, A.F.; Jiao, Y.; Beck, J. Flossing Is Associated with Improved Oral Health in Older Adults. J. Dent. Res. 2020, 99, 1047–1053. [Google Scholar] [CrossRef]
- Barbe, A.G.; Küpeli, L.S.; Hamacher, S.; Noack, M.J. Impact of regular professional toothbrushing on oral health, related quality of life, and nutritional and cognitive status in nursing home residents. Int. J. Dent. Hyg. 2020, 18, 238–250. [Google Scholar] [CrossRef]
- MacEntee, M.I.; Silver, J.G.; Gibson, G.; Weiss, R. Oral health in a long-term care institution equipped with a dental service. Community Dent. Oral Epidemiol. 1985, 13, 260–263. [Google Scholar] [CrossRef]
- Pearson, A.; Chalmers, J. Oral hygiene care for adults with dementia in residential aged care facilities. JBI Libr. Syst. Rev. 2004, 2, 1–89. [Google Scholar] [CrossRef]
- Al-Nasser, L.; Lamster, I.B. Prevention and management of periodontal diseases and dental caries in the older adults. Periodontol 2000 2020, 84, 69–83. [Google Scholar] [CrossRef]
- Patel, R.; Khan, I.; Pennington, M.; Pitts, N.B.; Robertson, C.; Gallagher, J.E. Protocol for A randomised feasibility trial comparing fluoride interventions to prevent dental decay in older people in care homes (FInCH trial). BMC Oral Health 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- ISRCTN. A Randomised Controlled Trial to Evaluate the Cost Effectiveness of Prescribing High Concentration Fluoride Toothpaste to Prevent Tooth Decay in Older Adults. 2017. Available online: http://www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN11992428 (accessed on 10 September 2021).
- Raghoonandan, P.; Cobban, S.J.; Compton, S.M. A scoping review of the use of fluoride varnish in elderly people living in long term care facilities. Can. J. Dent. Hyg. 2011, 45, 217–222. [Google Scholar]
- Wikstrom, M.; Kareem, K.L.; Almstahl, A.; Palmgren, E.; Lingstrom, P.; Wardh, I. Effect of 12-month weekly professional oral hygiene care on the composition of the oral flora in dentate, dependent elderly residents: A prospective study. Gerodontology 2017, 34, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Jabir, E.; McGrade, C.; Quinn, G.; McGarry, J.; Nic Iomhair, A.; Kelly, N.; Srinivasan, M.; Watson, S.; McKenna, G.J. Evaluating the effectiveness of fluoride varnish in preventing caries amongst Long-Term Care Facility Residents. Gerodontology 2021, 39, 250–256. [Google Scholar] [CrossRef]
- Ekstrand, K.; Martignon, S.; Holm-Pedersen, P. Development and evaluation of two root caries controlling programmes for home-based frail people older than 75 years. Gerodontology 2008, 25, 67–75. [Google Scholar] [CrossRef]
- Barbe, A.G.; Kottmann, H.E.; Derman, S.H.M.; Noack, M.J. Efficacy of regular professional brushing by a dental nurse for 3months in nursing home residents—A randomized, controlled clinical trial. Int. J. Dent. Hyg. 2019, 17, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Brailsford, S.R.; Fiske, J.; Gilbert, S.; Clark, D.; Beighton, D. The effects of the combination of chlorhexidine/thymol- and fluoride-containing varnishes on the severity of root caries lesions in frail institutionalised elderly people. J. Dent. 2002, 30, 319–324. [Google Scholar] [CrossRef]
- Girestam Croonquist, C.; Dalum, J.; Skott, P.; Sjögren, P.; Wårdh, I.; Morén, E. Effects of Domiciliary Professional Oral Care for Care-Dependent Elderly in Nursing Homes—Oral Hygiene, Gingival Bleeding, Root Caries and Nursing Staff’s Oral Health Knowledge and Attitudes. Clin. Interv. Aging 2020, 15, 1305–1315. [Google Scholar] [CrossRef]
- Tan, H.P.; Lo, E.C.; Dyson, J.E.; Luo, Y.; Corbet, E.F. A randomized trial on root caries prevention in elders. J. Dent. Res. 2010, 89, 1086–1090. [Google Scholar] [CrossRef]
- Seifo, N.; Robertson, M.; MacLean, J.; Blain, K.; Grosse, S.; Milne, R.; Seeballuck, C.; Innes, N. The use of silver diamine fluoride (SDF) in dental practice. Br. Dent. J. 2020, 228, 75–81. [Google Scholar] [CrossRef]
- Burgess, J.O.; Vaghela, P.M. Silver Diamine Fluoride: A Successful Anticarious Solution with Limits. Adv. Dent. Res. 2018, 29, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Edman, K.; Wårdh, I. Oral health care beliefs among care personnel working with older people—Follow-up of oral care education provided by dental hygienists. Int. J. Dent. Hyg. 2022, 20, 241–248. [Google Scholar] [CrossRef]
- Weening-Verbree, L.F.; Schuller, D.A.A.; Cheung, S.L.; Zuidema, P.; Schans, P.; Hobbelen, D. Barriers and facilitators of oral health care experienced by nursing home staff. Geriatr. Nurs. 2021, 42, 799–805. [Google Scholar] [CrossRef]
- Doshi, M.; Lee, L.; Keddie, M. Effective mouth care for older people living in nursing homes. Nurs. Older People 2021, 33, 18–23. [Google Scholar] [CrossRef]
- Simons, D.; Baker, P.; Jones, B.; Kidd, E.A.; Beighton, D. An evaluation of an oral health training programme for carers of the elderly in residential homes. Br. Dent. J. 2000, 188, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Kiyak, H.A.; Reichmuth, M. Barriers to and enablers of older adults’ use of dental services. J. Dent. Educ. 2005, 69, 975–986. [Google Scholar] [CrossRef]
- Lamont, T.; Schwendicke, F.; Innes, N. Why we need a core outcome set for trials of interventions for prevention and management of caries. Evid.-Based Dent. 2015, 16, 66–68. [Google Scholar] [CrossRef]


{kind=link}
| Author, Year | Title | Where Published | Reason for Exclusion |
|---|---|---|---|
| Wyatt, 2009, [33] | A 5-year follow-up of older adults residing in long-term care facilities: utilization of a comprehensive dental program | Gerodontology. 2009;26(4):282–90. | Wrong PICO |
| Wyatt and MacEntee, 2004, [34] | Caries management for institutionalized elders using fluoride and chlorhexidine mouth rinses | Community Dentistry & Oral Epidemiology. 2004;32(5):322–8. | Wrong PICO |
| Niessen, 2012, [35] | Chlorhexidine varnish, sodium fluoride varnish, and silver diamine fluoride solution can prevent the development of new root caries in elders living in senior homes in Hong Kong | Journal of Evidence-Based Dental Practice. 2012;12(2):95–6. | Wrong study design |
| López, Uribe, Rodríguez, and Casasempere, 2013, [36] | Comparison between amine fluoride and chlorhexidine with institutionalized elders: a pilot study | Gerodontology. 2013;30(2):112–8. | Wrong PICO |
| Yi Mohammadi, Franks, and Hines, 2015, [37] | Effectiveness of professional oral health care intervention on the oral health of residents with dementia in residential aged care facilities: a systematic review protocol | JBI Database System Rev Implement Rep. 2015;13(10):110–22. https://doi.org/10.11124/jbisrir-2015-2330. | Wrong study design |
| ClinicalTrials.gov, 2018, [38] | Effectiveness on SDF solution and PVP-I combined NaF varnish in preventing root caries in elders | Available online: https://clinicaltrials.gov/ct2/show/NCT03654820 (accessed on 10 September 2021) | Wrong study design |
| Mojon, Rentsch, Budtz-Jørgensen, and Baehni, 1998, [39] | Effects of an oral health program on selected clinical parameters and salivary bacteria in a long-term care facility | Eur J Oral Sci. 1998;106(4):827–34. | Wrong PICO |
| Ritter, 2013, [40] | The efficacy of fluoride on root caries progression may be dose-dependent | Journal of Evidence-Based Dental Practice. 2013;13(4):177–9. | Wrong study design |
| Marchesan, Byrd, Moss, Preisser, Morelli, Zandona et al., 2020, [41] | Flossing is associated with improved oral health in older adults | Journal of Dental Research. 2020;99(9):1047–53. | Wrong PICO |
| Barbe, Küpeli, Hamacher, and Noack, 2020, [42] | Impact of regular professional toothbrushing on oral health, related quality of life, and nutritional and cognitive status in nursing home residents | International Journal of Dental Hygiene. 2020;18(3):238–50. | Wrong study design |
| MacEntee, Silver, Gibson, and Weiss, 1985, [43] | Oral health in a long-term care institution equipped with a dental service | Community Dentistry & Oral Epidemiology. 1985;13(5):260–3. | Wrong study design |
| Pearson and Chalmers, 2004, [44] | Oral hygiene care for adults with dementia in residential aged care facilities | JBI Library of Systematic Reviews. 2004;2(3):65–113. | Wrong PICO |
| Al-Nasser and Lamster, 2020, [45] | Prevention and management of periodontal diseases and dental caries in the older adults | Periodontology 2000. 2020;84(1):69–83. | Wrong study design |
| Patel, Khan, Pennington, Pitts, Robertson, Gallagher, 2021, [46] | Protocol for a randomized feasibility trial comparing fluoride interventions to prevent dental decay in older people in care homes (FInCH trial) | BMC Oral Health. 2021;21(1):1–12. | Wrong PICO |
| TrialSearch.com, 2017, [47] | A randomized controlled trial to evaluate the cost effectiveness of prescribing high concentration fluoride toothpaste to prevent tooth decay in older adults | Available online: https://www.who.int/trialsearch/Trial2.aspx?TrialID=ISRCTN11992428. 2017. (accessed on 10 September 2021) | Wrong PICO |
| Ekstrand, Poulsen, Hede, Twetman, Qvist, and Ellwood, 2013, [13] | A randomized clinical trial of the anti-caries efficacy of 5000 compared to 1450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents | Caries Research. 2013;47(5):391–8. | Wrong PICO |
| Raghoonandan, Cobban, and Compton, 2011, [48] | A scoping review of the use of fluoride varnish in elderly people living in long term care facilities | Canadian Journal of Dental Hygiene. 2011;45(4):217–22. | Wrong study design |
| Wikstrom, Kareem, Almstahl, Palmgren, Lingstrom, and Wardh, 2017, [49] | Effect of 12-month weekly professional oral hygiene care on the composition of the oral flora in dentate, dependent elderly residents: a prospective study | Gerodontology. 2017;34(2):240–8. | Wrong PICO |
| Jabir, McGrade, Quinn, McGarry, Nic Iomhair, Kelly et al., 2022, [50] | Evaluating the effectiveness of fluoride varnish in preventing caries amongst long-term care facility residents | Gerodontology. 2022;39:250–6. | Wrong PICO |
| Ekstrand, Martignon, and Holm-Pedersen, 2008, [51] | Development and evaluation of two root caries controlling programmes for home-based frail people older than 75 years | Gerodontology. 2008;25(2):67–75. | High risk of bias (RoB) |
| RoB 2 | Randomization process | Deviations from the intended interventions (effect of assignment to intervention) | Deviations from the intended interventions (effect of adhering to intervention) | Missing outcome data | Measurement of the outcome | Selection of the reported result | Conflict of interest | Conclusive judgment |
|---|---|---|---|---|---|---|---|---|
| Ekstrand et al., 2008 [51] |  |  | | |  | | | |
| Barbe et al., 2019 [52] | | | | | | | | |
| Brailsford et al., 2002 [53] | | | | | | | | |
| Girestam Croonquist et al., 2020 [54] | | | | | | | | |
| Tan et al., 2010 [55] | | | | | | | | |
| Author(s) | Barbe, Kottmann, Derman, and Noack [52] | Brailsford, Fiske, Gilbert, Clark, and Beighton [53] | Girestam Croonquist, Dalum, Skott, Sjögren, Wårdh, and Morén [54] | Tan, Lo, Dyson, Luo, and Corbet [55] |
|---|---|---|---|---|
| Year | 2019 | 2002 | 2020 | 2010 |
| Country | Germany | Great Britain | Sweden | China |
| Title | Efficacy of regular professional brushing by a dental nurse for 3 months in nursing home residents—a randomized, controlled clinical trial. | The effects of the combination of chlorhexidine/thymol- and fluoride-containing varnishes on the severity of RCLs in frail institutionalized elderly people. | Effects of domiciliary professional oral care for care-dependent elderly in nursing homes—oral hygiene, gingival bleeding, root caries and nursing staff’s oral health knowledge and attitudes. | A randomized trial on root caries prevention in elders. |
| Aim | To investigate the impact of professional brushing, performed every 2 weeks by a dental nurse, on the number of teeth, incidence of root caries, and further short-term oral health parameters, compared with residents whose oral hygiene was performed or supervised by staff according to standards of care corresponding to German law concerning the care for the elderly. | To determine the effect of a fluoride-containing varnish (Fluor protector) in combination with either Cervitec or a placebo varnish on the clinical characteristics of existing RCLs. | To describe the effects, for nursing home residents, of professional cleaning, and individual OHIs provided by registered dental hygienists, in comparison with daily oral care as usual. | To compare the effectiveness of the following four methods in preventing new root surface caries: (1) only OHIs every 3 months; (2) OHIs and applications of Cervitec varnish every 3 months; (3) OHIs and application of Duraphat every 3 months; (4) OHI and annual application of SDF solution. |
| Study design | RCT | Randomized double-blind longitudinal study | RCT | RCT |
| Primary outcome | Number of teeth | Root caries | Bleeding on probing (BoP), measured using the modified sulcus bleeding index (MSB) | Development of new caries on the exposed sound root surfaces of participants during the study period |
| Number (n) of participants at baseline | n = 50 | n = 121 | n = 146 | n = 306 |
| Mean age, yrs, ± standard deviation | 83 ± 8 | I = 85.6 ± 1.3 C = 79.8 ± 1.4 | 88.9 ± 4.1 | 78 ± 6.2 |
| Gender | Female n = 34 Male n = 16 | Female n = 65 Male n = 37 | Female n = 108 Male n = 38 | Female = 233 Male = 73 |
| Mean number of teeth | 17 ± 9 | I = 13.73 ± 1.07 C = 15.50 ± 1.06 | 20.2 ± 3.0 | 14.3 ± 6.5 |
| Study duration | 3 mo | 52 wks | 6 mo | 3 yrs |
| Number (n) of dropouts | n = 14 | n = 19 | n = 22 | n = 103 |
| Root caries index (RCI) | RCI (RCI1–RCI5), DMFT index | Length/distance from gingival margin, height, and width. | Fejerskov et al.’s five-level RCI [28] | RCI, DFS root score |
| Time of data examination | B + 3 mo | B + 13 wks + 26 wks + 1 yr | B + 3 mo + 6 mo | B + 1 yr + 2 yrs + 3 yrs |
| Intervention, and number (n) of participants at baseline | Professional brushing every second week by dental nurse, n = 25 | Fluor protector varnish with Cervitec at baseline and at 6, 13, 26, and 39 wks, n = 52 | Monthly professional cleaning, individual OHIs, and information, n = 72 | (1) OHI + Cervitec every 3 mo, n = 71; (2) OHI + Duraphat every 3 mo, n = 80; (3) OHI + SDF every 12 mo, n = 72 |
| Intervention performed by | Dental nurse | Dentist | Dental hygienist | Dentist |
| Control and number (n) of participants at baseline | Oral care as usual or nurse-assisted, n = 25 | Fluor protector varnish with placebo at baseline and at 6, 13, 26 and 39 wks, n = 50 | Oral care as usual or nurse-assisted, n = 74 | OHI—placebo (water) every 12 mo, n = 83 |
| Risk of bias (RoB) | Moderate | Moderate | Moderate | Moderate |
| Author(s), Year, Country | Results per Study | |||||||
|---|---|---|---|---|---|---|---|---|
| Barbe et al., 2019 [52], Germany | Study groups | Baseline | 3 mo | New RCLs | ||||
| I¹ group mean (SD) for RCI | 1.1 (1.2) | 1.3 (1.3) | RCI increased in the control group between baseline and 3 months (p = 0.006). | |||||
| C group mean (SD) for RCI | 1.5 (1.8) | 2.6 (1.3) | ||||||
| p-value | 0.433 | 0.002 * | ||||||
| Brailsford et al., 2002 [53], Great Britain | Baseline—1 yr | |||||||
| No new RCLs were detected in either the I2 or the c/placebo group. | ||||||||
| Girestam Croonquist et al., 2020 [54], Sweden | RCI | Baseline—3 mo | Baseline—6 mo | 3–6 mo | ||||
| I3 | C | I3 | C | I3 | C | |||
| Healthy n (%) | Deteriorated | 20 (28.6) | 24 (39.3) | 22 (31.9) | 15 (27.3) | 15 (21.7) | 9 (16.4) | |
| Unchanged | 38 (54.3) | 27 (44.3) | 32 (46.4) | 26 (47.3) | 33 (47.8) | 28 (50.9) | ||
| Improved | 12 (17.1) | 10 (16.4) | 15 (21.7) | 14 (25.5) | 21 (30.4) | 18 (32.7) | ||
| p-value | 0.41 | 0.84 | 0.76 | |||||
| Initial caries n (%) | Deteriorated | 15 (21.4) | 18 (29.5) | 20 (29.0) | 14 (25.5) | 20 (29.0) | 10 (18.2) | |
| Unchanged | 44 (62.9) | 30 (49.2) | 39 (56.5) | 31 (56.4) | 38 (55.1) | 36 (65.5) | ||
| Improved | 11 (15.7) | 13 (21.3) | 10 (14.5) | 10 (18.2) | 11 (15.9) | 9 (16.4) | ||
| p-value | 0.29 | 0.82 | 0.39 | |||||
| Active caries n (%) | Deteriorated | 9 (12.9) | 3 (4.9) | 7 (10.1) | 9 (16.4) | 11 (15.9) | 11 (20.0) | |
| Unchanged | 40 (57.1) | 37 (60.7) | 41 (59.4) | 32 (58.2) | 46 (66.6) | 42 (76.4) | ||
| Improved | 21 (30.0) | 21 (34.4) | 21 (30.4) | 14 (25.5) | 12 (17.4) | 2 (3.6) | ||
| p-value | 0.28 | 0.55 | 0.05 * | |||||
| Tan et al., 2010 [55], China | Study groups | Mean number/SE of new active root caries or fillings in each study group | ||||||
| 1 yr (n = 247) | 2 yrs (n = 227) | 3 yrs (n = 203) | ||||||
| OHI | 1.5 (SE 0.2) | 2.0 (SE 0.3) | 2.5 (SE 0.5) | |||||
| OHI + Cervitec | 1.0 (SE 0.2) | 1.0 (SE 0.3) | 1.1 (SE 0.2) | |||||
| OHI + Duraphat | 0.8 (SE 0.2) | 0.9 (SE 0.2) | 0.9 (SE 0.3) | |||||
| OHI + SDF | 0.4 (SE 0.1) | 0.7 (SE 0.2) | 0.7 (SE 0.2) | |||||
| All groups | 0.9 (SE 0.1) | 1.2 (SE 0.1) | 1.3 (SE 0.2) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morén, E.; Skott, P.; Edman, K.; Gavriilidou, N.; Wårdh, I.; Domeij, H. The Effect of Domiciliary Professional Oral Care on Root Caries Progression in Care-Dependent Older Adults: A Systematic Review. J. Clin. Med. 2023, 12, 2748. https://doi.org/10.3390/jcm12072748
Morén E, Skott P, Edman K, Gavriilidou N, Wårdh I, Domeij H. The Effect of Domiciliary Professional Oral Care on Root Caries Progression in Care-Dependent Older Adults: A Systematic Review. Journal of Clinical Medicine. 2023; 12(7):2748. https://doi.org/10.3390/jcm12072748
Chicago/Turabian StyleMorén, Elisabeth, Pia Skott, Kristina Edman, Nivetha Gavriilidou, Inger Wårdh, and Helena Domeij. 2023. "The Effect of Domiciliary Professional Oral Care on Root Caries Progression in Care-Dependent Older Adults: A Systematic Review" Journal of Clinical Medicine 12, no. 7: 2748. https://doi.org/10.3390/jcm12072748