
Comparison of the Administration Route of Stem Cell Therapy for Ischemic Stroke: A Systematic Review and Meta-Analysis of the Clinical Outcomes and Safety
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Type of Outcome Measurements
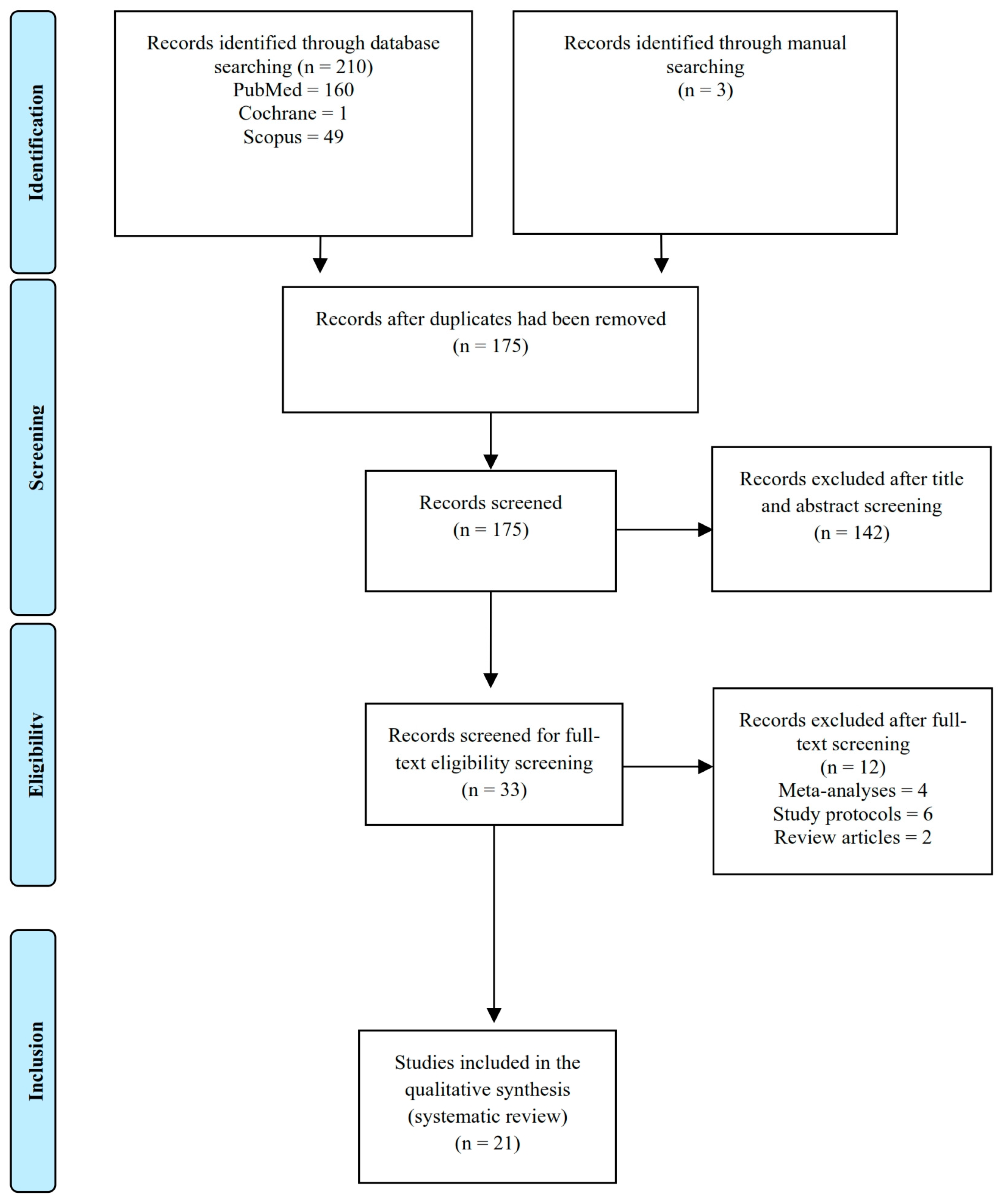
2.3. Search Methods and Identification of Studies
2.3.1. Information Sources
2.3.2. Search Protocol
2.4. Data Collection and Analysis
2.5. Data Extraction and Management
2.6. Risk of Bias Analysis

{kind=link}
{kind=link}
{kind=link}
| Author(s) | Study Design | Age (years) | Stroke Territory | Sample Size | Type of Graft | Number of Transplanted Cells | Route of Administration | Functional Outcome | Notes | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | 12 Months | 24 Months | |||||||||||||||||
| NIHSS | mRS | BI | NIHSS | mRS | BI | NIHSS | mRS | BI | NIHSS | mRS | BI | |||||||||
| Lee et al. (2010) [19] | RCT | 64.6 ± 13.6 | 52 MCA | 36 control | Autologous bone marrow MSC | 50 × 106 | Intravenous | 10.63 ± 3.00 | 4.80 ± 0.50 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Improvement in the early post-treatment phase, no improvement later on |
| 16 treatment | 10.17 ± 3.60 | 4.40 ± 0.90 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | ||||||||
| Honmou et al. (2011) [20] | Non-RCT | 60.5 (41–73) | 4 MCA 6 ICA 2 Lacunar | 12 treatment | Autologous bone marrow-derived MSC | 120 (60–160) × 106 | Intravenous | 8.25 ± 5.55 | n/a | n/a | n/a | n/a | n/a | 1.58 ± 2.02 | n/a | n/a | n/a | n/a | n/a | Significant improvement |
| Bhasin et al. (2012) [21] | Non-RCT | 46.58 ± 10.99 | 24 MCA | 12 control | Autologous bone marrow–derived MSC | 55 (50–58) × 106 | Intravenous | n/a | n/a | 49.92 ± 10.03 | n/a | n/a | 78.67 ± 11.35 | n/a | n/a | n/a | n/a | n/a | n/a | Significant improvement on modified BI only |
| 47.08 ± 9.90 | 12 treatment | n/a | n/a | 48.75 ± 10.57 | n/a | n/a | 69.75 ± 9.90 | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
| Prasad et al. (2012) [22] | Non-RCT | 54 (38–70) | 11 MCA | 11 treatment | Autologous bone marrow-derived MSC | 40 × 106 | Intravenous | 12.27 ± 5.16 | 3.45 ± 1.04 | 34.09 ± 22.23 | 4.80 ± 5.47 | 2.09 ± 1.30 | 79.09 ± 20.23 | n/a | n/a | n/a | n/a | n/a | n/a | Significant neurological outcome in the subacute stroke |
| Jiang et al. (2013) [23] | Prospective cohort | 48.5 (40–59) | 4 MCA | 4 treatment | Umbilical cord-derived MSC | 20 × 106 | Intra-arterial | n/a | 4.00 ± 0.816 | n/a | n/a | 3.25 ± 0.50 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Small size of samples; significant improvement |
| Banerjee et al. (2014) [24] | Non-RCT | 57 (45–75) | 4 MCA 1 PCA | 5 treatment | CD34 ± stem cell | 2.42 (1.2–2.79) × 106 | Intra-arterial | 10.40± 5.13 | 3.80 ± 0.84 | n/a | 2.20 ± 1.92 | 1.60 ± 1.14 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Significant improvement |
| Chen et al. (2014) [25] | RCT | 52.8 ± 9.0 | 30 MCA | 15 control | PBSC | (3–8) × 106 | Intracerebral | 9.60 ± 1.30 | 2.80 ± 0.40 | n/a | 9.40 ± 1.20 | 2.70 ± 0.50 | n/a | 8.70 ± 1.90 | 2.70 ± 0.50 | n/a | n/a | n/a | n/a | Significant clinical outcome improvement |
| 50.1 ± 7.7 | 15 treatment | 9.30 ± 0.50 | 2.90 ± 0.30 | n/a | 6.70 ± 1.70 | 2.50 ± 0.50 | n/a | 5.50 ± 1.80 | 2.10 ± 0.30 | n/a | n/a | n/a | n/a | |||||||
| Prasad et al. (2014) [26] | RCT | 18–75 | 60 control | Autologous bone marrow mononuclear stem cell | 280.75 × 106 | Intravenous | 11.00 ± 4.44 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Insignificant results | |
| 108 MCA 5 ACA 7 MCA+ACA | 60 treatment | 13.00 ± 4.44 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
| Qiao et al. (2014) [27] | Prospective cohort | 61.5 (45–85) | 5 MCA 1 ACA | 6 treatment | Umbilical cord mesenchymal stem cell | 0.5 × 106/kgbw | Intravenous | 8.17 ± 5.84 | 4.00 ± 1.10 | 40.83 ± 33.38 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Improved neurological function |
| Kalladka et al. (2016) [28] | Non-RCT | 78 (68–82) | 9 MCA 1 MCA+ACA 1 PCA | 3 (2 m) * | Human neural stem cell (CTX0E03) | 2 × 106 | Intracerebral | 7.67 ± 1.53 | 4.00 ± 0.00 | 11.00 ± 1.00 | 5.67 ± 2.08 | n/a | n/a | 4.33 ± 2.08 | n/a | 12.67 ± 1.15 | 5.67 ± 1.15 | n/a | 12.00 ± 1.73 | Improved neurological function; no controls |
| 69 (61–75) | 3 (5 m) * | 5 × 106 | 8.00 ± 2.00 | 3.67 ± 0.58 | 11.67 ± 2.52 | 6.33 ± 3.06 | n/a | n/a | 6.33 ± 2.89 | n/a | 14.67 ± 2.08 | 5.67 ± 4.04 | n/a | 14.33 ± 3.51 | ||||||
| 64 (60–68) | 3 (10 m) * | 10 × 106 | 7.33 ± 0.58 | 2.67 ± 0.58 | 14.33 ± 1.53 | 4.33 ± 0.58 | n/a | n/a | 4.67 ± 1.15 | n/a | 14.67 ±3.21 | 4.00 ± 1.73 | n/a | 13.33 ± 1.53 | ||||||
| 66 (61–71) | 2 (20 m) * | 20 × 106 | 6.50 ± 0.71 | 3.00 ± 0.00 | 13.50 ± 2.12 | 3.50 ± 2.12 | n/a | n/a | 3.50 ± 3.53 | n/a | 16 ± 2.83 | 4.00 ± 0.00 | n/a | 17.5 ± 3.53 | ||||||
| Hess et al. (2017) [29] | RCT | 18–33 | n/a | 63 control | Multipotent adult progenitor cell | (400–1200) × 106 | Intravenous | 13.40 ± 3.70 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Insignificant results |
| 71 treatment | 13.30 ± 3.50 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | ||||||||
| Jin et al. (2017) [30] | RCT | 53.10 ± 13.07 | 13 anterior circulation 7 posterior circulation | 10 control | Autologous bone marrow–derived MSC | 10 × 106 | Intracerebral | 10.70 ± 3.71 | 4.10 ± 0.99 | 15.00 ± 8.50 | 8.20 ± 3.49 | 3.90 ± 1.10 | 29.00 ± 12.87 | 6.50 ± 3.34 | 3.40 ± 0.97 | 41.5 ± 17.65 | 5.70 ± 3.12 | 3.10 ± 1.10 | 47.00 ± 24.06 | Lumbar subarachnoid injection; significant neurological improvement |
| 50.80 ± 17.43 | 10 treatment | 12.30 ± 3.95 | 4.60 ± 0.70 | 14.50 ± 13.01 | 9.40 ± 3.81 | 4.00 ± 0.82 | 26.00 ± 16.80 | 8.80 ± 3.71 | 3.60 ± 0.70 | 37.5 ± 15.86 | 8.60 ± 3.69 | 3.00 ± 1.333 | 51.50 ± 26.15 | |||||||
| Laskowitz et al. (2018) [31] | Non-RCT | 65.5 (45–79) | 10 MCA | 10 treatment | Umbilical cord blood stem cell | 1680 (840–2920) × 106 | Intravenous | 11.20 ± 1.62 | 4.40 ± 0.52 | 18.80 ± 12.26 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Significant improvement |
| Jailllard et al. (2019) [12] | RCT | 53 | n/a | 15 control | Autologous bone marrow–derived MSC | (100–300) × 106 | Intravenous | 12.75 ± 1.50 | 4.00 ± 0.00 | 42.50 ± 14.51 | 9.40 ± 4.70 | 3.00 ± 0.66 | 77.86 ± 25.40 | n/a | n/a | n/a | 8.43 ± 4.96 | 3.07 ± 1.10 | 85.00 ± 20.48 | Insignificant clinical outcome, except for the motoric score |
| 16 treatment | 13.5 ± 2.46 | 3.875 ± 0.16 | 45.00 ± 18.82 | 8.94 ± 5.20 | 3.00 ± 0.63 | 80.63 ± 30.87 | n/a | n/a | n/a | 7.73 ± 5.78 | 2.75 ± 0.93 | 82.00 ± 27.83 | ||||||||
| Savitz et al. (2019) [14] | RCT | 60.7 ± 10.4 | n/a | 19 control | Autologous bone marrow–derived ALD-401 | 3.8 × 106 | Intra-arterial | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | No significant improvement of the neurofunctional outcome between groups |
| 20 treatment | ||||||||||||||||||||
| Steinberg et al. (2019) [3] | Non-RCT | 64 (33–75) | n/a | 6 (2.5 m) * | Modified bone marrow MSC (SB623) | 2.5 × 106 | Intracerebral | 9.30 ± 1.70 | 3.22 ± 0.43 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Significant improvement of NIHSS score; insignificant result of mRS |
| 6 (5 m) * | 5 × 106 | |||||||||||||||||||
| 6 (10 m) * | 10 × 106 | |||||||||||||||||||
| Vahidy et al. (2019) [13] | Non-RCT | 63.7 ± 12.5 | n/a | 185 control | Autologous bone marrow–derived MSC | 10 × 106/kgbw | Intravenous | n/a | 0.40 ± 0.85 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Favorable safety |
| 60.7 ± 13.3 | 25 treatment | n/a | 0.08 ± 0.40 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
| Zhang et al. (2019) [11] | Prospective cohort | 42 (30–49) | n/a | 3 (12 m) * | Neural stem cell (NSI-566) | 12 × 106 | Intracerebral | 5.33 ± 3.51 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Significant improvement; imaging revealed new neural tissue formation |
| 43 (41–45) | 3 (24 m) * | 24 × 106 | 7.67 ± 2.08 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | ||||||
| 48 (37–54) | 3 (72 m) * | 72 × 106 | 6.00 ± 1.00 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | ||||||
| Chung et al. (2021) [32] | RCT | 64.27 ± 13.25 | n/a | 15 control | Autologous bone marrow–derived MSC | 1 × 106/kgbw | Intravenous | 14.47 ± 5.32 | 4.47 ± 0.83 | 19.80 ± 25.5 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Insignificant overall results; significant improvement in lower extremity motor function |
| 63.03 ± 14.36 | 39 treatment | 11.36 ± 5.20 | 4.26 ± 0.75 | 28.28 ± 26.63 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
| Kang Law et al. (2021) [33] | RCT | 64.0 ± 13.9 | 17 MCA | 9 control | Autologous bone marrow–derived MSC | 2 × 106/kgbw | Intravenous | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | Significant BI improvement compared with the control group |
| 54.60 ± 13.2 | 8 treatment | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
| Ruiz et al. (2022) [34] | RCT | 76 (69–80) | 19 MCA | 10 control | Adipose-derived MSC | 1 × 106/kgbw | Intravenous | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | No significant neurological improvement between the treatment groups |
| 78 (70–82) | 9 treatment | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | |||||||
3. Results
3.1. Demographics, Timing of Intervention, Territory of Stroke, and Type of Stem Cell
3.2. Route of Administration: Clinical Outcomes and Adverse Events
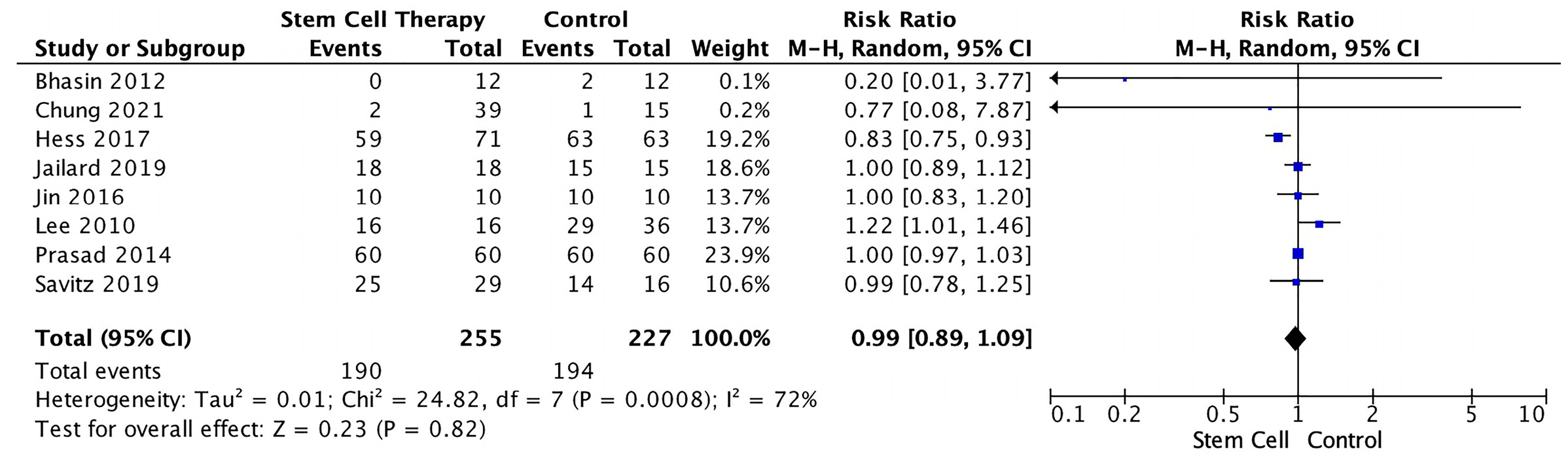
3.2.1. Clinical Outcome
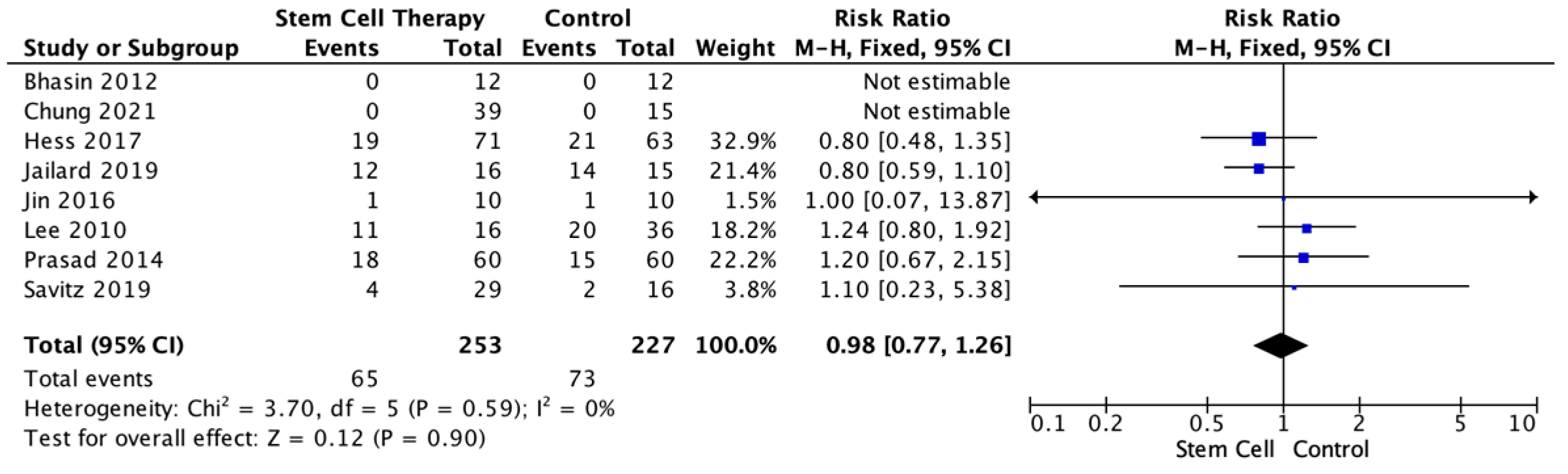
3.2.2. Adverse Events (Based on Route of Administration)
4. Discussion
4.1. Demographics, Timing of Intervention, Territory of Stroke, and Type of Stem Cell
4.2. Route of Administration: Clinical Outcome and Adverse Events
4.2.1. Intravenous Route
4.2.2. Intra-Arterial Route
4.2.3. Intracerebral Route
4.2.4. Adverse Events
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhatia, V.; Gupta, V.; Khurana, D.; Sharma, R.R.; Khandelwal, N. Randomized Assessment of the Safety and Efficacy of Intra-Arterial Infusion of Autologous Stem Cells in Subacute Ischemic Stroke. Am. J. Neuroradiol. 2018, 39, 899–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barthels, D.; Das, H. Current Advances in Ischemic Stroke Research and Therapies. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165620. [Google Scholar] [CrossRef]
- Steinberg, G.K.; Kondziolka, D.; Wechsler, L.R.; Lunsford, L.D.; Kim, A.S.; Johnson, J.N.; Bates, D.; Poggio, G.; Case, C.; McGrogan, M.; et al. Two-Year Safety and Clinical Outcomes in Chronic Ischemic Stroke Patients after Implantation of Modified Bone Marrow–Derived Mesenchymal Stem Cells (SB623): A Phase 1/2a Study. J. Neurosurg. 2019, 131, 1462–1472. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Murray, V.; Berge, E.; del Zoppo, G.J. Thrombolysis for Acute Ischaemic Stroke. Cochrane Database Syst. Rev. 2014, 2014, CD000213. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Derdeyn, C.P.; Biller, J.; Coffey, C.S.; Hoh, B.L.; Jauch, E.C.; Johnston, K.C.; Johnston, S.C.; Khalessi, A.A.; Kidwell, C.S.; et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals From the American. Stroke 2015, 46, 3020–3035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boltze, J.; Ayata, C. Challenges and Controversies in Translational Stroke Research-an Introduction. Transl. Stroke Res. 2016, 7, 355–357. [Google Scholar] [CrossRef] [Green Version]
- Singh, M.; Pandey, P.K.; Bhasin, A.; Padma, M.V.; Mohanty, S. Application of Stem Cells in Stroke: A Multifactorial Approach. Front. Neurosci. 2020, 14, 437. [Google Scholar] [CrossRef]
- Detante, O.; Jaillard, A.; Moisan, A.; Barbieux, M.; Favre, I.M.; Garambois, K.; Hommel, M.; Remy, C. Biotherapies in Stroke. Rev. Neurol. 2014, 170, 779–798. [Google Scholar] [CrossRef]
- Janowski, M.; Wagner, D.-C.; Boltze, J. Stem Cell-Based Tissue Replacement After Stroke: Factual Necessity or Notorious Fiction? Stroke 2015, 46, 2354–2363. [Google Scholar] [CrossRef] [Green Version]
- Bang, O.Y. Clinical Trials of Adult Stem Cell Therapy in Patients with Ischemic Stroke. J. Clin. Neurol. 2016, 12, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Li, Y.; Reuss, J.L.; Liu, N.; Wu, C.; Li, J.; Xu, S.; Wang, F.; Hazel, T.G.; Cunningham, M.; et al. Stable Intracerebral Transplantation of Neural Stem Cells for the Treatment of Paralysis Due to Ischemic Stroke. Stem Cells Transl. Med. 2019, 8, 999–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaillard, A.; Hommel, M.; Moisan, A.; Zeffiro, T.A.; Favre-Wiki, I.M.; Barbieux-Guillot, M.; Vadot, W.; Marcel, S.; Lamalle, L.; Grand, S.; et al. Autologous Mesenchymal Stem Cells Improve Motor Recovery in Subacute Ischemic Stroke: A Randomized Clinical Trial. Transl. Stroke Res. 2020, 11, 910–923. [Google Scholar] [CrossRef] [PubMed]
- Vahidy, F.S.; Haque, M.E.; Rahbar, M.H.; Zhu, H.; Rowan, P.; Aisiku, I.P.; Lee, D.A.; Juneja, H.S.; Alderman, S.; Barreto, A.D.; et al. Intravenous Bone Marrow Mononuclear Cells for Acute Ischemic Stroke: Safety, Feasibility, and Effect Size from a Phase I Clinical Trial. Stem Cells 2019, 37, 1481–1491. [Google Scholar] [CrossRef]
- Savitz, S.I.; Yavagal, D.; Rappard, G.; Likosky, W.; Rutledge, N.; Graffagnino, C.; Alderazi, Y.; Elder, J.A.; Chen, P.R.; Budzik, R.F.; et al. A Phase 2 Randomized, Sham-Controlled Trial of Internal Carotid Artery Infusion of Autologous Bone Marrow-Derived ALD-401 Cells in Patients With Recent Stable Ischemic Stroke (RECOVER-Stroke). Circulation 2019, 139, 192–205. [Google Scholar] [CrossRef]
- The Cochrane Collaboration Review Manager (RevMan); Version 5.4; John Wiley & Sons: Chichester, UK, 2020.
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.1.; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; Wiley & Sons: Chichester, UK, 2020. [Google Scholar]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing Reviewers’ to Authors’ Assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Hong, J.M.; Moon, G.J.; Lee, P.H.; Ahn, Y.H.; Bang, O.Y. A Long-Term Follow-Up Study of Intravenous Autologous Mesenchymal Stem Cell Transplantation in Patients With Ischemic Stroke. Stem Cells 2010, 28, 1099–1106. [Google Scholar] [CrossRef]
- Honmou, O.; Houkin, K.; Matsunaga, T.; Niitsu, Y.; Ishiai, S.; Onodera, R.; Waxman, S.G.; Kocsis, J.D. Intravenous Administration of Auto Serum-Expanded Autologous Mesenchymal Stem Cells in Stroke. Brain 2011, 134, 1790–1807. [Google Scholar] [CrossRef] [Green Version]
- Bhasin, A.; Srivastava, M.V.; Bhatia, R.; Mohanty, S.; Kumaran, S.S.; Bose, S. Autologous Intravenous Mononuclear Stem Cell Therapy in Chronic Ischemic Stroke. J. Stem Cells Regen. Med. 2012, 8, 181–189. [Google Scholar] [CrossRef]
- Prasad, K.; Mohanty, S.; Bhatia, R.; Srixivastava, M.V.P.; Garg, A.; Srivastava, A.; Goyal, V.; Tripathi, M.; Kumar, A.; Bal, C.; et al. Autologous Intravenous Bone Marrow Mononuclear Cell Therapy for Patients with Subacute Ischaemic Stroke: A Pilot Study. Indian J. Med. Res. 2012, 136, 221–228. [Google Scholar]
- Jiang, Y.; Zhu, W.; Zhu, J.; Wu, L.; Xu, G.; Liu, X. Feasibility of Delivering Mesenchymal Stem Cells via Catheter to the Proximal End of the Lesion Artery in Patients with Stroke in the Territory of the Middle Cerebral Artery. Cell Transpl. 2013, 22, 2291–2298. [Google Scholar] [CrossRef]
- Banerjee, S.; Bentley, P.; Hamady, M.; Marley, S.; Davis, J.; Shlebak, A.; Nicholls, J.; Williamson, D.A.; Jensen, S.L.; Gordon, M.; et al. Intra-Arterial Immunoselected CD34+ Stem Cells for Acute Ischemic Stroke. Stem Cells Transl. Med. 2014, 3, 1322–1330. [Google Scholar] [CrossRef]
- Chen, D.C.; Lin, S.Z.; Fan, J.R.; Lin, C.H.; Lee, W.; Lin, C.C.; Liu, Y.J.; Tsai, C.H.; Chen, J.C.; Cho, D.Y.; et al. Intracerebral Implantation of Autologous Peripheral Blood Stem Cells in Stroke Patients: A Randomized Phase II Study. Cell Transpl. 2014, 23, 1599–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, K.; Sharma, A.; Garg, A.; Mohanty, S.; Bhatnagar, S.; Johri, S.; Singh, K.K.; Nair, V.; Sarkar, R.S.; Gorthi, S.P.; et al. Intravenous Autologous Bone Marrow Mononuclear Stem Cell Therapy for Ischemic Stroke: A Multicentric, Randomized Trial. Stroke 2014, 45, 3618–3624. [Google Scholar] [CrossRef] [Green Version]
- Qiao, L.-Y.; Huang, F.-J.; Zhao, M.; Xie, J.-H.; Shi, J.; Wang, J.; Lin, X.-Z.; Zuo, H.; Wang, Y.-L.; Geng, T.-C. A Two-Year Follow-Up Study of Cotransplantation with Neural Stem/Progenitor Cells and Mesenchymal Stromal Cells in Ischemic Stroke Patients. Cell Transpl. 2014, 23, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalladka, D.; Sinden, J.; Pollock, K.; Haig, C.; McLean, J.; Smith, W.; McConnachie, A.; Santosh, C.; Bath, P.M.; Dunn, L.; et al. Human Neural Stem Cells in Patients with Chronic Ischaemic Stroke (PISCES): A Phase 1, First-in-Man Study. Lancet 2016, 388, 787–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hess, D.C.; Wechsler, L.R.; Clark, W.M.; Savitz, S.I.; Ford, G.A.; Chiu, D.; Yavagal, D.R.; Uchino, K.; Liebeskind, D.S.; Auchus, A.P.; et al. Safety and Efficacy of Multipotent Adult Progenitor Cells in Acute Ischaemic Stroke (MASTERS): A Randomised, Double-Blind, Placebo-Controlled, Phase 2 Trial. Lancet Neurol. 2017, 16, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Ying, L.; Yu, G.; Nan, G. Analysis of the Long-Term Effect of Bone Marrow Mononuclear Cell Transplantation for the Treatment of Cerebral Infarction. Int. J. Clin. Exp. Med. 2017, 10, 3059–3068. [Google Scholar]
- Laskowitz, D.T.; Bennett, E.R.; Durham, R.J.; Volpi, J.J.; Wiese, J.R.; Frankel, M.; Shpall, E.; Wilson, J.M.; Troy, J.; Kurtzberg, J. Allogeneic Umbilical Cord Blood Infusion for Adults with Ischemic Stroke: Clinical Outcomes from a Phase I Safety Study. Stem Cells Transl. Med. 2018, 7, 521–529. [Google Scholar] [CrossRef]
- Chung, J.-W.; Chang, W.H.; Bang, O.Y.; Moon, G.J.; Kim, S.J.; Kim, S.-K.; Lee, J.S.; Sohn, S.-I.; Kim, Y.-H. Efficacy and Safety of Intravenous Mesenchymal Stem Cells for Ischemic Stroke. Neurology 2021, 96, e1012–e1023. [Google Scholar] [CrossRef]
- Law, Z.K.; Tan, H.J.; Chin, S.P.; Wong, C.Y.; Wan Yahya, W.N.N.; Muda, A.S.; Zakaria, R.; Ariff, M.I.; Ismail, N.A.; Cheong, S.K.; et al. The Effects of Intravenous Infusion of Autologous Mesenchymal Stromal Cells in Patients with Subacute Middle Cerebral Artery Infarct: A Phase 2 Randomized Controlled Trial on Safety, Tolerability and Efficacy. Cytotherapy 2021, 23, 833–840. [Google Scholar] [CrossRef] [PubMed]
- de Celis-Ruiz, E.; Fuentes, B.; Alonso de Leciñana, M.; Gutiérrez-Fernández, M.; Borobia, A.M.; Gutiérrez-Zúñiga, R.; Ruiz-Ares, G.; Otero-Ortega, L.; Laso-García, F.; Gómez-de Frutos, M.C.; et al. Final Results of Allogeneic Adipose Tissue–Derived Mesenchymal Stem Cells in Acute Ischemic Stroke (AMASCIS): A Phase II, Randomized, Double-Blind, Placebo-Controlled, Single-Center, Pilot Clinical Trial. Cell Transpl. 2022, 31, 096368972210838. [Google Scholar] [CrossRef] [PubMed]
- Cancer Therapy Evaluation Program (CTEP). Common Terminology Criteria for Adverse Events (CTCAE); v.5.0 [5x7]; Cancer Therapy Evaluation Program (CTEP); 2017; p. 155. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 12 February 2023).
- De Silva, D.A.; Ebinger, M.; Davis, S.M. Gender Issues in Acute Stroke Thrombolysis. J. Clin. Neurosci. 2009, 16, 501–504. [Google Scholar] [CrossRef]
- Reeves, M.J.; Bushnell, C.D.; Howard, G.; Gargano, J.W.; Duncan, P.W.; Lynch, G.; Khatiwoda, A.; Lisabeth, L. Sex Differences in Stroke: Epidemiology, Clinical Presentation, Medical Care, and Outcomes. Lancet Neurol. 2008, 7, 915–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, M.A.; Ouyang, B.; Keppetipola, K.M.; Chen, M. Arterial Diameter and the Gender Disparity in Stroke Thrombectomy Outcomes. J. Neurointerv. Surg. 2018, 10, 949–952. [Google Scholar] [CrossRef]
- Lorenzano, S.; Ahmed, N.; Falcou, A.; Mikulik, R.; Tatlisumak, T.; Roffe, C.; Wahlgren, N.; Toni, D. Does Sex Influence the Response to Intravenous Thrombolysis in Ischemic Stroke? Stroke 2013, 44, 3401–3406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meseguer, E.; Mazighi, M.; Labreuche, J.; Arnaiz, C.; Cabrejo, L.; Slaoui, T.; Guidoux, C.; Olivot, J.-M.; Abboud, H.; Lapergue, B.; et al. Outcomes of Intravenous Recombinant Tissue Plasminogen Activator Therapy According to Gender. Stroke 2009, 40, 2104–2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S.V. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Executive Summary: Heart Disease and Stroke Statistics—2012 Update. Circulation 2012, 125, 188–197. [Google Scholar] [CrossRef]
- Borlongan, C.V.; Hadman, M.; Davis Sanberg, C.; Sanberg, P.R. Central Nervous System Entry of Peripherally Injected Umbilical Cord Blood Cells Is Not Required for Neuroprotection in Stroke. Stroke 2004, 35, 2385–2389. [Google Scholar] [CrossRef] [Green Version]
- Borlongan, C.V.; Glover, L.E.; Sanberg, P.R.; Hess, D.C. Permeating the Blood Brain Barrier and Abrogating the Inflammation in Stroke: Implications for Stroke Therapy. Curr. Pharm. Des. 2012, 18, 3670–3676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savitz, S.I. Cell Therapies: Careful Translation From Animals to Patients. Stroke 2013, 44, S107–S109. [Google Scholar] [CrossRef] [Green Version]
- Permana, A.T.; Bajamal, A.H.; Parenrengi, M.A.; Suroto, N.S.; Lestari, P.; Fauzi, A.A. Clinical Outcome and Safety of Stem Cell Therapy for Ischemic Stroke: A Systematic Review and Meta-Analysis. Surg. Neurol. Int. 2022, 13, 206. [Google Scholar] [CrossRef]
- Nogles, T.; Galuska, M. Middle Cerebral Artery Stroke; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kang, S.Y.; Kim, J.S. Anterior Cerebral Artery Infarction: Stroke Mechanism and Clinical-Imaging Study in 100 Patients. Neurology 2008, 70, 2386–2393. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Toyoda, K.; Matsuoka, H.; Okatsu, H.; Kasuya, J.; Takada, T.; Shimode, A.; Uehara, T.; Naritomi, H.; Minematsu, K. Isolated Anterior Cerebral Artery Territory Infarction: Dissection as an Etiological Mechanism. Cerebrovasc. Dis. 2010, 29, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.; Feuerstein, G.; Howells, D.W.; Hurn, P.D.; Kent, T.A.; Savitz, S.I.; Lo, E.H. Update of the Stroke Therapy Academic Industry Roundtable Preclinical Recommendations. Stroke 2009, 40, 2244–2250. [Google Scholar] [CrossRef]
- Lloyd, A.F.; Miron, V.E. The Pro-Remyelination Properties of Microglia in the Central Nervous System. Nat. Rev. Neurol. 2019, 15, 447–458. [Google Scholar] [CrossRef]
- Zacharek, A.; Shehadah, A.; Chen, J.; Cui, X.; Roberts, C.; Lu, M.; Chopp, M. Comparison of Bone Marrow Stromal Cells Derived From Stroke and Normal Rats for Stroke Treatment. Stroke 2010, 41, 524–530. [Google Scholar] [CrossRef] [Green Version]
- Yang, B.; Xi, X.; Aronowski, J.; Savitz, S.I. Ischemic Stroke May Activate Bone Marrow Mononuclear Cells to Enhance Recovery After Stroke. Stem Cells Dev. 2012, 21, 3332–3340. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, M.; Valente, S.G.; Sabongi, R.G.; Dos Santos, J.B.G.; Leite, V.M.; Ulrich, H.; Nery, A.A.; Da Silva Fernandes, M.J. Bone Marrow-Derived Mesenchymal Stem Cells versus Adipose-Derived Mesenchymal Stem Cells for Peripheral Nerve Regeneration. Neural Regen. Res. 2018, 13, 100–104. [Google Scholar] [CrossRef]
- Uccelli, A.; Laroni, A.; Freedman, M.S. Mesenchymal Stem Cells for the Treatment of Multiple Sclerosis and Other Neurological Diseases. Lancet Neurol. 2011, 10, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Simard, A.R.; Rivest, S. Bone Marrow Stem Cells Have the Ability to Populate the Entire Central Nervous System into Fully Differentiated Parenchymal Microglia. FASEB J. 2004, 18, 998–1000. [Google Scholar] [CrossRef] [Green Version]
- Kawabori, M.; Shichinohe, H.; Kuroda, S.; Houkin, K. Clinical Trials of Stem Cell Therapy for Cerebral Ischemic Stroke. Int. J. Mol. Sci. 2020, 21, 7380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xie, X.; Xiong, Y.; Liu, S.; Hu, G.; Cao, W.; Wu, X. Comparisons of the Therapeutic Effects of Three Different Routes of Bone Marrow Mesenchymal Stem Cell Transplantation in Cerebral Ischemic Rats. Brain Res. 2018, 1680, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Goyal, M.; Van Der Lugt, A.; Menon, B.K.; Majoie, C.B.L.M.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to Treatment with Endovascular Thrombectomy and Outcomes from Ischemic Stroke: Ameta-Analysis. JAMA-J. Am. Med. Assoc. 2016, 316, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Fernández, M.; Rodríguez-Frutos, B.; Álvarez-Grech, J.; Vallejo-Cremades, M.T.; Expósito-Alcaide, M.; Merino, J.; Roda, J.M.; Díez-Tejedor, E. Functional Recovery after Hematic Administration of Allogenic Mesenchymal Stem Cells in Acute Ischemic Stroke in Rats. Neuroscience 2011, 175, 394–405. [Google Scholar] [CrossRef]
- Borlongan, C.V.; Evans, A.; Yu, G.; Hess, D.C. Limitations of Intravenous Human Bone Marrow CD133+ Cell Grafts in Stroke Rats. Brain Res. 2005, 1048, 116–122. [Google Scholar] [CrossRef]
- Neal, E.G.; Liska, M.G.; Lippert, T.; Lin, R.; Gonzalez, M.; Russo, E.; Xu, K.; Ji, X.; Vale, F.L.; van Loveren, H.; et al. An Update on Intracerebral Stem Cell Grafts. Expert Rev. Neurother. 2018, 18, 557–572. [Google Scholar] [CrossRef]
- Ishizaka, S.; Horie, N.; Satoh, K.; Fukuda, Y.; Nishida, N.; Nagata, I. Intra-Arterial Cell Transplantation Provides Timing-Dependent Cell Distribution and Functional Recovery after Stroke. Stroke 2013, 44, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Balber, A.E. Concise Review: Aldehyde Dehydrogenase Bright Stem and Progenitor Cell Populations from Normal Tissues: Characteristics, Activities, and Emerging Uses in Regenerative Medicine. Stem Cells 2011, 29, 570–575. [Google Scholar] [CrossRef]
- Argibay, B.; Trekker, J.; Himmelreich, U.; Beiras, A.; Topete, A.; Taboada, P.; Pérez-Mato, M.; Vieites-Prado, A.; Iglesias-Rey, R.; Rivas, J.; et al. Intraarterial Route Increases the Risk of Cerebral Lesions after Mesenchymal Cell Administration in Animal Model of Ischemia. Sci. Rep. 2017, 7, 40758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Huang, Y.; Gong, J.; Wang, J.; Fan, Y.; Cai, J.; Wang, Y.; Qiu, Y.; Wei, Y.; Xiong, C.; et al. Transplantation of HPSC-Derived Pericyte-like Cells Promotes Functional Recovery in Ischemic Stroke Mice. Nat. Commun. 2020, 11, 5196. [Google Scholar] [CrossRef] [PubMed]
- Boshuizen, M.C.S.; Steinberg, G.K. Stem Cell–Based Immunomodulation After Stroke. Stroke 2018, 49, 1563–1570. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yu, S.; Tuazon, J.P.; Lee, J.-Y.; Corey, S.; Kvederis, L.; Kingsbury, C.; Kaneko, Y.; Borlongan, C.V. Neuroprotective Effects of Human Bone Marrow Mesenchymal Stem Cells against Cerebral Ischemia Are Mediated in Part by an Anti-Apoptotic Mechanism. Neural Regen. Res. 2019, 14, 597–604. [Google Scholar] [CrossRef]
- Rodríguez-Frutos, B.; Otero-Ortega, L.; Gutiérrez-Fernández, M.; Fuentes, B.; Ramos-Cejudo, J.; Díez-Tejedor, E. Stem Cell Therapy and Administration Routes After Stroke. Transl. Stroke Res. 2016, 7, 378–387. [Google Scholar] [CrossRef]
- Stonesifer, C.; Corey, S.; Ghanekar, S.; Diamandis, Z.; Acosta, S.A.; Borlongan, C.V. Stem Cell Therapy for Abrogating Stroke-Induced Neuroinflammation and Relevant Secondary Cell Death Mechanisms. Prog. Neurobiol. 2017, 158, 94–131. [Google Scholar] [CrossRef]
- Lioutas, V.A.; Alfaro-Martinez, F.; Bedoya, F.; Chung, C.C.; Pimentel, D.A.; Novak, V. Intranasal Insulin and Insulin-Like Growth Factor 1 as Neuroprotectants in Acute Ischemic Stroke. Transl. Stroke Res. 2015, 6, 264–275. [Google Scholar] [CrossRef]



| PICOS Item | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population |
|
|
| Intervention | Stem cell therapy via intracerebral administration | |
| Comparison |
| |
| Outcome measures |
| |
| Study design |
|
|
| Publication |
|
|
| Description | Number, n (%) | |
|---|---|---|
| Total patients | n | 817 participants |
| Median age | Median (min–max) | 60.6 years (30–85) |
| Gender | ||
| Male | n | 247 participants (60.83%) |
| Female | n | 159 participants (39.16%) |
| Comorbidities | ||
| Hypertension | n | 118 participants (29.06%) |
| Diabetes mellitus | n | 68 participants (16.74%) |
| Dyslipidemia | n | 70 participants (17.24%) |
| Cardiac problems | n | 54 participants (13.3%) |
| Smoking | n | 80 participants (19.7%) |
| Standard treatment modalities | ||
| Tissue Plasminogen Activator (TPA) | n | 2 studies |
| Mechanical revascularization | n | 2 studies |
| Patients with stem cell therapy | n | 406 participants (49.7%) |
| Based on the route of administration | ||
| Intracerebral group (5 studies) | n | 64 participants (15.76%) |
| Intra-arterial group (3 studies) | n | 38 participants (9.35%) |
| Intravenous group (13 studies) | n | 304 participants (74.87%) |
| Based on stroke onset | ||
| Acute (1–7 days) | n | 82 participants (20.2%) |
| Subacute (1–3 weeks) | n | 143 participants (35.22%) |
| Chronic (>3 weeks) | n | 108 participants (26.6%) |
| Based on stem cell source | ||
| Bone marrow | n | 265 participants (65.27%) |
| Peripheral blood | n | 20 participants (4.92%) |
| Umbilical blood | n | 20 participants (4.92%) |
| Multipotent stem cell | n | 71 participants (17.49%) |
| Neural stem cell | n | 20 participants (4.92%) |
| Adipose | n | 9 participants (2.21%) |
| Based on stroke territory | ||
| Anterior Cerebral Artery (ACA) and Middle Cerebral Artery (MCA) | n | 8 participants (2.4%) |
| ACA | n | 6 participants (1.8%) |
| MCA | n | 297 participants (87.6%) |
| Anterior circulation | n | 13 participants (3.8%) |
| Posterior circulation | n | 7 participants (2.09%) |
| Description | Number n (%) | |
|---|---|---|
| Clinical outcome baseline | ||
| NIHSS | ||
| Intracerebral group | Mean ± SD | 9.03 ± 1.76 |
| Intra-arterial group | Mean ± SD | 10.4 ± 5.13 |
| Intravenous group | Mean ± SD | 12.20 ± 4.10 |
| mRS | ||
| Intracerebral group | Mean ± SD | 3.36 ± 0.38 |
| Intra-arterial group | Mean ± SD | 3.89 ± 0.83 |
| Intravenous group | Mean ± SD | 3.30 ± 0.65 |
| BI | ||
| Intracerebral group | Mean ± SD | 13.48 ± 7.12 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 34.21 ± 21.64 |
| Clinical outcome after 6 months | ||
| NIHSS | ||
| Intracerebral group | Mean ± SD | 6.96 ± 2.36 |
| Intra-arterial group | Mean ± SD | 2.2 ± 1.92 |
| Intravenous group | Mean ± SD | 7.25 ± 5.31 |
| mRS | ||
| Intracerebral group | Mean ± SD | 3.34 ± 0.63 |
| Intra-arterial group | Mean ± SD | 2.33 ± 0.86 |
| Intravenous group | Mean ± SD | 2.63 ± 0.90 |
| BI | ||
| Intracerebral group | Mean ± SD | 26 ± 16.80 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 76.85 ± 21.41 |
| Clinical outcome after 12 months | ||
| NIHSS | ||
| Intracerebral group | Mean ± SD | 6.21 ± 2.49 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 1.58 ± 2.02 |
| mRS | ||
| Intracerebral group | Mean ± SD | 2.7 ± 0.46 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | n/a |
| BI | ||
| Intracerebral group | Mean ± SD | 25.38 ± 8.74 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | n/a |
| Clinical outcome after 24 months | ||
| NIHSS | ||
| Intracerebral group | Mean ± SD | 6.67 ± 4.03 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 7.73 ± 5.78 |
| mRS | ||
| Intracerebral group | Mean ± SD | 3 ± 1.33 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 2.75 ± 0.93 |
| BI | ||
| Intracerebral group | Mean ± SD | 31.86 ± 13.76 |
| Intra-arterial group | Mean ± SD | n/a |
| Intravenous group | Mean ± SD | 82 ± 27.83 |
| Author(s) | Patients | Sample Size | Route of Administration | AE | SAE (CTCAE 3 or More) | SAE Details |
|---|---|---|---|---|---|---|
| Jailllard et al. (2019) [12] | 31 | 15 control | Intravenous | 24 | 14 | 1 death, 1 recurrent stroke, 2 humeral fracture, 5 epileptic, 3 pneumonia, 1 gastrostomy, 1 atrial flutter |
| 16 treatment | 18 | 12 | 2 depression, 1 humeral fracture, 6 epileptic, 1 DVT, 2 pneumonia | |||
| Lee et al. (2010) [19] | 52 | 36 control | Intravenous | 29 | 20 | 1 new onset stroke, 2 angina, 9 pneumonia, 1 acute kidney injury, 1 systemic cancer, 1 benign mass, 5 seizure |
| 16 treatment | 18 | 11 | 2 new onset strokes, 1 angina, 1 PAOD, 3 pneumonia, 1 benign mass, 3 seizure | |||
| Honmou et al. (2011) [20] | 12 | 12 treatment | Intravenous | 6 | 0 | None |
| Bhasin et al. (2012) [21] | 24 | 12 control | Intravenous | 2 | 0 | None |
| 12 treatment | 0 | 0 | ||||
| Prasad et al. (2012) [22] | 11 | 11 treatment | Intravenous | 0 | 0 | None |
| Jiang et al., 2013 [23] | 4 | 4 treatment | Intra-arterial | n/a | 0 | None |
| Banerjee et al. (2014) [24] | 5 | 5 treatment | Intra-arterial | 1 | 1 | 1 pneumonia |
| Chen et al. (2014) [25] | 30 | 15 control | Intracerebral | n/a | 0 | None |
| 15 treatment | n/a | 0 | ||||
| Prasad et al. (2014) [26] | 120 | 60 control | Intravenous | 60 | 15 | 1 hypotension, 1 pneumonia, 1 fracture in lower limb, 5 death, 7 CNS AE |
| 60 treatment | 61 | 18 | 1 pneumonia, 1 PAOD, 2 fractures in the lower limb, 8 death, 6 CNS AE | |||
| Qiao et al. (2014) [27] | 6 | 6 treatment | Intravenous | 5 | 0 | 4 fever, 1 dizziness |
| Kalladka et al. (2016) [28] | 11 | 3 (2 m) | Intracerebral | n/a | 16 | 1 subdural hematoma, 1 epidural hematoma, 1 stroke, 1 cystoscopy, 2 bleed on burrhole site, 1 malignant melanoma, 5 gastrointestinal AE, 1 seizure, 1 alcohol withdrawal syndrome, 1 collapse, 1 community-acquired pneumonia |
| 3 (5 m) | ||||||
| 3 (10 m) | ||||||
| Hess et al. (2017) [29] | 134 | 2 (20 m) | Intravenous | 64 | 21 | 6 severe, 6 LT, 9 deaths |
| 71 treatment | 59 | 19 | 11 severe, 3 LT, 5 deaths | |||
| Jin et al. (2017) [30] | 20 | 10 control | Intracerebral | 12 | 1 | 1 death due to large infarction |
| 10 treatment | 12 | 1 | 1 pneumonia | |||
| Laskowitz et al. (2018) [31] | 10 | 10 treatment | Intravenous | 113 | 8 | 112 AEs were unrelated to the treatment group |
| Savitz et al. (2019) [15] | 48 | 19 control | Intra-arterial | 14 | 2 | 1 new onset stroke, 1 astrocytoma, |
| 20 treatment | 25 | 4 | 1 muscular pain, 1 UTI, 1 embolism, 1 brain edema | |||
| Steinberg et al. (2019) [3] | 18 | 6 (2.5 m) | Intracerebral | 20 | 9 | 1 seizure, 1 stenting of the carotid artery, 1 asymptomatic subdural hygroma, 1 TIA, 1 hypesthesia, 1 dysphagia, 1 UTI, 1 sepsis, 1 pneumonia |
| 6 (5 m) | 31 | |||||
| 6 (10 m) | 25 | |||||
| Zhang et al. (2019) [11] | 9 | 3 (12 m) | Intracerebral | 18 | 2 | 2 cholecystitis |
| 3 (24 m) | 2 | 0 | None | |||
| 3 (72 m) | 15 | 0 | None | |||
| Vahidy et al. (2019) [13] | 210 | 185 control | Intravenous | 227 | 24 | No study-related SAE in the therapy group |
| 25 treatment | ||||||
| Chung et al. (2021) [32] | 54 | 15 control | Intravenous | 1 | 0 | None |
| 39 treatment | 2 | 0 | None | |||
| Kang Law et al. (2021) [33] | 17 | 9 control | Intravenous | 2 | 2 | No study-related SAE in the therapy group |
| 8 treatment | 2 | 2 | ||||
| Ruiz et al. (2022) [34] | 19 | 10 control | Intravenous | 12 | 12 | No study-related SAE in the therapy group |
| 9 treatment | 0 | 0 |
| Route of Administration | Number of Patients in Studies Reporting AEs | Number of AEs | Number of SAEs | SAEs/Total Patients |
|---|---|---|---|---|
| Intravenous | 295 | 282 | 68 | 23.05% |
| Intra-arterial | 29 | 26 | 5 | 17.24% |
| Intracerebral | 63 | 123 | 28 | 44.44% |
| Total | 387 | 431 | 101 | 26.09% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fauzi, A.A.; Thamrin, A.M.H.; Permana, A.T.; Ranuh, I.G.M.A.R.; Hidayati, H.B.; Hamdan, M.; Wahyuhadi, J.; Suroto, N.S.; Lestari, P.; Chandra, P.S. Comparison of the Administration Route of Stem Cell Therapy for Ischemic Stroke: A Systematic Review and Meta-Analysis of the Clinical Outcomes and Safety. J. Clin. Med. 2023, 12, 2735. https://doi.org/10.3390/jcm12072735
Fauzi AA, Thamrin AMH, Permana AT, Ranuh IGMAR, Hidayati HB, Hamdan M, Wahyuhadi J, Suroto NS, Lestari P, Chandra PS. Comparison of the Administration Route of Stem Cell Therapy for Ischemic Stroke: A Systematic Review and Meta-Analysis of the Clinical Outcomes and Safety. Journal of Clinical Medicine. 2023; 12(7):2735. https://doi.org/10.3390/jcm12072735
Chicago/Turabian StyleFauzi, Asra Al, Ahmad Muslim Hidayat Thamrin, Andhika Tomy Permana, I. G. M. Aswin R. Ranuh, Hanik Badriyah Hidayati, Muhammad Hamdan, Joni Wahyuhadi, Nur Setiawan Suroto, Pudji Lestari, and Poodipedi Sarat Chandra. 2023. "Comparison of the Administration Route of Stem Cell Therapy for Ischemic Stroke: A Systematic Review and Meta-Analysis of the Clinical Outcomes and Safety" Journal of Clinical Medicine 12, no. 7: 2735. https://doi.org/10.3390/jcm12072735