
Real-World Use and Predictors of Response to Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Patient Evaluation and Management
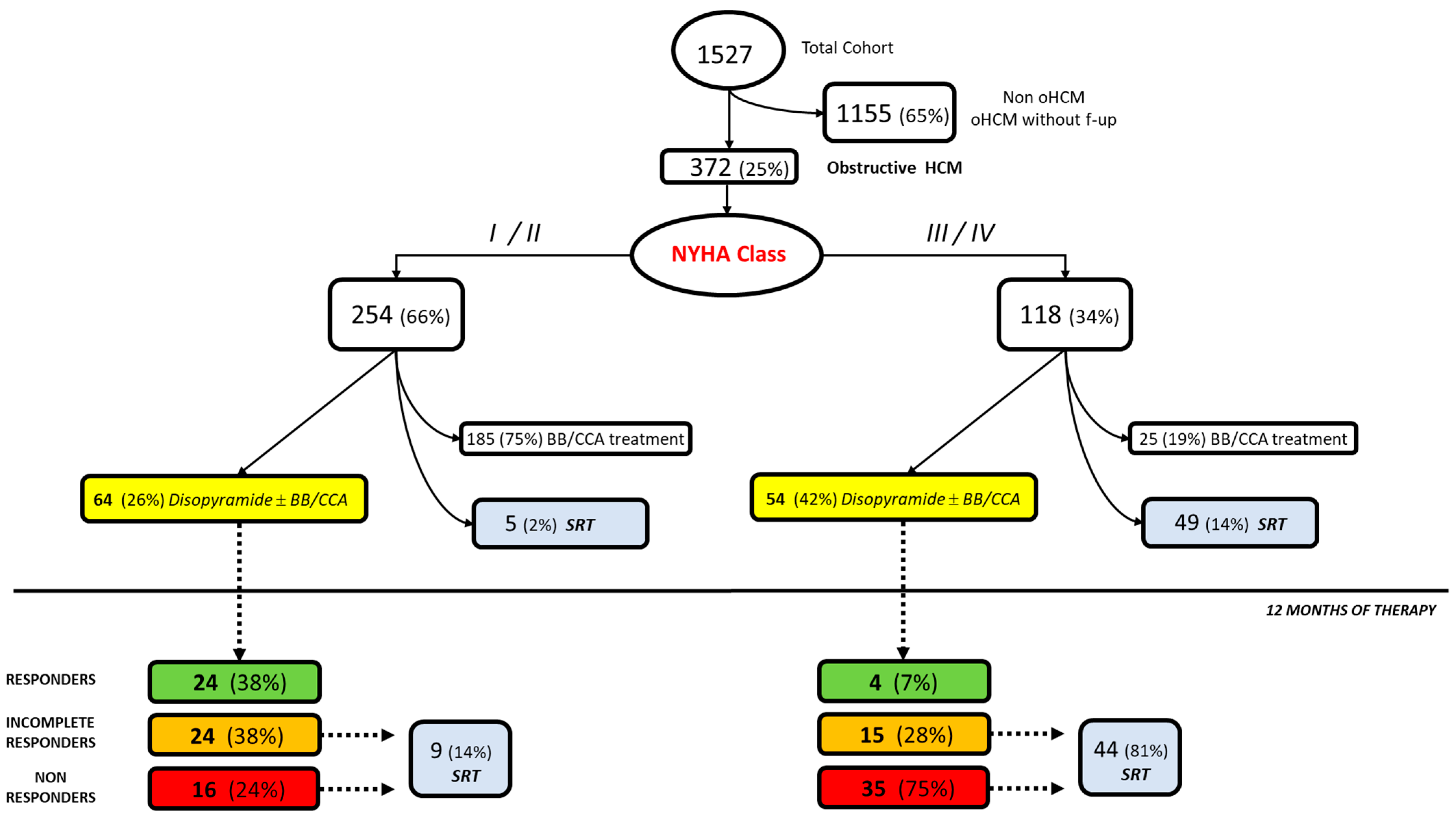
- Patients with a function class NYHA I and symptoms related to LVOT obstruction or NYHA II were treated with non-vasodilating beta-blockers titrated to maximum tolerated dose or, if contraindicated verapamil (starting dose 40 mg three times daily to maximum 480 mg daily);
- Patients with a function class NYHA I and symptoms related to LVOT obstruction or NYHA II-III, after ineffective 6-month treatment with beta-blockers/verapamil, disopyramide was introduced up to a maximum tolerated dose (usually 400–500 mg/day). Exclusion criteria for disopyramide initiation were glaucoma, men with prostatism, patient with baseline QTc > 550 msec, and those with LVEF < 50%;
- Patients with an LVOTO gradient ≥ 50 mm Hg, moderate-to-severe symptoms (New York Heart Association (NYHA) functional Class III–IV), and/or recurrent exertional syncope in spite of maximally tolerated negative inotropic therapy were proposed with an invasive management of LVOT gradient.
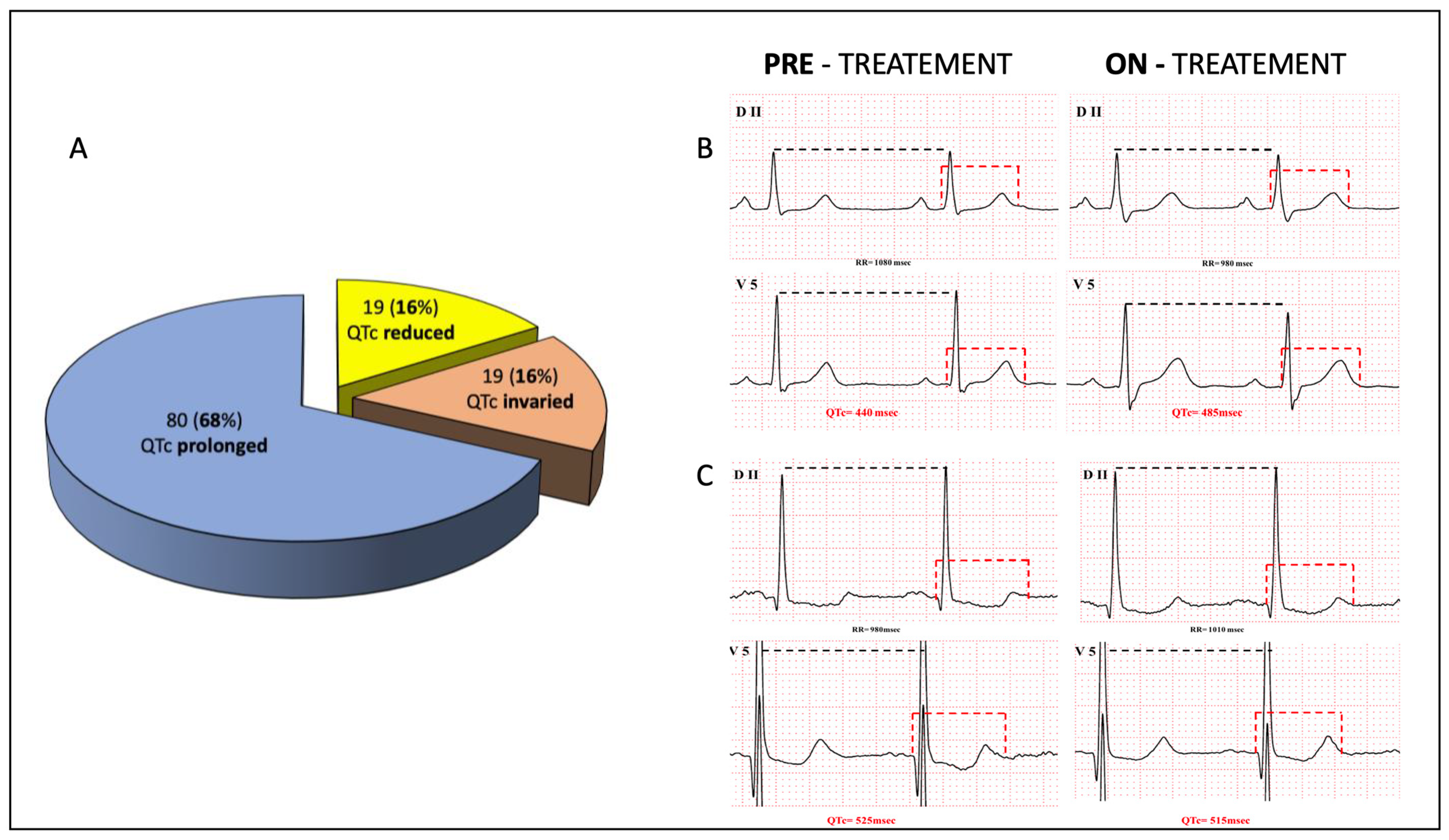
2.3. Twelve-Lead Electrocardiogram Analysis
2.4. Definition of the Response to Disopyramide
- Responders: patients with a functional class NYHA = I and a LVOT gradient < 30 mmHg.
- Incomplete responders: patients with a functional class NYHA > I and a LVOT gradient < 30 mmHg.
- Non-responders: symptomatic patients with no change in functional class NYHA and a LVOT gradient > 30 mmHg.
2.5. Statistical Analysis
3. Results
3.1. Clinical and Echocardiographic Profile of Patients with Obstructive HCM
3.2. Efficacy and Criteria of Response to Disopyramide Therapy
3.3. Safety of Disopyramide Therapy
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maron, B.J. Clinical course and management of hypertrophic cardiomyopathy. N. Engl. J. Med. 2018, 379, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Maurizi, N.; Olivotto, I.; Maron, M.S.; Bonacchi, G.; Antiochos, P.; Tomberli, B.; Fumagalli, C.; Poggesi, C.; Berteotti, M.; Girolami, F.; et al. Lifetime Clinical Course of Hypertrophic Cardiomyopathy: Outcome of the Historical Florence Cohort over Five Decades. JACC Adv. 2023, in press. [Google Scholar]
- Maron, M.S.; Olivotto, I.; Zenovich, A.G.; Link, M.S.; Pandian, N.G.; Kuvin, J.T.; Nistri, S.; Cecchi, F.; Udelson, J.E.; Maron, B.J. Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction. Circulation 2006, 114, 2232–2239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurizi, N.; Ammirati, E.; Coppini, R.; Morrone, A.; Olivotto, I. Clinical and Molecular Aspects of Cardiomyopathies: Emerging Therapies and Clinical Trials. Heart Fail. Clin. 2018, 14, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H. Authors/Task Force members. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [PubMed]
- Sherrid, M.V.; Barac, I.; McKenna, W.J.; Elliott, P.M.; Dickie, S.; Chojnowska, L.; Casey, S.; Maron, B.J. Multicenter study of the efficacy and safety of disopyramide in obstructive hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2005, 45, 1251–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrid, M.V.; Shetty, A.; Winson, G.; Kim, B.; Musat, D.; Alviar, C.L.; Homel, P.; Balaram, S.K.; Swistel, D.G. Treatment of obstructive hypertrophic cardiomyopathy symptoms and gradient resistant to first-line therapy with beta-blockade or verapamil. Circ. Heart Fail. 2013, 6, 694–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habib, M.; Hoss, S.; Bruchal-Garbicz, B.; Chan, R.H.; Rakowski, H.; Williams, L.; Adler, A. Markers of responsiveness to disopyramide in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2019, 297, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.; Fourey, D.; Weissler-Snir, A.; Hindieh, W.; Chan, R.H.; Gollob, M.H.; Rakowski, H. Safety of Outpatient Initiation of Disopyramide for Obstructive Hypertrophic Cardiomyopathy Patients. J. Am. Heart Assoc. 2017, 6, e005152. [Google Scholar] [CrossRef] [PubMed]
- Masri, A.; Olivotto, I. Cardiac Myosin Inhibitors as a Novel Treatment Option for Obstructive Hypertrophic Cardiomyopathy: Addressing the Core of the Matter. J. Am. Heart Assoc. 2022, 11, e024656. [Google Scholar] [CrossRef] [PubMed]
- Coppini, R.; Ferrantini, C.; Pioner, J.M.; Santini, L.; Wang, Z.J.; Palandri, C.; Scardigli, M.; Vitale, G.; Sacconi, L.; Stefàno, P.; et al. Electrophysiological and Contractile Effects of Disopyramide in Patients With Obstructive Hypertrophic Cardiomyopathy: A Translational Study. JACC Basic Transl. Sci. 2019, 4, 795–813. [Google Scholar] [CrossRef] [PubMed]
- Zampieri, M.; Argirò, A.; Marchi, A.; Berteotti, M.; Targetti, M.; Fornaro, A.; Tomberli, A.; Stefàno, P.; Marchionni, N.; Olivotto, I. Mavacamten, a Novel Therapeutic Strategy for Obstructive Hypertrophic Cardiomyopathy. Curr. Cardiol. Rep. 2021, 23, 79. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e533–e557. [Google Scholar] [PubMed]
- Honerjäger, P. The contribution of Na channel block to the negative inotropic effect of antiarrhythmic drugs. Basic Res. Cardiol. 1986, 81 (Suppl. 1), 33–37. [Google Scholar] [CrossRef] [PubMed]
- Quintana, E.; Bajona, P.; O Myers, P. Mavacamten for hypertrophic obstructive cardiomyopathy. Lancet 2021, 397, 369. [Google Scholar] [CrossRef] [PubMed]
- Gurwitz, J.H.; Maurer, M.S. Tafamidis—A Pricey Therapy for a Not-So-Rare Condition. JAMA Cardiol. 2020, 5, 247. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Oreziak, A.; Barriales-Villa, R.; Abraham, T.P.; Masri, A.; Garcia-Pavia, P.; Saberi, S.; Lakdawala, N.K.; Wheeler, M.T.; Owens, A.; et al. Mavacamten for treatment of symptomatic obstructive hypertrophic cardiomyopathy (EXPLORER-HCM): A randomised, double-blind, placebo-controlled, phase 3 trial; EXPLORER-HCM study investigators. Lancet 2020, 396, 759–769. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Total Cohort (n = 118) | Responders (n = 28) | Incomplete Responders (n = 39) | Non-Responders (n = 51) | |
|---|---|---|---|---|---|
| Demographic | |||||
| Age (ys) | 55 ± 16 | 48 ± 9 * | 51 ± 11 | 58 ± 12 | |
| Male sex (n, %) | 63 (53%) | 16 (57%) | 19 (49%) | 28 (55%) | |
| Medical History | |||||
| NYHA Class I–II (n, %) | 64 (54 %) | 24 (86%) * | 24 (62%) | 16 (31%) | |
| NYHA Class III (n, %) | 53 (46 %) | 3 (11%) | 15 (38%) | 35 (69%) * | |
| NYHA Class IV (n, %) | 1 (1.5%) | 1 (3%) | 0 | 0 | |
| Atrial fibrillation (n, %) | 32 (27%) | 6 (21%) | 11 (28%) | 15 (29%) | |
| Syncope (n, %) | 27 (0.12 %) | 1 (4%) * | 12 (31%) | 14 (27%) | |
| PM/ICD (n, %) | 11 (9%) | 1 (4%) * | 3 (8%) | 7 (14%) | |
| NSVT (n, %) | 22 (19%) | 3 (11%) | 6 (15%) | 13 (25%) | |
| Cardiac Arrest (n, %) | 1 (0.8%) | 0 | 1 (2.5%) | 0 | |
| Treatments | |||||
| Beta-blockers (n, %) | 99 (84 %) | 22 (79%) | 35 (90%) | 42 (81%) | |
| Calcium-Antagonist (n, %) | 14 (8 %) | 2 (8%) | 4 (10%) | 8 (16%) | |
| Amiodarone (n, %) | 12 (10 %) | 1 (4%) | 4 (10%) | 7 (14%) | |
| Echocardiogram | |||||
| SAM (n, %) | 95 (80%) | 22 (78%) | 33 (85%) | 40 (78%) | |
| Left Atrial diameter (mm) | 45 ± 7 | 42 ± 5 * | 44 ± 6 | 46 ± 7 | |
| LV Maximal Wall Thickness (mm) | 22 ± 5 | 21 ± 4 | 22 ± 5 | 22 ± 6 | |
| Resting LVOTO (mmHg) | 72 ± 36 | 69 ± 21 | 70 ± 18 | 73 ± 22 | |
| 30 mmHg < LVOTO < 50 mmHg (n, %) | 42 (36%) | 13 (46%) | 10 (26%) | 19 (37%) | |
| LVOTO > 50 mmHg (n, %) | 76 (64%) | 15 (54 %) | 29 (74 %) * | 32 (63%) | |
| Maximal LVOTO (mmHg) | 88 ± 35 | 71 ± 12 | 91 ± 13 | 85 ± 21 | |
| LV Ejection Fraction (%) | 66 ± 7 | 69 ± 8 | 66 ± 6 | 63 ± 8 * |
| Variables | Pre-Treatment | On Treatment | p Values |
|---|---|---|---|
| HR (bpm) | 60 ± 8 | 59 ± 79 | 0.45 |
| PR (msec) | 178 ± 22 | 183 ± 24 | <0.01 |
| AVB I (n) | 10 (8%) | 22 (17%) | <0.01 |
| QRS (msec) | 101 ± 22 | 109 ± 26 | 0.10 |
| New Onset Bundle Branch Block (n) | 14 (11%) | 20 (16%) | 0.62 |
| QTcmax (msec) | 423 ± 29 | 475 ± 41 | 0.67 |
| QTc ≥ 480 msec | 30 (24%) | 56 (48%) | <0.01 |
| QTc ≥ 500 msec | 14 (11%) | 36 (28%) | <0.01 |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Age (per 10 decrease) | 1.4 | [0.5–3.6] | 0.03 | |||
| NYHA Class I-II (n) | 5.1 | [2.3–11.2] | <0.01 | 1.5 | [1.1–4.5] | 0.03 |
| Left atrial diameter (per 2 mm decrease) | 2.1 | [0.9–7.8] | <0.01 | |||
| LV EF (per 5 increase) | 4.2 | [1.3–9.9] | <0.01 | 1.9 | [0.9–6.4] | 0.07 |
| Total Cohort (n = 118) | Treatment Reduction | Treatment Suspension | |
|---|---|---|---|
| Anticholinergic collateral effects | 29 (24%) | 5 (4%) | 10 (8%) |
| Xerostomia/Xerophthalmia | 13 (11%) | 4 (3%) | 8 (7%) |
| Stypsis | 10 (8%) | 1 (0.8%) | 1 (0.8%) |
| Blurred vision | 2 (2%) | 1 (0.8%) | 0 |
| Urinary Retention | 4 (3%) | 0 | 1 |
| Sustained Ventricular Arrhythmias | 0 | - | - |
| Torsade de Pointes | 0 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maurizi, N.; Chiriatti, C.; Fumagalli, C.; Targetti, M.; Passantino, S.; Antiochos, P.; Skalidis, I.; Chiti, C.; Biagioni, G.; Tomberli, A.; et al. Real-World Use and Predictors of Response to Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy. J. Clin. Med. 2023, 12, 2725. https://doi.org/10.3390/jcm12072725
Maurizi N, Chiriatti C, Fumagalli C, Targetti M, Passantino S, Antiochos P, Skalidis I, Chiti C, Biagioni G, Tomberli A, et al. Real-World Use and Predictors of Response to Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy. Journal of Clinical Medicine. 2023; 12(7):2725. https://doi.org/10.3390/jcm12072725
Chicago/Turabian StyleMaurizi, Niccolò, Chiara Chiriatti, Carlo Fumagalli, Mattia Targetti, Silvia Passantino, Panagiotis Antiochos, Ioannis Skalidis, Chiara Chiti, Giulia Biagioni, Alessia Tomberli, and et al. 2023. "Real-World Use and Predictors of Response to Disopyramide in Patients with Obstructive Hypertrophic Cardiomyopathy" Journal of Clinical Medicine 12, no. 7: 2725. https://doi.org/10.3390/jcm12072725